

According to the latest report of The International Agency for Research on Cancer (GLOBOCAN 2012), breast cancer (BC) is by far the world’s most common cancer among women, and the most likely cause that a woman will die from cancer worldwide (1).
The disease is reported as the most frequent cancer among women in 140 of 184 countries worldwide including China the world’s most populous country (1,2). Notably, the incidence rates of BC varies dramatically across the globe, being always highest in more developed regions, namely North America, Western Europe (more than 90 new cases/105 women annually), compared with less than 30/105 women annually in regions like Eastern Asia (1). In the current issue of JTD, Zeng et al. (3), have published the first national dataset on the incidence and mortality of female BC in China, for the year 2010, highlighting also some trends in incidence, and mortality, in different geographical regions within China. The authors should be commended for being the first to provide the literature with a wealth of data regarding BC statistics in China, which harbors around one fifth of all women around the world. According to the authors’ estimations, the age standardized incidence rate (ASIR) of BC is 24.2/105 and age standardized mortality rate (ASMR) is 6.36/105. As such, these figures would confirm the known fact, that the mainland Chinese women have one of lowest BC incidence and mortality rates, when compared to the rest of the world.
Two important questions should be raised with this kind of findings: how far the authors could accurately quantify BC burden (occurrence and outcome) in China? and if their figures are true, then why the mainland Chinese women are so much protected against BC versus Chinese women in other Asian or western counties?
To start with, we need to emphasize that Zeng et al. analysis included only 12.96% of the female population of China. This means that the vast majority of Chinese women are not truly represented in their analysis, especially in the western region (less than 10% of their sample size), where the incidence is ~30% less than that reported in other areas. Obviously, “a cautious interpretation” is warranted with this kind of national epidemiological studies, when so many regions in a given country have low or no accurate registry data. Nonetheless, this is a common situation in many countries with emerging population-based registries (4). For instance, in Egypt; with its much smaller scale in geographical and population size, a network of five regional population-based registries, spreading over the whole country, was developed during the last two decades. For the sake of national cancer statistics, Egypt was divided into three regions namely upper, middle and lower Egypt. One or more defined states (governorates), with a regional population-based registry, were selected to represent each region (4). The data evolved on cancer incidence from each cancer registry were extrapolated in a similar methodology like that adopted by Chinese group. BC is estimated to be the most common female cancer in both China and Egypt, despite a marked difference in incidence rates, being much higher among Egyptian women compared to Chinese (ASIR are 48.8/105 and 24.2/105 respectively) (3,4). In the two countries BC incidence differs considerably among rural and urban populations, with the higher urban incidence being consistent across all women above the age of 45 years (3,5). A similar observation was also found in many developing countries like India, where BC incidence in rural registry of Barshi was 7.2/105 compared to 31.3/105 in adjoining city of Mumbai (6). In fact, the urban population in developing countries, might suffer from a higher exposure to xenoestrogens, which have been linked to evolution of hormone receptor positive BC in industrialized countries (7).
Pattern of age specific incidence of BC from east to west
Like other countries the age-specific incidence rates in both Egypt and China show a progressive increase after the age of 30 years, to reach a sharp peak of 80/105 at the age group of 55-59 years in China, versus a sharp peak of 177.4/105 at the age group of 60-64 years in Egypt (3,4). Importantly, in both countries there was a gradually decline in the age-specific incidence thereafter. This pattern of the age specific incidence is in clear contradistinction with western countries, where a continuous rise in BC incidence is observed with increasing age, to reach a peak of ~450/105, at the age 80 years, thus rendering the differences in age-specific incidence especially large in elderly women (8-10) (Figure 1).
Figure 1.
