

Abstract
Background: This study was designed to assess the effect of sesame seed on lipid profile and oxidative stress biomarkers in knee osteoarthritis (OA) patients.
Methods: Fifty patients with knee OA were allocated into two groups receiving 40 g of sesame seed daily along with standard medical therapy (n=25) or standard treatment (n=25) for two months. Serum total antioxidant capacity, malondialdehyde (MDA) and lipid profile (total cholesterol (TC), HDL-cholesterol, LDL-cholesterol, triglycerides) were measured.
Results: After the intervention period two months of study, serum TC, LDL-cholesterol and MDA decreased significantly in the sesame group (P<0.05), while no significant difference in serum values of lipid profile and oxidative stress parameters was seen in the control group (P>0.05). There was no significant difference in pre and post-treatment values of lipid profile and oxidative parameters between the two groups (P>0.05).
Conclusion: Current study showed a positive effect of sesame seed in improving lipid profile and oxidative stress in patients with knee OA and indicated the fact that sesame seed might be of help to reduce oxidative stress in OA patients.
Keywords: Sesame, Oxidative stress, Antioxidant, Lipid profile, Osteoarthritis
Introduction
Osteoarthritis (OA) is one of the most common musculoskeletal disorders.1 Outstanding characteristic of disease is progressive destruction of articular cartilage that causes limited joint motion, pain and ultimate disability.1,2 The knee joints are often amongst the most affected joints in OA.1,2 Since OA is a multi-factorial process of joint degeneration, various mechanisms may be involved in its development.3 Imbalance between pro-oxidants and antioxidants leads to cellular oxidative stress which plays an important role in progression of OA.4 Oxidative damage induced by reactive oxygen species results from an increased production of superoxide anions and their metabolites or reduced bioavailability of antioxidant defenses.4 Lipid peroxidation has been implicated as key source of oxidative stress in age-related oxidative stress.4It generates a variety of hydroperoxide and aldehydic products that are highly reactive with cellular components and extracellular matrix. Malondialdehyde (MDA), a toxic aldehydic end product of lipid peroxidation, mediates the oxidation and degradation of cartilage collagen.4 Previous studies have reported an increased level of MDA and a decreased level of superoxide dismutase (SOD), glutathione peroxidase, protein kinase C, vitamins C and E and catalase activity in OA.5,6 Oxidative stress along with aging lead to the increased destruction of chondrocytes.5,6 It is suggested that antioxidants have an important role in protection of knee cartilage and bone health.5,6 Oxidative stress in OA patients is an effective factor in decreased response to the treatment.5,6 Therefore, improvement in antioxidant capacity could have an important role in prevention and treatment of OA.5,6 Some epidemiological studies7,9 have concluded that patients with OA have altered levels of serum lipids, mainly in form of increased concentration of serum total cholesterol. This finding could play an independent role as a systemic risk factor for OA.7,9
It seems that medical treatment of OA may have several side-effects for patients.10 In addition, other therapies such as surgery or joint replacement are stressful, expensive and time-consuming.10,11 Recently, studies on pharmaceutical plants have demonstrated beneficial and promising effects in prevention and treatment of chronic diseases such as OA.12 One of these pharmaceutical plants is sesame seed.13 Sesame (Sesamum indicum L.) is an important traditional health food that has been used to improve nutritional status and prevent various diseases in Asian countries for thousands of years. Sesame seeds are not only rich in oil and protein, but also in lignans (eg, sesamin and sesamolin).13 Existing data from animal and human studies support the hypothesis that sesame seed and its lignans may have antioxidant and hypocholesterolemic effects.14,17 However, no interventional studies have investigated these potential effects of sesame seed in treatment of OA patients.
The current study was designed to evaluate the effects of sesame seed on lipid profile and oxidative stress in OA patients.
Materials and Methods
Sesame preparation
Sesame seeds were provided from Nojehmehr Village of Hadishahr City in East-Azerbaijan Province, Iran. After clean-up, washing and drying stages, sesame seeds were then ground into powder to enhance digestion and absorption. Then sesame powder was packed (each pack contained 40 g of sesame seeds) before delivery to study volunteers.
