

Unanticipated cancellation of scheduled operations causes economic burdens to hospitals because of wasted resources, including idle medical staff and inefficient use of operating room facilities, as well as patient inconvenience. Previous authors have reported cancellation rates ranging from 1.96% to 20.5% [1,2,3,4,5]. Reasons for cancellations vary from one institution to another, depending on a variety of practice settings. Therefore, each hospital must have its own reliable cancellation data to develop ways to reduce cancellations. In our practice, we run an expandable operating time system, which allows surgeons to finish their cases once they are on the scheduling list. Furthermore, patients undergo preoperative medical evaluation by surgeons.
We conducted this prospective study to identify reasons for cancellation and to propose recommendations to reduce the cancellation rate that are appropriate to the circumstances we have. After institutional review board approval, we reviewed the list of surgery cancellations at a teaching hospital (500 resourced beds, 9 operating rooms) in a metropolitan area from December 2011 to November 2012.
A cancellation of planned surgery was defined as any operation that was on the final scheduling list (generated at 2 PM the previous day) and that was not accomplished on that day. In accordance with our procedures, the surgeon should inform the anesthesia administrative staff to call off a planned case, and the anesthesiologist identifies the reason for cancellation and judges whether the event was hospital related or patient related. We also divided the reasons for cancellation into avoidable versus unavoidable. The definition of "avoidable" was a cancellation due to circumstances or information available prior to registration; it could have been avoided with judicious review of medical records or communication with patients.
A total of 5,260 cases were registered for elective surgeries during the study period, of which 463 cases (8.8%) were cancelled. In all, 301 cases (65%) were judged to be avoidable cancellations versus 162 that were judged to be unavoidable. Three quarters of the avoidable cancellations (218/301) were patient-related, with the main reason being that patients simply changed their minds about undergoing surgery (Table 1). Unfortunately, there is no designated department in charge of sending text messages or reminder calls to patients about their appointments at our hospital. We assume that some surgeons call patients if they are not admitted for planned surgery and others do not try to contact patients.
Table 1.
Reasons for Cancellation of Surgery (n = 463)
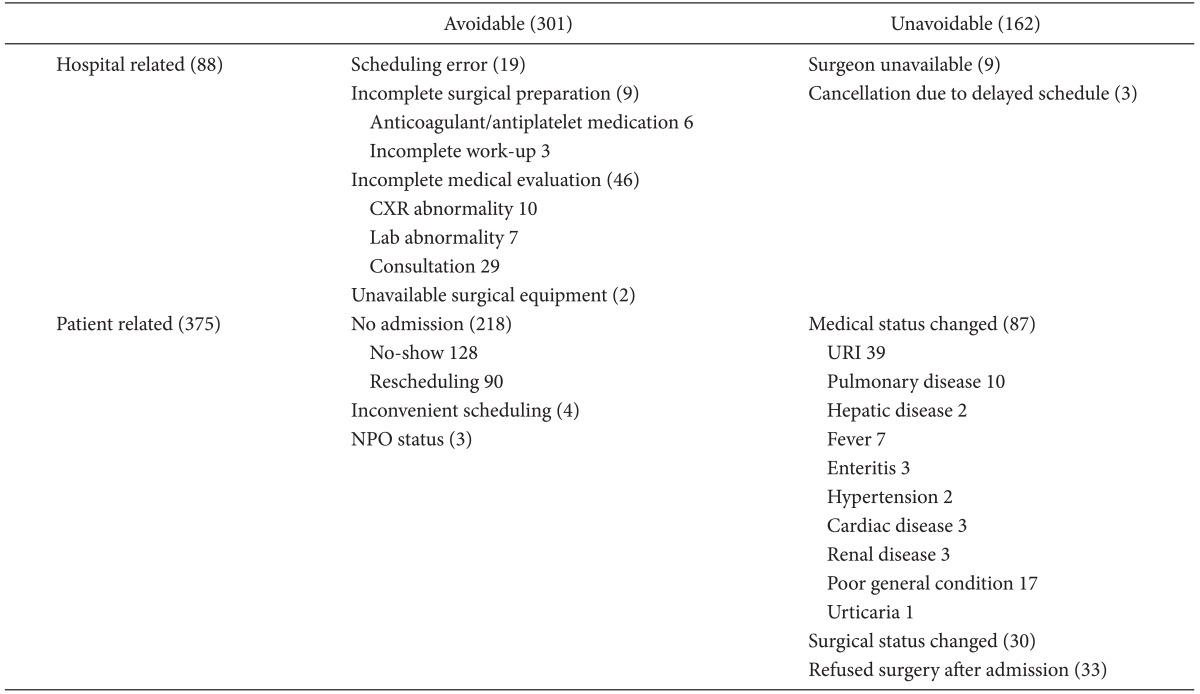
CXR: chest X-ray, URI: upper respiratory infection, NPO: non per os.
