

Abstract
Cohen and Wills (Cohen, S., & Wills, T. A., 1985, Stress, social support, and the buffering hypothesis. Psychological Bulletin, 98, 310–357) described two broad models whereby social support could mitigate the deleterious effects of stress on health: a main effect model and stress-buffering model. A specific application of these models was tested in a three-wave, multimethod study of 1888 children to assess ways parental support (social support) mitigates the effects of peer victimization (stress) on children’s depressive symptoms and depression-related cognitions (health-related outcomes). Results revealed that (a) both supportive parenting and peer victimization had main effects on depressive symptoms and cognitions; (b) supportive parenting and peer victimization did not interact in the prediction of depressive thoughts and symptoms; (c) these results generalized across age and gender; and (d) increases in depressive symptoms were related to later reduction of supportive parenting and later increase in peer victimization. Although supportive parenting did not moderate the adverse outcomes associated with peer victimization, results show that its main effect can counterbalance or offset these effects to some degree. Implications for practice and future research are discussed.
Keywords: parenting, peer victimization, bullying, depression, children and adolescents
Can positive and supportive parenting alleviate the adverse effects of peer victimization on depressive thoughts and symptoms in children and young adolescents? Peer victimization has been linked to serious psychological outcomes, most notably, internalizing disorders such as depression (Hawker & Boulton, 2000; Reijntjes, Kamphuis, Prinzie, & Telch, 2010). In contrast, various types of social support, including parental support, are related to lower levels of childhood depression (e.g., McLeod, Weisz, & Wood, 2007). Somewhat surprisingly, relatively few studies have examined the combined effects of supportive parenting and peer victimization on depressive symptoms in childhood. At least two processes are possible (Cohen & Wills, 1985). One is that supportive parenting has a main effect1 that mitigates depression-related outcomes in young people, irrespective of their level of peer victimization. The other possibility is that supportive parenting is especially helpful to youths who are victimized by their peers; that is, supportive parenting could moderate or buffer the adverse effect of peer victimization. The primary goal of the current study was to examine these two processes whereby supportive parenting may mitigate the depressive effects of peer victimization in young people.
Depression is one of the most common psychiatric problems experienced by children and adolescents. By age 18, nearly one fourth of all children will have experienced clinically significant symptoms of depression (Lewinsohn, Hops, Roberts, Seeley, & Andrews, 1993). One psychosocial factor that has been repeatedly linked to psychosocial maladjustment in general and depression in particular is peer victimization. Cross-sectional and longitudinal linkages between peer victimization and psychological maladjustment have been well documented. Hawker and Boulton’s (2000) meta-analysis of cross-sectional studies showed that, compared to nonvictimized peers, victimized children show substantially higher rates of internalizing problems. In a subsequent quantitative review of longitudinal studies, Reijntjes et al. (2010) reported that internalizing problems functioned as both an antecedent and a consequence of victimization. Still other studies have demonstrated that peer victimization can interact with particular individual difference variables (e.g., cognitive style) to increase the likelihood of developing an internalizing disorder (Barchia & Bussey, 2010; Prinstein & Aikins, 2004). Taken together, these results suggest that victimized children are at greater risk of developing internalizing problems, such as depression, than are their nonvictimized peers.
Given the strength of these connections, understanding factors that may mitigate the depressive effects of victimization is critical. Previous research has noted that supportive interpersonal relationships and supportive parenting in particular, can protect against symptoms of depression (e.g., Auerbach, Bigda-Peyton, Eberhart, Webb, & Ho, 2011; Cornwell, 2003), mitigate the development of cognitive diatheses for depression (e.g., negative automatic thoughts about self, world, and future), and foster the development of several domains of self-perceived competence (Bruce et al., 2006). Adolescents with high parental support are better adjusted and less distressed than adolescents with low parental support (Holahan, Valentiner, & Moos, 1995). In addition, higher levels of supportive parenting are associated with lower levels of depressive symptoms (Allen et al., 2006; Dallaire et al., 2006). Less supportive interactions between a parent and child are associated with more serious depressive symptoms and more negative cognitive styles (Lewinsohn et al., 1994; Mezulis, Hyde, & Abramson, 2006; Rapee, 1997). Less supportive (and more conflictual) family environments are associated with higher levels of child depression, both at the time of measurement and 1 year later (Sheeber, Hops, Alpert, Davis, & Andrews, 1997). Literature reviews show that low levels of parental support (and high levels of parental rejection) are linked to high levels of childhood depression and anxiety (McLeod et al., 2007; Rapee, 1997).
Exactly how supportive parenting may mitigate the adverse effects of peer victimization with regard to depression is unclear. Cohen and Wills (1985) proposed two broad models whereby stress and social support can conjointly influence psychological adjustment. One is a stress-buffering model in which social support moderates the deleterious effect of the stressor. This model can be applied here, as peer victimization represents a major childhood stressor (Newman, Holden, & Delville, 2005; Spirito, Stark, Grace, & Stamoulis, 1991) and supportive parenting represents a major source of social support for children (Bokhorst, Sumter, & Westenberg, 2010; Furman, & Buhrmester, 1992). Such moderation (or buffering) could occur because supportive parenting affects the stress appraisal process; that is, supportive parenting could foster the belief that resources are available, which then diminishes the perception of stress. In other words, supportive parenting could make peer victimization seem less bad, thereby detoxifying peer victimization at least to some degree. Statistical support for the stress-buffering model would consist of a statistical interaction between social support and the stressor in the predication of psychological symptoms (Cohen & Wills, 1985).
Cohen and Wills (1985) also described a main effect model, which suggests that social support has a positive effect on psychological outcomes regardless of the level of stress or adversity experienced. Applied to peer victimization and depression in young people, this model dovetails with our own speculations about the developmental psychopathology of depression. We have suggested that cognitive diatheses for depression likely develop when children are exposed to (and then internalize) repeated negative feedback about themselves (Cole, 1991; Cole, Martin, & Powers, 1997; Cole, Maxwell, & Dukewich 2010; see also Beck, 1967). This effect is strongest in late childhood and early adolescence when a major developmental task is the construction of competency-related self-perceptions (Garber, 1984). On the one hand, chronic peer victimization constitutes a major source of negative self-relevant information that can lead to construction of incompetence beliefs and even depressive cognitive self-schemas. On the other hand, supportive parenting conveys acceptance and worthiness to the child, positive information that can lead to the construction of competency beliefs, which can offset or counterbalance the depressive effects of incompetency beliefs (Harter, 1999, 2012; Cole, 1991). Statistical support for such a model would consist of a positive main effect for social support over-and-above the negative main effect of the stressor (Cohen & Wills, 1985).
Five previous studies have examined the relation of peer victimization and supportive parenting on depressive symptoms. Results have been mixed. First, Conners-Burrow et al. (2009) divided groups of 5th, 9th, and 11th grade students into four bully/victim status groups. Parental social support was protective for all groups, in a manner consistent with the main effects model; however, the effects were strongest for children who were both victims and bullies (in a manner suggestive of the stress-buffering model). In a second study, Papafratzeskakou, Kim, Longo, and Riser (2011) examined the effects of parental support and peer victimization on depression in a sample of 261 children between the ages of 10 and 14. They found a main effect of parental support on depressive symptoms, regardless of victimization status or gender. Third, Stadler, Feifel, Rohrmann, Verneiren, and Poustka (2010) examined the effects of parental support and peer victimization on mental health problems in a sample of 986 German students between the ages of 11 and 18. They reported a significant parental support × peer victimization interaction and a significant main effect for parental support, providing support for both models (especially for younger female students). Fourth, Davidson and Demaray (2007) examined the relation between peer victimization, parental support and internalizing distress in 355 4th to 6th graders. Their results suggested parental support moderated the effects of bullying on “internalizing distress” in girls but not boys. Finally, Tanigawa, Furlong, Felix, and Sharkey (2011) formally tested Cohen and Wills’ (1985) main effect versus stress-buffering models in a sample of 7th and 8th grade students. They reported a main effect of parental support on depressive symptoms in girls and an interaction between parental support and peer victimization for boys.
The Current Study
A close examination of these studies plus careful attention to the theoretical groundwork described above suggests clear directions for the current study. First, developmental and psychopathology theory clearly emphasize that social support and stress make prospective, if not causal, contributions to various health-related outcomes (Beck, 1967; Cohen & Wills, 1985; Cole, 1991). Consequently, we addressed these issues in the context of a longitudinal study (noting, of course, that any discovery of prospective effects supports predictive but not necessarily causal relations). Second, cognitive developmental theories of depression (Beck, 1967; Cole, 1991) and appraisal theory (Blascovich & Mendes, 2000; Carver & Scheier, 1981) both imply that children’s awareness of supportive parenting is partially responsible for the inhibitory effect on children’s affective and cognitive outcomes; consequently, we assessed perceived not enacted supportive parenting (that is, positive parental reinforcement of child behavior, parental assistance in child tasks, esteem-supporting communications from parent to child, time spent in positive or shared activities, and child-focused positive conversation; Bruce et al., 2006; Hazzard, Christensen, & Margolin, 1983). Third, peer victimization is a complex collection of behaviors ranging from those intended to damage reputational or social status to those intended to inflict physical harm (e.g., Prinstein & Cillessen, 2003). As these types are highly correlated (r = .82 in Cole et al.’s [2010] multitrait–multimethod analysis; see also Prinstein, Boergers, & Vernberg, 2001), we defined peer victimization to include diverse types of peer victimization (Ladd & Kochenderfer-Ladd, 2002). Fourth, because Cohen and Wills’ (1985) models as well as prior research (Bruce et al., 2006; Lewinsohn et al., 1994; Mezulis et al., 2006; Rapee, 1997) suggest that supportive parenting has both cognitive and affective consequences, we elected to measure not only depressive symptoms but the positive and negative self-cognitions as well. Fifth, in light of some evidence of gender differences in prior studies, we opted to test for gender as a moderator of both supportive parenting and peer victimization. Finally, we focused on elementary and middle school students, as the rates of peer victimization are especially high during late middle childhood and early adolescence (Nansel et al., 2001; Turner, Finkelhor, Hamby, Shattuck, & Ormrod, 2011).
