

Abstract
Background:
Dental fear, anxiety and phobia have consistently been reported as widespread problems that persist despite the technological advances that have made dentistry less painful and less uncomfortable. The aim of this study was to assess the prevalence of dental anxiety (DA) and its relation to age and sex among Coastal Andhra (Visakhapatnam) population.
Materials and Methods:
A randomized controlled study was designed among 340 individuals at GITAM Dental College and Hospital, Visakhapatnam. The sample for the study consisted of 180 female and 160 male subjects between 15 and 65 years of age; all were supplied with two questionnaires (Corah DA scale [CDAS] and Clarke and Rustvold dental concerns assessment scale describing anxiety provoking stimuli. The Mann-Whitney U-test and the Kruskal-Wallis test were applied (significance level P < 0.05). The correlations between the two questionnaires were calculated using the Spearman's rank correlation coefficient.
Results:
Two questionnaires were collected from all 340 individuals and the Indian translation of both instruments was found to be internally reliable with a Cronbach's alpha of 0.093. Overall prevalence of DA was high (77.4%) but severe (22.6%) anxiety (phobia) was low. Kruskal-Wallis test showed a significant relation between age and DA. The mean CDAS scores were high in 25-35 (11.08) and low in 55-65 (9.45) year age groups. Mann-Whitney U test showed significant relation between sex and DA. Mean CDAS score levels were significantly higher in females (10.88) than in males (9.96) (P < 0.0001).
Conclusion:
Patients anxious about dental procedures are often more difficult to treat. If Dentists become aware about the level of DA among their patients, they can anticipate patient's behavior and can be prepared to take behavioral/pharmacological measures to reduce anxiety levels.
Keywords: Dental anxiety, dental anxiety scale, dental concerns assessment scale, dental fear, prevalence
INTRODUCTION
In general, anxiety is expressed as imaginary threat about unknown and unfamiliar process. Furthermore anxiety is described as a vague, unpleasant feeling accompanied by the premonition that something undesirable is going to happen. It is a reaction to a perceived danger that is known to the individual. On the other hand, fear is a biological response to a specific threat and is a reaction to a known danger or threat.[1,2] Dental anxiety (DA) is defined as a patient's response to stress that is specific to the dental situation. DA is ranked 5th[3] among common fear situations with about 6-15% of the population suffering from high DA.[4]
It is a significant determinant of whether people will make regular dental visits, a significant barrier to dental care. High degree of fear and anxiety toward dental treatment is an undeniable and unfortunate expression. According to Todd and Walker,[5] nearly, 43% of people reported that they avoided going to Dentist unless they experience trouble with their teeth. Curson and Coplans[6] reported that anxiety contributes to delay in visiting Dentist. DA, a major problem for many adults and children acts as a barrier to treatment by avoiding or attending treatment irregularly or for visiting a Dentist for emergencies only.
The etiology of DA is poorly understood. The onset of DA is thought to originate in childhood, peak in early adulthood, and decline with age.[7] In the investigations of DA since 1960s, the occurrence of DA has been attributed to many factors: Personality characteristics; traumatic or painful dental experiences in childhood; learned attitudes toward dental services that elicit fear from dentally anxious family members or peers (vicarious learning/modeling) perception of body image: Blood-injury fears: Coping styles (vigilant, avoidant and emotion-focused): And pain reactivity.[8,9,10,11] It has been found that Dentist's communicative styles as well as perceived technical competence were predictive of levels of DA during treatment.[12]
DA scale (DAS) developed by Corah (1969) is a well-known accepted tool to measure anxiety among adults. The DAS is a brief, four item questionnaire with a consistent answering scheme for each item ranging from “not anxious” to “extremely anxious.” It is summed together to construct a Likert Scale with a minimum score of 4 and a maximum of 20. It has good psychometric properties, is relatively quick to complete and scoring is easy. This scale is simple to complete, reliable, and valid for evaluating DA.[13,14,15] It has been used in both adults[16,17,18] and children, showing a high internal consistency and test-retest reliability.[19] Existing data suggest that completion of the questionnaire can significantly reduce state anxiety in the practice setting.[20] However Corah DAS (CDAS) has limitations including its focus on only the cognitive dimension of anxiety, limited validity and outdated questions related to the clinician as male and a Dentist.
