

Abstract
There are several conditions that results in excessive gingival display. In case of class I vertical maxillary excess the reason for this excessive display is the hypermobile lip. Though orthodontic treatment is the choice of treatment, surgical repositioning along with the orthodontics gives more predictable and stable results. This case report discusses cosmetic surgical management of case with class I vertical maxillary excess with excessive gingival display. The technique involves removal of strip of mucosal tissue from the labial vestibule thereby limiting the retraction of elevator muscles.
Keywords: Esthetics, gummy smile, lip repositioning, periodontal esthetic surgery
INTRODUCTION
Smile is the most recognized expression in the world and is the cornerstone of social interaction. A smile is defined as pleasant when the upper teeth are completely exposed and approximately 1 mm of buccal gingival tissue. However, a gum exposure not exceeding 2-3 mm is also considered pleasant, whereas an excessive exposure (>3 mm) is generally considered as not attractive.[1] Excessive gingival display or gummy smile as commonly described poses an esthetic problem and makes a person conscious of ones smile.
Although numerous factors cause excess gingival display, it is common for the condition to occur as a result of interplay of several etiologies. Etiological factors resulting in gummy smile can be:[2]
Skeletal (vertical maxillary excess)
Gingival (passive eruption)
Muscular (hyper functional upper lip)
It is essential to analyze several characteristics: Symmetry of lips and face during smile; gum exposure; level of gingival margins; alignment of gingival margins (size of teeth and proportions) and smile-line.[3] Treatment options range from Le fort I osteotomy, crown lengthening, intrusion, myectomy to muscle resection etc. Whenever there is increased maxillary vertical excess, orthognathic surgery is the choice of treatment. However, it requires hospital setting and surgery performed under general anesthesia and is morbid. When there is hyperactive lip, the treatment of choice would be surgical lip repositioning or use of botulinum toxin type A. Use of botox is minimally invasive, but results are less stable.[4]
CASE REPORT
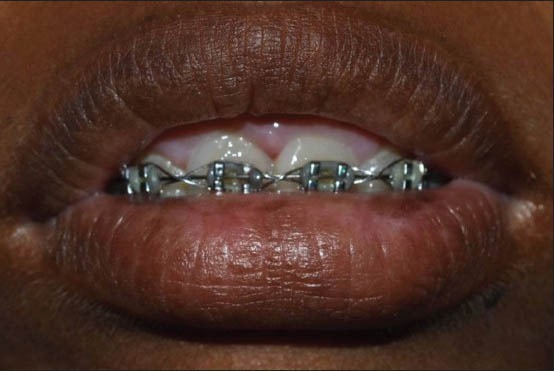
An 18-year-old young female patient reported to the Department of Periodontology, Meenakshi Ammal Dental College and Hospital, with a chief complaint of excessive gingival display on smiling [Figure 1]. Patient had class I vertical maxillary excess with hyperactive maxillary lip. Patient was under orthodontic treatment and was not willing for orthognathic surgery.
Figure 1.
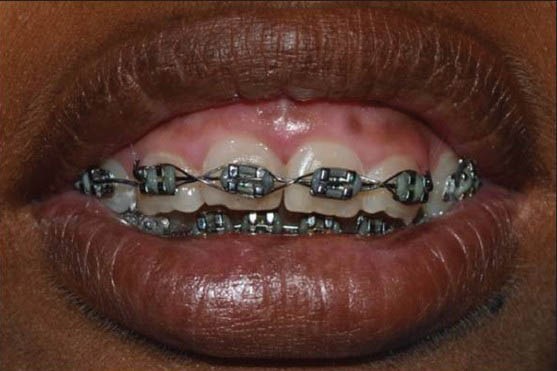
Pre-operative presentation
Pre-treatment evaluation
Patient had an increased lower facial height. A moderate gingival display was seen during smiling that extended from maxillary right first premolar to maxillary left first premolar. The gingival display (From the gingival margin) was about 6 mm at the central incisor region [Figure 2]. The upper lip length was 17 mm and the lip was incompetent. Accordingly, a treatment plan of surgical lip repositioning with mucosal strip technique was explained to the patient and with informed consent the procedure was carried out.
Figure 2.
