

Abstract
Background
Diseases of the heart valves constitute a major cause of cardiovascular morbidity and mortality worldwide with rheumatic heart disease (RHD) being the dominant form of valvular heart disease (VHD) in developing nations. The current study was undertaken at a tertiary care cardiac center with the objective of establishing the incidence and patterns of VHD by Echocardiography (Echo).
Methods
Among the 136,098 first-time Echocardiograms performed between January 2010 and December 2012, an exclusion criterion of trivial and functional regurgitant lesions yielded a total of 13,289 cases of organic valvular heart disease as the study cohort.
Results
In RHD, the order of involvement of valves was mitral (60.2%), followed by aortic, tricuspid and pulmonary valves. Mitral stenosis, predominantly seen in females, was almost exclusively of rheumatic etiology (97.4%). The predominant form of isolated MR was rheumatic (41.1%) followed closely by myxomatous or mitral valve prolapse (40.8%). Isolated AS, more common in males, was the third most common valve lesion seen in 7.3% of cases. Degenerative calcification was the commonest cause of isolated AS (65.0%) followed by bicuspid aortic valve (BAV) (33.9%) and RHD (1.1%). Multiple valves were involved in more than a third of all cases (36.8%). The order of involvement was MS + MR > MS + AR > MR + AR > AS + AR > MR + AS > MS + AS. Overall, 9.7% of cases had organic tricuspid valve disease.
Conclusion
RHD contributed most to the burden of VHD in the present study with calcific degeneration, myxomatous disease and BAV being the other major forms of VHD. Multiple valves were affected in more than a third of all cases.
Keywords: Valvular heart disease, Incidence, Echocardiography, Rheumatic heart disease
1. Introduction
Diseases of the heart valves constitute a major cause of cardiovascular morbidity and mortality worldwide with an enormous burden on healthcare resources. Rheumatic heart disease (RHD) continues to be the dominant form of heart valve disease in developing nations.1 The prevalence of RHD has greatly decreased in developed nations; however, increasing life expectancy and atherosclerotic risk factors have increased the risk of acquiring age-related degenerative valvular heart disease (VHD). Although the patterns of valve disease differ among these nations, the burden of valvular heart disease continues unabated across the globe. With RHD affecting predominantly the young population in their productive years, the socio-economic impact on the society is enormous. Little data exists on the prevalence of valvular heart disease as studied by Echocardiography (Echo), although several autopsy2–4 and surgical pathology5–8 series form a rich source of literature on the patterns of valvular heart disease. The current study was undertaken to establish the incidence and patterns of heart valve disease as studied by Echo. While pathological examination of valves obtained at surgery or autopsy remains the gold standard in morphological analysis, with the current advances in techniques, comparable information on the anatomy and hemodynamic effects of valve disease can be obtained by Echo.
2. Methods
The current study was undertaken at Sri Jayadeva Institute of Cardiovascular Sciences and Research, a tertiary care high-volume cardiac center located at Bangalore, South India, where more than 100,000 Echocardiograms are performed annually. All the Echocardiograms done over a period of 3 years from January 2010 through December 2012 were analyzed for the present study. Among the 409,468 Echocardiograms performed during the period, only the first-time Echo of each patient was included for the study to avoid repetition bias. Hence, a total of 136,098 discrete Echo reports were available for inclusion. From the total database of 60,535 cases for any valvular heart disease, the following were excluded from the study: trivial, functional or unspecified mechanisms of mitral regurgitation (MR), trivial to mild aortic regurgitation (AR) due to sclerotic aortic valve or unspecified causes and trivial or functional tricuspid regurgitation (TR), with the remaining 13,289 cases of organic valvular heart disease forming the study cohort for the present analysis (Fig. 1). Trace to small degrees of MR and TR can be detected in up to 80–90% of individuals on careful Doppler Echo and can confound the estimates of disease prevalence.9,10 Also, the study was designed to determine the patterns of primary or organic valve disease; hence trivial, functional or insignificant regurgitation was excluded from the analysis to avoid erroneous estimates that can be produced by these large numbers of insignificant lesions.