Subjects and treatments
The study was approved by the Ethics Committee of Tabriz University of Medical Sciences and registered at the www.irct.ir, identifier: IRCT201011164105N4. All subjects were made aware of the content of the study and written informed consent was obtained from each subject. Fifty patients (10 men and 40 women) aged 50-70 years old who had knee osteoarthritis with disease severity ranged from mild to moderate (based on the criteria of American College of Rheumatology18) were selected from Shohada and Shahid-Madani Hospitals. Shohada and Shahid-Madani Hospitals, located in Tabriz, are the two specialty and subspecialty orthopedic centers in the north-west of Iran and serve secondary and tertiary care for patients. Sample size was determined based on information obtained from Mosallaee study19 on primary endpoint of total cholesterol including mean (SD) in experimental and control groups. Considering a confidence level of 95%, power of 80% and using Pocock Formula, the sample was determined at least 21 in each group. The sample size was increased to 25 in each group (81.82% females) for a possible dropout of 20%.
Exclusion criteria were body mass index (BMI)>30 kg/m2 or BMI<18.5 kg/m2, cardiovascular disease, diabetes mellitus, liver and kidney disease, any history of peptic or duodenal ulcers, smoking, alcohol intake, using multivitamin-mineral supplements, having an allergy to sesame and use of lipid-lowering and non-steroidal anti-inflammatory drugs. Eligible patients were recruited in the study based on convenience sampling method (Fig. 1). Patients were randomly allocated in to two groups named sesame and control group based on randomized block permutation procedure whose random sequence was generated by Random Allocation Software. Subjects in the control group (25 patients) received only standard medical therapy including two 500 mg acetaminophen twice a day and one glucosamine 500 mg once a day; however, the intervention group (25 patients) received 40 g of sesame powder13 per day by oral administration during the two-month trial with the standard drug therapy including two 500 mg acetaminophen twice a day and one glucosamine 500 mg once a day. All subjects were instructed to maintain their usual diet and physical activity throughout the study.
Fig. 1 .
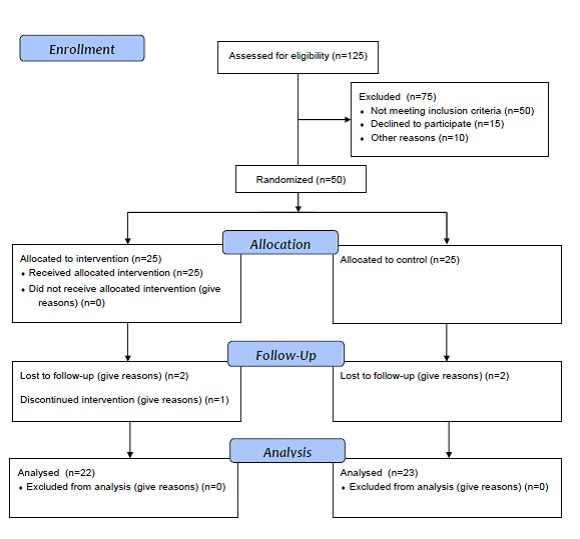
Consort 2010 flow diagram
Anthropometric & Biochemical measurements
Body weight of each subject was measured with barefoot and wearing light clothing to the nearest 0.1 kg with a Seca scale (Dubai, United Arab Emirates). Height of each subject was measured with barefoot using a measuring tape with the subject’s arm hanging freely at sides and recorded to the nearest 0.5 cm. BMI was calculated as weight (kg) divided by height2 (m2). After a 12-hour overnight fast, 5 ml blood sample was obtained. Serum TAC was measured using a Randox (Lot:213NX, France) total antioxidant status kit in which 2,2’-azino-bis (3-ethylbenzothiazoline-6-sulfanate) (ABTS) is incubated with a peroxidase and H2O2 to produce the radical cation ABTS+. This has a stable blue-green color, which is measured at 600 nm. Antioxidants in the added sample cause suppression of this color production to a degree that is proportional to their concentration. MDA levels were determined by the thiobarbitoric acid reaction with acid, which was extracted with n-butanol and measured spectrophotometrically at a wavelength of 523 nm and compared with a standard curve. Serum total cholesterol, HDL-cholesterol and triglycerides were measured using kit (Pars-azmoon, Tehran, Iran) and enzymatic-colorimetric method. Friedewald formula was used for measuring LDL-cholesterol.20
Statistical analysis
Statistical analysis was performed using the Statistical Package for the Social Sciences (SPSS Inc, Chicago, IL, USA) version 11.5. Continuous variables were presented as mean and standard deviation (SD) while categorical variables were presented as number and percentage. The results were normally distributed (Kolmogorov–Smirnov test). Pre and post-treatment differences in mean values were analyzed using paired t-test. Differences in mean values between the two groups were analysed using independent t-test. ANCOVA analysis was used for the comparison of post-treatment values with adjusting on baseline values. P<0.05 was considered to indicate statistical significance.
