

Abstract
Electronic cigarettes (ECIGs), also referred to as electronic nicotine delivery systems (ENDS) or ‘e-cigarettes’, generally consist of a power source (usually a battery) and heating element (commonly referred to as an atomizer) that vaporizes a solution (e-liquid). The user inhales the resulting vapor. ECIGs have been increasing in popularity since they were introduced into the US market in 2007. Many questions remain about these products, and limited research has been conducted. This review will describe the available research on what ECIGs are, effects of use, survey data on awareness and use, and the utility of ECIGs to help smokers quit using tobacco cigarettes. This review will also describe arguments for and against ECIGs, and concludes with steps to move research on ECIGs forward.
Keywords: electronic cigarette, review
INTRODUCTION
Electronic cigarettes (ECIGs) have been increasing in popularity since they were introduced into the US market in 2007 (Regan, et al., 2013). Sales for 2013 are expected to be over $1 billion (Rohbemed, 2013) and use rates are increasing among youth and adults (CDC, 2013; Pepper and Brewer, 2013). In addition, ECIGs are appearing in movies, on television, and in advertisements (e.g., Grana et al., 2011), and media coverage is increasing in the US and other countries (for example: in the UK and Scotland; Rooke and Amos, 2013). Popularity can also be measured by internet search queries; searches for ECIGs, compared to other smoking alternatives, have been increasing, most notably in the US (data from Google collected between 2008 – 2010; Ayers et al., 2011).
Although ECIGs are increasing in popularity, many questions remain about them, and limited research has been conducted. This paper describes the available research on ECIGs, including what they are, what they contain, studies in humans, survey data on awareness and use, and their utility for quitting smoking. This paper will also describe the current arguments for and against ECIGs, including opinions on regulation of these products. Finally, steps for moving forward will be outlined.
WHAT ARE ELECTRONIC CIGARETTES?
ECIGs, also referred to as electronic nicotine delivery systems (ENDS) or ‘e-cigarettes’, generally consist of a power source (usually a battery) and heating element (commonly referred to as an atomizer) that vaporizes a solution (e-liquid). The user inhales the resulting vapor. E-liquids contain humectants such as propylene glycol and/or vegetable glycerin, flavorings and usually, but not always, nicotine (Etter, 2012a). While most ECIGs contain the aforementioned basic components, there are a wide variety of ECIG models with substantial differences among them, such as the way in which the solution is stored, the method for heater activation, the electrical power flowing through (and dissipated by) the heater, and overall device appearance (see Figure 1).
Figure 1.
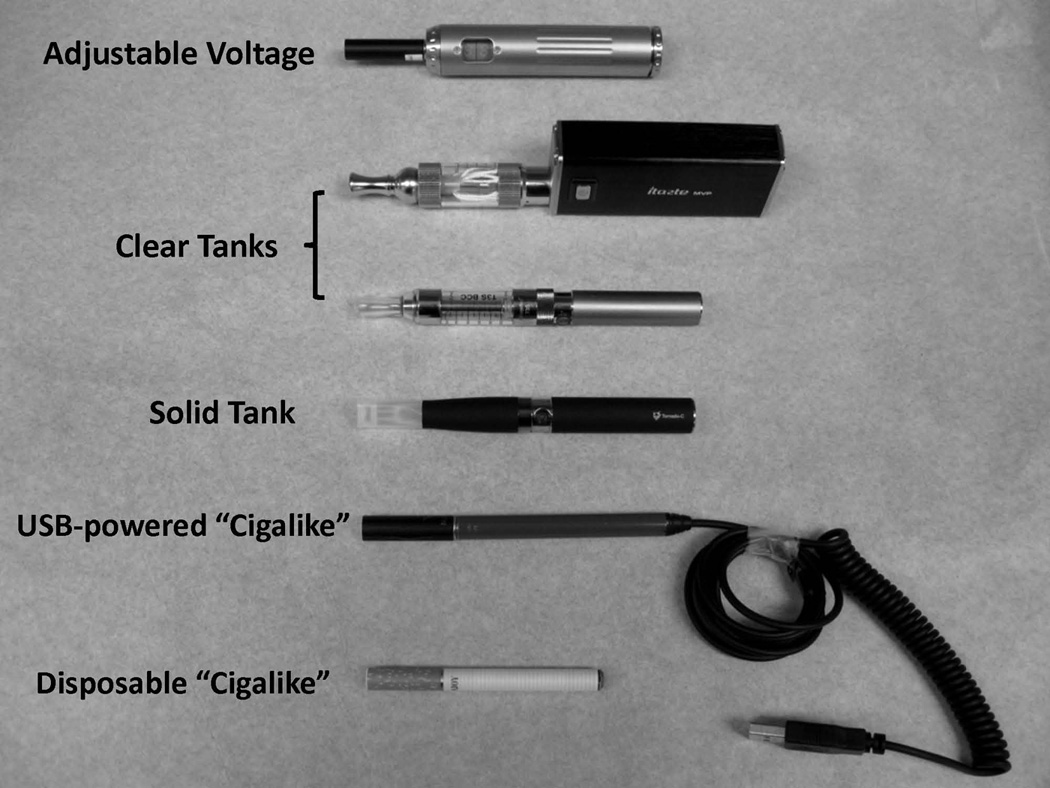
Some types of electronic cigarettes.
Electronic Cigarette Models
Perhaps the most well-known ECIGs are the cigarette-stylized models sometimes referred to as ‘cig-alikes’ (Cassidy, 2011). Cigarette-stylized models are designed so that their appearance resembles tobacco cigarettes closely. These models often are the same size and shape of a cigarette, and have a mouthpiece that looks like a cigarette filter (Cassidy, 2011). Cigarette-stylized models also typically have a light-emitting diode (LED) light at the non-mouth end that glows when the heating element is activated, and the heating element is often activated pneumatically (i.e., from the air pressure of the user’s inhalation; Etter, 2012a). The liquid solution is stored in a cartridge that often also contains the heating element. This solution/heater combination is referred to as a ‘cartomizer’, and cartomizers also contain other components such as fabric-like material that surrounds the heater. After the solution is depleted, certain cigarette-stylized models allow the user to replace or refill the cartomizer while others require the user to dispose of the entire ECIG (Cassidy, 2011).
Other ECIG models do not resemble cigarettes (Etter, 2012a) and use either a cartomizer or a “tank” system that stores the liquid in a reservoir (see Figure 1). Many of these models allow for manual rather than pneumatic heater activation, usually by pressing a button located near the mouth end of the device. In some ECIG models, users can alter the power flowing through the heater in an effort to alter characteristics of the resulting vapor (Etter, 2012a; Shihadeh et al., 2013). In another variation, users can drip liquid directly onto the heating element, also with the intent of altering vapor characteristics (McQueen, et al., 2011). The variability in ECIG design and use makes clear that ECIGs are not a single product but rather a class of products, and the rapid pace of design changes presents a challenge to understanding ECIG effects.