Fig. 1.
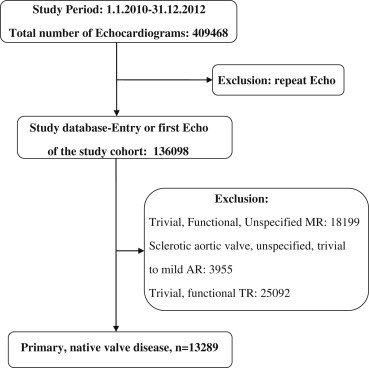
Algorithm showing the inclusion and exclusion criteria of cases for the present study (AR = Aortic Regurgitation, MR = Mitral Regurgitation, TR = Tricuspid Regurgitation).
3. Results
The Echocardiograms were analyzed in two parts: all the isolated valve lesions were analyzed first followed by various combinations of valve lesions. The data is presented in tables and charts. Data is expressed in numbers, percentages and ratios. An overview of the patterns of valve disease is presented in Fig. 2.
Fig. 2.
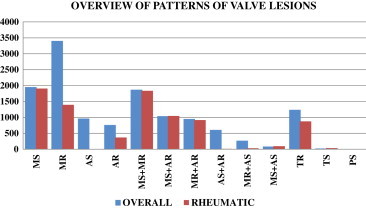
Overview of patterns of valvular heart disease (AR = Aortic Regurgitation, AS = Aortic Stenosis, MR = Mitral Regurgitation, MS = Mitral Stenosis, PS = Pulmonary Stenosis, TR = Tricuspid Regurgitation, TS = Tricuspid Stenosis).
Mitral valve was the most common involved valve in the rheumatic group, seen in 60.2% of the cases. Another 24.5% of cases had involvement of aortic valve as well, making the overall involvement of mitral valve in RHD to be 84.7%. When the overall cohort was considered, the corresponding figures were 54.4%, 18% and 72.4% respectively; thus making mitral the most common involved valve in VHD. Among patients with isolated mitral valve involvement, pure mitral stenosis (MS) was the dominant lesion (37.1%). Another 35.7% of cases had MR in addition to MS; thus, MS was seen in a total of 72.8% of patients with isolated rheumatic mitral valve disease with the remaining patients having pure MR (27.2%). Aortic valve (AV) was involved in 29.1% of cases making it the second most common valve to be involved in RHD; most cases had associated mitral valve involvement. Isolated involvement of AV was rare in the rheumatic group. In the overall cohort, aortic valve was involved in 35.8% of patients. Next most common to be involved was Tricuspid valve (10.7% and 9.7% of rheumatic and overall cohorts respectively). Most of the lesions were TR (10.4%). Tricuspid stenosis (TS) was rare (0.3%). Pulmonary was the least common valve to be involved in RHD (0.04%); all cases had associated MS.
3.1. Isolated MS
The distribution of cases according to etiology and gender is shown in Table 1. Age- and Sex-wise distribution of rheumatic MS cases is shown in Fig. 3. A steady increase in the incidence of rheumatic MS can be seen with each decade with a peak occurring at 30–39 years. This trend was seen in both female and male patients. Nearly two-thirds (65.9%) of MS patients were females. Interestingly, MS was seen as an isolated lesion even in elderly patients (≥60 years).
Table 1.
Distribution of Mitral Stenosis cases according to etiology and gender (F:M = Female:Male, MS = Mitral Stenosis).
| Etiology | No (%) | Female | Male | F:M |
|---|---|---|---|---|
| Rheumatic MS | 1909 (97.4%) | 1259 | 650 | 1.93:1 |
| Congenital Heart diseasea | 30 (1.5%) | 19 | 11 | 1.73:1 |
| Post-Mitral valve repair | 15 (0.8%) | 10 | 5 | 2.0:1 |
| Sclero-degenerative | 5 (0.3%) | 5 | 0 | – |
| 1959 | 1293 | 666 | 1.94:1 |
0.4% – parachute mitral valve/single papillary muscle and 1.1% – MS associated with other congenital heart diseases (including atrial septal defect, ventricular septal defect, situs inversus with dextrocardia).