Results
Twenty-two patients in intervention group and twenty-three patients in control group completed the study. Baseline characteristics of the participants are presented in Table 1. No significant difference was found between the two groups in weight, height, BMI and disease duration (P>0.05). Serum total cholesterol, LDL-cholesterol and MDA were significantly decreased in treatment group (P<0.05) while there was no significant change in serum TAC compared with baseline (Table 2). In the control group, a non-significant increase in serum total cholesterol and triglycerides and a non-significant decrease in serum HDL-cholesterol and LDL-cholesterol was seen after two months of study (Table 2). Moreover, no significant difference was observed in serum values of oxidative stress biomarkers in control group (Table 2). After adjusting for the baseline values, there was no significant difference in post-treatment serum MDA between the two groups. In addition, no difference was observed in the results of independent t-test and analysis of covariance (ANCOVA) regarding the other serum parameters.
Table 1. Baseline characteristics of participants in case and control groups .
| Characteristic | Sesame group (n=22) | Control group (n=23) |
| Age* (yr) | 54.90±6.39 | 60.27±7.84 |
| Weight (kg) | 72.38±8.45 | 70.63±7.01 |
| Hight (cm) | 162.29±7.02 | 160.29±6.59 |
| BMI† (kg/m2) | 27.45±2.64 | 27.39±2.71 |
| Disease duration (yr) | 4.09±3.35 | 5.23±5.50 |
* P<0.05 /† Body Mass Index
Table 2. Serum lipid profile and oxidative stress biomarkers in case and control groups .
| Parameters | Sesame group (n=22) | Control group (n=23) | P* | ||||
| Before Mean±SD | After Mean±SD | ** P | Before Mean±SD | After Mean±SD | ** P | ||
| TC (mg/dl) | 224.54±49.36 | 209.09±49.43 | 0.003 | 218.31±36.58 | 219.72±34.86 | 0.801 | 0.414 |
| HDL- C (mg/dl) | 47.63±8.27 | 46.00±6.50 | 0.070 | 49.81±10.79 | 49.59±11.40 | 0.856 | 0.207 |
| LDL-C (mg/dl) | 147.43±43.15 | 135.20±45.70 | 0.017 | 134.71±37.98 | 133.40±34.45 | 0.815 | 0.869 |
| TG (mg/dl) | 145.59±80.76 | 139.45±73.57 | 0.071 | 168.95±85.83 | 183.68±94.39 | 0.756 | 0.090 |
| MDA (µmol/L) | 2.65±1.89 | 1.90±1.79 | 0.046 | 2.33±1.94 | 2.48±2.18 | 0.709 | 0.351 |
| TAC† (mmol/L) | 0.50±0.14 | 0.49±0.10 | 0.533 | 0.51±0.19 | 0.51±0.15 | 0.330 | 0.991 |
* P for differences between groups based on ANCOVA for comparing after intervention measures adjusting for baseline measures / ** P for differences within groups/† Total antioxidant capacity
Discussion
OA is the most common joint disorder in world and considered to be as one of the most frequent causes of pain, loss of function and disability in adults. Radiographic evidence of OA occurs in majority of people by 65 years of age and in about 80% of those aged over 75 years.21 According to the COPCORD study conducted in 2008 including 10291 adults over the age of 15 years, about 994 of the subjects had pain complaint and 528 of them had stiffness in their hand or finger joints. About 94 cases of hand osteoarthritis were identified in the study.22 To the best of our knowledge, this study is one of the first investigations that were conducted to assess the effect of sesame seed on lipid profile and oxidative stress parameters in patients with knee osteoarthritis. Our study indicated a significant decrease in serum total cholesterol and LDL-cholesterol in sesame group. There have been several reports that support our results and emphasize the hypolipidemic effects of sesame.23,26 In a study on patients with type 2 diabetes mellitus, sesame oil supplementation led to the significant decrease in plasma TC, LDL-C and TG levels and significant increase in plasma HDL-C (20%, 33.8%, 14% and 15.7%, respectively vs before treatment).24 Another study27 showed that TG and HDL-C levels did not change significantly in mice after being fed with diet contained sesame oil for 4 weeks which is in agreement with the current study. In contrast to our results, Sankar et al.24, Mitra et al.25 and Biswas et al.28 showed a significant decrease in serum triglycerides and VLDL and a significant increase in serum HDL-C. The reason why triglycerides and HDL-C did not change significantly in present study could be the result of the fact that our patients had lower serum triglycerides and higher serum HDL-C at the beginning