ELECTRONIC CIGARETTE SOLUTIONS (E-LIQUIDS)
Nicotine Concentrations
Another challenge to understanding ECIG effects is the variability across solutions intended for them. Solutions can be found for purchase over the internet in nicotine concentrations that range from 0 to 36 mg/ml, and with flavors that come in categories with labels such as tobacco (e.g., “classic”, “sahara”, “Cuban cigar”), menthol (e.g., “menthol ice”, “peppermint patty”), dessert (e.g., “cotton candy”, “bubble gum”, “cheesecake”), and fruit (e.g., “apple”, “raspberry”, “watermelon”; Vaperzone Inc., 2013). To add to the complexity, the actual nicotine concentrations may differ from the product labeling (Trehy et al., 2011). Moreover, some solutions are labeled with ‘low’, ‘medium’, or ‘high’ nicotine levels, but there is not a standard definition for these categories (Cameron, 2013). Indeed, there is even variation in nicotine levels between identical replacement cartridges of the same brand and manufacturer (Cheah et al., 2012). In some instances, trace amounts of nicotine have been detected in e-liquids advertised as containing 0 mg/ml of nicotine (Westenberger, 2009; Hadwiger et al., 2010; Trehy et al., 2011; Kubica et al., 2013).
Nicotine is a psychomotor stimulant that can cause severe side effects (Davies, 2001; CDC, 2005), including death (Corkery et al., 2010). Nicotine itself may also have cancer-promoting effects on the user, and may make traditional cancer treatments less efficacious (Warren and Singh, 2013). There is a health risk to adults and especially to children associated with the availability of this drug in solutions that are labeled and flavored as candy, dessert, or fruit and in vials that may contain toxic doses (e.g., 1,080 mg nicotine in a 30 ml bottle of 36 mg/ml “Tutti Fruti Gumball”; Vaperzone Inc., 2013). Another concern is that some ECIG users mix their own solutions to customize flavors and/or nicotine concentrations (Etter, 2012a). Mixing solutions in a non-sterile environment carries the risk of contamination, and failure to use proper safety clothing and procedures could lead to accidental nicotine poisoning.
Additionally, four attempted suicides by e-liquid ingestion have been recorded (Cervellin et al., 2013; Christensen et al., 2013). Reportedly, one individual attempted suicide by e-liquid ingestion on two occasions (ingesting 360 mg and 1,500 mg of nicotine respectively); both led to nausea and vomiting. Another individual, age 13, ingested 3 ml of nicotine of an unknown concentration and experienced similar symptoms (Christensen et al., 2013). Another individual apparently attempted suicide by injecting approximately 3 mg of nicotine solution mixed with liquid methadone in addition to orally ingesting roughly 34 mg of e-liquid (Cervellin et al., 2013). One fatality due to e-liquid ingestion has been reported: a two-year old child orally ingested an unknown quantity and concentration of e-liquid (Eisenbud, 2013).
Other E-liquid Ingredients
In addition to nicotine, ECIG solutions contain several other potentially dangerous ingredients, most prominent of which are the humectants (propylene glycol and/or vegetable glycerin: Uryupin et al., 2011; Cheah et al., 2012; Pellegrino et al., 2012). When heated, propylene glycol and vegetable glycerin produce carbonyls such as acetaldehyde, formaldehyde, and acrolein that are toxic to the user (Uchiyama et al., 2010). Also, inhalation of vegetable glycerin can result in lipoid pneumonia, although there have only been two recorded cases in ECIG users (Etter, 2012a; McCauley et al., 2012). Similar to nicotine, there is considerable variability in the concentrations of humectants in e-liquids across brands and manufactures (Cheah et al., 2012). Unfortunately, there are no data concerning the effects on the human lung of hundreds of daily inhalations of these humectants over the course of many years.
Certain ECIG solution flavorings may also be toxic (Bahl et al., 2012; Behar et al., 2013). One study assessed the cytotoxicity of 35 different e-liquids of varying flavors (including cinnamon, butterscotch, caramel, menthol, and bubblegum) and nicotine concentrations (0 mg – 24 mg) in human embryonic and adult cells. Embryonic cells were generally more sensitive to the ECIG solutions, but no correlation was found between nicotine dose and cytotoxicity for either type of cell. Alternatively, within particular flavors (such as butterscotch and caramel) cytotoxicity was highly variable and correlated positively with flavor concentration (Bahl et al., 2012). Cinnamon-flavored ECIG solutions were the most cytotoxic (see also Behar et al., 2013). Propylene glycol and vegetable glycerin alone were not cytotoxic, but the authors noted that prolonged inhalation of humectants may still pose health risks (Bahl et al., 2012).
Tobacco-specific nitrosamines (TSNAs), potent carcinogens found in tobacco smoke, have also been detected in ECIG solutions, again in a variety of concentrations (Laugesen et al., 2008; Westenberger, 2009; Kim et al., 2013). Reports sponsored by ECIG manufacturers have suggested TSNAs are only present in trace amounts, thus posing no health risk (Laugesen, 2008). Other research has suggested TSNAs are present across a wide variety of solutions (Kim et al., 2013), although the meaning of the levels reported is unclear. Differences in measurement make comparisons across these studies difficult.
ELECTRONIC CIGARETTE VAPOR
Toxicants
ECIGs do not cause combustion when operated normally, and therefore do not produce some of the toxicants (such as carbon monoxide and polycyclic aromatic hydrocarbons) produced by tobacco cigarettes (Goniewicz et al., 2013). In fact, some research suggests ECIG vapor is considerably less toxic than cigarette smoke. In one study, the cytotoxicity of ECIG vapor generated from a “510 T” ECIG was investigated by exposing rodent fibroblasts to it (Romanga et al., 2013). The vapor from only one of the 21 ECIG solutions examined had cytotoxic effects, and all fibroblasts exposed to ECIG vapor were significantly more viable than those exposed to cigarette smoke. Fibroblast cells are critical for tissue healing and constructing the structural framework of animal tissues, and research has shown that cigarette smoke decreases the efficacy of fibroblasts, which diminishes the repair of damaged lung tissue (Carnevali et al., 1998).
However, potentially hazardous substances found in cigarette smoke have also been detected in ECIG vapor, albeit in varying and lesser amounts (McAuley et al., 2012; Schripp et al., 2012; Goniewicz et al., 2013). In one study, vapors were generated from 12 different brands of e-cigarettes and analyzed for four groups of common cigarette smoke toxicants (carbonyls, volatile organic compounds, TSNAs, and metals). All four toxicant groups were detected in ECIG vapor, but the levels of the toxicants present ranged from nine to 450 times lower than conventional cigarette smoke, and in many instances the toxicant levels from ECIG vapor were comparable with trace levels generated by the nicotine inhaler (Goniewicz et al., 2013; Table 1). Overall, the extant data support the notion that ECIG vapor contains fewer tobacco toxicants than does tobacco cigarette smoke while, at the same time, containing more tobacco toxicants than air. The extent to which chronic, long-term exposure to ECIG toxicants does or does not cause dependence, disability, disease, and death is unknown.
Table 1.