Fig. 3.
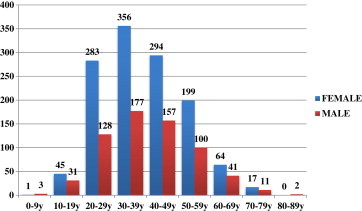
Age and Sex-wise distribution of Rheumatic Mitral Stenosis cases.
3.1.1. Severity of MS
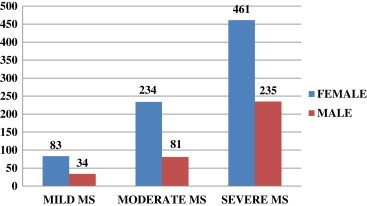
At presentation, most patients (47.2%) were found to have severe MS, defined as a mitral valve orifice area (MVOA) ≤1.0 cm2; moderate (MVOA 1.0–1.5 cm2) and mild MS (MVOA >1.5 cm2) were nearly equal in frequency (27.6% and 25.2% respectively) (Fig. 4).
Fig. 4.
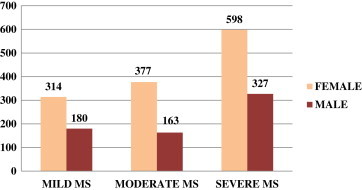
Distribution of cases across the three severities of MS (MS = Mitral Stenosis).
3.1.2. Pulmonary hypertension
The distribution of cases with pulmonary hypertension is shown in Fig. 5. Pulmonary hypertension was identified in more than half of isolated MS cases (57.6%). More than two-thirds (68.9%) of patients in whom pulmonary hypertension was diagnosed were women. It can be seen from the figure that the incidence of pulmonary hypertension was in proportion to the severity of MS (10.4% of mild MS, 27.9% of moderate MS, and 61.7% of severe MS respectively).
Fig. 5.
Distribution of cases with pulmonary hypertension (MS = Mitral Stenosis).
3.2. Isolated MR
MR occurred as an isolated lesion in 25.6% of all the cases making it the most common isolated valve lesion. The predominant form of MR was rheumatic (41.1%) followed closely by myxomatous or mitral valve prolapse (40.8%) (Fig. 6). Isolated MR was seen more often in females in all the three categories of disease. In the rheumatic group, peak incidence of MR was in the second decade (28.8%) which was in contrast to MS, where peak incidence was in the fourth decade (27.9%). A bimodal peak was seen in the incidence of MR due to mitral valve prolapse (MVP). First peak was in the second decade (18.8%) and the second in older adult life (fifth decade; 15.9%).
Fig. 6.
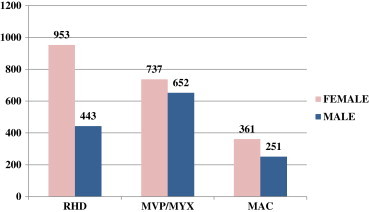
Incidence of various etiologies of isolated mitral regurgitation (MAC = Mitral Annular Calcification, MVP/MYX = Mitral Valve Prolapse/Myxomatous mitral valve, RHD = Rheumatic Heart Disease).
3.3. Isolated aortic stenosis (AS)
Isolated AS was the third most common valve lesion among the 13,289 cases (7.3%). The age and etiology-wise distribution of cases is shown in Fig. 7. Degenerative calcification was the commonest cause of isolated AS (65.0%) followed by bicuspid aortic valve (BAV) (33.9%). RHD contributed a minority of cases to this valve lesion (1.1%). Associations of bicuspid AS included Coarctation of Aorta, supravalvular AS, supramitral ring and hypoplastic arch/left ventricle. It was interesting to note that isolated AS was more common in males in all the three groups (male:female ratio 1.5–2.1:1, overall ratio being 1.7:1).
Fig. 7.

Age and Etiology-wise distribution of cases of isolated aortic stenosis.