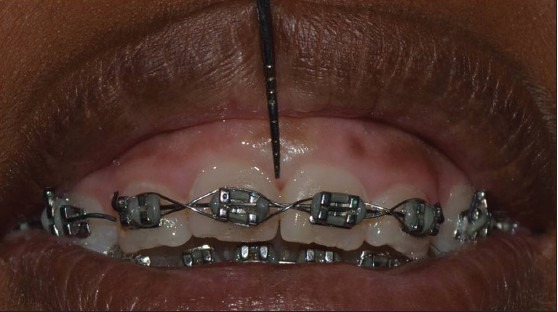
6 mm gingival display
SURGICAL PROCEDURE
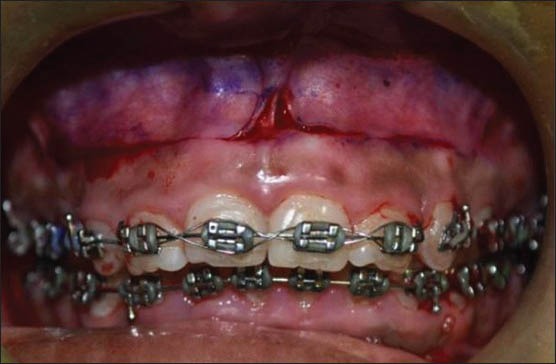
Disinfection of the surgical site was done with 2% betadine. The procedure was carried out under local anesthesia (lignocaine HCl with 2% epinephrine 1:200,000). The incision outline was first marked with a sterile indeliable pencil [Figure 3]. The inferior border of incision was at the mucogingival line and the superior border was parallel to the lower border and was at a distance twice the gingival display (distance between upper and the lower incision margins = 12 mm). The two incisions were connected at the mesial ends of the second premolars on either side to create an elliptical outline. Incision was given with no 15 BP blade [Figure 4].
Figure 3.

Incision outline
Figure 4.
Incisions
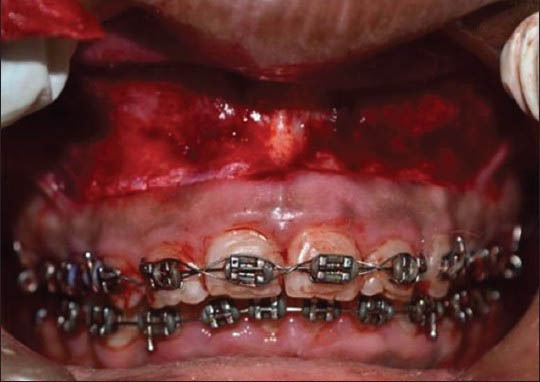
A partial thickness dissection was made at the mucogingival junction and the entire epithelium is excised along the elliptical outline, exposing the underlying connective tissue [Figures 5 and 6]. The entire strip of mucosa between the two incisions was excised [Figure 7]. The incision lines were approximated with continuous interlocking sutures (4-0 black silk) ensuring correct alignment of the midline of lip with the midline of teeth [Figure 8]. Periodontal dressing (Coe pac) was placed.
Figure 5.
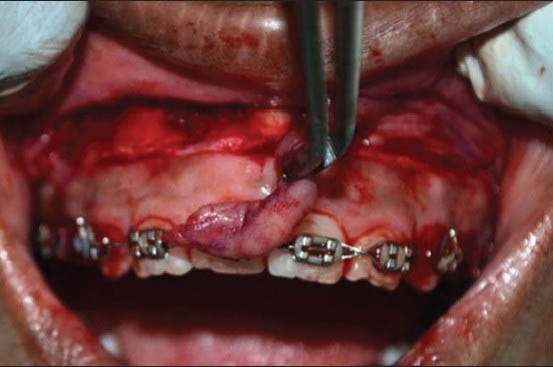
Separating the mucosal strip
Figure 6.
Exposed connective tissue
Figure 7.

Excised mucosal strip
Figure 8.
Continuous interlocking sutures
Post-operatively analgesic (ibuprofen 400 mg BD for 2 days) and antibiotic (amoxicillin 500 mg TD for 5 days) was prescribed. Patient was instructed to use ice compresses. Post-operative instructions were given and the patient was dismissed.
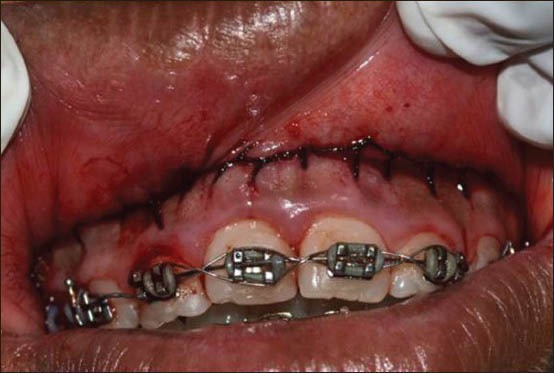
Patient was recalled 10 days post-operative and the area were examined. There was minimal discomfort with a feel of tension reported by the patient. The healing was satisfactory and the sutures were removed. Patient was again recalled after 2 weeks. The healing was complete and patient reported of no discomfort. There was also no apparent scarring in the sutured region [Figure 9]. This contradicted the other reports.[5] The gingival display reduced by 4 mm [Figure 10]. The case was followed for 18 months and the results were stable [Figure 11].
Figure 9.

At 2 weeks post-operative — healing without scarring along the suture line
Figure 10.
At 2 weeks post-operative
Figure 11.