We had four goals: three primary and one secondary. The first was to examine the longitudinal relations of supportive parenting and peer victimization to depressive symptoms and related cognitions as a test of Cohen and Wills’ (1985) main effect model. The second was to examine the interaction between supportive parenting and peer victimization as a test of Cohen and Wills’ stress-buffering hypothesis. Third, we examined the moderating effects of age and gender to help resolve the conflicting results of previous research. Fourth, our secondary goal derived from the fact that our longitudinal design enabled us to put these relations in a broader context—one with other prospective relations, a few of which are anticipated by limited research. For example, depressive symptoms could predict later victimization as suggested by Tran et al. (2012) or later parental support (Branje, Hale, Frijns, & Meeus, 2010).
Method
Participants
We recruited students from five public elementary and four public middle schools in middle Tennessee. Data were collected at three time points, each 6 months apart. At the beginning of the study, students were in the spring semester of Grades 3–6 (ages 8–14). Of 2,999 recruits, a total of 1,888 students obtained parental consent, provided child assent, and actually participated in at least one wave of the study. At Waves 2 and 3, we rerecruited from the same schools and classrooms, thus losing some students (largely due to their moving out of the school district or matriculating into a nonparticipating middle school) and adding new students (largely due to their moving into the school district or matriculating from a nonparticipating elementary school). We started with 1,310 participants at Wave 1. At Wave 2, we lost 290 (22.1%) due to attrition and gained 285 (21.7%) due to rerecruiting, yielding a Wave 2 sample size of 1,305. At Wave 3, we lost 310 (23.8%) and added 293 (22.5%), yielding a Wave 3 sample size of 1,288. Our data analytic strategy required two adjacent waves of data per analysis, either Waves 1 and 2 or Waves 2 and 3, thereby avoiding the impact of the larger Wave 1 to Wave 3 attrition rate. In both sets of analyses, we used full information maximum likelihood estimation methods in order to avoid data loss due to list-wise deletion. Consequently, our Ns were 1,595 for the Wave 1–2 analyses and 1,598 for the Wave 2–3 analyses.
This procedure yielded two primary patterns of missing data for each set of analyses: dropouts, those who left the study between the two waves, and joiners, those who were added to the study between the two waves. Comparisons of dropouts, joiners, and participants with complete data revealed no significant differences on age, gender, ethnicity, or other study variables (ps > .20). Participants’ ages ranged from 8 to 14 years (M = 10.70, SD = 1.08). The sample was 54.3% female and ethnically diverse: 56.2% Caucasian, 30.7% African American, 7.6% Hispanic, 5.2% Asian American, 1.8% Native American, and 5.2% other (note that percentages do not sum to 100%, because ethnic categories were not mutually exclusive). As these were public, urban schools, socioeconomic status was low, with 33%–86% (M = 58%) of participants qualifying for free or reduced lunch programs because of financial need. On average, families had 2.8 children living at home (with a range from 1 to 9).
Measures
Peer victimization
To offset problems associated with mono-methodism, we assessed peer victimization using both self-report and peer-nomination measures (De Los Reyes & Prinstein, 2004). Our self-report measure contained six items designed to assess relational and physical victimization, expanding on items used by Ladd and Kochenderfer-Ladd (2002) to reflect a broader range of victimization. For all items, the stem was, “Does anyone in your class ever ….” The three relational items were (1) “Tell others to stop being your friend,” (2) “Say you can’t play with them,” and (3) “Say mean things to others kids about you.” The three physical items were (4) “Kick you,” (5) “Hit you,” and (6) “Push you.” Items were rated on 4-point scales (1 = never, 2 = rarely, 3 = sometimes, 4 = a lot) and summed to form a composite. In a sample of elementary and middle school students, multitrait–multimethod analyses reveal strong evidence of convergent validity with peer nomination and parent-report measures of victimization (Cole et al., 2010). Previous studies have shown the scales to have acceptable internal consistency, with Cronbach’s alphas of 0.77 and 0.86 for relational and physical victimization, respectively (Tran et al. 2012). In the current study, alphas ranged from 0.80 to 0.82 across the three waves.2
Our peer nomination method was modeled after those used in studies of children’s social status (e.g., Coie, Dodge, & Coppotelli, 1982). Each participant received a randomly sorted list of the other consented students in the targeted classrooms. Separate forms were used to obtain peer nominations of relational and physical victimization. For physical victimization, the instructions were as follows: “Some kids get picked on or hurt by other kids at school. They might get pushed around. They might get bullied by others. They might even get beaten up. Who gets treated like this? Who gets pushed around or bullied by others?” For relational victimization, we asked: “Some kids get picked on by other kids at school in different ways. They might get ignored, talked about or made fun of. Other kids may say or do mean things behind their backs. They may even be left out or kicked out of groups. From the list below, circle the names of the kids who get treated like this.” Instructions asked respondents to mark the names of all classmates who fit a particular question. Scores for each student were the proportions of participating classmates who indicated that the student was physically or relationally victimized.
In 9- to 14-year-old children, the measure has shown good evidence of convergent validity with self-report and parent-report measures of peer victimization (Cole et al., 2010).
Supportive parenting
The Parent Perception Inventory-Child version (PPIC; Bruce et al., 2006) is a 36-item questionnaire that assesses how children view their mothers, fathers, or primary caregivers and the role they play in the children’s lives. The PPIC was originally based on the Hazzard et al. (1983) Parent Perception Interview. The original interview inquired about children’s perceptions of 18 parental behaviors (nine positive and nine negative). Bruce et al. (2006) converted these 18 behaviors into a 36-item questionnaire by generating two items designed to measure each of the 18 behaviors. Children rate on 5-point scales (1 = not at all to 5 = all the time) how often the parent engages in a variety of supportive and harsh parenting behaviors. In a sample of 7- to 13-year-olds, factor analysis revealed a strong two-factor solution, reflecting warm/supportive parenting and harsh/critical parenting (Bruce et al., 2006), both of which showed significant convergent validity with subscales of a parent-report measure of similar behaviors (Lovejoy, Weis, O’Hare, & Rubin, 1999). Given that supportive parenting was the focus of this study, we used only the warm/supportive parenting subscale, with items reflecting levels of physical affection/warmth and emotional support. Items begin with the stem “How often does this person … .” The warm/supportive items are as follows: “… . tell you they like what you did,” “… . talk to you when you feel bad to help you feel better,” “… . have a good talk with you,” “… . spend time with you,” “… . say nice things to you,” “… . help you with your homework,” “… . hug you,” “… . pay attention to you,” “… . give you something or let you do something special when you’re good,” “… . help you with a problem,” “… . ask about your day,” “… . ask ‘What should we do today,’ ” “… . do things with you that you like to do,” “… . say something nice about you,” “… . let you do things on your own,” “… . help you with a hard job when you need it,” “… . smile at you,” and “… . listen to you?” In the current study, Cronbach’s alphas ranged from 0.81 to 0.83 across the three waves.
Depression
The Children’s Depression Inventory (CDI; Kovacs, 1981) is a 27-item self-report measure that assesses symptoms of depression in children. Each item consists of three statements in order of increasing severity from 0 to 2. Children select the one sentence from each group that best describes themselves for the past 2 weeks (e.g., “I am sad once in a while,” “I am sad many times,” or “I am sad all the time”). The CDI has high levels of reliability and validity, especially in nonclinical samples of elementary, middle, and junior high school students (e.g., Craighead, Smucker, Craighead, & Ilardi, 1998). In the current study, Cronbach’s alphas ranged from 0.89 to 0.91 over the three waves.
Self-cognition measures
The Cognitive Triad Inventory for Children (CTI-C; Kaslow, Stark, Printz, Livingston, & Tsai, 1992) is a 36-item self-report questionnaire assessing children’s views of themselves (e.g., “I am a failure”), their world (e.g., “The world is a very mean place”), and their future (e.g., “Nothing is likely to work out for me”). Children indicate whether they have had specific thoughts by marking yes, maybe, or no (scored 0, 1, or 2) such that higher scores indicate stronger negative cognitions. Despite the word “triad” in the title, recent factor analysis of the measure reveals that a two-factor solution emerges over the course of middle childhood (LaGrange et al., 2008). One is a positive cognition factor; the other is a negative cognition factor. In non-clinic samples of elementary and middle school students, the scales have high internal consistency and good construct validity, correlating with measures of self-perception, self-worth, self-control, perceived contingency, and attributional style (Kaslow et al., 1992; LaGrange et al., 2008). In the current study, Cronbach’s alphas for the positive CTI-C ranges from 0.87 to 0.90, and alphas for the negative CTI-C scales ranged from 0.88 to 0.89 across the three waves.
The Children’s Automatic Thoughts Scale (CATS; Schniering & Rapee, 2002) is a self-report questionnaire that assesses negative self-cognitions in young people. The questionnaire asks children to rate the frequency with which they have had 56 different negative thoughts in the previous week. Participants respond on 5-point scales (1 = not at all to 5 = all the time). The CATS has four subscales: Physical Threat (e.g., “I’m going to get hurt”), Social Threat (e.g., “I’m afraid I will make a fool of myself”), Personal Failure (e.g., “It’s my fault that things have gone wrong”), and Hostility (e.g., “I won’t let anyone get away with picking on me”). In both clinical and nonclinical 7 to 16 year olds, the CATS has good test–retest reliability: 0.79 at 1 month and 0.76 at 3 months (Schniering & Rapee, 2002) and has been used in test development and validation efforts. For the purpose of this study, we used the two subscales most relevant to peer victimization: Social Threat (αs ranged from 0.87 to 0.89) and Personal Failure (α = .90 for all waves).
Harter’s (1985) Self-Perception Profile for Children (SPPC) is a self-report inventory with 36 items reflecting developmentally appropriate domains of self-concept (i.e., scholastic competence, social acceptance, behavioral conduct, physical appearance, and sports competence) plus a global self-worth scale. For each item, children select one of two statements to indicate whether they are more like a child who is good or a child who is not so good at a particular activity. Then they select statements indicating whether the selected statement is “sort of true” or “really true” about them. Responses are converted to 4-point rating scales with high scores reflecting better self-perceptions. The SPPC has a highly interpretable factor structure, and all subscales have good internal consistency (Harter, 1982, 1985). In the current study, Cronbach’s alphas ranged from 0.78 to 0.84 for the social acceptance subscale, 0.83 to 0.85 for the physical appearance subscale, and 0.81 to 0.85 for the global self-worth subscale.
Procedures
Prior to Time 1 data collection, we distributed consent documents to 3rd, 4th, 5th, and 6th grade classrooms. We offered a $100 donation to each classroom if 90% of children in a classroom returned a consent form signed by a parent or guardian, either granting or denying permission for the child’s participation. Students returned signed consent forms to classroom teachers in sealed envelopes that were collected later by research assistants. During regular school hours, psychology graduate assistants and undergraduate research assistants gathered consented students into small groups and administered the questionnaires by reading each question out loud and asking participants to follow along and fill in their answers on their own questionnaire form. At the end of the questionnaires, participants were given a snack and a decorative pencil for their participation. We repeated the entire procedure every 6 months for Waves 2 and 3, respectively.