Many of the studies have been conducted to identify the anxiety provoking stimuli, but they limit because they cover very few of the anxiety provoking stimuli in the dental setting. Hence in the present study, Clarke and Rustvold dental concerns assessment scale (DCAS) revised[21] has been selected for assessing the level of anxiety based on cognitive and behavioral dimensions of DA as it covers most of the anxiety provoking stimuli.
As no published data was available regarding the prevalence of DA for population residing in Visakhapatnam city, this study was purposed to assess the prevalence of DA using two questionnaires among the individuals attending the Oral Medicine and Radiology department of GITAM Dental College and Hospital, in Visakhapatnam., A.P.
Objectives
To assess the prevalence of DA among Coastal Andhra population.
To determine the levels of DA among two genders and in selected population.
To assess levels of anxiety among different age groups in selected population.
To test the reliability and validity of two translated questionnaires.
MATERIALS AND METHODS
Ethical approval was obtained from ethical committee of GITAM Dental College, Visakhapatnam. A representative sample of 340 non-institutionalized adult subjects (aged 15-65 years) was randomly selected from regular Outpatient Department of Dental Hospital. Patients were informed about the study and those, who consented, were included. Patients undergoing psychiatric therapy or were suffering from generalized anxiety disorders were excluded from the study.
Instruments
Two instruments, CDAS (four item) and Clarke and Rustvold DCAS (30 items) were distributed among the subjects in regional language for patient convenience. To establish full congruity between the Telugu and English versions, the Telugu version was back translated into English and tested for inconsistencies. All the 340 individuals were asked to select the option that best represented their experience in the DAS, and the total score was then calculated by summing the values of each selected option.
Clarke and Rustvold DCAS contained 30 items, which assess a broader array of dental stimuli than the CDAS, such as feeling the sound of drill, smelling the dental office, local anesthetic injections and the like. The total possible scores range from 30 to 120. CDAS is a four item questionnaire. Each item is answered on a five point scale and the total possible Score range from 4 to 20. The final assessment of the level of anxiety is given by the sum of points of scale items: Less than 8 is considered as low anxiety, 9-12 is moderate anxiety, 13-14 is high anxiety, and 15-20 is severe anxiety bordering on phobia. On both measures, higher scores refer to high levels of DA.
RESULTS
The data was analyzed by statistical package for the social sciences computer software (SPSS, version 20.0, SPSS Inc., Chicago, IL,USA) using Pearson's Chisquare test, a P < 0.05 was considered to be significant. Mean scores, standard deviation (SD) and internal consistency were calculated for the total sample and gender separately. The translated instrument was tested for internal consistency by Cronbach's alpha, inter-item and item total correlation coefficients. Kruskal-Wallis test was performed to assess the relation between DA scores with different age groups, which showed significant association between them. Mann-Whitney U test was performed to assess the relation between DA scores with sex, which showed significant P value.
Out of the total sample, the majority of patients were females (180) and males (160), divided into five age groups. Most of the participants amongst the five age groups were in the 15-25 year age group (35.9%) followed by 25-35 year age group (30.3%) and least were in the above 55 years age group (6.5%) [Table1].
Table 1.