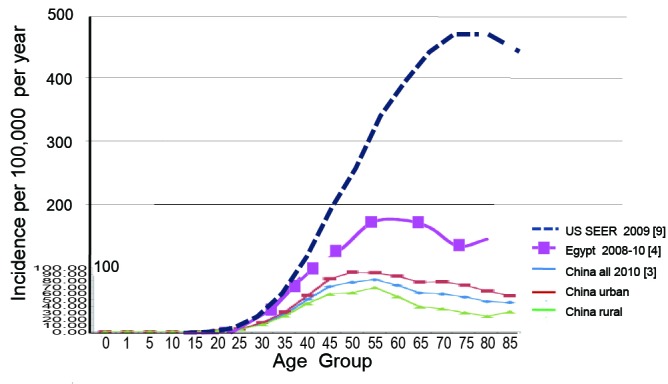
Age specific incidence rates of breast cancer in China, Egypt, and USA.
We do not know whether this difference is completely real, or it is partially induced by under-reporting of BC cases specifically among elderly patients, in countries with emerging cancer registry programs. Notably, a pattern of BC age specific incidence, similar to that seen in China and Egypt, has been reported in some Asian countries with a completed national cancer registries like Japan and Singapore (11,12). This would certainly challenge the rule of “The Older the Age; The Higher the BC Risk”, which might not be a default hypothesis, when it comes to North African and East Asian women.
Are the mainland Chinese women more protected from BC?
The reasons for the wide international variation in incidence rates of BC are not fully explained. However, it seems true that the low-risk Chinese (and other Asian) populations are enjoying a multitude of biological and lifestyle features that collectively provide a significant protection against the development of BC. In a cross sectional study, Chinese women were found to be significantly less obese (~14 kg less), have their menarche a year later, are more often parous, and consume a lower western diet, compared to Caucasian women (13). The protective effect of Chinese diet was highly emphasized during the last decade. In one study on 1,602 BC women and 1,500 healthy women, all living in Shanghai, it was found that a “meat and sweet” western-style diet was independently associated with a 60% increased risk of BC, compared to a “soy and vegetable” traditional Chinese diet (14). The effect was more significant for estrogen-receptor positive tumors, where the risk of getting this phenotype of BC was almost doubled, among women utilizing western diet (14). A recent meta-analysis, found that the Chinese diet intake is associated with a 41% reduction in BC risk among Asian women (15). This main part explain why Chinese women migrating to North America, adopting a westernized lifestyle, will show a significant rise of BC incidence over a few generations (10,16). Taken together, lifestyle and socio-demographic factors stand as major players in the low BC burden, reported in China and other developing East Asian countries. However and in spite of the major similarities in lifestyle, the incidence rate of BC among Chinese women in the mainland is strikingly lower than that reported for Chinese women in other Asian countries. For example, in Singapore, where a complete national registry coverage is accomplished, an ASIR of 63.7/105 has been reported among the Chinese population there (12). Similar figures were also reported in Hong Kong (61/105) (17) and Malaysian Chinese (59.9/105) (18), with a somewhat lower incidence among Taiwanese women (44.45/105) (19) (Table 1).
Table 1. Breast cancer ASIR and ASMR for East and West Chinese women.
| Chinese population | ASIR+ | ASMR++ |
|---|---|---|
| Chinese Mainland [3] | 24.2 | 6.36 |
| Chinese Singapore [12] | 63.7 | 14.2 |
| Chinese Hong Kong [17] | 59.9 | NA* |
| Chinese Malaysia [18] | 61 | 9.1 |
| Chinese Taiwan [19] | 44.45 | NA* |
| Chinese US [16] | 73.5 | 11.5 [10]** |
+ASIR, age standardized incidence rate; ++ASMR, age standardized mortality rate; *NA, not available in the published reference; **, for all Asian-Americans.
It does not seem that, factors like life expectancy, more urbanization and presence of BC screening programs, can fully explain a 2-3 fold decrease in BC incidence among the mainland Chinese women, compared to Chinese women in other far east countries.
In conclusion, many factors can be directly responsible for the large variation in BC epidemiology across the globe; including life style, life expectancy, wide spread use of screening mammography and accuracy of national cancer statistics. The later factor is specifically crucial in developing countries, where the emerging population—based cancer registries may suffer from under—recording of some of the occurring BC (as well as other cancers). We believe that a wider expansion of the national cancer registries in both China as well as Egypt, will be able to answer some of the many questions, related to variations in BC statistics in the developing countries.