3.4. Isolated aortic regurgitation
Isolated AR was seen in 774 cases (5.8%) making it the fourth most common lesion. Etiology and Sex-specific distribution of cases is shown in Fig. 8. As can be seen in the diagram, RHD was the commonest cause of isolated AR in the present study followed by bicuspid aortic valve and AR associated with other congenital heart diseases, which included Tetralogy of Fallot, ventricular septal defect, patent ductus arteriosus and complete transposition of great arteries.
Fig. 8.
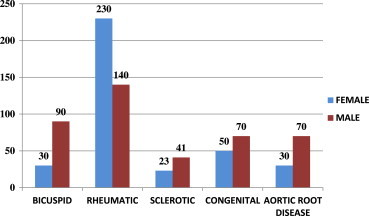
Etiology and Sex-specific distribution of cases of isolated aortic regurgitation.
3.5. Mutivalvular disease
Multiple valves were involved in more than a third of all cases (36.8%). The anatomic and hemodynamic combinations of lesions were analyzed systematically. The results are as summarized in Fig. 9 and Table 2. Overall, the combination of MS and MR (MS + MR) was the commonest followed by the combination of MS and AR (MS + AR). The least common lesion combination was that of MS and AS (MS + AS). Multivalvular disease was seen more often in females in a ratio of 1.2:1. It was also observed that lesion combinations involving MS were commoner in females while all AS involving combinations were more common in males. In Rheumatic heart disease, the combinations were in the following order of involvement: MS + MR (46.6%) > MS + AR (26.5%) > MR + AR (23.3%) > MS + AS (2.4%) > MR + AS (0.9%) > AS + AR (0.3%).
Fig. 9.
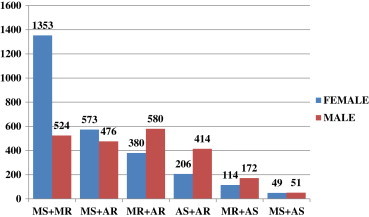
Patterns of anatomic/hemodynamic combinations of valve lesions (Abbreviations are as used in Fig. 2).
Table 2.
Systematic, etiology-specific analysis of various combinations of lesions (AR = Aortic Regurgitation, AS = Aortic Stenosis, MR = Mitral Regurgitation, MS = Mitral Stenosis, TR = Tricuspid Regurgitation, TS = Tricuspid Stenosis).
| Combination | Congenital | Rheumatic | Degenerative | Post-surgical | Total |
|---|---|---|---|---|---|
| MS + MR | 17 (0.9)a | 1835 (97.8) | 11 (0.6) | 14 (0.7)b | 1877 (38.4) |
| MS + AR | 0 (0) | 1046 (99.7) | 3 (0.3) | 0 (0) | 1049 (21.4) |
| MR + AR | 0 (0) | 918 (95.6) | 42 (4.4)c | 0 (0) | 960 (19.6) |
| AS + AR | 70 (11.3)d | 12 (1.9) | 538 (86.8) | 0 (0) | 620 (12.7) |
| MR + AS | 26 (9.1)e | 34 (11.9) | 226 (79.0) | 0 (0) | 286 (5.7) |
| MS + AS | 0 (0) | 96 (96) | 4 (4) | 0 (0) | 100 (2.0) |
| Total | 113 (2.3) | 3941 (80.6) | 824 (16.8) | 14 (0.3) | 4892 |
Includes parachute mitral valve (MV) and the combination seen in dextrocardia and atrial septal defect.
Includes post-MV repair status.
Includes myxomatous MV, sclerotic aortic valve (AV), calcific MV and AV.
BAV.
Includes BAV.
3.6. Organic tricuspid valve disease
Since tricuspid valve disease was found most often in combination with other valve disease, especially mitral, the patterns of involvement of tricuspid valve were analyzed separately. Overall, 9.7% of cases had organic involvement of tricuspid valve.
3.6.1. Tricuspid stenosis
Tricuspid stenosis (TS) is a rare lesion (0.3% of all valvular lesions) occurring predominantly in association with mitral stenosis. More than 90% of the cases were seen in RHD. The patterns of involvement are shown in Table 3.
Table 3.