Results
Preliminary Analyses
For the three waves of the study, correlations among all study variables, as well as their descriptive statistics, are presented in Table 1. Within each wave, victimization and supportive parenting were significantly correlated with every cognitive and depression measure in the expected directions. Means and standard deviations were similar to those reported in other studies of nonreferred, school-based samples (e.g., LaGrange et al., 2008; Muris, Meesters, & Fijen, 2003). Approximately 10% of the sample had CDI scores >19 (a conventional cutoff for severe depression), and 20% of the sample exceeded a cutoff of 12 for moderate depression (Kazdin, Colbus, & Rodgers, 1986; Kendall, Cantwell, & Kazdin, 1989). Peer victimization estimates revealed that 11.5% to 13.6% of participants reported experiencing “a lot” of at least one type of peer victimization in any given year. As students were recruited from classrooms, within-classroom statistical dependencies were possible, potentially requiring the nesting of participants within classroom; however, intraclass correlations for all study variables were small (intraclass correlation coefficients ranged from 0.00 to 0.04), obviating the need for nesting. As anticipated by De Los Reyes and Prinstein (2004), cross-informant correlations between peer nomination and self-report measures of peer victimization were moderate (rs = 0.34 to 0.43); see also De Los Reyes and Kazdin (2005).
Table 1.
Correlations Broken Down by Wave
| Measures
|
||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | |
| Wave 1 | ||||||||||||
| 1. Age | 1.00 | |||||||||||
| 2. PV-SR | −0.15** | 1.00 | ||||||||||
| 3. PV-PN | −0.13** | 0.34** | 1.00 | |||||||||
| 4. CDI | −0.04 | 0.50** | 0.26** | 1.00 | ||||||||
| 5. CTI-N | −0.05 | 0.48** | 0.25** | 0.76** | 1.00 | |||||||
| 6. CTI-P | 0.01 | 0.42** | 0.23** | 0.72** | 0.64** | 1.00 | ||||||
| 7. CATS-PF | −0.10** | 0.48** | 0.23** | 0.67** | 0.69** | 0.58** | 1.00 | |||||
| 8. CATS-S | −0.11** | 0.62** | 0.29** | 0.60** | 0.56** | 0.52** | 0.73** | 1.00 | ||||
| 9. SPPC-S | 0.12** | −0.43** | −0.30** | −0.51** | −0.45** | −0.49** | −0.43** | −0.51** | 1.00 | |||
| 10. SPPC-G | 0.01 | −0.39** | −0.23** | −0.68** | −0.65** | −0.62** | −0.68** | −0.56** | 0.50** | 1.00 | ||
| 11. SPPC-A | −0.11** | −0.31** | −0.14** | −0.55** | −0.47** | −0.48** | −0.46** | −0.51** | 0.46** | 0.64** | 1.00 | |
| 12. PPIC | −0.09** | −0.16** | −0.10** | −0.48** | −0.46** | −0.52** | −0.32** | −0.21** | 0.30** | 0.42** | 0.30** | 1.00 |
| M | 10.69 | 19.35 | 0.24 | 7.86 | 25.18 | 21.88 | 14.12 | 15.69 | 12.65 | 14.71 | 12.71 | 75.56 |
| SD | 1.08 | 6.82 | 0.32 | 7.89 | 6.40 | 5.06 | 6.54 | 7.69 | 4.57 | 3.92 | 4.90 | 14.19 |
| Wave 2 | ||||||||||||
| 1. Age | 1.00 | |||||||||||
| 2. PV-SR | −0.16** | 1.00 | ||||||||||
| 3. PV-PN | −0.08** | 0.36** | 1.00 | |||||||||
| 4. CDI | −0.03 | 0.48** | 0.20** | 1.00 | ||||||||
| 5. CTI-N | −0.02 | 0.40** | 0.19** | 0.78** | 1.00 | |||||||
| 6. CTI-P | 0.02 | 0.42** | 0.15** | 0.77** | 0.68** | 1.00 | ||||||
| 7. CATS-P | −0.06 | 0.48** | 0.19** | 0.74** | 0.68** | 0.64** | 1.00 | |||||
| 8. CATS-S | −0.05 | 0.63** | 0.27** | 0.65** | 0.54** | 0.54** | 0.72** | 1.00 | ||||
| 9. SPPC-S | 0.06* | −0.44** | −0.31** | −0.58** | −0.50** | −0.53** | −0.52** | −0.57** | 1.00 | |||
| 10. SPPC-G | −0.02 | −0.42** | −0.19** | −0.73** | −0.67** | −0.72** | −0.69** | −0.60** | 0.60** | 1.00 | ||
| 11. SPPC-A | −0.09** | −0.34** | −0.14** | −0.61** | −0.48** | −0.54** | −0.54** | −0.53** | 0.53** | 0.67** | 1.00 | |
| 12. PPIC | −0.13** | −0.16** | −0.09** | −0.48** | −0.47** | −0.52** | −0.31** | −0.24** | 0.33** | 0.45** | 0.35** | 1.00 |
| M | 11.24 | 18.07 | 0.18 | 7.12 | 24.72 | 21.28 | 13.67 | 15.12 | 13.28 | 14.82 | 12.95 | 76.92 |
| SD | 1.10 | 6.20 | 0.29 | 7.46 | 6.38 | 5.06 | 6.24 | 7.65 | 4.34 | 4.08 | 4.88 | 13.38 |
| Wave 3 | ||||||||||||
| 1. Age | 1.00 | |||||||||||
| 2. PV-SR | −0.11** | 1.00 | ||||||||||
| 3. PV-PN | −0.11** | 0.43** | 1.00 | |||||||||
| 4. CDI | −0.03 | 0.51** | 0.22** | 1.00 | ||||||||
| 5. CTI-N | 0.00 | 0.45** | 0.23** | 0.77** | 1.00 | |||||||
| 6. CTI-P | 0.00 | 0.41** | 0.15** | 0.73** | 0.65** | 1.00 | ||||||
| 7. CATS-P | −0.03 | 0.45** | 0.16** | 0.74** | 0.69** | 0.65** | 1.00 | |||||
| 8. CATS-S | −0.04 | 0.63** | 0.24** | 0.64** | 0.56** | 0.51** | 0.67** | 1.00 | ||||
| 9. SPPC-S | 0.10** | −0.50** | −0.34** | −0.57** | −0.48** | −0.51** | −0.46** | −0.53** | 1.00 | |||
| 10. SPPC-G | −0.03 | −0.37** | −0.16** | −0.70** | −0.63** | −0.65** | −0.62** | −0.55** | 0.55** | 1.00 | ||
| 11. SPPC-A | −0.08* | −0.32** | −0.15** | −0.58** | −0.50** | −0.49** | −0.47** | −0.50** | 0.46** | 0.68** | 1.00 | |
| 12. PPIC | −0.09** | −0.21** | −0.10** | −0.43** | −0.42** | −0.48** | −0.33** | −0.25** | 0.28** | 0.37** | 0.29** | 1.00 |
| M | 11.78 | 17.49 | 0.17 | 6.66 | 24.26 | 21.12 | 13.37 | 15.15 | 13.38 | 15.01 | 13.01 | 77.24 |
| SD | 1.08 | 6.27 | 0.28 | 7.46 | 6.29 | 5.14 | 6.08 | 7.82 | 4.61 | 3.98 | 4.87 | 14.20 |
Note. The SPPC is scaled in the opposite direction of the CATS and CTI. PV-SR = Peer Victimization Self-Report; PV-PN = Peer Victimization Peer-Nominated; CATS = Children’s Automatic Thoughts Scale (PF = Personal Failure, S = Social Threat); CTI = Cognitive Triad Inventory for Children (N = Negative, Ps = Positive); SPPC = Self-Perception Profile for Children (A = Appearance; G = Global; S = Social).
p < .05.
p < .01.
Analysis Overview
We performed a series of multiple linear regressions3 to examine the longitudinal effects of supportive parenting and peer victimization on depressive symptoms and depression-related cognitions. In each analysis, a measure of depressive symptoms or cognitions (from Wave 2 or Wave 3) served as the dependent variable. A measure of the dependent variable from the prior wave (Wave 1 or Wave 2, respectively) was entered as a control variable. Predictor variables from the previous wave were age, gender, supportive parenting, and peer victimization. We also tested all interactions among the predictors. Higher-order effects were tested while controlling for all lower-order effects. Age and all of the control variables were centered at their means and gender was coded males = −1 and females = 1. We conducted all analyses twice, once using the peer nomination measure of peer victimization and then using the self-report measure.
Regressions Using Peer Nominations to Measure Peer Victimization
Tests of interactions
Very few higher-order interactions were statistically significant, even using an uncorrected alpha level of .05. Across eight dependent variables, 88 interactions were tested, and only six were significant. None of the significant interactions from the Wave 1–2 analyses replicated in the Wave 2–3 analyses. Even a relatively liberal family-wise control for multiple analyses (α = .05/8) eliminated all of these interactions. Perhaps most importantly, none of the six significant interactions involved the Supportive Parenting × Victimization effect that is critical to the stress-buffering hypothesis.
Tests of main effects
Attributing the relatively few and inconsistent interactions to chance, we conducted main effects tests ignoring all higher-order interactions. As shown in Table 2, supportive parenting had a main effect on six of eight of the dependent variables: CDI, CTI-Negative, CTI-Positive, CATS-Social Threat, SPPC-Global Self-worth, and SPPC-Social Acceptance. All but one of these effects replicated from the Wave 1–2 analyses to the Wave 2–3 analyses. The main effect of supportive parenting on SPPC-Social Acceptance did not replicate, and the effect of supportive parenting on CATS-Personal Failure was not significant at either wave. Sizes of the significant effects (Cohen’s f2s) ranged from .02 to .068 (see Table 2). The direction of the significant effects was quite consistent, with supportive parenting predicting lower levels of depressive symptoms, lower levels of negative self-cognition, and higher levels of positive self-cognition over time.
Table 2.