of the study. In fact, only 50% and 30% of patients in each group (sesame and control) was hypertriglyceridemic and had lower HDL-C, respectively. In addition, some of the studies indicated that monounsaturated fatty acids tend to increase and polyunsaturated fatty acids decreases serum HDL-C. Sesame seed has high levels of both mentioned fatty acids.29 In a study of normocholesterolemic mice, Eltahir et al.30 found that diet which contained sesame seed, did not affect serum lipid levels. Some potential explanations may be responsible for this contrary result: First, patient population may vary in different investigations. Additional factors that might influence the results are the amount and form of the product (sesame seed, oil, extract, or chemical compounds) used in different studies. For instance, lignans and effective compounds of Iranian sesame varieties could be entirely different with sesame varieties of other regions. Duration of the intervention in each study might also vary.
Our study showed a significant decrease in serum MDA in the treatment group. Several reports support our results and emphasize the antioxidant effects of sesame.24,26,31 Other studies32,33 on mice also had demonstrated similar results. There is not any exact mechanism to show how sesame products could decrease oxidative stress but it is believed that its protective effects are due to its lignans including sesamin, sesamol and sesamolin and vitamin E content. Sesame seed has phenolic lignans such as sesamol. Antioxidant effects of lignans were shown in previous studies.34,35 In addition, it is clear that diets containing polyphenols and flavonoids increase catalase and SOD activity, decrease MDA and improve lipid profile.36,37 Nakai et al.37 showed that CYP450 metabolized sesamin in liver which results in inversion of methylene dioxyphenyl to dihydrophenyl (strong radical scavenger). Previously, scientific evidence has proved the fact that protective effects of sesame seed are due to the suppression of oxygen species production.38 In addition, sesame lignans have an ability to increase vitamin E level in various tissues39,40 and increase in gamma-tocopherol levels that could lead to the suppression of different free radicals (those usually increase in age-related diseases).41 No significant change was found in serum TAC in present study. Since total antioxidant capacity of different varieties and species of sesame is different,42 therefore this might be the reason for any change in serum TAC. Moreover, it is assumed that antioxidant capacity is affected by other dietary factors. Since recruiting the patients was according to the ACR criteria,18 therefore there was an age limit above 50 years old in this study; whereas knee OA could be observed in lower ages, too.
Since we were not able to have a placebo in present study, therefore lack of blindness in this study can be considered as a limitation of our study. Another limitation of this study was that consumption of suggested amounts of sesame was more difficult for some patients which implied that sesame should be replaced with sesame oil or sesame extract in order to increase compliance among patients.
Conclusion
Overall results of the present study demonstrated a positive effect of sesame seed in decreasing serum total cholesterol, LDL-cholesterol and MDA in patients with knee osteoarthritis and indicated the fact that sesame seed might be of help to reduce oxidative stress in OA patients.
Acknowledgments
This article was written based on a data set of MSc thesis, registered in Tabriz University of Medical Sciences. The authors wish to thank the Research Vice Chancellor of Tabriz University of Medical Sciences for funding this project. We also thank Hamid Taghavi for his assistance and guidance in this research. We also thank all the patients for their participation in this research.
Competing interests
The authors declare that there is no conflict of interests.
References
- 1.Anandacoomarasamy A, March L. Current evidence for osteoarthritis treatments. Ther Adv Musculoskelet Dis. 2010;2:17–28. doi: 10.1177/1759720X09359889. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Duncan K. Medical nutrition therapy for rheumatic disease. In: K Mahan, S Escott-Stump, editors. Krause’s Food & Nutrition Therapy. Philadelphia: Saunders;2008.