Toxicant levels in conventional cigarettes (Counts et al., 2005) and 12 brands of ECIGS (Goniewicz et al., 2013).
| Toxic compound | Conventional cigarette (µg in mainstream smoke) |
Electronic cigarette (µg per 15 puffs) |
|---|---|---|
| Formaldehyde | 1.6–52 | 0.20–5.61 |
| Acetaldehyde | 52–140 | 0.11–1.36 |
| Acrolein | 2.4–62 | 0.07–4.19 |
| Toluene | 8.3–70 | 0.02–0.63 |
| NNN (N′-nitrosonornicotine) | 0.005–0.19 | 0.00008–0.00043 |
| NNK (4-methylnitrosoamino-1-3-pyridyl-1-butanone) | 0.012–0.11 | 0.00011–0.00283 |
Environmental Exposure
The visible vapor produced from ECIGs raises concerns about environmental exposure. One study examined air quality after producing vapor from various ECIGs and detected traces of volatile organic compounds (VOCs), flavoring substances (diacetin), propylene glycol, glycerol, and nicotine (Scripp et al., 2012). However, the toxicant levels detected in the air after ECIG use were significantly lower than the toxicant levels after conventional cigarette use, and the different ECIGs tested produced variable toxicant levels. Other research, funded by a pro-ECIG organization, concluded that there are toxicants in ECIG vapor that are emitted into the air, but at far lower levels than conventional cigarettes (McAuley et al., 2012). In addition, ECIGs emit significantly lower amounts of particulate matter relative to tobacco cigarettes, suggesting a lower risk of environmental vapor exposure (Pellegrino et al., 2012).
HUMAN LABORATORY STUDIES
Studies involving human participants allow for another level of understanding of ECIGs, in terms of physiological effects on the user, tobacco abstinence symptom suppression, smoking behavior (puff topography), cognitive effects, and abuse liability.
Physiological Effects
Pulmonary Function
The long term effects of ECIG use on lung function remain unclear, but some research with a few ECIG models suggests that ECIGs produce short-term adverse effects on pulmonary function similar to acute adverse effects observed from cigarette smoking. For example,Vardavas et al. (2012) found that after five minutes of using a Nobacco “black line” ECIG with 11 mg/ml nicotine solution, users exhibited decreases in exhaled nitric oxide (FENO) and increases in total respiratory resistance, total respiratory impedance, and peripheral airway resistance; all of these outcomes are common acute effects associated with cigarette smoking. Conversely,Flouris et al. (2013) concluded that the ECIGs used in their study did not impair lung function acutely after active or passive use (second-hand exposure). Another study similarly concluded that active ECIG use of one particular brand produced no acute lung deficiencies (Chorti et al., 2012). The variety of devices and e-liquids available make generalizations difficult. Different product combinations may induce greater or lesser acute and long-term effects.
Nicotine Delivery
Inhaled nicotine produces similar acute physiological effects on the user (increases heart rate and blood pressure), whether it is delivered from an ECIG (Vansickel et al., 2013) or a tobacco cigarette (Rhee et al., 2007). However, ECIGs do not always deliver nicotine to the user with the same efficacy. Research using inexperienced ECIG users has shown that some ECIGs do not deliver nicotine in measurable amounts (Vansickel et al., 2010). Alternatively, at least some brands of ECIGs can deliver nicotine to experienced users under certain conditions (Dawkins and Cocoran, 2013; Vansickel and Eissenberg, 2013; Farsalinos, Spyrou, Tsimopoulou, Stefapoulos, Romanga, & Voudris, 2014). In some cases, the amount of nicotine delivered to the experienced ECIG user can reach plasma concentrations that approximate those seen after cigarette use (Vansickel and Eissenberg, 2013; see Figure 2).
Figure 2.
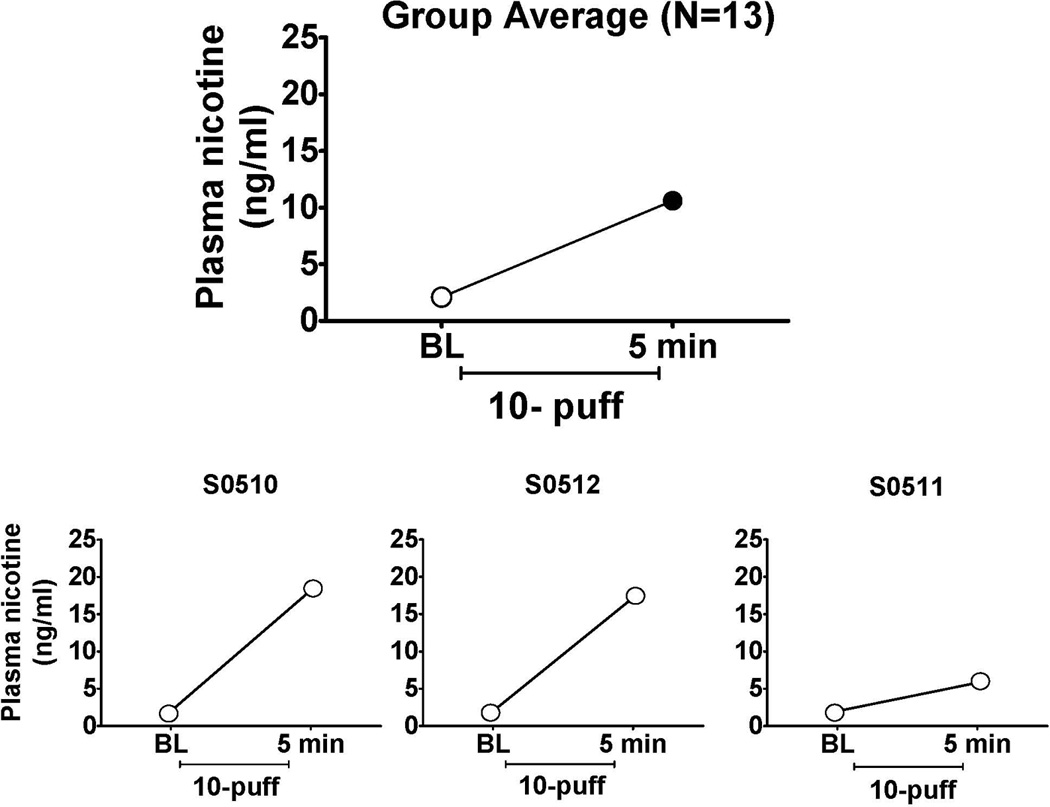
Plasma nicotine concentrations in ECIG users. Top panel shows the mean plasma nicotine concentration before and after thirteen experience ECIG users took 10 puffs (30 second interpuff interval) from their preferred device using a cartomizer loaded with their preferred liquid (for methodological detail, see Vansickel & Eissenberg, 2012). Filled symbol indicates a significant difference in plasma nicotine after the 10 puffs [t (12) = −5.3, p < .001]. The lower three panels show the plasma nicotine data from three individuals who participated in this study and who each took 10 puffs using the same device and liquid strength (26 mg/ml). These data demonstrate that ECIGs can deliver cigarette-like doses of nicotine to their users, but that there may be considerable variability in nicotine delivery across users of the same device/liquid.
These discrepancies associated with ECIG nicotine delivery could be explained by the apparent learning curve associated with ECIG users’ puff topography. Puff topography commonly is used to assess nicotine self-administration in cigarette smokers, and involves measuring variables such as puff volume, duration, number, and interpuff interval (Puustinen et al., 1987; Breland et al., 2002; Blank et al., 2009). Specifically, the few studies that have addressed this topic suggest that experienced ECIG users take longer puffs (about 4 seconds) whereas ECIG-naïve cigarette smokers tend to take shorter puffs (about 2 seconds), similar to tobacco cigarette puff durations (Hua et al., 2011; Farsalinos et al., 2013). In addition, ECIGs require stronger vacuums (suction from the user) relative to conventional cigarettes (Trtchounian et al., 2010). ECIG use behavior may depend on a variety of factors, including nicotine product design features, in a manner akin to how smoking behavior can depend on cigarette design features (e.g., compensatory behaviors observed when smokers of cigarettes with unventilated filters switch to those that have ventilated filters; Benowitz, 2001). More research on this topic is needed to understand how user behavior and device operating characteristics interact to influence delivery of nicotine and other toxicants.