Distribution of sample according to age, total DCAS scores and total DAS scores in both sex
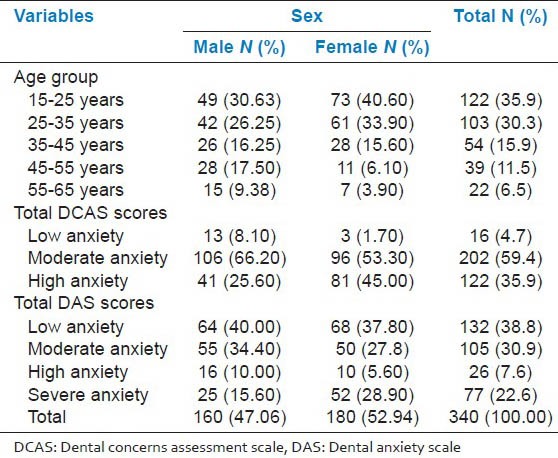
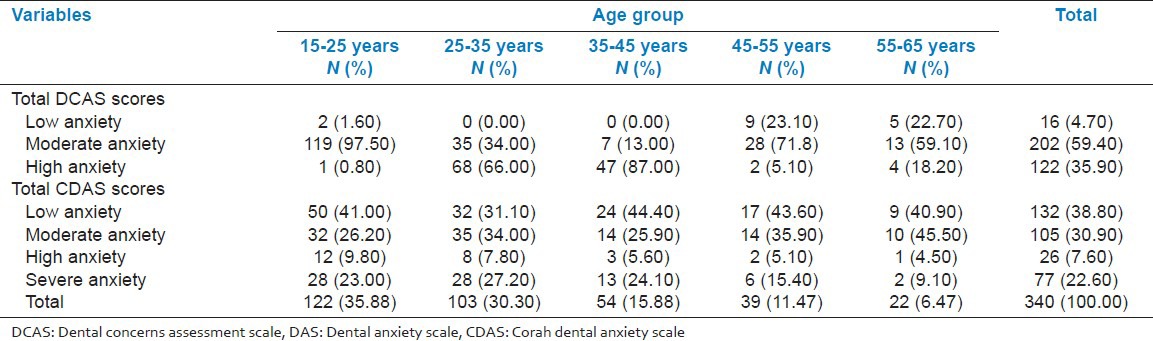
Table 2 presents the prevalence of high and low DA in relation to age group. DCAS showed that 97.5% of the study population belonging to the younger age group, similarly about 71.8% individuals belonging to the 45-55 year age group experienced moderate DA. Anxiety levels were high in individuals belonging to age groups 25-35 (66%) and 35-45 (87%). For CDAS, the individuals with mild (38.8%) and moderate (30.9%) anxiety were high compared with severe anxiety (30.3%) in both males and females. Similarly for DCAS, most of the respondents showed moderate anxiety (59.4%) and followed by severe anxiety (35.9%) [Table 2].
Table 2.
Total DCAS scores and total DAS scores in different age groups
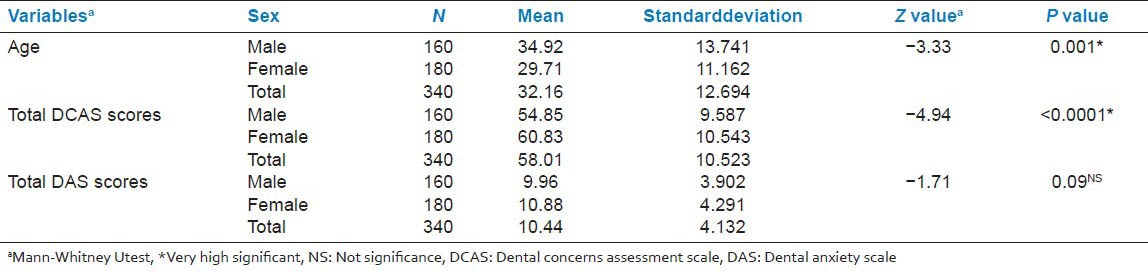
Out of a possible score of 20, the mean score from CDAS in the entire sample was 10.4, with a SD of 4.13 and the mean age of the entire sample was 32.16 years. This value is higher than the mean originally obtained from Corah,[13] which was 8.89 using a total of 1232 undergraduate psychology students and lower from other studies of DA conducted in different countries. The mean ± SD total CDAS score of male participants was 9.96 ± 3.9 and mean age of males was 34.9 years while that of females was 10.8 ± 4.2 and mean age of females was 29.7 years. DCAS had a mean of 58.01 out of a possible score of 90 with a SD of 10.5. The mean ± SD of DCAS total score was seen to be significantly higher in female participants (60.8 ± 10) than male participants (54.8 ± 9.5) [Table 3].
Table 3.