- 3.Livshits G, Zhai G, Hart DJ, Kato BS, Wang H, Williams FM. et al. Interleukin-6 is a significant predictor of radiographic knee osteoarthritis: The Chingford study. Arthritis Rheum. 2009;60:2037–2045. doi: 10.1002/art.24598. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Bhattacharya I, Saxena R, Gupta V. Efficacy of vitamin E in knee osteoarthritis management of North Indian geriatric population. Ther Adv Musculoskelet Dis. 2012;4:11–19. doi: 10.1177/1759720X11424458. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Surapaneni KM, Venkataramana G. Status of lipid peroxidation, glutathione, ascorbic acid, vitamin E and antioxidant enzymes in patients with osteoarthritis. Indian J Med Sci. 2007;61:9–14. [PubMed] [Google Scholar]
- 6.McAlindon TE, Jacques P, Zhang Y, Hannan MT, Aliabadi P, Weissman B. et al. Do antioxidant micronutrients protect against the development and progression of knee osteoarthritis? Arthritis Rheum. 1996;39:648–656. doi: 10.1002/art.1780390417. [DOI] [PubMed] [Google Scholar]
- 7.Gkretsi V, Simopoulou T, Tsezou A. Lipid metabolism and osteoarthritis: Lessons from atherosclerosis. Prog Lipid Res. 2011;50:133–140. doi: 10.1016/j.plipres.2010.11.001. [DOI] [PubMed] [Google Scholar]
- 8.Stürmer T, Sun Y, Sauerland S, Zeissig I, Günther KP, Puhl W. et al. Serum cholesterol and osteoarthritis. The baseline examination of the Ulm osteoarthritis study. J Rheumatol. 1998;25:1827–1832. [PubMed] [Google Scholar]
- 9.Tsezou A, Iliopoulos D, Malizos KN, Simopoulou T. Impaired expression of genes regulating cholesterol efflux in human osteoarthritic chondrocytes. J Orthop Res. 2010;28:1033–1039. doi: 10.1002/jor.21084. [DOI] [PubMed] [Google Scholar]
- 10.Pagnano M, Westrich G. Successful nonoperative management of chronic osteoarthritis pain of the knee: safety and efficacy of retreatment with intra-articular hyaluronans. Osteoarthritis Cartilage. 2005;13:751–761. doi: 10.1016/j.joca.2005.04.012. [DOI] [PubMed] [Google Scholar]
- 11.Brandt KD. Non-surgical treatment of osteoarthritis: a half century of "advances". Ann Rheum Dis. 2004;63:117–122. doi: 10.1136/ard.2002.004606. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Ameye LG, Chee WS. Osteoarthritis and nutrition. From nutraceuticals to functional foods: a systematic review of the scientific evidence. Arthritis Res Ther. 2006;8:R127. doi: 10.1186/ar2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Chen PR, Chien KL, Su TC, Chang CJ, Liu TL, Cheng H, Tsai C. Dietary sesame reduces serum cholesterol and enhances antioxidant capacity in hypercholesterolemia. Nutr Res. 2005;25:559–567. [Google Scholar]
- 14.Kang MH, Naito M, Tsujihara N, Osawa T. Sesamolin inhibits lipid peroxidation in rat liver and kidney. J Nutr. 1998;128:1018–1022. doi: 10.1093/jn/128.6.1018. [DOI] [PubMed] [Google Scholar]
- 15.Hirata F, Fujita K, Ishikura Y, Hosoda K, Ishikawa T, Nakamura H. Hypocholesterolemic effect of sesame lignan in humans. Atherosclerosis. 1996;122:135–136. doi: 10.1016/0021-9150(95)05769-2. [DOI] [PubMed] [Google Scholar]
- 16.Nakano D, Itoh C, Ishii F, Kawanishi H, Takaoka M, Kiso Y. et al. Effects of sesamin on aortic oxidative stress and endothelial dysfunction in deoxycorticosterone acetate-salt hypertensive rats. Biol Pharm Bull. 2003;26:1701–1705. doi: 10.1248/bpb.26.1701. [DOI] [PubMed] [Google Scholar]