Regression Results Using a Peer Nomination (PN) Measure of Peer Victimization (Cohen’s f2 reported for significant peer nomination or peer victimization effects)
| Predictor | Wave 1 → Wave 2
|
Wave 2 → Wave 3
|
||||||
|---|---|---|---|---|---|---|---|---|
| B | SE(B) | Beta | f2 | B | SE(B) | Beta | f2 | |
| DV = CDI | ||||||||
| Intercept | 10.05*** | 2.07 | 11.11*** | 1.52 | ||||
| prior CDI | 0.41*** | 0.05 | 0.45 | 0.67*** | 0.04 | 0.66 | ||
| Gender | 0.48 | 0.33 | 0.07 | 0.13 | 0.24 | 0.02 | ||
| Age | −0.27 | 0.28 | −0.05 | −0.11 | 0.22 | −0.02 | ||
| Peer Victimization (PN) | 2.44* | 1.21 | 0.10 | 0.018 | 0.83 | 0.89 | 0.03 | — |
| Supportive Parenting | −0.06* | 0.03 | −0.12 | 0.022 | −0.07*** | 0.02 | −0.12 | 0.050 |
|
| ||||||||
| DV = CTI-Negative | ||||||||
| Intercept | 27.45*** | 1.62 | 26.36*** | 1.29 | ||||
| prior CTI-Negative | 0.39*** | 0.05 | 0.45 | 0.59*** | 0.04 | 0.63 | ||
| Gender | 0.07 | 0.26 | 0.01 | 0.25 | 0.20 | 0.04 | ||
| Age | −0.22 | 0.22 | −0.05 | 0.12 | 0.18 | 0.02 | ||
| Peer Victimization (PN) | 2.52** | 0.95 | 0.13 | 0.030 | 1.86** | 0.75 | 0.09 | 0.026 |
| Supportive Parenting | −0.06** | 0.02 | −0.15 | 0.034 | −0.04** | 0.02 | −0.10 | 0.025 |
|
| ||||||||
| DV = CTI-Positive | ||||||||
| Intercept | 25.75*** | 1.63 | 27.65*** | 1.28 | ||||
| prior CTI-Positive | 0.42*** | 0.06 | 0.43 | 0.52*** | 0.04 | 0.51 | ||
| Gender | −0.02 | 0.25 | −0.01 | 0.39* | 0.20 | 0.07 | ||
| Age | −0.21 | 0.21 | −0.05 | −0.17 | 0.18 | −0.04 | ||
| Peer Victimization (PN) | 1.26 | 0.93 | 0.07 | — | 1.18 | 0.74 | 0.06 | — |
| Supportive Parenting | −0.05** | 0.02 | −0.14 | 0.025 | −0.07*** | 0.02 | −0.18 | 0.068 |
|
| ||||||||
| DV = CATS-Personal Failure (PF) | ||||||||
| Intercept | 14.15*** | 1.55 | 14.32*** | 1.27 | ||||
| prior CATS-PF | 0.30*** | 0.05 | 0.34 | 0.57*** | 0.04 | 0.60 | ||
| Gender | 0.44 | 0.26 | 0.09 | 0.69*** | 0.21 | 0.12 | ||
| Age | −0.02 | 0.22 | −0.01 | 0.33 | 0.19 | 0.06 | ||
| Peer Victimization (PN) | 4.13*** | 0.95 | 0.22 | 0.071 | 1.66* | 0.75 | 0.08 | 0.018 |
| Supportive Parenting | −0.03 | 0.02 | −0.09 | — | −0.02 | 0.02 | −0.06 | — |
|
| ||||||||
| DV = CATS-Social Threat (ST) | ||||||||
| Intercept | 18.74*** | 2.15 | 19.04*** | 1.49 | ||||
| prior CATS-ST | 0.29*** | 0.05 | 0.30 | 0.66*** | 0.04 | 0.65 | ||
| Gender | 0.82* | 0.37 | 0.11 | 0.80*** | 0.25 | 0.11 | ||
| Age | 0.04 | 0.32 | 0.01 | 0.21 | 0.22 | 0.03 | ||
| Peer Victimization (PN) | 2.29 | 1.41 | 0.09 | — | 0.74 | 0.93 | 0.03 | — |
| Supportive Parenting | −0.06* | 0.03 | −0.13 | 0.020 | −0.06** | 0.02 | −0.11 | 0.042 |
|
| ||||||||
| DV = SPPC: Social Acceptance (SA) | ||||||||
| Intercept | 12.61*** | 1.14 | 10.32*** | 0.99 | ||||
| prior SPPC-SA | 0.57*** | 0.05 | 0.60 | 0.57*** | 0.04 | 0.55 | ||
| Gender | 0.00 | 0.19 | 0.00 | −0.18 | 0.16 | −0.04 | ||
| Age | −0.11 | 0.16 | −0.03 | 0.27 | 0.15 | 0.06 | ||
| Peer Victimization (PN) | −0.41 | 0.67 | −0.03 | — | −1.71** | 0.61 | −0.10 | 0.030 |
| Supportive Parenting | 0.02 | 0.01 | 0.06 | — | 0.05*** | 0.01 | 0.14 | 0.053 |
|
| ||||||||
| DV = SPPC: Physical Appearance (PA) | ||||||||
| Intercept | 11.01*** | 1.39 | 11.40*** | 1.03 | ||||
| prior SPPC-PA | 0.50*** | 0.05 | .502 | 0.63*** | 0.04 | 0.65 | ||
| Gender | −0.66** | 0.24 | −.132 | −0.45** | 0.17 | −0.09 | ||
| Age | −.04 | 0.20 | −.009 | −0.16 | 0.16 | −0.04 | ||
| Peer Victimization (PN) | .69 | 0.84 | .040 | — | 0.60 | 0.60 | 0.03 | — |
| Supportive Parenting | .03 | 0.02 | .082 | — | 0.03* | 0.01 | 0.07 | 0.020 |
|
| ||||||||
| DV = SPPC: Global Self-worth (GS) | ||||||||
| Intercept | 13.15*** | 1.13 | 13.43*** | 0.89 | ||||
| prior SPPC-GS | 0.40*** | 0.06 | 0.40 | 0.55*** | 0.04 | 0.58 | ||
| Gender | −0.43** | 0.18 | −0.12 | −0.32* | 0.14 | −0.08 | ||
| Age | −0.04 | 0.15 | −0.01 | −0.02 | 0.13 | −0.01 | ||
| Peer Victimization (PN) | −1.02 | 0.65 | −0.08 | — | 0.27 | 0.50 | 0.02 | — |
| Supportive Parenting | 0.03* | 0.01 | 0.13 | 0.021 | 0.03* | 0.01 | 0.09 | 0.020 |
Note. CDI = Children’s Depression Inventory; CATS = Children’s Automatic Thoughts Scale; CTI = Cognitive Triad Inventory for Children; SPPC = Self-Perception Profile for Children. The SPPC is scaled in the opposite direction of the CATS and CTI.
p < .05.
p < .01.
p < .001.
Also shown in Table 2, the main effect of peer victimization (by peer nomination) was significant for four of eight dependent variables (i.e., CDI, CTI-Negative, CATS-Personal Failure, and SPPC-Social Acceptance); however, only the effects on CTI-Negative and CATS-Personal Failure replicated from the Wave 1–2 analyses to the Wave 2–3 analyses. Sizes of the significant effects ranged from f2 = .018 to .071 (see Table 2). The significant effects supported a consistent interpretation: being nominated by classmates as a person who is frequently victimized by peers predicted higher levels of depression, higher levels of negative self-cognition, and lower levels of positive self-cognition.
Regressions Using Child Self-Reports to Measure Peer Victimization
Tests of interactions
Only six of 88 interactions were statistically significant, using an alpha level of .05. The pattern of results was inconsistent, and none of the effects replicated from the Wave 1–2 analyses to the Wave 2–3 analyses. Any control of family-wise alpha (e.g., α = .05/8) eliminated all of these interactions. None of the six significant interactions involved the Supportive Parenting × Victimization effect.
Tests of main effects
We conducted main effects tests ignoring all higher-order interactions. As shown in Table 3, supportive parenting had a main effect on seven of eight of the dependent variables: CDI, CTI-Negative, CTI-Positive, CATS-Personal Failure, CATS-Social Threat, SPPC-Social Acceptance, and SPPC-Global Self-worth. Five of seven of these effects replicated from the Wave 1–2 analyses to the Wave 2–3 analyses. The main effects of supportive parenting on CATS-Personal Failure and SPPC-Social Acceptance did not. Sizes of the significant effects ranged from f2 = .018 to .089 (see Table 3). The significant effects reflected the conclusion that supportive parenting predicted lower levels of depressive symptoms, lower levels of negative self-cognition, and higher levels of positive self-cognition over time.
Table 3.
