

Abstract
Coronary artery anomalies are found in 1–5% of all coronary angiograms. Single coronary artery is a rare congenital anomaly. The prevalence of the anomaly is 0.024–0.066% of the general population and percutaneous coronary intervention in this anomaly is performed infrequently. The highest incidence of this condition is reported from India. We report a case of a 55 year old patient of anterior wall ST elevation myocardial infarction with L1 group of single coronary artery who underwent successful angioplasty and stenting to left anterior descending artery. The unique features and inherent risks of percutaneous coronary intervention to single coronary artery are discussed.
Keywords: Single coronary artery, Myocardial infarction, Percutaneous coronary intervention
1. Introduction
A single coronary artery (SCA) is a rare congenital anomaly. Reports of SCA with acute myocardial infarction (AMI) are sparse and percutaneous coronary intervention (PCI) in such situations are not only few in number but also technically challenging and potentially catastrophic. We report a case of L1 variety of SCA with anterior wall AMI with successful PCI to left anterior descending artery (LAD).
2. Case report
A 55 year old male presented to our hospital with history of chest pain for past 3 days. He was a chronic smoker, non diabetic and non hypertensive. His family history was unremarkable. At admission, his heart rate was 100 bpm and BP was 110/80 mm Hg. ECG showed ST elevation in lead I, aVL, V1–V6 with complete RBBB. Echocardiogram showed hypokinesia of the anterior wall with an ejection fraction of 40%. Coronary angiography (Fig. 1) was performed using the traditional Judkin's method angiography of left coronary artery revealed a normal left main coronary artery (LMCA) which divided into LAD and left circumflex artery (LCx). The LAD was occluded in the mid portion. The LCX was a dominant vessel which coursed within the left atrioventricular groove, crossed the crux of the heart and continued in the right atrioventricular groove as the right coronary artery (RCA). Attempts to engage the right coronary catheter to the right coronary ostium were futile and aortography (Fig. 2) displayed the absence of the right coronary ostium. CT coronary angiography (Fig. 3) confirmed the presence of single coronary artery with LCx continuing in the course of the RCA. The patient was subjected to percutaneous coronary intervention. Left main coronary artery was engaged with LAUNCHER 6F guide catheter. The lesion was crossed with a balanced middle weight soft guide wire and it was stented with a drug eluting stent with subsequent TIMI 3 flow distally (Fig. 4). The patient had an uneventful course after the intervention and was discharged in stable condition after 3 days.
Fig. 1.
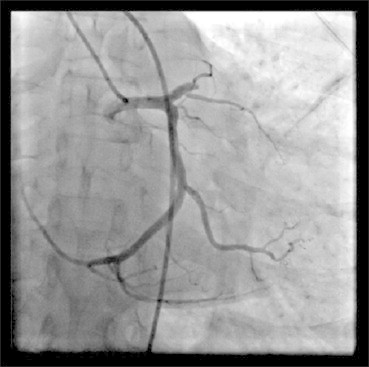
Angio 1 – angiography showing LMCA origin & its course.
Fig. 2.

Angio 2 – aortogram showing single coronary artery.
Fig. 3.

CT Angio 2 – CT angiography showing single coronary artery.
Fig. 4.

Post PCI Angio – angiography showing recanalization of LAD.
3. Discussion
Coronary anomalies may occur in 1% to 5% of patients undergoing coronary arteriography.1 An isolated single coronary artery is a solitary coronary vessel arising from the ascending aorta, giving rise to the major coronary branches and thus nourishing the entire heart. In effect, both the right coronary artery and the left main coronary artery arise from a single aortic sinus.2 The They are seen in 0.3% to 1.3% of patients undergoing coronary angiography1 and in 0.17% of routine autopsy studies. In the younger age groups, they may be responsible for 4% to 15% of cases of sudden death.3,4 The prevalence of this anomaly is 0.024 to 0.066% in the general population.5 They reportedly constitute <3% of all coronary anomalies.6 The highest incidence (i.e. 8.8% of all coronary anomalies) was reported from India.7 Shirani and Roberts reviewed the literature and reported 97 cases of this anomaly, 46 and 51 originating from the left and right sinus of Valsalva respectively.8 Prognosis for patients with this anomaly varies from excellent with normal life expectancy to sudden death depending on the course and the presence and severity of atherosclerosis.