Acknowledgements
Disclosure: The authors declare no conflict of interest.
References
- 1.Ferlay J, Soerjomataram I, Ervik M, et al. GLOBOCAN 2012 v1.0, Cancer Incidence and Mortality Worldwide (2013). IARC CancerBase No. 11 Lyon, France: International Agency for Research on Cancer. Available online: http://globocan.iarc.fr/
- 2.Chen W, Zheng R, Zhang S, et al. Annual report on status of cancer in China, 2010. Chin J Cancer Res 2014;26:48-58 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Zeng H, Zheng R, Zhang S, et al. Female breast cancer statistics of 2010 in China: estimates based on data from 145 population-based cancerregistries. J Thorac Dis 2014;6:466-70 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Ibrahim A, Khaled H, Mikhail N, et al. Cancer Incidence in Egypt: Results of the National Population-Based Cancer Registry Program. Journal of Cancer Epidemiology 2014. Available online: http://cancerregistry.gov.eg/publications.aspx [DOI] [PMC free article] [PubMed]
- 5.Dey S, Soliman AS, Hablas A, et al. Urban-rural differences in breast cancer incidence in Egypt (1999-2006). Breast 2010;19:417-23 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Risk Factors for Breast Cancer in India: an INDOX Case-Control Study. Available online: INDOX Cancer Research Network. 2010.
- 7.Brody JG, Moysich KB, Humblet O, et al. Environmental pollutants and breast cancer: epidemiologic studies. Cancer 2007;109:2667-711 [DOI] [PubMed] [Google Scholar]
- 8.Mistry M, Parkin DM, Ahmad AS, et al. Cancer incidence in the United Kingdom: projections to the year 2030. Br J Cancer 2011;105:1795-803 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Howlader N, Noone AM, Krapcho M, et al. eds. SEER Cancer Statistics Review, 1975-2009 (Vintage 2009 Populations), National Cancer Institute. Bethesda, MD, 2012. Retrieved September 7, 2012. [Google Scholar]
- 10.DeSantis C, Ma J, Bryan L, et al. Breast cancer statistics, 2013. CA Cancer J Clin 2014;64:52-62 [DOI] [PubMed] [Google Scholar]
- 11.Tominaga S, Kuroishi T.Epidemiology of breast cancer in Japan. Cancer Lett 1995;90:75-9 [DOI] [PubMed] [Google Scholar]
- 12.Peng LH, Ling C, Yew CK, et al. Singapore Cancer Registry Interim Annual Registry Report Trends in Cancer Incidence in Singapore 2008-2012. National Registry of Diseases Office (NRDO).
- 13.Tam CY, Martin LJ, Hislop G, et al. Risk factors for breast cancer in postmenopausal Caucasian and Chinese-Canadian women. Breast Cancer Res 2010;12:R2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Cui X, Dai Q, Tseng M, et al. Dietary patterns and breast cancer risk in the shanghai breast cancer study. Cancer Epidemiol Biomarkers Prev 2007;16:1443-8 [DOI] [PubMed] [Google Scholar]
- 15.Chen M, Rao Y, Zheng Y, et al. Association between soy isoflavone intake and breast cancer risk for pre- and post-menopausal women: a meta-analysis of epidemiological studies. PLoS One 2014;9:e89288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Gomez SL, Quach T, Horn-Ross PL, et al. Hidden breast cancer disparities in Asian women: disaggregating incidence rates by ethnicity and migrant status. Am J Public Health 2010;100Suppl 1:S125-31 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Hong Kong Cancer Registry 2011. Available online: www.pco.org.hk
- 18.Abdullah NA, Wan Mahiyuddin WR, Muhammad NA, et al. Survival rate of breast cancer patients in Malaysia: a population-based study. Asian Pac J Cancer Prev 2013;14:4591-4 [DOI] [PubMed] [Google Scholar]
- 19.Chiang CJ, Chen YC, Chen CJ, et al. Cancer trends in Taiwan. Jpn J Clin Oncol 2010;40:897-904 [DOI] [PubMed] [Google Scholar]