Regression Results Using a Self-Report Measure of Peer Victimization (Cohen’s f2 Reported for Significant Peer Nomination or Peer Victimization Effects)
| Predictor | Wave 1 → Wave 2
|
Wave 2 → Wave 3
|
||||||
|---|---|---|---|---|---|---|---|---|
| B | SE(B) | Beta | f2 | B | SE(B) | Beta | f2 | |
| DV = CDI | ||||||||
| Intercept | 9.56*** | 2.30 | 9.39*** | 1.60 | ||||
| Prior CDI | 0.43*** | 0.05 | 0.46 | 0.61*** | 0.04 | 0.60 | ||
| Gender | 0.52 | 0.33 | 0.07 | 0.16 | 0.23 | 0.02 | ||
| Age | −0.35 | 0.28 | −0.06 | 0.04 | 0.21 | 0.01 | ||
| PV-SR | 0.06 | 0.06 | 0.05 | — | 0.14*** | 0.04 | 0.12 | 0.050 |
| Supportive parenting | −0.06* | 0.03 | −0.12 | 0.023 | −0.08*** | 0.02 | −0.14 | 0.072 |
| DV = CTI-N | ||||||||
| Intercept | 26.30*** | 1.80 | 24.54*** | 1.47 | ||||
| Prior CTI-N | 0.38*** | 0.05 | 0.44 | 0.54*** | 0.04 | 0.56 | ||
| Gender | 0.01 | 0.26 | 0.00 | 0.03 | 0.21 | 0.01 | ||
| Age | −0.20 | 0.22 | −0.04 | 0.17 | 0.19 | 0.03 | ||
| PV-SR | 0.08* | 0.04 | 0.10 | 0.017 | 0.15*** | 0.04 | 0.15 | 0.062 |
| Supportive parenting | −0.06** | 0.02 | −0.14 | 0.034 | −0.05** | 0.02 | −0.11 | 0.032 |
| DV = CTI-Ps | ||||||||
| Intercept | 25.20*** | 1.77 | 26.97*** | 1.37 | ||||
| Prior CTI-Ps | 0.42*** | 0.06 | 0.43 | 0.48*** | 0.04 | 0.47 | ||
| Gender | −0.05 | 0.25 | −0.01 | 0.36 | 0.19 | 0.07 | ||
| Age | −0.21 | 0.21 | −0.05 | −0.08 | 0.18 | −0.02 | ||
| PV-PN | 0.05 | 0.04 | 0.07 | — | 0.09** | 0.04 | 0.10 | 0.022 |
| Supportive parenting | −0.05** | 0.02 | −0.14 | 0.028 | −0.08*** | .02 | −0.21 | 0.089 |
| DV = CATS-PF | ||||||||
| Intercept | 12.02*** | 1.80 | 13.18*** | 1.43 | ||||
| Prior CATS-PF | 0.29*** | 0.05 | 0.33 | 0.53*** | 0.04 | 0.54 | ||
| Gender | 0.33 | 0.26 | 0.06 | 0.59** | 0.21 | 0.10 | ||
| Age | −0.01 | 0.22 | −0.00 | 0.37* | 0.19 | 0.07 | ||
| PV-SR | 0.17*** | 0.04 | 0.21 | 0.062 | 0.13*** | 0.04 | 0.13 | 0.034 |
| Supportive parenting | −0.03 | 0.02 | −0.09 | — | −0.03* | 0.02 | −0.08 | — |
| DV = CATS-S | ||||||||
| Intercept | 15.52*** | 2.56 | 14.77*** | 1.70 | ||||
| Prior CATS-S | 0.24*** | 0.06 | 0.25 | 0.53*** | 0.04 | 0.52 | ||
| Gender | 0.80* | 0.37 | 0.11 | 0.85*** | 0.24 | 0.11 | ||
| Age | 0.05 | 0.32 | 0.01 | 0.38 | 0.23 | 0.06 | ||
| PV-SR | 0.19** | 0.07 | 0.17 | 0.028 | 0.25*** | 0.05 | 0.20 | 0.093 |
| Supportive parenting | −0.06* | 0.03 | −0.12 | 0.018 | −0.06*** | 0.02 | −0.11 | 0.042 |
| DV = SPPC-SA | ||||||||
| Intercept | 13.24*** | 1.28 | 11.10*** | 1.10 | ||||
| Prior SPPC-SA | 0.56*** | 0.05 | 0.59 | 0.56*** | 0.04 | 0.54 | ||
| Gender | 0.04 | 0.19 | 0.01 | −0.15 | 0.16 | −0.03 | ||
| Age | −0.12 | 0.16 | −.04 | 0.19 | 0.15 | 0.04 | ||
| PV-SR | −0.03 | 0.03 | −0.05 | — | −0.08** | 0.03 | −0.10 | 0.024 |
| Supportive parenting | 0.02 | 0.01 | 0.05 | — | 0.05*** | 0.01 | 0.15 | 0.059 |
| DV = SPPC-PA | ||||||||
| Intercept | 11.87*** | 1.60 | 11.70*** | 1.15 | ||||
| Prior SPPC-PA | 0.49*** | 0.05 | 0.48 | 0.62*** | 0.04 | 0.65 | ||
| Gender | −0.68** | 0.24 | −0.14 | −0.46** | 0.17 | −0.09 | ||
| Age | −0.08 | 0.20 | −0.02 | −0.19 | 0.16 | −0.04 | ||
| PV-PN | −0.04 | 0.04 | −0.06 | — | −0.01 | 0.03 | −0.01 | — |
| Supportive parenting | 0.03 | 0.02 | 0.08 | — | 0.02 | 0.01 | 0.07 | — |
| DV = SPPC-GS | ||||||||
| Intercept | 13.88*** | 1.28 | 14.03*** | 0.96 | ||||
| Prior SPPC-GS | 0.41*** | 0.06 | 0.41 | 0.52*** | 0.04 | 0.55 | ||
| Gender | −0.43** | 0.18 | −0.12 | −0.31* | 0.14 | −0.08 | ||
| Age | −0.04 | 0.16 | −0.01 | −0.07 | 0.13 | −0.02 | ||
| PV-SR | −0.04 | 0.03 | −0.07 | — | −0.04 | 0.03 | −0.07 | — |
| Supportive parenting | 0.03* | 0.01 | 0.12 | 0.018 | 0.03** | 0.01 | 0.10 | 0.022 |
Note. The SPPC is scaled in the opposite direction of the CATS and CTI. PV-SR = Peer Victimization Self-Report; CTI = Cognitive Triad Inventory for Children (N = Negative, Ps = Positive); CDI = Children’s Depression Inventory; PV-PN = Peer Victimization Peer-nominated; CATS = Children’s Automatic Thoughts Scale (PF = Personal Failure, S = Social Threat); SPPC = Self-Perception Profile for Children (PA = Personal Appearance; G = Global; SA = Social Acceptance); DV = Dependent Variable.
p < .05.
p < .01.
p < .001.
Table 3 also revealed that the main effect of peer victimization (by self-report) was significant on six of eight dependent variables: the CDI, CTI-Negative, CTI-Positive, CATS-Personal Failure, CATS-Social Threat, and SPPC-Social Acceptance. Only three of these effects replicated from the Wave 1–2 analyses to the Wave 2–3 analyses: CTI-Negative, CATS-Personal Failure, and CATS-Personal Failure. Sizes of the significant effects ranged from f2 = .017 to .093 (see Table 3). Replicated significant effects revealed that higher levels of self-reported peer victimization predicted higher levels of negative self-cognition. Nonreplicated significant effects suggested that higher levels of peer victimization predicted higher levels of depressive symptoms and lower levels of positive self-cognition.
Cross-Lag Panel Analyses
Finally, we used path analysis to conduct four two-wave cross-lag panel analyses: Wave 1 → 2 using peer nominations, Wave 2 → 3 using peer nominations, Wave 1 → 2 using self-report, and Wave 2 → 3 using self-report. In each, we regressed wave k measures of supportive parenting, depressive symptoms, and peer victimization onto the same three Wave k − 1 predictors, plus age and gender. The results are depicted in Figures 1 and 2, in which we used boldface font to indicate which standardized path coefficients were significant at p < .05. Three patterns emerged. First, the main effects of supportive parenting and peer victimization were unchanged from the previous analysis. Second, in all four analyses, higher levels of prior depressive symptoms predicted lower levels of supportive parenting, and third, in two out of four analyses, higher levels of prior depressive symptoms also predicted higher levels of peer victimization.
Figure 1.

Two-wave cross-panel analyses (w1 → w2 and w2 → w3) of supportive parenting (Supp. Par.), depressive symptoms (Depress.), and peer nomination measures of peer victimization (Peer Vic.).
Figure 2.

Two-wave cross-panel analyses (w1 → w2 and w2 → w3) of supportive parenting (Supp. Par.), depressive symptoms (Depress.), and self-report measures of peer victimization (Peer Vic.).
Clinical Significance
One way to examine clinical significance is to examine the size of the adverse effect that peer victimization has relative to the size of the ameliorating effect of supportive parenting. Several things are evident from the depiction of these effects in Figure 3: (1) High peer victimization without strong supportive parenting drives the expected CDI scores above 12.0, sometimes regarded as a cutoff for moderate depression; (2) High peer victimization with strong supportive parenting brings CDI scores back down to a level substantially below this same cutoff. Another way to demonstrate clinical significance is to examine change in depression status. In Waves 1 and 2, 10%–11% of high-victimized participants had CDI scores above 19. Among these, the odds of becoming depressed (i.e., changing status from <19 to >19) were 3:1 when the child had low levels of supportive parenting, but improved to 1:3 when the child had high levels of parental support.
Figure 3.
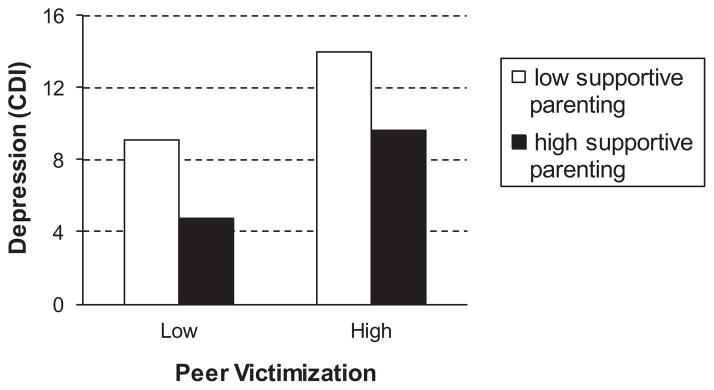
Compensatory effect of high supportive parenting given high peer victimization.
Discussion
Four major results emerged from this longitudinal study on the effects of supportive parenting and peer victimization on depressive thoughts and symptoms in children. First, we found substantial support for Cohen and Wills’ (1985) main effect model: supportive parenting had a main effect on depressive symptoms and cognitions, over-and-above the effect of peer victimization. Second, virtually no evidence of an interaction between supportive parenting and peer victimization emerged, providing no support for Cohen and Wills’ stress-buffering model. Third, support for Cohen and Wills’ main effect model (as applied to supportive parenting and peer victimization) generalized across age and gender. Finally, in addition to evidence that the main effect of supportive parenting offset the main effect of peer victimization on depressive symptoms, we also found some evidence that depressive symptoms predicted peer victimization and strong evidence that depressive symptoms predicted reduced parental support.
Strong Implications Emerge for Intervention, Prevention, and Future Research
Our first major finding was substantial support for an application of Cohen and Wills’ (1985) main effect model to parental support, peer victimization, and depression-related outcomes. The main effect model suggests that social support reduces psychological symptoms regardless of one’s level of stress or adversity. We tested an instantiation of their model that pertains specifically to parental support, adversity-associated peer victimization, and psychological outcomes related to depression in children and adolescents. We found a relatively consistent significant longitudinal main effect for supportive parenting (over-and-above the main effect of peer victimization) on depressive symptoms and depression-related cognitions.