Experienced ECIG users also vary considerably in their ability to obtain nicotine from ECIGs (Dawkins and Corcoran, 2013; Vansickel and Eissenberg, 2013). Individual differences in nicotine yield may be due to nicotine being converted to vapor with differing consistencies and efficacies across brands and models (Westenberger, 2009; Goniewicz et al., 2012). Individual differences in nicotine plasma concentrations may also be due to differences in experienced users’ puff topography. Some experienced users may never learn to increase their puff durations and/or lower their puffing flow rates to obtain nicotine reliably, suggesting there may be some behavioral components that are relevant (see Figure 2).
Psychological Effects
Subjective Effects
ECIGs can reduce tobacco abstinence symptoms in cigarette smokers (e.g., Bullen et al., 2010; Vansickel et al., 2010; Dawkins et al., 2013), but the extent to which this abstinence symptoms suppression is explained by nicotine delivery and/or explained by the behavioral stimuli that accompany ECIG use remains unclear. For example, some ECIGs have been shown to decrease tobacco abstinence symptoms significantly without actually delivering nicotine to the user (Vansickel et al., 2010). Likewise, ECIGs with and without nicotine did not differ in their ability to reduce the desire to smoke in women, though in men nicotine-containing ECIGs were more effective at reducing the desire to smoke (Dawkins et al., 2012).
Commonly reported negative effects of ECIGs include throat and mouth irritation, and dry cough (Bullen et al., 2010; Caponetto et al., 2013; Chen, 2013; Polosa et al., 2013). Other less frequently reported side effects include nausea, dry mouth, headaches, and dizziness. Reports of more serious adverse effects commonly associated with tobacco cessation such as depression, insomnia, and anxiety thus far have been rare (Polosa et al., 2013). In one study, serious adverse events in ECIG users included hypotension, seizure, chest pain, rapid heartbeat, disorientation, and congestive heart failure but the extent to which these effects were attributable to ECIG use was unclear. Less severe adverse events included sore throat, abdominal pain, headache, blurry vision, cough, and nausea/vomiting (Chen, 2013).
Cognitive Effects
Deficits observed in cognition and concentration in smokers as a result of acute smoking cessation can be improved via nicotine administration (Heishman et al., 2010). To date, only two ECIG studies have used cognitive outcome measures. In the first study, “White Super” “cig-alikes” containing 18 mg/ml of nicotine improved working memory relative to placebo ECIGs of the same brand in nicotine-dependent abstinent smokers (Dawkins et al., 2012). In another study (Dawkins et al., 2013), abstinent cigarette smokers using 18 mg/ml “Tornado” ECIGs (which were not “cig-alikes”) showed significant improvement in prospective memory relative to those using placebo. However, nicotine ECIGs only improved time-based and not event-based prospective memory. More work is needed to understand the effects of ECIGs on the cognitive function of all those who may use them.
Abuse liability
The potential for ECIG abuse has been examined behaviorally in humans in one study that combined subjective effects assessment with a behavioral task known as the multiple choice procedure (Vansickel et al., 2012). In one study session, cigarette smokers sampled a “Vapor King” “cig-alike” containing 18 mg/ml of nicotine solution, and then chose between taking 10 puffs of an ECIG and varying amounts of money. In a second session, participants choose between 10 puffs of their own brand of cigarette and varying amounts of money. The abuse potential of the product (i.e. ECIGs or tobacco cigarettes) was assessed by observing the maximum value of money at which the product was chosen over money (i.e., the cross-over value). The average crossover value for ECIGs was $1.06 as opposed to $1.50 for own brand cigarettes, suggesting that for these smokers, their own brand of cigarettes was more reinforcing (and had more abuse potential) relative to the particular brand/strength of ECIG tested (Vansickel et al., 2012). This single study of the abuse liability of one ECIG brand is hardly sufficient to address the issue. A comprehensive approach to determining ECIG abuse liability would include a variety of assessment methods across many populations of interest with varying experience with nicotine delivering products and the full range of ECIG devices/liquids on the market. Thus, a program of research addressing this issue is needed now.
In addition, other methods for misusing ECIGs as nicotine delivery devices may arise, and learning about them will be critical for monitoring the likely individual and public health effects of ECIGs. In terms of using ECIGs to deliver drugs other than nicotine, there have been reports in the media regarding this phenomenon, there are sections of the internet devoted to the topic, and a recent press release suggests that at least on ECIG vendor is developing a product with this goal in mind (e.g., VaporBrands International, 2014). At this writing there are no empirical investigations of this behavior.
USE OF ELECTRONIC CIGARETTES AMONG ADULTS AND ADOLESCENTS
Survey Data on Awareness and Use of Electronic Cigarettes—US Adults
Several national surveys of US adults (including smokers and non-smokers) that assessed ECIG use have been conducted since 2009. Although the surveys differ in items and sampling methods, a trend toward increased awareness and use of ECIGs is clear. For example, a national survey of US adults was conducted in 2009 and 2010; results showed that awareness of ECIGs increased from 16% in 2009 to 32% in 2010 (Regan et al., 2011). Furthermore, the percentage of respondents who had ever tried an ECIG increased from 0.6% in 2009 to 2.7% in 2010 (Regan et al., 2011). Similarly, a nationally representative survey was conducted in 2010, and results indicated an ECIG awareness rate of 40%, and an ECIG ever use rate of 3% (Pearson et al., 2012). Another nationally representative survey (also conducted in 2010) showed that 2% of respondents had tried an ECIG (McMillen et al., 2012). Finally, another national survey of US adults reported that awareness was 39–40% in 2010, and increased to 58% by 2011. Ever use of ECIGs increased from 2% in 2010 to 6% in 2011 (King et al., 2013).
Most ECIG users appear to be smokers of conventional cigarettes (Regan et al., 2011; McMillen et al., 2012; Pearson et al., 2012; King et al., 2013). Other data shows that “dual users” of tobacco (users of both cigarettes and cigars) are more likely to have ever used ECIGs, compared to those who only smoke cigarettes (Richardson et al., 2012). Indeed, data collected in 2010–2011 revealed that most current and former cigarette smokers were aware of ECIGs (73%), and that 15% had tried them and 6% were current users (Adkison et al., 2013). Understanding the prevalence of ECIG and other tobacco use (e.g., dual use of ECIGs and cigarettes) is particularly important. To the extent that ECIG availability helps to maintain smoking of cigarettes and other tobacco products (e.g., by allowing nicotine dependent users to self-administer nicotine where combustible tobacco products are banned), these products could maintain or increase the individual and public health threat associated with tobacco use.
Survey Data on Awareness and Use of Electronic Cigarettes—US Adolescents and Young Adults
A few studies have examined ECIG use among US youth and young adults. Most notably, data from the 2011–2012 National Youth Tobacco Survey showed a large increase in ECIG use among middle school and high school students. From 2011 to 2012, ever use among all students (grades 6–12) increased from 3.3% to nearly 7%. In 2012, 9.3 % of students who reported ever use of ECIGs also reported never smoking tobacco cigarettes (CDC, 2013). Another study (done in 2011) used a small national sample of adolescent males aged 11–19. Awareness of ECIGs was also high (67%), although ever use was low (less than 1%; Pepper et al., 2013).