Relationship between total DCAS scores and total DAS scores in sex group (males and females)
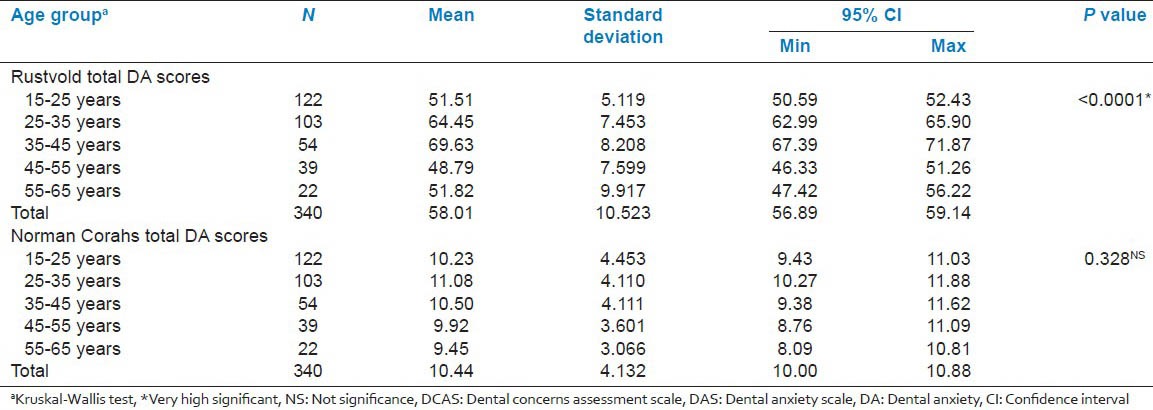
Age factor was also seen to be significantly related to DA. The anxiety levels of younger age groups (15-25 and 25-35 years) were significantly higher than the older age groups (>55 years). For both measures, the anxiety levels of the 55-65 years age group were significantly lower than the other four age groups [Table 4]. This study revealed a significant relationship between age and sex in DA (Chi-square value = 17.50, df = 2, P = 0.002 (0.001 < P < 0.05, high significant)
Table 4.
Total DCAS scores and total DAS scores in different age groups
The Indian translation of the DAS and DCAS were found to be internally reliable with a Cronbach's alpha of 0.093. Validity was demonstrated by a statistically significant correlation between two items with the correlation coefficient of 0.072. Spearman rank correlation was employed, and it revealed that a 0.06 correlation existed between the two instruments, which was not significant at the P > 0.05 level.
DISCUSSION
Despite the technological advances made in modern dentistry, anxiety about dental treatment and fear of pain associated with it remain prevalent. The impact that DA can have on an individual's life is broad and dynamic, leading to the avoidance of dental care and unwanted effects, such as sleep disorders, low self-esteem, and psychological problems. Fear of visiting the Dentist is common, even among adults, and is one of the most important issues for dentists regarding child and adolescent patients. Unlike fear, the feelings of anxiety are often felt when a stimulus or threat is not immediately present or readily identifiable. Gatchel et al.[22] indicated that 70% of patients visiting the Dentist exhibit feelings of apprehension and 15% avoid dental visits due to their anxiety. Other studies have shown more conservative ranges such as 2.6% to 20.4% of the general population exhibiting DA.[8] Overall prevalence of DA in the present study was high (77.4%), but severe (22.6%) anxiety (phobia) was low. This was consistent with the results of other studies,[23,24,25,26] which found a considerably greater percentage of participants with DA. The mean DAS score of selected population (10.4 ± 4.13) was more than the score found by Peretz and Efrat[27] in Israeli population(9.49 ± 3.2) and Israeli kibbutz[28] population (8.98) and Pakistani (8.56 ± 3.59)[29] individuals. In relation to gender, we found that in the selected population, females scored higher on both fear measures, but the statistical analysis revealed no significant difference in this respect between the genders, which has been frequently noted in other studies[30,31,32,33,34,35] of DA. This might be due to cultural differences. The literature shows that women have a lower tolerance to pain and generally report higher levels of anxiety.
The study results showed that the mean anxiety score reduced with increasing age, in agreement with the previous studies.[36,37,38,39] Liddell and Locker[40] suggested that the age dependent decline in DA might be due to the general decline in anxiety with aging and greater exposure to other diseases and their treatment. Studies have shown that fears and phobias decline with age, which could be attributed to age dependent cerebral deterioration, factors like extinction or habituation, and adaptive resignation toward the inevitable.[3,25]
Comparison of the two instruments showed a significant correlation between the anxiety scores. However, significant relation was not found between both the instruments. Overall prevalence of DA is high (77.4%) in the entire sample. The possible reason for the high levels of anxiety can be attributed to the high percentage of young patients who are usually apprehensive. The prevalence of DA was somewhat similar to findings in other countries. However, lack of national data covering a wide range of age groups, differences in measurement and categorization of DA make it difficult to make direct comparisons. Limitations include that the study did not consider the major demographic variables such as education, personality features, socio-cultural factors, annual income, employment, which were found to relate strongly with DA. Of interest in particular for this study was the relationship of age group and gender with the categorization of high versus low/moderate DA.