Effective action plans should be instituted to reduce cancellations due to absence of a patient. We could improve patients' compliance with agreed procedures by conducting a laboratory workup before scheduling, so patients could be more careful with decision-making. Close communication with patients through a formal route such as a call center could be another alternative.
Of the avoidable cancellations, inadequate medical evaluation was the second most important reason, representing 46 of 301 cases. The major reasons were abnormal laboratory test results or patients' preexisting disease that needed further medical treatment or evaluation. Surgeons scheduled their patients without proper evaluation in most of these cases. Although several authors have emphasized the introduction of preanesthesia clinics for better preoperative management, this has not yet been fully implemented in Korea [1,2].
Thanks to our expandable scheduling system for operations, surgeries are rarely cancelled due to a shortage of available theater time. Instead, surgeons should wait their turn because fewer operating rooms are open after regular working hours. Three cases were cancelled because surgeons did not want to wait their turn. Where operating room hours were regulated, the most common reason for surgery cancellation was overbooked surgeries [3,4].
Trentman et al. [5] reviewed cancelled surgeries over 1 year and reported that 238 of 12,176 surgeries (1.96%) were cancelled and judged 109 cases as avoidable cancellations. They had a preoperative medical evaluation clinic in the anesthesiology department and ran a schedule of flexible operating room time. The cancellation rate in our study was four times higher although both hospitals have flexible operating room schedules. This discrepancy came from the large number of cancellations due to expected patients not being admitted because they changed their minds in our study. There were only 11 cancelled cases because patients changed their minds in Trentman's study compared to 218 cases in our study. We categorized these cases as avoidable because the surgeon or other medical personnel could have contacted patients before cases were confirmed. This is why avoidable cases outweighed unavoidable cases in our study.
There have been many studies regarding surgery cancellation, but the authors focused on idling resources. However, as an anesthesiologist myself, I think we have overlooked the hard work done by anesthesiologists because of cancellation: informing scrub nurses and assigned anesthesiologists, and finding substitute cases for a vacant slot. Unnecessary chart review for noshow patients is also a nuisance and waste of time. If avoidable cancellation cases were filtered, the extra work done by anesthesiologists could be eased.
References
- 1.Yoon SJ, Choi KO, Yoon SM, Lim HJ, Lee HW, Cho H, et al. A statistical analysis of the causes of cancellation of elective operation. Korean J Anesthesiol. 2001;40:139–143. [Google Scholar]
- 2.Song SO, Kim SY, Song SK. Reasons of the cancellation of an elective planned surgery. Korean J Anesthesiol. 1992;25:602–609. [Google Scholar]
- 3.Kumar R, Gandhi R. Reasons for cancellation of operation on the day of intended surgery in a multidisciplinary 500 bedded hospital. J Anaesthesiol Clin Pharmacol. 2012;28:66–69. doi: 10.4103/0970-9185.92442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Schofield WN, Rubin GL, Piza M, Lai YY, Sindhusake D, Fearnside MR, et al. Cancellation of operations on the day of intended surgery at a major Australian referral hospital. Med J Aust. 2005;182:612–615. doi: 10.5694/j.1326-5377.2005.tb06846.x. [DOI] [PubMed] [Google Scholar]
- 5.Trentman TL, Mueller JT, Fassett SL, Carla L, Dormer CL, Weinmeister KP. Day of surgery cancellations in a tertiary care hospital: a one year review. J Anesth Clinic Res. 2010 Dec 10; Available from http://omicsonline.org/2155-6148/2155-6148-1-109.pdf. [Google Scholar]