The various main effects of supportive parenting were in the expected directions. Supportive parenting behaviors predicted lower levels of depressive symptoms, lower levels of negative self-cognitions, and higher levels of positive self-cognitions. This finding is consistent with previous research showing that supportive parenting behaviors are associated with fewer depressive symptoms (Allen et al., 2006; Dallaire et al, 2006). More importantly, the current results reinforce the idea that supportive parenting behaviors might protect against the depressive symptoms that can accompany peer victimization. In fact, the magnitudes of the positive results for supportive parenting tended to be as large as or larger than the negative results for peer victimization. Our support for the main effect model not only reflects previous research (Conners-Burrow et al., 2009; Papafratzeskakou et al., 2011; Stadler et al., 2010; Tanigawa et al., 2011), but methodological strengths of the current study advance the field insofar as our study involved a relatively large, three-wave longitudinal design with (1) measures that clearly assessed supportive parenting and depressive symptoms, (2) a model that focused specifically on the Cohen and Wills’ (1985) models, and (3) a statistical approach that did not involve categorization of continuous measures (issues that affect interpretation of previous studies).
This pattern of results implies that supportive parenting can counterbalance the relation of peer victimization to depression. One can liken these results to a bank account. Peer victimization represents the withdrawal of funds. Supportive parenting represents a deposit. Although supportive parenting can replenish the deficit incurred by peer victimization, it does not imply that the deficit never occurred. The downside is that our findings suggest that (on average) victimized children with supportive parents have less in their bank accounts than do nonvictimized children with equally supportive parents. The upside, however, is that supportive parenting may be sufficient to prevent the victimized child from going bankrupt; that is, supportive parenting may counterbalance peer victimization enough to prevent the child from reaching the threshold for depression.
Cohen and Wills (1985) argued that social support could have a positive main effect on health (off-setting the negative effects of stress) for a wide variety of reasons. These reasons include esteem support (i.e., social support communicates that a person is valued by others), informational support (i.e., supportive others help the individual to understand and cope with the stressors), social companionship (i.e., fulfilling a need for social belongingness and/or distracting the individual from the stressors), and instrumental support (i.e., providing material support such as money for the acquisition of related services). Given our focus on children, peer victimization, and depression, and given our use of a relatively generic measure of perceived parental support, we interpret our results as primarily reflective of esteem support. Other kinds of support may have been operating as well, but were not directly assessed in the current study. Esteem support may be especially critical in middle childhood and early adolescence. Garber (1984) suggested that a major developmental task during these years is the construction of self-worth. Cole (1991) and Harter (Harter & Whitesell, 1996) described dynamic processes whereby youths not only receive feedback about their competence in various domains and from various significant others, but they strategically value (or devalue) such feedback and depending on the importance of the domain. Being able to value positive feedback from parents may enable the child to devalue the importance of negative feedback from the class bully.
Our second major finding was a complete lack of support for Cohen and Wills’ (1985) stress-buffering hypothesis. Using different measures and different time lags, we conducted 16 tests of the supportive parenting × victimization interaction. We conducted an additional 48 tests in which a supportive parenting × victimization effect was embedded in higher-order interactions involving age or gender. Few were significant before controlling for Type I error, and none were afterward. On the one hand, our results are similar to those reported by Davidson and Demaray (2007) and by Papafratzeskakou et al. (2011), who also found no support for a supportive parenting × victimization interaction in young people. On the other hand, our results stand in contrast to other studies that did find evidence for such an interaction (Conners-Burrow et al., 2009; Stadler et al., 2010; Tanigawa et al., 2011). We speculate that methodological differences between their studies and ours (e.g., testing for interactions after categorizing continuous variables, combining a measure of parental support with measures of parental supervision and parental inconsistency) could be responsible for the discrepant results.
The results of Cohen and Wills’ (1985) broad review of the stress/social support literature revealed that generic social support tends to have a main effect on healthy outcomes, whereas stressor-specific forms of social support tend to interact with the stressor to buffer its effect. If something similar were true in the narrower realm of peer victimization and supportive parenting, then it might be the case that parents could enhance their effectiveness by adding victimization-specific informational or instrumental supports to an already supportive parenting style. These speculations clearly go beyond the current study but suggest an important direction for future research.
Our third major finding was that support for Cohen and Wills’ (1985) main effect model generalized across age and gender. That is, no consistent evidence emerged that either age or gender moderated the relation of supportive parenting and peer victimization to depressive symptoms and cognitions. Of 176 interactions tested, only 12 interactions with age or gender were significant, and none of these replicated from the Wave 1–2 analyses to the Wave 2–3 analyses. Further, all 12 significant interactions were eliminated after applying even a fairly liberal method to control the family-wise alpha. Power analyses reveal that with our sample sizes, we had .80 power to detect what Cohen (1988) declared a small effect size (f2 = 0.02).
These results stand in contrast to previous findings by Tanigawa et al. (2011) and Stadler et al. (2010). Tanigawa et al. reported that supportive parenting buffered the effects of peer victimization for boys but not for girls; however, they divided the sample by gender without testing the gender × parenting × victimization interaction. Stadler et al. also reported gender differences in the supportive parenting × victimization interaction; however, their measure of parenting assessed more than supportive behaviors, and their outcome measure assessed more behavior problems than depression per se. Focusing specifically on supportive parenting, peer victimization, and depressive symptoms, the current study found no evidence of moderation by either age or gender.
Fourth, our cross-lag panel analyses revealed two additional findings. The first pertained to the adverse predictive relation of depressive symptoms to supportive parenting. This effect is anticipated by Coyne’s (1976) theory about the adverse effect of depression on the social response of others. Although aspects of this theory remain controversial, little doubt exists about the emotional effect that living with a depressed person has on significant others (Coyne et al., 1987; Coyne, Burchill, & Stiles, 1991). Branje et al.’s (2010) longitudinal study supports the application of this theory to adolescent depression and perceived parental responses. Second, we found some support for a prospective relation of depression to peer victimization. This result likely reflects a different dynamic. Tran et al. (2012) speculated that expression of depressive symptoms may represent a sign of vulnerability or weakness, which may appeal to potential bullies looking for a new target. Bearing in mind that causal inference is premature, we tentatively note that these results could reflect (1) a kind of vicious cycle in which peer victimization is both a contributor to and a consequence of depression and (2) a kind of vicious trap in which parental support, which could protect against depression, is inhibited by the child’s depressive symptoms.
Results of the current study have several important clinical implications. First, the prospective main effects of peer victimization suggest that being bullied by peers affects not just depressive symptoms but the negative cognitive diatheses that put children at risk for depression in the first place. Peer victimization conveys negative self-relevant information to the victim. Either explicitly or indirectly, it effectively communicates messages such as, “You’re weak,” “You’re unlikeable,” “You’re funny looking,” and so forth at an age when a major developmental task is the construction of self-perceived competence (Garber, 1984), such information constitutes an unfortunate set of building blocks. Having many domains of self-perceived incompetence that are offset by relatively few domains of self-perceived competence is a formula for depression in childhood and adolescence (Cole, 1991; Cole et al., 1997; Cole & Turner, 1993). Whether undertaken by teachers, school counselors, clinicians, or parents, the sometimes daunting clinical tasks are to intervene before the child completely internalizes such negative self-information, to help the child challenge these negative precepts, and to facilitate the child’s construction of positive self-competence beliefs to offset the negative.
Second, the value of such efforts is reinforced by our discovery of main effects for supportive parenting on depressive symptoms and related cognition. No doubt, school-based bullying prevention programs are important; however, none has been able to eradicate all episodes of victimization (Merrell, Gueldner, Ross, & Isava, 2008). Not only will some school-based peer victimization filter through even the best school-based prevention programs, but peer victimization can also occur outside the school setting. The current results suggest that parental support can serve as an effective additional line of defense. To be effective, however, at least three things are critical. First is parental awareness. Children are often not effective at informing parents about their victimization experiences. Embarrassment, fear of a negative reaction, poor communication skills, and even children’s lack of awareness that they are in fact being victimized (especially in the case of relational victimization) all contribute to parental unawareness. For these reasons, communication from teachers and counselors to parents is essential. Second is the parent’s belief that peer victimization is important. Stereotypic beliefs that physical bullying is an example of boys being boys or that relational aggression is an example of girls being girls can undermine a parent’s inclination to provide support. A key step often involves convincing parents that peer victimization is a big deal. Third is knowing what to do. Coaching parents in the diversity of behaviors that constitute parental support (and reducing parental behaviors that constitute nonsupport) should be fundamental aspects of parent-focused interventions (Linares, Montalto, Li, & Oza, 2006).
Third, despite the fact that incidence of victimization varies by age and by gender (Boivin, Petitclerc, Feng, & Barker, 2010; Grills & Ollendick, 2002; Prinstein et al., 2001), the current results suggest that parental support can offset at least some of the depressive effects of peer victimization irrespective of age and gender. Whether one is 8 or 15 years old and whether one is a boy or a girl, peer victimization predicts an increase in depressive symptoms, and supportive parenting predicts the opposite. Previous studies note that the severity of peer victimization can increase with age as perpetrators become capable of more vicious forms of aggression (Williams & Guerra, 2007). Consequently, parents and teachers may take less seriously those kinds of victimization that happen at younger ages. Such inaction at younger ages is unwise for two reasons. First, peer victimization is detrimental, and supportive parenting reparative across a wide age range. Second, peer victimization is relatively stable across time and across setting (Rueger, Malecki, & Demaray, 2011). Learning sooner to interrupt it, cope with it, or obtain social supports to offset it should diminish its potential depressogenic consequences.
Shortcomings of the current study suggest directions for future research. One methodological limitation was that we used a paper-and-pencil measure of depressive symptoms (one of our dependent variables). Consequently, we lack information about the effects of victimization and supportive parenting on the incidence of actual episodes of major depression. Although findings often generalize from measures of depression severity to episodes of clinical diagnosis (e.g., Hammen, 1988), future studies using diagnostic interviews are needed to test this generalization. A second concern is that we obtained only children’s reports of supportive parenting. These measures are reliable representations of children’s perceptions of parental support; however, extension of the current study using either parent reports or behavioral observation measures of supportive parenting could reveal other ways in which supportive parenting can help. A third issue is that we used a relatively broadband measure of parental support. Our measure did not inquire about victimization-specific types of parental support. Logic suggests that support for a stress-buffering model could emerge for stressor-specific forms of social support. Fourth, the goal of the current study focused on symptoms and cognitions specific to depression. Time constraints on our access to students prevented the assessment of other forms of psychopathology. A valuable direction for future research would be to assess the generalizability of these effects to proximal and distal forms of psychopathology, for example, social anxiety (Prinstein, Cheah, & Guyer, 2005) and conduct disorder (Schwartz, Proctor, & Chien, 2001). Finally, we chose to focus on children between the grades of 3 and 7 (children ages 8–14) because middle childhood is a time when children are especially vulnerable to victimization (Pellegrini & Long, 2002); however, peer victimization happens at both younger and older ages as well. Age-related changes in the countervailing effect of parental support might be evident in studies of both younger children and older adolescents.