Isolated Single coronary artery was classified in 3 groups in 1979 by Lipton et al9 The anomalous coronary artery is first designated as “R” or “L” depending upon whether the ostium is located in the right or left sinus of Valsalva. It is then designated as group I, II, III. In group I, either a single coronary artery courses as the right coronary or circumflex artery and finally continues as the left anterior descending artery, or a single left main coronary artery gives off two branches as the left anterior descending and circumflex artery and right coronary artery is formed by the extension of the circumflex across the crux. In group II, the anomalous artery arises from the proximal part of normal right or left coronary artery and cross the base of the heart before assuming its normal position. Group III describes the anomaly where the left anterior descending and circumflex artery arise separately from the proximal part of the normal right coronary artery. The final designation refers to the relationship between the anomalous coronary artery and the aorta and pulmonary artery. The letters “A”, “B”, and “P” refer to “anterior”, “between”, and “posterior” patterns. In 1990, Yamanaka and Hobbs modified the Lipton et al classification by adding “septal” (S) and “combined” (C) types. The present case, as per Lipton's classification, belongs to the L1 group of single coronary artery anomaly. The L1 group has an incidence of 0–0.035% and constitutes 1.2% of all coronary anomalies.9 Chou et al10 reviewed 11 previous cases and reported one case of L1 group. Other than this, a handful of case reports are available, none of which had obstructive coronary artery disease. Regarding prognosis, Yamanaka et al6 stated that it has a benign clinical course but Chou et al10 reported that 33% of these patients required CABG. Moreover, if the artery courses within the aortic wall or between the aorta and pulmonary artery, intussusception of the ectopic proximal vessel may occur and can cause myocardial ischemia.
The coexistence of Single coronary artery with acute myocardial infarction is even rarer. Gur et al11 and Giorgi et al12 have reported cases of it, all of the R subgroup. Takano13 et al reported acute myocardial infarction in a patient where the right coronary artery was a branch of the mid left anterior descending artery.
Previous reports of coronary intervention in a patient of LI subgroup are anecdotal. Quintal et al14 reviewed 18 cases of it. The single ostium was in the left sinus of Valsalva in 8 patients of which the artery addressed during intervention was left anterior descending artery in 3 patients, right coronary artery in 3 patients and circumflex artery in 2 patients. Gambhir et al15 reported intervention in RII subgroup of this anomaly. Takano's case (described earlier) underwent intervention to left anterior descending artery. Wiliams16 et al described emergent PCI to the LAD in a patient with LII subtype of SCA. Kafkas17 reported the first case of successful intervention in L1 variety wherein the LAD was stented in a patient of acute coronary syndrome. Nasir18 reported primary PCI in a patient of L1 subtype with anterior wall STEMI. To the best of our knowledge, this is the second case of PCI in STEMI in a patient with L1 subtype of SCA.
A few pertinent points must be kept in mind while performing PCI in a SCA. Firstly, delineation of the anatomy of anomalous arteries is mandatory before planning interventions, to identify other mechanisms of myocardial ischemia (e.g. vascular compression) and to choose the appropriate treatment (medical, PCI or surgical). Coronary CT angiography is helpful in this regard. Secondly, the risks associated with PCI of a single coronary artery is similar to PCI of unprotected left main because dissection of the single ostium by guide catheter can be lethal and occlusion of the site of dilatation due to dissection or thrombus can put sizeable myocardium in jeopardy. Thirdly, the guiding catheter should correspond to the sinus of origin rather than the artery to be addressed and is usually the same configuration as that used during diagnostic angiography. If the artery to be dilated has an abnormal course, good coaxial guide support is imperative and the guiding catheter must be accordingly chosen.
4. Conclusion
Therefore described case is a rare instance of a patient with SCA (L1 group) with STEMI undergoing PCI to the LAD. To the best of our knowledge, this is the second such case in the world and the first from India. PCI in SCA has its unique risks but with improving technology and expertise is likely to be performed more frequently and successfully in the future.
Conflicts of interest
All authors have none to declare.