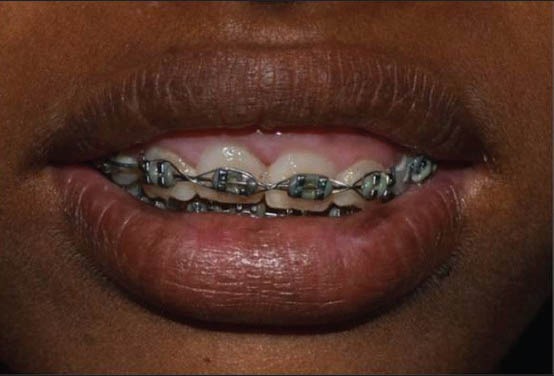
At 18 months post-operative
DISCUSSION
One objective of esthetic dentistry is to create ideal esthetics for the patient's smile. However, some patients who present with gingival and skeletal deformities may require more complex esthetic rehabilitation.[6]
It is of utmost importance to evaluate the lips and the teeth (size, shape and position) in patient with esthetic requirements.[7] If the size and shape of the teeth and the localization of the gingival margins are perfectly normal, an excessive exposure of gums can be caused either by the position of the upper maxillary bone, exceeding vertically or by the inadequate size of the upper lip.[3] In such cases the treatment of choice would be surgical lip repositioning.
The mucosal strip technique presented in this case was described in 1973 in the medical literature.[8] This procedure involves the retraction of the elevator muscles of the lip (zygomaticus minor, levator anguli, orbicularis oris and levator labii superioris) thereby resulting in the decreased gingival display. Litton and Fournier advocated this procedure for the correction of excessive gingival display in the presence of a short upper lip, by detaching the muscles from the bony structures to coronally position the upper lip and no complications were reported.[9] To achieve optimal results the flap was advanced a distance of two times gingival display as in these case reports. Humayun documented this procedure as mucosal coronally positioned flap and reported stable results of up to 1 year post-operatively.[10]
The following precautions must be taken during the surgery: Care must be taken to avoid damage to minor salivary glands in submucosa, Clinicians must look for adequate width of attached gingiva. With inadequate attached gingiva the technique cannot be performed. Severe skeletal deformities are also contraindications for this procedure and should ideally be treated with orthognathic surgery. Some cases with a rare complication reported in the literature are paresthesia[11] and transient paralysis.[12]
This procedure is simple and safe and the case presented here showed good stable results for 18 months. There were no adverse events reported during this follow-up period. This technique offers a promising alternative to the orthognathic surgery. Careful diagnosis and case selection are critical factors in the successful outcomes.
CONCLUSION
Lip repositioning is a simple alternative to other morbid techniques of treating excessive gingival display. The long-term stability is still to be explored.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Allen EP. Use of mucogingival surgical procedures to enhance esthetics. Dent Clin North Am. 1988;32:307–30. [PubMed] [Google Scholar]
- 2.Sahoo KC, Raghunath N, Shivalinga BM. Botox in gummy smile — A review. Indian J Dent Sci. 2012;1:51–4. [Google Scholar]
- 3.Monica M, Martina S, Matteo M, Claudio M, Zucchelli G. Periodontal treatment in patients with passive altered eruption. J Parodontol Implantol Orale. 2010;29:45–56. [Google Scholar]
- 4.Polo M. Botulinum toxin type A (Botox) for the neuromuscular correction of excessive gingival display on smiling (gummy smile) Am J Orthod Dentofacial Orthop. 2008;133:195–203. doi: 10.1016/j.ajodo.2007.04.033. [DOI] [PubMed] [Google Scholar]
- 5.Gupta KK, Srivastava A, Singhal R, Srivastava S. An innovative cosmetic technique called lip repositioning. J Indian Soc Periodontol. 2010;14:266–9. doi: 10.4103/0972-124X.76936. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Simon Z, Rosenblatt A, Dorfman W. Eliminating a gummy smile with surgical lip repositioning. J Cosmet Dent. 2007;23:102–9. [Google Scholar]
- 7.Tjan AH, Miller GD, The JG. Some esthetic factors in a smile. J Prosthet Dent. 1984;51:24–8. doi: 10.1016/s0022-3913(84)80097-9. [DOI] [PubMed] [Google Scholar]
- 8.Rosenblatt A, Simon Z. Lip repositioning for reduction of excessive gingival display: A clinical report. Int J Periodontics Restorative Dent. 2006;26:433–7. [PubMed] [Google Scholar]
- 9.Litton C, Fournier P. Simple surgical correction of the gummy smile. Plast Reconstr Surg. 1979;63:372–3. doi: 10.1097/00006534-197903000-00014. [DOI] [PubMed] [Google Scholar]
- 10.Humayun N, Kolhatkar S, Souiyas J, Bhola M. Mucosal coronally positioned flap for the management of excessive gingival display in the presence of hypermobility of the upper lip and vertical maxillary excess: A case report. J Periodontol. 2010;81:1858–63. doi: 10.1902/jop.2010.100292. [DOI] [PubMed] [Google Scholar]
- 11.Miskinyar SA. A new method for correcting a gummy smile. Plast Reconstr Surg. 1983;72:397–400. doi: 10.1097/00006534-198309000-00027. [DOI] [PubMed] [Google Scholar]
- 12.Kamer FM. “How I do it” – Plastic surgery. Practical suggestions on facial plastic surgery. Smile surgery. Laryngoscope. 1979;89:1528–32. doi: 10.1002/lary.5540890917. [DOI] [PubMed] [Google Scholar]