Acknowledgments
This research was supported by a gift from Patricia and Rodes Hart, by support from the Warren Family Foundation, and by National Institute of Child Health and Human Development Grant 1R01HD059891 to David A. Cole. We thank Joy Guss, Audrey Hollowman, Cherish Piche, Dottie Critchlow, Teresa Dennis, Shari Carter, Patti Yon, Alison Effinger, and Latrice Reynolds for their support at various stages of this project. We also thank the children, teachers, and parents who participated in the study.
Footnotes
Although we use terms like “main effect” and “psychological outcome” throughout the article, we do not mean to imply that our results provide evidence of causal relations. Although the data derived from a longitudinal study, random assignment to level of victimization or type of parenting was (of course) impossible, leaving open the possibility of many other explanatory variables.
In both our self-report and peer nomination measures, we focused on full-scale scores, so as to have a measure of multiple subtypes of peer victimization. Although peer victimization is known to be multidimensional, the primary concern of the current study is about the impact of supportive parenting over-and-above peer victimization. By using a measure of victimization that combines subtypes of victimization, we have set the bar high for supportive parenting. That is, supportive parenting must be significant over-and-above a measure of multiple types of peer victimization. If we were to focus on only one victimization subtype at a time, the bar would be lower. Supportive parenting could appear to be significant over-and-above one type of victimization, even though it might not be significant over-and-above multiple types of victimization. Correlations between victimization subtypes ranged from 0.48 to 0.69 (Mdn = 0.59) when measured by self-report and from 0.67 to 0.74 (Mdn = 0.71) when measured by peer nomination, further justifying the aggregation of victimization subtypes.
We elected to conduct multiple regression analyses in lieu of structural equation modeling because the examination of interaction effects in latent variable models requires nonlinear parameter constraints that frequently generate convergence failures and boundary problems even under the best of circumstances.
References
- Allen JP, Insabella G, Porter MR, Smith FD, Land D, Phillips N. A social-interactional model of the development of depressive symptoms in adolescence. Journal of Consulting and Clinical Psychology. 2006;74:55–65. doi: 10.1037/0022-006X.74.1.55. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Auerbach RP, Bigda-Peyton JS, Eberhart NK, Webb CA, Ho MR. Conceptualizing the prospective relationship between social support, stress, and depressive symptoms among adolescents. Journal of Abnormal Child Psychology. 2011;39:475–487. doi: 10.1007/s10802-010-9479-x. [DOI] [PubMed] [Google Scholar]
- Barchia K, Bussey K. The psychological impact of peer victimization: Exploring social-cognitive mediators of depression. Journal of Adolescence. 2010;33:615–623. doi: 10.1016/j.adolescence.2009.12.002. [DOI] [PubMed] [Google Scholar]
- Beck AT. Depression. Harper and Row; New York: 1967. [Google Scholar]
- Blascovich J, Mendes WB. Challenge and threat appraisals: The role of affective cues. In: Forgas JP, editor. Feeling and thinking: The role of affect in social cognition. New York, NY: Cambridge University Press; 2000. pp. 59–82. [Google Scholar]
- Boivin M, Petitclerc A, Feng B, Barker ED. The developmental trajectories of peer victimization in middle to late childhood and the changing nature of their behavioral correlates. Merrill-Palmer Quarterly. 2010;56:231–260. doi: 10.1353/mpq.0.0050. [DOI] [Google Scholar]
- Bokhorst CL, Sumter SR, Westenberg PM. Social support from parents, friends, classmates, and teachers in children and adolescents aged 9 to 18 years: Who is perceived as most supportive? Social Development. 2010;19:417–426. doi: 10.1111/j.1467-9507.2009.00540.x. [DOI] [Google Scholar]
- Branje SJT, Hale WW, Frijns T, Meeus WHJ. Longitudinal associations between perceived parent-child relationship quality and depressive symptoms in adolescence. Journal of Abnormal Child Psychology. 2010;38:751–763. doi: 10.1007/s10802-010-9401-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bruce AE, Cole DA, Dallaire DH, Jacquez FM, Pineda AQ, LaGrange B. Relations of parenting and negative life events to cognitive diatheses for depression in children. Journal of Abnormal Child Psychology. 2006;34:310–322. doi: 10.1007/s10802-006-9019-x. [DOI] [PubMed] [Google Scholar]
- Carver CS, Scheier MF. The self attention-induced feedback loop and social facilitation. Journal of Experimental Social Psychology. 1981;17:545–568. doi: 10.1016/0022-1031(81)90039-1. [DOI] [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. 2. New York, NY: Lawrence Erlbaum Associates; 1988. [Google Scholar]
- Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychological Bulletin. 1985;98:310–357. doi: 10.1037/0033-2909.98.2.310. [DOI] [PubMed] [Google Scholar]
- Coie JD, Dodge KA, Coppotelli H. Dimensions and types of social status: A cross-age perspective. Developmental Psychology. 1982;18:557–570. doi: 10.1037/0012-1649.18.4.557. [DOI] [Google Scholar]
- Cole DA. Preliminary support for a competency-based model of depression in children. Journal of Abnormal Psychology. 1991;100:181–190. doi: 10.1037/0021-843X.100.2.181. [DOI] [PubMed] [Google Scholar]
- Cole DA, Martin JM, Powers B. A competency-based model of child depression: A longitudinal study of peer, parent, teacher, and self-evaluations. The Journal of Child Psychology and Psychiatry. 1997;38:505–514. doi: 10.1111/j.1469-7610.1997.tb01537.x. [DOI] [PubMed] [Google Scholar]
- Cole DA, Maxwell MA, Dukewich TL, Yosick R. Targeted peer victimization and the construction of positive and negative self-cognitions: Connections to depression in children. Journal of Clinical Child and Adolescent Psychology. 2010;39:421–435. doi: 10.1080/15374411003691776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cole DA, Turner JE., Jr Models of cognitive mediation and moderation in self-reported child depression. Journal of Abnormal Psychology. 1993;102:271–281. doi: 10.1037/0021-843X.102.2.271. [DOI] [PubMed] [Google Scholar]
- Conners-Burrow N, Johnson DL, Whiteside-Mansell L, McKelvey L, Gargus RA. Adults matter: Protecting children from the negative impacts of bullying. Psychology in the Schools. 2009;46:593–604. doi: 10.1002/pits.20400. [DOI] [Google Scholar]
- Cornwell B. The dynamic properties of social support: Decay, growth, and staticity, and their effects on adolescent depression. Social Forces. 2003;81:953–978. doi: 10.1353/sof.2003.0029. [DOI] [Google Scholar]
- Coyne JC. Depression and the response of others. Journal of Abnormal Psychology. 1976;85:186–193. doi: 10.1037/0021-843X.85.2.186. [DOI] [PubMed] [Google Scholar]
- Coyne JC, Burchill SAL, Stiles WB. An interactional perspective on depression. In: Snyder CR, Forsyth DO, editors. Handbook of social and clinical psychology: The health perspective. New York, NY: Pergamon Press; 1991. pp. 327–349. [Google Scholar]
- Coyne JC, Kessler RC, Tal M, Turnbull J, Wortman CB, Greden JF. Living with a depressed person. Journal of Consulting and Clinical Psychology. 1987;55:347–352. doi: 10.1037/0022-006X.55.3.347. [DOI] [PubMed] [Google Scholar]
- Craighead WE, Smucker MR, Craighead LW, Ilardi SS. Factor analysis of the children’s depression inventory in a community sample. Psychological Assessment. 1998;10:156–165. doi: 10.1037/1040-3590.10.2.156. [DOI] [Google Scholar]
- Dallaire DH, Pineda AQ, Cole DA, Ciesla JA, Jacquez F, LaGrange B, Bruce AE. Relation of positive and negative parenting to children’s depressive symptoms. Journal of Clinical Child and Adolescent Psychology. 2006;35:313–322. doi: 10.1207/s15374424jccp3502_15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Davidson LM, Demaray MK. Social support as a moderator between victimization and internalizing-externalizing distress from bullying. School Psychology Review. 2007;36:383–405. [Google Scholar]
- De Los Reyes A, Kazdin AE. Informant discrepancies in the assessment of childhood psychopathology: A critical review, theoretical framework, and recommendations for further study. Psychological Bulletin. 2005;131:483–509. doi: 10.1037/0033-2909.131.4.483. [DOI] [PubMed] [Google Scholar]
- De Los Reyes A, Prinstein MJ. Applying depression-distortion hypotheses to the assessment of peer victimization in adolescents. Journal of Clinical Child and Adolescent Psychology. 2004;33:325–335. doi: 10.1207/s15374424jccp3302_14. [DOI] [PubMed] [Google Scholar]
- Furman W, Buhrmester D. Age and sex differences in perceptions of networks of personal relationships. Child Development. 1992;63:103–115. doi: 10.2307/1130905. [DOI] [PubMed] [Google Scholar]
- Garber J. Classification of childhood psychopathology: A developmental perspective. Child Development. 1984;55:30–48. doi: 10.2307/1129833. [DOI] [PubMed] [Google Scholar]
- Grills AE, Ollendick TH. Peer victimization, global self-worth, and anxiety in middle school children. Journal of Clinical Child and Adolescent Psychology. 2002;31:59–68. doi: 10.1207/S15374424JCCP3101_08. [DOI] [PubMed] [Google Scholar]
- Hammen C. Self-cognitions, stressful events, and the prediction of depression in children of depressed mothers. Journal of Abnormal Child Psychology. 1988;16:347–360. doi: 10.1007/BF00913805. [DOI] [PubMed] [Google Scholar]
- Harter S. The perceived competence scale for children. Child Development. 1982;53:87–97. doi: 10.2307/1129640. [DOI] [PubMed] [Google Scholar]
- Harter S. Manual for the self-perception profile for children. Denver, CO: University of Denver; 1985. [Google Scholar]
- Harter S. The construction of the self: A developmental perspective. New York, NY: Guilford Press; 1999. [Google Scholar]