Other studies have focused on young adults, and rates of ever use of ECIGs range from 2% to 13%, depending on the study and year data were collected. In one nationally representative survey, 2.5% of young adults aged 18–24 reported ever use of ECIGs (McMillen et al., 2012). Survey data from young adults (aged 20–28) from the Midwestern US, collected in 2010–2011, showed that most were aware of ECIGs (70%), 7% had ever tried them, and 1% had used them in the past 30 days (Choi and Forster, 2013). Additional data from the same survey showed that those adolescents who had beliefs that ECIGS are less harmful than traditional cigarettes were more likely to experiment with ECIGs (Choi & Forster, 2014). Survey data from young adults attending colleges in North Carolina in 2009 revealed that nearly 5% of students reported ever using an ECIG (Sutfin et al., 2013). In addition, while ECIG users were most likely to be smokers of conventional cigarettes, the authors reported a concerning finding: 12% of those who had tried ECIGs were never-smokers of conventional cigarettes (Sutfin et al., 2013). One recent study examined the possibility that youth who experiment with ECIGs may have a greater chance of cigarette use (Dutra et al., 2014), but more work is needed. Finally, a survey of one class of college students (aged 19–22) was conducted at one Colorado university. Most had heard of ECIGs (71%), and fewer (13%) had tried them (Trumbo and Harper, 2013).
Survey Data on Awareness and Use of Electronic Cigarettes—Other Countries
A number of other studies have examined ECIG awareness and use in countries other than the US, including: the UK, Canada, Australia, Korea, Switzerland, France, Belgium, Poland, China, the Czech Republic, and New Zealand. For example, a nationally representative survey from Great Britain (data collected in 2010 and 2012) showed increased use and awareness during that period (Dockrell et al., 2013). Also, most ECIG users were current smokers (6.7% of smokers were also current ECIG users, compared to 0.1% of never-smokers who were current ECIG users; Dockrell et al., 2013). Survey data of young men from Switzerland, collected between 2010 and 2013, showed that nearly 5% had ever tried ECIGs (Douptcheva, Gmel, Studer, et al., 2013). In that study, most current users of ECIGs were also current cigarette smokers (89.2% were current smokers; Douptcheva, Gmel, Studer, et al., 2013).
Surveys assessing ECIG awareness and use also have been conducted internationally among current and former cigarette smokers. For example, a nationally representative survey of current and former cigarette smokers, conducted in the UK, Canada, Australia, and the US revealed lower awareness of ECIGs in non-US countries (20–54%, compared to 73% in the US), and lower ever use of ECIGs in Canada and Australia compared to the US and UK (Adkison et al., 2013). Current and former smokers in New Zealand have also been surveyed about ECIG use. Few (7%) reported ever purchasing an ECIG; those who were aged 18–24 were more likely to have purchased one (Li et al., 2013). Another survey of current smokers (using a convenience sample of individuals seen smoking or purchasing cigarettes) was conducted in the Czech Republic. Many reported ever use of an ECIG (50%) and approximately 9% reported regular use (Kralikova et al., 2013).
Fewer ECIG-relevant surveys have been conducted with adolescents from non-US countries. Cho et al. (2011) analyzed data collected in 2008 from middle and high school students in Korea (average age = 14 – 16.5 years). About 10% were aware of ECIGs, and less than 1% had ever tried an ECIG.
DO ELECTRONIC CIGARETTES HELP PEOPLE QUIT SMOKING?
Each year, 69% of tobacco cigarette smokers say they want to quit (CDC, 2011), and 52% make a quit attempt (CDC, 2012). However, relapse rates are very high—most smokers will fail to quit smoking (approximately 6% are successful; CDC, 2011). Existing smoking cessation methods can help to a certain extent: behavioral methods can increase quit rates to 11–16%, and medications, such as nicotine replacement therapy (NRT) can help increase quit rates to 20 or 30% (Fiore et al., 2008). Clearly, more effective tobacco cessation methods are needed.
One issue that current behavioral methods and medications techniques do not address (and which may be a cause for low success rates; Caldwell et al., 2012) is replacement of the non-nicotine stimuli to which smokers are accustomed, such as hand-to-mouth movement, the feeling of nicotine/tobacco at the back of the throat, and the sight/feel/taste of smoke. These non-nicotine stimuli suppress tobacco abstinence symptoms in cigarette smokers (Buchhalter et al., 2005; Donny et al., 2007). ECIGs may address some of these non-nicotine stimuli, in addition to delivering nicotine (under some conditions), and thus theoretically could be a useful cessation method. Importantly, ECIGs currently are not marketed explicitly in the US as smoking cessation aids. However, some individuals report using them to quit smoking, and a few studies have examined their utility for smoking cessation.
Electronic Cigarettes and Cessation: Users’ Perceptions
Most studies on the use of ECIGs as an aid to quitting smoking have reported on ECIG users’ perceptions. For example, ECIG users appear to believe that ECIGs can assist with quit attempts; an online survey of Polish ECIG users reported that 41% said they had tried ECIGs in an effort to quit smoking (Goniewicz et al., 2012). Similarly, a representative survey in Great Britain of current smokers (over one third of whom had used ECIGs) showed that 51% said that they believed that ECIGs could help them give up smoking (Dockrell et al., 2013). Cigarette smokers also have favorable perceptions of ECIGs as a method to quit smoking. Among conventional smokers and recent quitters in New Zealand, over half reported that they would use ECIGs to quit smoking conventional cigarettes (Li et al., 2013).
Some ECIG users report that ECIGs helped them quit or reduce smoking conventional cigarettes. For example, an online survey of ECIG users (first-time purchasers) showed that 31% reported quitting smoking six months after purchasing an ECIG (Siegel et al., 2011). Results from another online survey of ECIG users (recruited from ECIG websites) showed that 74% of respondents reported quitting smoking conventional cigarettes for several weeks or months (Dawkins et al., 2013). A study of daily cigarette smokers in Hawaii showed that 13% had used ECGs to quit smoking (Pokhrel et al., 2013). Data from several studies (conducted in the US and in other countries) shows that many or most ECIG users (recruited from a meeting of ECIG enthusiasts, from ECIG discussion forums, and from state tobacco quitlines, respectively) surveyed use ECIGs to quit smoking (Foulds et al., 2011; Goniewicz et al., 2012; Vickerman et al., 2013) and/or to reduce use of conventional cigarettes (Kralikova et al., 2013). One longitudinal study using an international sample (recruited from various ECIG and smoking cessation websites) found that at one year follow-up, 46 % of those who had initially reported daily or occasional dual use of ECIGs and cigarettes had stopped smoking cigarettes (Etter and Bullen, 2014). However, the relevant sample size at follow-up was small (N=35) and cessation was not verified biochemically. While these findings are encouraging, the results must be interpreted with caution. Many of the studies used samples recruited from ECIG websites, ECIG forums or meetings of ECIG enthusiasts. Thus, it is possible that in some studies, respondents were biased, as individuals visiting ECIG websites, forums, and meetings likely have favorable views of ECIGs.