Tricuspid Stenosis (AS = Aortic Stenosis, MR = Mitral Regurgitation, MS = Mitral Stenosis, RA = Right Atrial, TR = Tricuspid Regurgitation, TS = Tricuspid Stenosis).
| Etiology | Female | Male | Total | Associations |
|---|---|---|---|---|
| Rheumatic | 30 | 7 | 37 (90.4) | Almost exclusively seen in association with MS; only 1 case seen in a patient with pure MR. |
| Ebstein's anomaly | 1 | 0 | 1 (2.4) | – |
| Post-tricuspid valve repair | 1 | 0 | 1 (2.4) | Moderate TR |
| Glycogen storage disease | 0 | 1 | 1 (2.4) | MS + AS (all Mild) |
| RA mass/myxoma | 0 | 1 | 1 (2.4) | TS |
| Total | 32 (78.1) | 9 (21.9) | 41 | – |
3.6.2. Tricuspid regurgitation
Tricuspid regurgitation due to primary involvement of the tricuspid valve constituted only a minority of the total number of TR cases (4.7%) which includes functional as well as physiological TR seen across various spectra of heart diseases. The most common cause was RHD (70.2%). Females were more likely to have TR in all the etiological groups. All cases of tricuspid valve prolapse (TVP) were seen in patients who had mitral valve prolapse. Conversely, 6% of MVP cases had associated TVP. The distribution of TR cases is shown in Fig. 10.
Fig. 10.
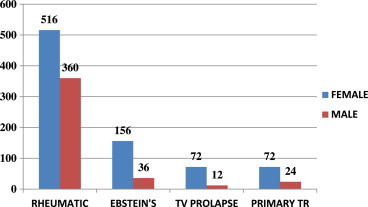
Distribution of Tricuspid Regurgitation cases (TR = Tricuspid Regurgitation, TV = Tricuspid Valve).
3.7. Pulmonary valve
Three cases of pulmonary stenosis were seen in rheumatic heart disease group. All 3 cases had associated MS. One patient had combined stenosis of mitral, tricuspid and pulmonary valves.
4. Discussion
The present study was undertaken in a tertiary care high-volume cardiac center in South India with the objective of systematically analyzing the large volume of echocardiographic data on valvular heart disease that is stored in the Echo laboratory. To the best of our knowledge, this is the largest study of echocardiographic patterns of valvular heart disease done in a single center. Echo now plays the dominant role in the evaluation of the anatomic and hemodynamic effects of valve lesions. This has almost obviated the need for invasive cardiac catheterization in the management of valvular heart disease. Echo is now the single most important modality of investigation in the diagnosis, management and follow up of patients with valvular heart disease. The superiority of Echo over clinical examination in identifying subclinical rheumatic heart disease has been conclusively shown in various school surveys done across India.11,12 This may result in more children receiving secondary prophylaxis for rheumatic fever thus reducing the burden of established rheumatic heart disease.
Rheumatic heart disease contributed the most to the burden of valvular heart disease (64.3%) in the present study. RHD continues to affect millions of children and young adults in the Indian subcontinent with prevalence rates varying from 4.54 to 6 per 100013,14 with estimates as high as 51 per 1000 in some studies,11 although some recent large series of school surveys have shown a decline in the prevalence of RHD (0.5–0.68 per 1000).15,16 Our results are in contrast to another echocardiographic study of valvular heart disease, the Euro Heart Survey,17 a multicenter study involving 5001 patients from 92 centers in 25 European countries. The most common lesions were AS and MR, mostly of degenerative etiology. This difference conforms to the differing prevalence of valve disease among the developed and the developing nations. The order of involvement of valve lesions in RHD in the current study was mitral, aortic, tricuspid and pulmonary. This reflects the pathological involvement of the cardiac valves in acute rheumatic fever with mitral being the most common and pulmonary, the least.18
Mitral stenosis was almost exclusively of rheumatic etiology (97.4%) in the current study. Surgical pathologic series show rheumatic involvement in almost 99% of excised stenotic valves5,19 similar to the results of the large necropsy series of Roberts WC (100%).2 Congenital MS, seen in <1% of cases is rare in adults, given that the median age at death is only 2 months.20 Degenerative calcification of the mitral annulus often causes MR, but rarely can cause stenosis of the mitral valve in <3% of cases.21
MR was the most common isolated valve lesion. Rheumatic involvement constituted the dominant cause followed closely by myxomatous or mitral valve prolapse, similar to the surgical series of Olson5 (31% and 38% respectively) and Duren7 (40% and 33% respectively). The peak incidence of rheumatic MR was two decades earlier than that of MS. This is explained by the fact that a long latent period following the acute attack of rheumatic fever generally exists before the stenotic mitral lesion manifests clinically.22 In the present study, MR was much more common than MS in the pediatric age group (<19 years) whereas in adults ≥20 years, MS was twice as common as MR.