- 17.Ikeda S, Tohyama T, Yamashita K. Dietary sesame seed and its lignans inhibit 2,7,8-trimethyl- 2(2'-carboxyethyl)-6-hydroxychro-man excretion into urine of rats fed gamma-tocopherol. J Nutr. 2002;132:961–966. doi: 10.1093/jn/132.5.961. [DOI] [PubMed] [Google Scholar]
- 18.Altman R, Asch E, Bloch D, Bole G, Borenstein D, Brandt K. et al. Development of criteria for the classification and reporting of osteoarthritis. Classification of osteoarthritis of the knee. Diagnostic and Therapeutic Criteria Committee of the American Rheumatism Association. Arthritis Rheum. 1986;29:1039–1049. doi: 10.1002/art.1780290816. [DOI] [PubMed] [Google Scholar]
- 19.Mosallaieepour-Yazdi M, Eghtesadi Sh, Kaseb F, Afkhami-Ardakani M, Hoseini F. Effects of sesame oil on blood glucose and lipid profile in Type II diabetic patients referring to the Yazd Diabetes Research Center. Journal of Shahid Sadoughi University of Medical Sciences . 2008;16:31–35. [In Persian]. [Google Scholar]
- 20.Krummel DA. Medical nutrition therapy for cardiovascular disease. In: In: K Mahan, S Escott-Stump, editors. Krause’s Food & Nutrition Therapy. Philadelphia: Saunders;2008.
- 21.Arden N, Nevitt MC. Osteoarthritis: epidemiology. Best Pract Res Clin Rheumatol. 2006;20:3–25. doi: 10.1016/j.berh.2005.09.007. [DOI] [PubMed] [Google Scholar]
- 22.Davatchi F, Jamshidi AR, Banihashemi AT, Gholami J, Forouzanfar MH, Akhlaghi M. et al. WHO-ILAR COPCORD Study (Stage 1, Urban Study) in Iran. J Rheumatol. 2008;35:1384. [PubMed] [Google Scholar]
- 23.Tsuruoka N, Kidokoro A, Matsumoto I, Abe K, Kiso Y. Modulating effect of sesamin, a functional lignan in sesame seeds, on the transcription levels of lipid- and alcohol-metabolizing enzymes in rat liver: a DNA microarray study. Biosci Biotechnol Biochem. 2005;69:179–188. doi: 10.1271/bbb.69.179. [DOI] [PubMed] [Google Scholar]
- 24.Sankar D, Ali A, Sambandam G, Rao R. Sesame oil exhibits synergistic effect with anti-diabetic medication in patients with type 2 diabetes mellitus. Clin Nutr. 2011;30:351–358. doi: 10.1016/j.clnu.2010.11.005. [DOI] [PubMed] [Google Scholar]
- 25.Mitra A. Study on the benefits of sesame oil over Coconut oil in patients of insulin resistance syndrome, notably Type 2 Diabetes and dyslipidaemia. J Hum Ecol. 2007;22:61–66. [Google Scholar]
- 26.Sankar D, Sambandamb G, Ramakrishna Rao M, Pugalendi KV. Modulation of blood pressure, lipid profiles and redox status in hypertensive patients taking different edible oils. Clin Chim Acta. 2005;355:97–104. doi: 10.1016/j.cccn.2004.12.009. [DOI] [PubMed] [Google Scholar]
- 27.Abou-Gharbia HA, Shehata AAY, Shahidi F. Effect of processing on oxidative stability and lipid classes of sesame oil. Food Res Int. 2000;33:331–340. [Google Scholar]
- 28.Biswas A, Dhar P, Ghosh S. Biswas A, Dhar P, Ghosh SAntihyperlipidemic effect of sesame (Sesamum indicumL) protein isolate in rats fed a normal and high cholesteroldiet. J Food Sci . 2010;75:H274–279. doi: 10.1111/j.1750-3841.2010.01821.x. [DOI] [PubMed] [Google Scholar]
- 29.Mensink RP, Katan MB. Mensink RP, Katan MBEffect of dietary fatty acids on serum lipids and lipoproteinsA meta-analysis of 27 trials. Arterioscler Thromb . 1992;12:911–919. doi: 10.1161/01.atv.12.8.911. [DOI] [PubMed] [Google Scholar]