Other survey data may cast some doubt on ECIGs as cessation tools. A nationally representative survey of smokers showed that interest in ECIGs was high among those who intended to quit, but unsuccessful quitters were more likely to have tried ECIGs, compared to successful recent quitters (Popova and Ling, 2013). Of course, there are multiple explanations for this finding-- unsuccessful quitters may be trying more methods (including ECIGs). As the authors note, the study was not designed to determine if ECIGs can lead to more quit attempts. Similarly, data collected from tobacco quitline callers in six US states revealed that ECIG users were less likely to have actually quit using tobacco, compared to respondents who had never used ECIGs (Vickerman et al., 2013). Again, this finding must be interpreted with caution, as those using ECIGs may in fact be less likely to quit, or may be individuals who are having more difficulty quitting use of conventional tobacco products (Vickerman et al., 2013).
Electronic Cigarettes and Cessation: Case Reports and Clinical Trials
One case series and one case report on the use of ECIGs as a method to quit smoking have been published. Caponnetto et al., (2011) described the experience of three cigarette smokers using ECIGs to quit smoking. All were heavy smokers who previously had tried to quit smoking. All three were able to quit smoking by using an ECIG and remain abstinent for at least 6 months. In addition, Schneiderhan (2013) published a case report describing a cigarette smoker who reportedly was able to quit smoking by using a combination of ECIGs and nicotine lozenges.
Only five studies have assessed whether or not EICGs can help cigarette smokers to quit smoking, and of those five studies, only two were randomized trials with a control condition. First, Polosa et al., (2011) published a single-arm, uncontrolled study of 40 cigarette smokers who did not want to quit smoking (27 completed the study), who were given a “cig-alike” ECIG with 7.4 mg cartridges to use over six months. Six months after enrolling, about a third were able to reduce their cigarette use by 50% or more, and 23% were able quit smoking cigarettes completely. A second single-arm, uncontrolled study was conducted with schizophrenic smokers who were not willing to quit smoking. Participants (N = 14) were given a “cig-alike” ECIG with 7.4 mg cartridges to use over 1 year (Capponetto et al., 2013). Half of the participants reduced their smoking of conventional cigarettes by 50%, and also reduced their carbon monoxide levels. Two participants were able to quit smoking (Capponetto et al., 2013). In another single-arm, uncontrolled trial of smokers not wanting to quit, the authors reported that participants were able to reduce their use of conventional cigarettes by 44% over a 1-week period of using ECIGs (participants used several “cig-alike” ECIG types and a variety of nicotine doses; Wagener et al., 2013). Two of these three studies used expired air carbon monoxide to biochemically verify smoking reduction or smoking cessation (Polosa et al., 2011; Capponetto et al., 2013).
Ideally, determining whether or not ECIGs are effective cessation devices will be done with randomized, controlled trials, using a representative group of smokers. These trials should use biochemical verification of cigarette abstinence (Hughes et al., 2003), biochemical assessment of nicotine delivery during the trial (e.g., via urine analysis of the nicotine metabolite cotinine), assessment of puffing behavior (as it may influence nicotine delivery), adequate duration of treatment, and long-term follow-up (i.e., six months or more).
Two randomized controlled trials have been published to date. One trial randomized 657 smokers who wanted to quit smoking to one of three arms: Elusion ECIGs (a “cig-alike” product) with 16 mg nicotine, nicotine patches, or Elusion ECIGs with no nicotine (placebo ECIGs; Bullen et al., 2013a; Bullen et al., 2013b). Participants who were randomized to nicotine patches were given a voucher for the patches that they needed to redeem at a pharmacy. All participants were followed for six months. Overall, ECIGs helped 7% of the participants to quit smoking, compared to 6% who quit smoking with the nicotine patches and 4% with the placebo ECIG. Another trial randomized 300 cigarette smokers who did not want to quit smoking to three arms: Categoria ECIGs (a “cig-alike” product), with 7.2 mg nicotine for 12 weeks, Categoria ECIGs with 7.2 mg nicotine for 6 weeks and then Categoria ECIGs with 5.4 mg nicotine for another 6 weeks, or placebo Categoria ECIGs for 12 weeks (Caponnetto et al., 2013). Participants were followed for one year in total. Results showed that all of the ECIG groups showed a reduction in smoking, although no differences were observed across arms in terms of quit rates. Some participants did quit smoking completely: 11% at 12 weeks and 9% at one year (Caponnetto et al., 2013). Both studies used expired air carbon monoxide to verify cigarette abstinence.
Obviously, a discrepancy exists between ECIG users’ reports about quitting smoking and the evidence from the clinical trials available. As noted earlier, surveys of ECIG users may be biased, as they recruit from websites frequented by EICG enthusiasts, and results are based on self-report (Odum et al., 2012). Also, both of the published randomized controlled trials used ECIGs with low to moderate doses of nicotine, which may have impacted the quit rates reported (because low nicotine levels may not have suppressed withdrawal adequately, leading participants to return to conventional cigarettes). In addition, neither study measured nicotine delivery biochemically during the trial in all participants (e.g., via plasma nicotine sampling and analysis) to determine if the devices were actually delivering nicotine to the blood. Also, neither study assessed whether the users were puffing in a way that could maximize nicotine delivery. Finally, some methodological issues may explain the cessation rates observed in these studies. For example, in one of them, participants randomized to the nicotine patch condition were required to use a voucher to obtain this treatment, and the nicotine patch itself is a less flexible method of dosing than either ECIGs or other cessation medications; Bullen et al., 2013a). Overall, based on the limited research available, whether or not ECIGs can help the majority of smokers quit smoking is still unclear.
ARGUMENTS FOR AND AGAINST ELECTRONIC CIGARETTES
ECIGs have fueled the already fiery debate on tobacco harm reduction and there are far more opinions than there are data to support them. There are arguments in favor of ECIGs as a revolutionary product to increase smoking cessation rates, as well as arguments against ECIGs, for their potential to revive interest in conventional cigarettes, as well as other concerns. Both sides are presented below.
Arguments for Electronic Cigarettes
Proponents of ECIGs argue that getting conventional tobacco smokers to switch to alternative tobacco products, such as ECIGs, is a viable and useful harm reduction strategy that could reduce tobacco-related morbidity and mortality significantly (e.g., Phillips, 2009; Hajek, 2012). This reduction, if it is achieved, would be critical, as existing techniques/medications for quitting smoking are associated with fairly low levels of success. Proponents also argue that existing research regarding the ingredients in the ECIG solutions and the toxicant content of the vapor is sufficient to demonstrate that toxicants in ECIGs are orders of magnitude lower than tobacco cigarettes and ECIG toxicity is comparable to other nicotine replacement products (Cahn and Siegel, 2011).
Arguments against Electronic Cigarettes
Opponents of ECIGs have a variety of concerns. First, opponents of ECIGS are not convinced of their long-term safety (e.g., Cobb et al., 2010) and/or note potential harm (Trtchounian and Talbot, 2011; Avdalovic and Murin, 2012). Second, opponents of ECIGs argue that cigarette smokers should use current, evidence-based strategies to quit smoking (such as nicotine replacement treatment, non-nicotine medications, and psychosocial techniques; Cobb and Abrams, 2011). Third, opponents are concerned that ECIGs may become popular with youth, leading to nicotine exposure and potentially, switching to conventional cigarettes (Cobb et al., 2010; Grana, 2013). Fourth, opponents worry that tobacco companies can’t be trusted to market ECIGs (based on their past behavior), and will use EICGs to try to maintain conventional cigarette use among smokers (Chapman, 2013). Also, as stated earlier, dual use of ECIGs and tobacco cigarettes allows nicotine dependent users to self-administer nicotine where combustible tobacco products are banned, thus possibly decreasing the likelihood of successful quit attempts and potentially allowing a renormalization of tobacco cigarette smoking. A final concern is that ECIG use among former smokers may lead to relapse to tobacco use (Yamin et al., 2010).