Calcific degeneration was the predominant etiology of isolated aortic stenosis whereas rheumatic etiology dominated the isolated AR cases. In three surgical series from 1965 through 1990,23–25 a changing pattern of aortic stenosis pathology can be noted, with degenerative disease now being the most common cause of AS. RHD was the commonest cause of isolated AR in the older surgical series of Mayo clinic,26 but in the recent series,25 aortic dilatation and/or degenerative valve changes were responsible for half the cases.
Bicuspid aortic valve was well represented in the present study. Out of 547 cases, 357 (65.3%) had pure AS, 120 cases (21.9%) had pure AR and the rest had combined AS and AR (12.8%). This is comparable to the natural history autopsy series of 85 cases by Roberts.3 72% of bicuspid valves had developed stenosis while 13% had pure AR in that study.
Anatomic or hemodynamic combinations of lesions (multivalvular disease) were fairly common in this study occurring in more than a third of cases. An important observation of our study was the differing incidence of mitral and aortic valve combinations in the pediatric (≤19 years) and adult (≥20 years) age groups. While MR + AR was commoner than MS + AR in the pediatric age group, the reverse was true in the adult age group reflecting the natural progression of valve lesions following an attack of acute rheumatic fever. In a study of 100 cases of combined aortic and mitral valve replacement, Melvin found that MR + AR was the most common combination of rheumatic valvular lesions.27 In a series of 150 patients with combined aortic and mitral valve disease, only 10 patients (6.7%) were found to have essentially pure AS and MS28; we found a slightly lower incidence of 4.2% for this combination in a similar analysis.
The commonest etiology of TS was RHD and was almost exclusively seen in association with MS. In the necropsy series of Roberts and Virmani,4 though 12% of cases had some pathological involvement of tricuspid valve, stenosis of the valve was seen in only 2% and was seen only when associated MS and AS were present. In a surgical pathology series of tricuspid valve disease, RHD was the commonest cause of pure TR followed by Ebstein's anomaly (41 and 14% respectively)8; the corresponding figures in our study were 70.2 and 15.4%.
5. Limitations of the study
-
a.
The present study is not a population based study and hence subject to several biases inherent in such studies. For example, symptomatic lesions are more likely to be represented in a study based in a tertiary referral center.
-
b.
There may be a bias towards the severity patterns of lesions as patients with more severe lesions likely to be over-represented in studies conducted in tertiary care referral centers.
-
c.
Although strict morphologic and clinical criteria were used to ascribe etiology to a particular valve lesion, an Echo based study has inherent limitations in comparison to surgical or autopsy based studies.
6. Conclusions
RHD contributed most to the burden of VHD in the present study with calcific degeneration, myxomatous disease and BAV being the other major forms of VHD. Multiple valves were affected in more than a third of all cases. The current study, done in a high volume tertiary care cardiac center, is the largest of its kind and can be thought to reflect the current incidence and patterns of valvular heart disease. Although recent school surveys in India continue to demonstrate a declining trend in the prevalence of RHD, rheumatic involvement is still the dominant form of valvular heart disease in India. The patterns described correlate well with the surgical and autopsy series described over several decades. This was a comprehensive evaluation of valvular heart disease across all the age groups and gender and hence an understanding of natural history can be retrospectively inferred. With the advances in techniques and increasing experience of the operators, Echo has nearly obviated the need for invasive cardiac catheterization for the anatomic and hemodynamic assessment of valve lesions. Echocardiography is now the single most important modality of evaluation for the management of patients with valvular heart disease.