In this study, we found good evidence for the internal consistencies and reliabilities of translated DASs. The Telugu version of CDAS was shown to be reliable with a Cronbach's alpha value of 0.093. Comparison of the two instruments showed a statistically significant correlation between the anxiety scores. As other authors have commented, the DAS has the advantage of being brief, and therefore may be preferred for clinic purposes. On the other hand, DCAS assesses more stimuli and its increased comprehensiveness may be preferred for research purposes.
It is evident from this study that the Telugu version of DAS is reliable and valid. Construct validity was evident, but needs further evaluation since factors influencing DA have not been established in this population and also very few studies are available at present in the South Indian Telugu speaking population. Assessment of degree of DA helps in taking steps toward Patient's motivation and successful treatment. It might be of value in planning intervention aimed at alleviating DA and in systematic desensitization. These will help the Dentist to accomplish more effective time and patient management. This study has valid applications as DA has important clinical considerations and treatment success depends upon patient compliance. Furthermore, measuring anxiety indirectly measures psychological and social well-being.
CONCLUSION
Individuals with dental fear represent a particularly difficult population to treat and present special challenges to dental staff in terms of the management of care. Patient perceptions of behaviors and attitudes of Dentists can affect DA and could influence his or her decision to access dental care. Significant correlation existed between age and levels of DA as per the analysis of data recorded during the course of this study. The fear and anxiety of an individual could affect the patient-Dentist relationship and the dental treatment plan. Therefore, before starting up with the dental treatment, patient's anxiety and fear levels should be assessed and a proper counseling should be given. However, this study did not focus on the major possible causes for anxiety or the variety of treatments and other factors that may influence anxiety.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Rubin JG, Slovin M, Krochak M. The psychodynamics of dental anxiety and dental phobia. Dent Clin North Am. 1988;32:647–56. [PubMed] [Google Scholar]
- 2.Chadwick BL. Assessing the anxious patient. Dent Update. 2002;29:448–54. doi: 10.12968/denu.2002.29.9.448. [DOI] [PubMed] [Google Scholar]
- 3.Agras S, Sylvester D, Oliveau D. The epidemiology of common fears and phobia. Compr Psychiatry. 1969;10:151–6. doi: 10.1016/0010-440x(69)90022-4. [DOI] [PubMed] [Google Scholar]
- 4.Eli I, Uziel N, Blumensohn R, Baht R. Modulation of dental anxiety — The role of past experiences, psychopathologic traits and individual attachment patterns. Br Dent J. 2004;196:689–94. doi: 10.1038/sj.bdj.4811352. [DOI] [PubMed] [Google Scholar]
- 5.Todd JE, Walker A. London: H.M.S.O; 1980. Adult Dental Health in England and Wales. [Google Scholar]
- 6.Curson I, Coplans MP. The need for sedation in conservative dentistry. An investigation in the inner London area. Br Dent J. 1970;128:19–22. doi: 10.1038/sj.bdj.4802422. [DOI] [PubMed] [Google Scholar]
- 7.Locker D, Liddell A, Dempster L, Shapiro D. Age of onset of dental anxiety. J Dent Res. 1999;78:790–6. doi: 10.1177/00220345990780031201. [DOI] [PubMed] [Google Scholar]