Opinions on Electronic Cigarette Regulation
ECIGS are unregulated in many countries, although, in the US, the FDA soon may begin to regulate them as tobacco products. In Canada, nicotine-containing ECIGs are regulated like other drugs, and sellers must obtain market authorization by the government (no nicotine-containing ECIGs are currently legally sold). Many ECIG proponents and opponents agree that some type of regulation is important. Some argue that ECIGs should be removed from the market until regulated (Cobb, 2010, 2012), others argue that they should be available but regulated closely (e.g., restricted advertising, no sales to minors; Borland, 2011; Kamerow, 2013). Foulds and Veldheer (2011) argue that some regulation is necessary, to ensure quality control. Others argue that some types of regulation (e.g., regulating EICGs as medical devices, or prohibiting them altogether) would hinder the use of ECIGs as an effective harm reduction strategy (Etter, 2013; Etter, 2012b; Wagener et al., 2012), or that overly restrictive regulation could actually benefit the tobacco industry (Abrams, 2014).
CONCLUSION: THE ROLE OF SCIENCE IN UNDERSTANDING ELECTRONIC CIGARETTES
The most important roles that science can play in the current ECIG debate are to identify and then fill the substantial knowledge gaps that exist today. The review of the literature presented here highlights clearly that very little is known about the acute and longer-term effects of ECIG use for individuals and the public health, especially given the dramatic variability in ECIG devices, liquids, and user behavior. For example, the few published studies examining ECIG toxicant content, yield, delivery, and effects on users involved a very limited set of devices and liquids; detailed analysis of user behavior (e.g., puff topography) has been absent. Similarly, the few published clinical trials have used ECIG device/dose combinations that likely did not deliver cigarette-like doses of nicotine to participants, and also did not provide instructions to participants on how to extract nicotine effectively (whatever those instructions might be). No existing studies address the extent to which the inhalation of ECIG vapor hundreds of times every day over a period of multiple years influences human health, particularly pulmonary function. The extent to which tobacco cigarette smokers use ECIGs as a supplement or substitute for combustible tobacco has been addressed only recently, and, again, the extant data do not address the variability of products and populations. Thus, any generalizations of the small body of work reviewed here to the entire ECIG landscape and to the long-term effects in individuals and to public health are premature.
Given today’s inability to generalize across ECIGs, individuals, and populations, all stakeholders in the ECIG debate (producers, users, researchers, regulators), regardless of their opinions concerning the public health effects of ECIGs, must acknowledge that there is much to be learned about this rapidly evolving product category. Similarly, all stakeholders must acknowledge that generalization in the absence of data is speculation, not science. We must all recall that the dramatic gains in individual and public health achieved over the past two centuries have come from following some basic procedures: forming hypotheses, testing them objectively and empirically, and drawing conclusions based on the resulting data. Fortunately, there have been many similar calls for this scientific approach (e.g., Cobb et al., 2010; Etter, Bullen, Flouris, Laugesen, & Eissenberg, 2011; Flouris and Oikonomou, 2010; Henningfield and Zaatari, 2010; Yamin et al., 2010; Lee et al., 2011; Noel et al., 2011; Hastings et al., 2012; Wagener et al., 2012; Chapman, 2013; Kamerow et al., 2013), and resources are being devoted to this topic in the U.S. and elsewhere. Everyone is aware of the individual and public health benefit of a product that could eliminate or at least reduce substantially tobacco-caused disability, disease, and death. No one can say today with scientific certainty the extent to which ECIGs are or will become that product.
Acknowledgement
Research reported in this publication was supported by the National Institute on Drug Abuse of the National Institutes of Health under Award Number P50DA036105 and the Center for Tobacco Products of the U.S. Food and Drug Administration. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health or the Food and Drug Administration."
REFERENCES
- 1.Abrams DB. Promise and peril of e-cigarettes: can disruptive technology make cigarettes obsolete? JAMA. 2014;311(2):135–136. doi: 10.1001/jama.2013.285347. [DOI] [PubMed] [Google Scholar]
- 2.Adkison SE, O'Connor RJ, Bansal-Travers M, et al. Electronic nicotine delivery systems: international tobacco control four-country survey. Am J Prev Med. 2013;44:207–215. doi: 10.1016/j.amepre.2012.10.018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Avdalovic MV, Murin S. Electronic cigarettes: no such thing as a free lunch...Or puff. Chest. 2012;141:1371–1372. doi: 10.1378/chest.12-0205. [DOI] [PubMed] [Google Scholar]
- 4.Ayers JW, Ribisl KM, Brownstein JS. Tracking the rise in popularity of electronic nicotine delivery systems (electronic cigarettes) using search query surveillance. Am J Prev Med. 2011;40:448–453. doi: 10.1016/j.amepre.2010.12.007. [DOI] [PubMed] [Google Scholar]
- 5.Bahl V, Lin S, Xu N, Davis B, Wang Y, Talbot P. Comparison of electronic cigarette refill fluid cytotoxicity using embryonic and adult models. Reprod Toxicol. 2012;34:529–537. doi: 10.1016/j.reprotox.2012.08.001. [DOI] [PubMed] [Google Scholar]
- 6.Barbeau AM, Burda J, Siegel M. Perceived efficacy of e-cigarettes versus nicotine replacement therapy among successful e-cigarette users: a qualitative approach. Addict Sci Clin Pract. 2013;8:5. doi: 10.1186/1940-0640-8-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Behar RZ, Davis B, Wang Y, Bahl V, Lin S, Talbot P. Identification of toxicants in cinnamon-flavored electronic cigarette refill fluids. Toxicol in Vitro. 2013 doi: 10.1016/j.tiv.2013.10.006. [DOI] [PubMed] [Google Scholar]
- 8.Benowitz NL. National Cancer Institute. Risks Associated with Smoking Cigarettes with Low Machine-Measured Yields of Tar and Nicotine. Smoking and Tobacco Control Monograph No. 13. Bethesda, MD: U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute, NIH Pub. No. 02-5074; 2001. Oct, Compensatory smoking of low-yield cigarettes. [Google Scholar]
- 9.Borland R. Electronic cigarettes as a method of tobacco control. BMJ. 2011;343:d6269. doi: 10.1136/bmj.d6269. [DOI] [PubMed] [Google Scholar]
- 10.Breland AB, Buchhalter AR, Evans SE, Eissenberg T. Evaluating acute effects of potential reduced-exposure products for smokers: clinical laboratory methodology. Nicotine Tob Res. 2002;4:131–140. doi: 10.1080/1462220021000032780. [DOI] [PubMed] [Google Scholar]