Conflicts of interest
All authors have none to declare.
References
- 1.Carapetis J.R. Rheumatic heart disease in developing countries. N Engl J Med. 2007;357:439–441. doi: 10.1056/NEJMp078039. [DOI] [PubMed] [Google Scholar]
- 2.Roberts W.C. Morphologic features of the normal and abnormal mitral valve. Am J Cardiol. 1983;51:1005–1028. doi: 10.1016/s0002-9149(83)80181-7. [DOI] [PubMed] [Google Scholar]
- 3.Roberts W.C. The congenitally bicuspid aortic valve: a study of 85 autopsy cases. Am J Cardiol. 1970;26:72–83. doi: 10.1016/0002-9149(70)90761-7. [DOI] [PubMed] [Google Scholar]
- 4.Roberts W.C., Virmani R. Aschoff bodies at necropsy in valvular heart disease. Circulation. 1977;57:803–807. doi: 10.1161/01.cir.57.4.803. [DOI] [PubMed] [Google Scholar]
- 5.Olson L.J., Subramanian R., Ackermann D.M. Surgical pathology of the mitral valve: a study of 712 cases spanning 21 years. Mayo Clin Proc. 1987;62:22–34. doi: 10.1016/s0025-6196(12)61522-5. [DOI] [PubMed] [Google Scholar]
- 6.Dare A.J., Harrity P.J., Tazelaar H.D. Evaluation of surgically excised mitral valves: revised recommendations based on changing operative procedures in the 1990s. Hum Pathol. 1993;24:1286–1293. doi: 10.1016/0046-8177(93)90261-e. [DOI] [PubMed] [Google Scholar]
- 7.Duren D.R., Becker A.E., Dunning A.J. Long-term follow-up of idiopathic mitral valve prolapse in 300 patients: a prospective study. J Am Coll Cardiol. 1988;11:42–47. doi: 10.1016/0735-1097(88)90164-7. [DOI] [PubMed] [Google Scholar]
- 8.Hauck A.J., Freeman D.P., Ackermann D.M. Surgical pathology of the tricuspid valve: a study of 363 cases spanning 25 years. Mayo Clin Proc. 1988;63:851–863. doi: 10.1016/s0025-6196(12)62687-1. [DOI] [PubMed] [Google Scholar]
- 9.Singh J.P., Evans J.C., Levy D. Prevalence and clinical determinants of mitral, tricuspid, and aortic regurgitation (the Framingham Heart Study) Am J Cardiol. 1999;83:897–902. doi: 10.1016/s0002-9149(98)01064-9. [DOI] [PubMed] [Google Scholar]
- 10.Shah P.M., Raney A.A. Tricuspid valve disease. Curr Probl Cardiol. 2008;33:47–84. doi: 10.1016/j.cpcardiol.2007.10.004. [DOI] [PubMed] [Google Scholar]
- 11.Bhaya Maneesha, Panwar Sadiak, Beniwal Rajesh. High prevalence of rheumatic heart disease detected by echocardiography in school children. Echocardiography. 2010;27:448–453. doi: 10.1111/j.1540-8175.2009.01055.x. [DOI] [PubMed] [Google Scholar]
- 12.Saxena Anita, Ramakrishnan Sivasubramanian, Roy Ambuj. Prevalence and outcome of subclinical rheumatic heart disease in India: the RHEUMATIC (Rheumatic Heart Echo Utilisation and Monitoring Actuarial Trends in Indian Children) study. Heart. 2011;97:2018–2022. doi: 10.1136/heartjnl-2011-300792. [DOI] [PubMed] [Google Scholar]
- 13.Lalchandani A., Kumar H.R.P., Alam S.M. Prevalence of rheumatic fever and rheumatic heart disease in rural and urban school children of district Kanpur. Indian Heart J. 2000;52:672. [Google Scholar]
- 14.Padmavati S. Rheumatic fever and rheumatic heart disease in India at the turn of the century. Indian Heart J. 2001;53:35–37. [PubMed] [Google Scholar]