- Harter S. The construction of the self: Developmental and socio-cultural foundations. 2. New York, NY: Guilford Press; 2012. [Google Scholar]
- Harter S, Whitesell NR. Multiple pathways to self-reported depression and psychological adjustment among adolescents. Development and Psychopathology. 1996;8:761–777. doi: 10.1017/S0954579400007410. [DOI] [Google Scholar]
- Hawker DSJ, Boulton MJ. Twenty years’ research on peer victimization and psychosocial maladjustment: A meta-analytic review of cross-sectional studies. Journal of Child Psychology and Psychiatry. 2000;41:441–455. doi: 10.1111/1469-7610.00629. [DOI] [PubMed] [Google Scholar]
- Hazzard A, Christensen A, Margolin G. Children’s perceptions of parental behaviors. Journal of Abnormal Child Psychology. 1983;11:49–59. doi: 10.1007/BF00912177. [DOI] [PubMed] [Google Scholar]
- Holahan CJ, Valentiner DP, Moos RH. Parental support, coping strategies, and psychological adjustment: An integrative model with late adolescents. Journal of Youth and Adolescence. 1995;24:633–648. doi: 10.1007/BF01536948. [DOI] [Google Scholar]
- Kaslow NJ, Stark KD, Printz B, Livingston R, Tsai SL. Cognitive Triad Inventory for Children: Development and relation to depression and anxiety. Journal of Clinical Child Psychology. 1992;21:339–347. doi: 10.1207/s15374424jccp2104_3. [DOI] [Google Scholar]
- Kazdin AE, Colbus D, Rodgers A. Assessment of depression and diagnosis of depressive disorder among psychiatrically disturbed children. Journal of Abnormal Child Psychology. 1986;14:499–515. doi: 10.1007/BF01260519. [DOI] [PubMed] [Google Scholar]
- Kendall PC, Cantwell DP, Kazdin AE. Depression in children and adolescents: Assessment issues and recommendations. Cognitive Therapy and Research. 1989;13:109–146. doi: 10.1007/BF01173268. [DOI] [Google Scholar]
- Kovacs M. The Children’s Depression Inventory (CDI) Psycho-pharmacology Bulletin. 1985;21:995–998. [PubMed] [Google Scholar]
- Ladd GW, Kochenderfer-Ladd B. Identifying victims of peer aggression from early to middle childhood: Analysis of cross-informant data for concordance, estimation of relational adjustment, prevalence of victimization, and characteristics of identified victims. Psychological Assessment. 2002;14:74–96. doi: 10.1037/1040-3590.14.1.74. [DOI] [PubMed] [Google Scholar]
- LaGrange B, Cole DA, Dallaire DH, Ciesla JA, Pineda AQ, Truss AE, Folmer A. Developmental changes in depressive cognitions: A longitudinal evaluation of the Cognitive Triad Inventory for Children. Psychological Assessment. 2008;20:217–226. doi: 10.1037/1040-3590.20.3.217. [DOI] [PubMed] [Google Scholar]
- Lewinsohn PM, Hops HE, Roberts RE, Seeley JR, Andrews JR. Adolescent psychopathology: I. prevalence and incidence of depression and other DSM-III–R disorders in high school students. Journal of Abnormal Psychology. 1993;102:133–144. doi: 10.1037/0021-843X.102.1.133. [DOI] [PubMed] [Google Scholar]
- Lewinsohn PM, Roberts RE, Seeley JR, Rohde P, Gotlib IH, Hops H. Adolescent psychopathology: II. Psychosocial risk factors for depression. Journal of Abnormal Psychology. 1994;103:302–315. doi: 10.1037/0021-843X.103.2.302. [DOI] [PubMed] [Google Scholar]
- Linares LO, Montalto D, Li M, Oza VS. A promising parenting intervention in foster care. Journal of Consulting and Clinical Psychology. 2006;74:32–41. doi: 10.1037/0022-006X.74.1.32. [DOI] [PubMed] [Google Scholar]
- Lovejoy MC, Weis R, O’Hare E, Rubin EC. Development and initial validation of the parent behavior inventory. Psychological Assessment. 1999;11:534–545. doi: 10.1037/1040-3590.11.4.534. [DOI] [Google Scholar]
- McLeod BD, Weisz JR, Wood JJ. Examining the association between parenting and childhood depression: A meta-analysis. Clinical Psychology Review. 2007;27:986–1003. doi: 10.1016/j.cpr.2007.03.001. [DOI] [PubMed] [Google Scholar]
- Merrell KW, Gueldner BA, Ross SW, Isava DM. How effective are school bullying intervention programs? A meta-analysis of intervention research. School Psychology Quarterly. 2008;23:26–42. doi: 10.1037/1045-3830.23.1.26. [DOI] [Google Scholar]
- Mezulis AH, Hyde JS, Abramson L. The developmental origins of cognitive vulnerability to depression: Temperament, parenting, and negative life events in childhood as contributors to negative cognitive style. Developmental Psychology. 2006;42:1012–1025. doi: 10.1037/0012-1649.42.6.1012. [DOI] [PubMed] [Google Scholar]
- Muris P, Meesters C, Fijen P. The self-perception profile for children: Further evidence for its factor structure, reliability, and validity. Personality and Individual Differences. 2003;35:1791–1802. doi: 10.1016/S0191-8869(03)00004-7. [DOI] [Google Scholar]
- Nansel TR, Overpeck M, Pilla RS, Ruan WJ, Simons-Morton B, Scheidt P. Bullying behaviors among US youth: Prevalence and association with psychosocial adjustment. Journal of the American Medical Association. 2001;285:2094–2100. doi: 10.1001/jama.285.16.2094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Newman ML, Holden GW, Delville Y. Isolation and the stress of being bullied. Journal of Adolescence. 2005;28:343–357. doi: 10.1016/j.adolescence.2004.08.002. [DOI] [PubMed] [Google Scholar]
- Papafratzeskakou E, Kim J, Longo GS, Riser DK. Peer victimization and depressive symptoms: Role of peers and parent–child relationship. Journal of Aggression, Maltreatment & Trauma. 2011;20:784–799. doi: 10.1080/10926771.2011.608220. [DOI] [Google Scholar]
- Pellegrini AD, Long JD. Longitudinal study of bullying, dominance, and victimization during the transition from primary through secondary school. British Journal of Developmental Psychology. 2002;20:259–280. doi: 10.1348/026151002166442. [DOI] [Google Scholar]
- Prinstein MJ, Aikins JW. Cognitive moderators of the longitudinal association between peer rejection and adolescent depressive symptoms. Journal of Abnormal Child Psychology. 2004;32:147–158. doi: 10.1023/B:JACP.0000019767.55592.63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Prinstein MJ, Cheah CSL, Guyer AE. Peer victimization, cue interpretation, and internalizing symptoms: Preliminary concurrent and longitudinal findings for children and adolescents. Journal of Clinical Child and Adolescent Psychology. 2005;34:11–24. doi: 10.1207/s15374424jccp3401_2. [DOI] [PubMed] [Google Scholar]
- Prinstein MJ, Cillessen AHN. Forms and functions of adolescent peer aggression associated with high levels of peer status. Merrill-Palmer Quarterly. 2003;49:310–342. doi: 10.1353/mpq.2003.0015. [DOI] [Google Scholar]
- Prinstein MJ, Boegers J, Vernberg EM. Overt and relational aggression in adolescents: Social-psychological adjustments of aggressors and victims. Journal of Clinical Child Psychology. 2001;30:479–491. doi: 10.1207/S15374424JCCP3004_05. [DOI] [PubMed] [Google Scholar]
- Rapee RM. Potential role of childrearing practices in the development of anxiety and depression. Clinical Psychology Review. 1997;17:47–67. doi: 10.1016/S0272-7358(96)00040-2. [DOI] [PubMed] [Google Scholar]
- Reijntjes A, Kamphuis JH, Prinzie P, Telch MJ. Peer victimization and internalizing problems in children: A meta-analysis of longitudinal studies. Child Abuse & Neglect. 2010;34:244–252. doi: 10.1016/j.chiabu.2009.07.009. [DOI] [PubMed] [Google Scholar]
- Rueger SY, Malecki CK, Demaray MK. Stability of peer victimization in early adolescence: Effects of timing and duration. Journal of School Psychology. 2011;49:443–464. doi: 10.1016/j.jsp.2011.04.005. [DOI] [PubMed] [Google Scholar]
- Schniering CA, Rapee RM. Development and validation of a measure of children’s automatic thoughts: The children’s automatic thoughts scale. Behaviour Research and Therapy. 2002;40:1091–1109. doi: 10.1016/S0005-7967(02)00022-0. [DOI] [PubMed] [Google Scholar]
- Schwartz D, Proctor LJ, Chien DH. The aggressive victim of bullying: Emotional and behavioral dysregulation as a pathway to victimization by peers. In: Schwartz D, Proctor LJ, Chien DH, editors. Peer harassment in school: The plight of the vulnerable and victimized. New York, NY: Guilford Press; 2001. pp. 147–174. [Google Scholar]
- Sheeber L, Hops H, Alpert A, Davis B, Andrews J. Family support and conflict: Prospective relations to adolescent depression. Journal of Abnormal Child Psychology. 1997;25:333–344. doi: 10.1023/A:1025768504415. [DOI] [PubMed] [Google Scholar]
- Spirito A, Stark LJ, Grace N, Stamoulis D. Common problems and coping strategies reported in childhood and early adolescence. Journal of Youth and Adolescence. 1991;20:531–544. doi: 10.1007/BF01540636. [DOI] [PubMed] [Google Scholar]
- Stadler C, Feifel J, Rohrmann S, Vermeiren R, Poustka F. Peer-victimization and mental health problems in adolescents: Are parental and school support protective? Child Psychiatry and Human Development. 2010;41:371–386. doi: 10.1007/s10578-010-0174-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tanigawa D, Furlong MJ, Felix ED, Sharkey JD. The protective role of perceived social support against the manifestation of depressive symptoms in peer victims. Journal of School Violence. 2011;10:393–412. doi: 10.1080/15388220.2011.602614. [DOI] [Google Scholar]
- Tran CV, Cole DA, Weiss B. Testing reciprocal longitudinal relations between peer victimization and depressive symptoms in young adolescents. Journal of Clinical Child and Adolescent Psychology. 2012;41:353–360. doi: 10.1080/15374416.2012.662674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Turner HA, Finkelhor D, Hamby SL, Shattuck A, Ormrod RK. Specifying type and location of peer victimization in a national sample of children and youth. Journal of Youth and Adolescence. 2011;40:1052–1067. doi: 10.1007/s10964-011-9639-5. [DOI] [PubMed] [Google Scholar]
- Williams KR, Guerra NG. Prevalence and predictors of Internet bullying. Journal of Adolescent Health. 2007;41:S14–S21. doi: 10.1016/j.jadohealth.2007.08.018. [DOI] [PubMed] [Google Scholar]