- 8.Locker D, Shapiro D, Liddell A. Overlap between dental anxiety and blood-injury fears:Psychological characteristics and response to dental treatment. Behav Res Ther. 1997;35:583–90. doi: 10.1016/s0005-7967(97)00016-8. [DOI] [PubMed] [Google Scholar]
- 9.Seeman K, Molin C. Psychopathology, feelings of confinement and helplessness in the dental chair, and relationship to the dentist in patients with disproportionate dental anxiety (DDA) Acta Psychiatr Scand. 1976;54:81–91. doi: 10.1111/j.1600-0447.1976.tb00099.x. [DOI] [PubMed] [Google Scholar]
- 10.Benjamin C, Schuurs A, Kooreman T, Hoogstraten J. Self reported and physiologically measured dental anxiety, coping styles and personality traits. Anxiety Stress Coping. 1996;9:151–62. [Google Scholar]
- 11.Ost LG, Hugdahl K. Acquisition of blood and dental phobia and anxiety response patterns in clinical patients. Behav Res Ther. 1985;23:27–34. doi: 10.1016/0005-7967(85)90139-1. [DOI] [PubMed] [Google Scholar]
- 12.Corah NL, O’Shea RM, Bissell GD. The dentist-patient relationship:Perceptions by patients of dentist behavior in relation to satisfaction and anxiety. J Am Dent Assoc. 1985;111:443–6. doi: 10.14219/jada.archive.1985.0144. [DOI] [PubMed] [Google Scholar]
- 13.Corah NL. Development of a dental anxiety scale. J Dent Res. 1969;48:596. doi: 10.1177/00220345690480041801. [DOI] [PubMed] [Google Scholar]
- 14.Newton JT, Edwards JC. Psychometric properties of the modified dental anxiety scale:An independent replication. Community Dent Health. 2005;22:40–2. [PubMed] [Google Scholar]
- 15.Humphris GM, Freeman R, Campbell J, Tuutti H, D’Souza V. Further evidence for the reliability and validity of the Modified Dental Anxiety Scale. Int Dent J. 2000;50:367–70. doi: 10.1111/j.1875-595x.2000.tb00570.x. [DOI] [PubMed] [Google Scholar]
- 16.Bedi R, McGrath C. Factors associated with dental anxiety among older people in Britain. Gerodontology. 2000;17:97–103. doi: 10.1111/j.1741-2358.2000.00097.x. [DOI] [PubMed] [Google Scholar]
- 17.Cohen LA, Snyder TL, LaBelle AD. Correlates of dental anxiety in a university population. J Public Health Dent. 1982;42:228–35. doi: 10.1111/j.1752-7325.1982.tb02639.x. [DOI] [PubMed] [Google Scholar]
- 18.Hägglin C, Hakeberg M, Ahlqwist M, Sullivan M, Berggren U. Factors associated with dental anxiety and attendance in middle-aged and elderly women. Community Dent Oral Epidemiol. 2000;28:451–60. doi: 10.1034/j.1600-0528.2000.028006451.x. [DOI] [PubMed] [Google Scholar]
- 19.Corah NL, Gale EN, Illig SJ. Assessment of a dental anxiety scale. J Am Dent Assoc. 1978;97:816–9. doi: 10.14219/jada.archive.1978.0394. [DOI] [PubMed] [Google Scholar]
- 20.Dailey YM, Humphris GM, Lennon MA. Reducing patients’ state anxiety in general dental practice:A randomized controlled trial. J Dent Res. 2002;81:319–22. doi: 10.1177/154405910208100506. [DOI] [PubMed] [Google Scholar]
- 21.Clarke JH, Rustvold SR. Dental issues and techniques–1893. J Oreg Dent Assoc. 1993;62:36–8. [PubMed] [Google Scholar]
- 22.Gatchel RJ, Ingersoll BD, Bowman L, Robertson MC, Walker C. The prevalence of dental fear and avoidance:A recent survey study. J Am Dent Assoc. 1983;107:609–10. doi: 10.14219/jada.archive.1983.0285. [DOI] [PubMed] [Google Scholar]
- 23.Al-Omari WM, Al-Omiri MK. Dental anxiety among university students and its correlation with their field of study. J Appl Oral Sci. 2009;17:199–203. doi: 10.1590/S1678-77572009000300013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Halonen H, Salo T, Hakko H, Räsänen P. Association of dental anxiety to personality traits in a general population sample of Finnish University students. Acta Odontol Scand. 2012;70:96–100. doi: 10.3109/00016357.2011.598182. [DOI] [PubMed] [Google Scholar]