References
- 1.Angelini P., Velasco J.A., Flamm S. Coronary anomalies: incidence, pathophysiology, and clinical relevance. Circulation. 2002;105:2449–2454. doi: 10.1161/01.cir.0000016175.49835.57. [DOI] [PubMed] [Google Scholar]
- 2.Canbay A., Özcan Ö., Aydogdu S., Diker E. Single coronary artery anomaly: a report of three cases. Türk Kardiyol Dern Arş. 2008;36:473–475. [PubMed] [Google Scholar]
- 3.Alexander R.W., Griggith G.C. Anomalies of the coronary arteries and their clinical significance. Circulation. 1956;14:800–805. doi: 10.1161/01.cir.14.5.800. [DOI] [PubMed] [Google Scholar]
- 4.Arteaga R.B., Tronolone J., Mandawat M. Single coronary ostium–a right coronary artery arising from the left main coronary artery. J Invasive Cardiol. 2006;18:E241–E243. [PubMed] [Google Scholar]
- 5.Desmet W., Vanhaecke J., Vrolix M. Isolated single coronary artery: a review of 50,000 consecutive coronary angiographies. Eur Heart J. 1992;13:1637–1640. doi: 10.1093/oxfordjournals.eurheartj.a060117. [DOI] [PubMed] [Google Scholar]
- 6.Yamanaka O., Hobbs R.E. Coronary artery anomalies in 126,595 patients undergoing coronary arteriography. Cathet Cardiovasc Diagn. 1990;21:28–40. doi: 10.1002/ccd.1810210110. [DOI] [PubMed] [Google Scholar]
- 7.Harikrishnan S., Jacob S.P., Tharakan J. Congenital coronary anomalies of origin and distribution in adults: a coronary arteriographic study. Indian Heart J. 2002;54:271–275. [PubMed] [Google Scholar]
- 8.Shirani J., Roberts W.C. Solitary coronary ostium in the aorta in the absence of other major congenital cardiovascular anomalies. J Am Coll Cardiol. 1993:2137–2143. doi: 10.1016/0735-1097(93)90728-j. [DOI] [PubMed] [Google Scholar]
- 9.Lipton M.J., Barry W.H., Obrez I., Silverman J.F., Wexler L. Isolated single coronary artery: diagnosis, angiographic classification, and clinical significance. Radiology. 1979;130:39–47. doi: 10.1148/130.1.39. [DOI] [PubMed] [Google Scholar]
- 10.Chou L.P., Kao C., Lee M.C., Lin S.L. Right coronary artery originating from distal left circumflex artery in a patient with an unusual type of isolated single coronary artery. Jpn Heart J. 2004;45:337–342. doi: 10.1536/jhj.45.337. [DOI] [PubMed] [Google Scholar]
- 11.Gür M., Yıldız A., Demirbağ R., Yılmaz R. Isolated single coronary artery originating from a single right coronary ostium in a patient with acute myocardial infarction. Arch Turk Soc Cardiol. 2006;34:173–176. [Google Scholar]
- 12.Giorgi B., Dymarkowski S., Rademakers F.E., Lebrun F., Bogaert J. Single coronary artery as cause of acute myocardial infarction in a 12-year-old girl: a comprehensive approach with MR imaging. AJR. 2002;179:1535–1537. doi: 10.2214/ajr.179.6.1791535. [DOI] [PubMed] [Google Scholar]
- 13.Takano M., Seimiya K., Yokoyama S. Unique single coronary artery with acute myocardial infarction: observation of the culprit lesions by intravascular ultrasound and coronary angioscopy. Jpn Heart J. 2003;44:271–276. doi: 10.1536/jhj.44.271. [DOI] [PubMed] [Google Scholar]
- 14.Quintal R., Nguyen T., Glancy L.D. Successful percutaneous coronary angioplasty via solitary ostium in the aorta (single coronary artery) J Invasive Cardiol. 2003;8:446–447. [PubMed] [Google Scholar]
- 15.Gambhir D.S., Singh S., Bharadwaj S., Arora R. Rotablation and elective stenting of stenosis in the left anterior descending coronary artery arising from an anomalous single coronary artery. Indian Heart J. 2000;52:459–460. [PubMed] [Google Scholar]
- 16.Wuilliams P.D., Bury R.W., Brack M.J. Emergency percutaneous coronary intervention in the setting of a single left coronary ostium. Circ Cardiovasc Interv. 2009;2:149–151. doi: 10.1161/CIRCINTERVENTIONS.109.851642. [DOI] [PubMed] [Google Scholar]
- 17.Kafkas N., Triantafyllou K., Babalis D. An isolated single L-I type coronary artery with severe LAD lesions treated by transradial PCI. J Invasive Cardiol. 2011;23:E216–E218. [PubMed] [Google Scholar]
- 18.Nasir J.M., Hawkins K., Patino G., Furgerson J., Soh E.K. Anterior ST-segment elevation myocardial infarction in a patient with an L-I type single coronary artery. J Am Coll Cardiol Intv. 2012;5:e9–e10. doi: 10.1016/j.jcin.2011.09.030. [DOI] [PubMed] [Google Scholar]