- 30.Eltahir MM, Shaddad SAI, Eltayeb IB. The effect of sesame oil on serum lipids level in normochole sterolemic and hypercholesterolemic diet-fed rats. ournal of food technology. 2005;3:552–554. [Google Scholar]
- 31.Sankar D, Rao MR, Sambandam G, Pugalendi KV. A pilot study of open label sesame oil in hypertensive diabetics. J Med Food. 2006;9:408–412. doi: 10.1089/jmf.2006.9.408. [DOI] [PubMed] [Google Scholar]
- 32.Visavadiya NP, Narasimhacharya AV. Sesame as a hypocholesteraemic and antioxidant dietary component. Food Chem Toxicol. 2008;46:1889–1895. doi: 10.1016/j.fct.2008.01.012. [DOI] [PubMed] [Google Scholar]
- 33.Ahmad S, Yousuf S, Ishrat T, Khan MB, Bhatia K, Fazli IS, Khan JS, Ansari NH, Islam F. Effect of dietary sesame oil as antioxidant on brain hippocampus of rat in focal cerebral ischemia. Life Sci. 2005;79:1921–1928. doi: 10.1016/j.lfs.2006.06.017. [DOI] [PubMed] [Google Scholar]
- 34.Kapadia GJ, Azuine MA, Tokuda H, Takasaki M, Mukainaka T, Konoshima T. et al. Chemopreventive effect of resveratrol, sesamol, sesame oil and sunflower oil in the Epstein–Barr virus early antigen activation assay and the mouse skin two-stage carcinogenesis. Pharmacol Res. 2002;45:499–505. doi: 10.1006/phrs.2002.0992. [DOI] [PubMed] [Google Scholar]
- 35.Toyokuni S, Tanaka T, Kawaguchi W, Fang NR, Ozeki M, Akatsuka S. et al. Effects of the phenolic contents of Mauritian endemic plant extracts on promoter activities of antioxidant enzymes. Free Radic Res. 2003;37:1215–1224. doi: 10.1080/10715760310001598150. [DOI] [PubMed] [Google Scholar]
- 36.Ralay Ranaivo H, Rakotoarison O, Tesse A, Schott C, Randriantsoa A, Lobstein A, Andriantsitohaina R. Cedrelopsis grevei induced hypotension and improved endothelial vasodilatation through an increase of Cu/Zn SOD protein expression. Am J Physiol Heart Circ Physiol. 2004;286:H775–781. doi: 10.1152/ajpheart.00584.2003. [DOI] [PubMed] [Google Scholar]
- 37.Nakai M, Harada M, Nakahara K, Akimoto K, Shibata H, Miki W. et al. Novel antioxidative metabolites in rat liver with ingested sesamin. J Agric Food Chem. 2003;51:1666–1670. doi: 10.1021/jf0258961. [DOI] [PubMed] [Google Scholar]
- 38.Jeng KCG, Hou RCW. Sesamin and Sesamolin: Nature’s therapeutic lignans. Curr Enzym Inhib. 2005;1:11–20. [Google Scholar]
- 39.Kamal-Eldin A, Frank J, Razdan A, Tengblad S, Basu S, Vessby B. Effects of dietary phenolic compounds on tocopherol, cholesterol, and fatty acids in rats. Lipids. 2000;35:427–435. doi: 10.1007/s11745-000-541-y. [DOI] [PubMed] [Google Scholar]
- 40.Kamal-Eldin A, Pettersson D, Appelqvist LA. Sesamin (a compound from sesame oil) increases tocopherol levels in rats fedad libitum. Lipids. 1995;30:499–505. doi: 10.1007/BF02537023. [DOI] [PubMed] [Google Scholar]
- 41.Kontush A, Spranger T, Reich A, Baum K, Beisiegel U. Lipophilic antioxidants in blood plasma as markers of atherosclerosis: the role of alpha-carotene and gamma-tocopherol. Atherosclerosis. 1999;144:117–122. doi: 10.1016/s0021-9150(99)00044-1. [DOI] [PubMed] [Google Scholar]
- 42.Erbas M, Sekerci H, Gül S, Furat S, Yol E, Uzun B. Changes in total antioxidant capacity of sesame (Sesamum sp.) by variety. Asian J Chem. 2009;21:5549–5555. [Google Scholar]