- 15.Misra M., Mittal M., Singh R. Prevalence of rheumatic heart disease in school-going children of eastern Uttar Pradesh. Indian Heart J. 2007;59:42–43. [PubMed] [Google Scholar]
- 16.Jose V. Jacob, Gomathi M. Declining prevalence of rheumatic heart disease in rural schoolchildren in India: 2001–2002. Indian Heart J. 2003;55:158–160. [PubMed] [Google Scholar]
- 17.Iung B., Baron G., Tornos P. Valvular heart disease in the community: a European experience. Curr Probl Cardiol. 2007;32:609–661. doi: 10.1016/j.cpcardiol.2007.07.002. [DOI] [PubMed] [Google Scholar]
- 18.Chandrashekhar Y., Narula Jagat. Rheumatic fever. In: Alpert Joseph S., editor. Valvular Heart Disease. 3rd ed. Lippincott Williams and Wilkins; Philadelphia: 2000. pp. 46–48. [Google Scholar]
- 19.Hanson T.P., Edwards B.S., Edwards J.E. Pathology of surgically excised mitral valves: one hundred consecutive cases. Arch Pathol Lab Med. 1985;109:823–828. [PubMed] [Google Scholar]
- 20.Ruckman R.N., Van Praagh R. Anatomic types of congenital mitral stenosis: report of 49 autopsy cases with consideration of diagnosis and surgical implications. Am J Cardiol. 1978;42:592–601. doi: 10.1016/0002-9149(78)90629-x. [DOI] [PubMed] [Google Scholar]
- 21.Hammer W.J., Roberts W.C., deLeon A.C. “Mitral stenosis” secondary to combined “massive” mitral anular calcific deposits and small, hypertrophied left ventricles: Hemodynamic documentation in four patients. Am J Med. 1978;64:371–376. doi: 10.1016/0002-9343(78)90214-0. [DOI] [PubMed] [Google Scholar]
- 22.Wood P. An appreciation of mitral stenosis. Part I. Clinical features. Br Med J. 1954;1:1051. doi: 10.1136/bmj.1.4870.1051. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Subramanian R., Olson L.J., Edwards W.D. Surgical pathology of pure aortic stenosis: a study of 374 cases. Mayo Clin Proc. 1984;59:683. doi: 10.1016/s0025-6196(12)62057-6. [DOI] [PubMed] [Google Scholar]
- 24.Peterson M.D., Roach R.M., Edwards J.E. Types of aortic stenosis in surgically removed valves. Arch Pathol Lab Med. 1985;109:829–832. [PubMed] [Google Scholar]
- 25.Dare A.J., Veinot J.P., Edwards W.D. New observations on the etiology of aortic valve disease: a surgical pathologic study of 236 cases from 1990. Hum Pathol. 1993;24:1330–1338. doi: 10.1016/0046-8177(93)90267-k. [DOI] [PubMed] [Google Scholar]
- 26.Olson L.J., Subramanian R., Edwards W.D. Surgical pathology of pure aortic regurgitation: a study of 225 cases. Mayo Clin Proc. 1984;59:835–841. doi: 10.1016/s0025-6196(12)65618-3. [DOI] [PubMed] [Google Scholar]
- 27.Melvin D.B., Tecklenberg P.L., Hollingsworth J.F. Computer-based analysis of preoperative and postoperative prognostic factors in 100 patients with combined aortic and mitral valve replacement. Circulation. 1973;48(suppl III):56–62. doi: 10.1161/01.cir.48.1s3.iii-56. [DOI] [PubMed] [Google Scholar]
- 28.Zitnik R.S., Piemme T.E., Messer R.J. The masking of aortic stenosis by mitral stenosis. Am Heart J. 1965;69:22. doi: 10.1016/0002-8703(65)90212-7. [DOI] [PubMed] [Google Scholar]