- 25.Locker D, Liddell A, Burman D. Dental fear and anxiety in an older adult population. Community Dent Oral Epidemiol. 1991;19:120–4. doi: 10.1111/j.1600-0528.1991.tb00125.x. [DOI] [PubMed] [Google Scholar]
- 26.Sghaireen MG, Zwiri AM, Alzoubi IA, Qodceih SM, Al-Omiri MK. Anxiety due to dental treatment and procedures among university students and its correlation with their gender and field of study. Int J Dent 2013. 2013:647436. doi: 10.1155/2013/647436. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Peretz B, Efrat J. Dental anxiety among young adolescent patients in Israel. Int J Paediatr Dent. 2000;10:126–32. doi: 10.1046/j.1365-263x.2000.00181.x. [DOI] [PubMed] [Google Scholar]
- 28.Peretz B, Zadik D. Dental anxiety of parents in an Israeli kibbutz population. Int J Paediatr Dent. 1994;4:87–92. doi: 10.1111/j.1365-263x.1994.tb00110.x. [DOI] [PubMed] [Google Scholar]
- 29.Attaullah, Ali khan A. Prevalence of dental anxiety among University students in Islamabad, Pakistan. J Khyber Coll Dent. 2011;1:71–7. [Google Scholar]
- 30.Locker D. Psychosocial consequences of dental fear and anxiety. Community Dent Oral Epidemiol. 2003;31:144–51. doi: 10.1034/j.1600-0528.2003.00028.x. [DOI] [PubMed] [Google Scholar]
- 31.Bergdahl M, Bergdahl J. Temperament and character personality dimensions in patients with dental anxiety. Eur J Oral Sci. 2003;111:93–8. doi: 10.1034/j.1600-0722.2003.00028.x. [DOI] [PubMed] [Google Scholar]
- 32.Abrahamsson KH, Berggren U, Hakeberg M, Carlsson SG. The importance of dental beliefs for the outcome of dental-fear treatment. Eur J Oral Sci. 2003;111:99–105. doi: 10.1034/j.1600-0722.2003.00016.x. [DOI] [PubMed] [Google Scholar]
- 33.Kumar S, Bhargav P, Patel A, Bhati M, Balasubramanyam G, Duraiswamy P, et al. Does dental anxiety influence oral health-related quality of life? Observations from across-sectional study among adults in Udaipur district, India. J Oral Sci. 2009;51:245–54. doi: 10.2334/josnusd.51.245. [DOI] [PubMed] [Google Scholar]
- 34.Economou GC. Dental anxiety and personality:Investigating the relationship between dental anxiety and self-consciousness. J Dent Educ. 2003;67:970–80. [PubMed] [Google Scholar]
- 35.Berggren U, Carlsson SG. Psychometric measures of dental fear. Community Dent Oral Epidemiol. 1984;12:319–24. doi: 10.1111/j.1600-0528.1984.tb01463.x. [DOI] [PubMed] [Google Scholar]
- 36.Acharya S. Factors affecting dental anxiety and beliefs in an Indian population. J Oral Rehabil. 2008;35:259–67. doi: 10.1111/j.1365-2842.2007.01777.x. [DOI] [PubMed] [Google Scholar]
- 37.Settineri S, Tati F, Fanara G. Gender differences in dental anxiety:Is the chair position important? J Contemp Dent Pract. 2005;6:115–22. [PubMed] [Google Scholar]
- 38.Yuan S, Freeman R, Lahti S, Lloyd-Williams F, Humphris G. Some psychometric properties of the Chinese version of the Modified Dental Anxiety Scale with cross validation. Health Qual Life Outcomes. 2008;6:22. doi: 10.1186/1477-7525-6-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Appukuttan D, Datchnamurthy M, P Deborah S, J Hirudayaraj G, Tadepalli A, J Victor D. Reliability and validity of the Tamil version of Modified Dental Anxiety Scale. J Oral Sci. 2012;54:313–20. doi: 10.2334/josnusd.54.313. [DOI] [PubMed] [Google Scholar]
- 40.Liddell A, Locker D. Gender and age differences in attitudes to dental pain and dental control. Community Dent Oral Epidemiol. 1997;25:314–8. doi: 10.1111/j.1600-0528.1997.tb00945.x. [DOI] [PubMed] [Google Scholar]