- 11.Buchhalter AR, Acosta MC, Evans SE, Breland AB, Eissenberg T. Tobacco abstinence symptom suppression: the role played by the smoking-related stimuli that are delivered by denicotinized cigarettes. Addiction. 2005;100:550–559. doi: 10.1111/j.1360-0443.2005.01030.x. [DOI] [PubMed] [Google Scholar]
- 12.Bullen C, McRobbie H, Thornley S, Glover M, Lin R, Laugesen M. Effect of an electronic nicotine delivery device (e cigarette) on desire to smoke and withdrawal, user preferences and nicotine delivery: randomized cross-over trial. Tob Control. 2010;19:98–103. doi: 10.1136/tc.2009.031567. [DOI] [PubMed] [Google Scholar]
- 13.Bullen C, Howe C, Laugesen M, et al. Electronic cigarettes for smoking cessation: a randomised controlled trial. Lancet. 2013a doi: 10.1016/S0140-6736(13)61842-5. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 14.Bullen C, Williman J, Howe C, Laugesen M, McRobbie H, Parag V, Walker N. Study protocol for a randomised controlled trial of electronic cigarettes versus nicotine patch for smoking cessation. BMC public health. 2013b;13(1):210. doi: 10.1186/1471-2458-13-210. (2013) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Byrnes HF, Miller BA, Aalborg AE, Plasencia AV, Keagy CD. Implementation fidelity in adolescent family-based prevention programs: relationship to family engagement. Health Educ Res. 2010;25:531–541. doi: 10.1093/her/cyq006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cahn Z, Siegel M. Electronic cigarettes as a harm reduction strategy for tobacco control: a step forward or a repeat of past mistakes? J Public Health Policy. 2011;32:16–31. doi: 10.1057/jphp.2010.41. [DOI] [PubMed] [Google Scholar]
- 17.Caldwell B, Sumner W, Crane J. A systematic review of nicotine by inhalation: is there a role for the inhaled route? Nicotine Tob Res. 2012;14:1127–1139. doi: 10.1093/ntr/nts009. [DOI] [PubMed] [Google Scholar]
- 18.Cameron JM, Howell DN, White JR, Andreyak DM, Layton ME, Roll JM. Variable and potentially fatal amounts of nicotine in e-cigarette nicotine solutions. Tob Control. 2013 doi: 10.1136/tobaccocontrol-2012-050604. [DOI] [PubMed] [Google Scholar]
- 19.Caponnetto P, Campagna D, Cibella F, et al. EffiCiency and Safety of an eLectronic cigAreTte (ECLAT) as tobacco cigarettes substitute: a prospective 12-month randomized control design study. PLoS One. 2013;8:e66317. doi: 10.1371/journal.pone.0066317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Caponnetto P, Auditore R, Russo C, Cappello GC, Polosa R. Impact of an electronic cigarette on smoking reduction and cessation in schizophrenic smokers: a prospective 12-month pilot study. Int J Environ Res Public Health. 2013;10:446–461. doi: 10.3390/ijerph10020446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Caponnetto P, Polosa R, Russo C, Leotta C, Campagna D. Successful smoking cessation with electronic cigarettes in smokers with a documented history of recurring relapses: a case series. J Med Case Rep. 2011;5:585. doi: 10.1186/1752-1947-5-585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Carnevali S, Nakamura Y, Mio T, et al. Cigarette smoke extract inhibits fibroblast-mediated collagen contraction. Am J Physiol. 1998;274:591–598. doi: 10.1152/ajplung.1998.274.4.L591. [DOI] [PubMed] [Google Scholar]
- 23.Cassidy S. [Accessed October 16, 2013];How Electronic Cigarettes Work. 2011 Available at: http:Science.howstuffworks.com.
- 24.Cervellin G, Luci M, Bellini C, Lippi G. Bad news about an old poison. A case of nicotine poisoning due to both ingestion and injection of the content of an electronic cigarette refill. Emergency Care Journal. 2013;9:53–54. [Google Scholar]
- 25.Centers for Disease Control and Prevention. [Accessed November 30, 2013];Case Definition: Nicotine [Centers for Disease Control and Prevention website] 2005 Mar 17; Available at: http://www.bt.cdc.gov/agent/nicotine/casedef.asp.
- 26.Centers for Disease Control and Prevention. Quitting Smoking Among Adults—United States, 2001–2010. Morbidity and Mortality Weekly Report. 2011;60:1513–1519. [PubMed] [Google Scholar]
- 27.Centers for Disease Control and Prevention. Current Cigarette Smoking Among Adults — United States, 2011. Morbidity and Mortality Weekly Report. 2012;61:889–894. [PubMed] [Google Scholar]
- 28.Centers for Disease Control and Prevention. Electronic cigarette use among middle and high school students - United States, 2011–2012. Morbidity and Mortality Weekly Report. 2013;62:729–730. [PMC free article] [PubMed] [Google Scholar]
- 29.Cheah NP, Chong NW, Tan J, Morsed FA, Yee SK. Electronic nicotine delivery systems: Regulatory and safety challenges: Singapore perspective. Tob Control. 2012 doi: 10.1136/tobaccocontrol-2012-050483. [DOI] [PubMed] [Google Scholar]
- 30.Chen I. FDA summary of adverse events on electronic cigarettes. Nicotine Tob Res. 2013;15:615–616. doi: 10.1093/ntr/nts145. [DOI] [PubMed] [Google Scholar]
- 31.Cho JH, Shin E, Moon SS. Electronic-cigarette smoking experience among adolescents. J. Adolesc Health. 2011;49:542–546. doi: 10.1016/j.jadohealth.2011.08.001. [DOI] [PubMed] [Google Scholar]
- 32.Choi K, Forster J. Characteristics associated with awareness, perceptions, and use of electronic nicotine delivery systems among young US Midwestern adults. Am J Public Health. 2013;103:556–561. doi: 10.2105/AJPH.2012.300947. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 33.Choi K, Forster JL. Beliefs and experimentation with electronic cigarettes: a prospective analysis among young adults. Am J Prev Med. 2014;46(2):175–178. doi: 10.1016/j.amepre.2013.10.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Chorti M, Poulianiti K, Jamurtas A, et al. Effects of active and passive electronic and tobacco cigarette smoking on lung function. Toxicol Lett. 2012;211:64. [Google Scholar]
- 35.Christensen LB, Veen TV, Bang J. Three cases of attempted suicide by ingestion of nicotine liquid used in e-cigarettes. Clin Toxicol. 2013;51:290. [Google Scholar]
- 36.Cobb NK, Abrams DB. E-cigarette or drug-delivery device? Regulating novel nicotine products. N Engl J Med. 2011;365:193–195. doi: 10.1056/NEJMp1105249. [DOI] [PubMed] [Google Scholar]
- 37.Cobb NK, Byron MJ, Abrams DB, Shields PG. Novel nicotine delivery systems and public health: the rise of the"e-cigarette". Am J Public Health. 2010;100(12):2340–2342. doi: 10.2105/AJPH.2010.199281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Corkery JM, Button J, Vento AE, Schifano F. Two UK suicides using nicotine extracted from tobacco employing instructions available on the internet. Forensic Sci Int. 2010;199:9–13. doi: 10.1016/j.forsciint.2010.02.004. [DOI] [PubMed] [Google Scholar]
- 39.Counts ME, Morton MJ, Laffoon SW, et al. Smoke composition and prediciting relationships for international commercial cigarettes smoked with three machine-smoking conditions. Regul Toxicol Pharmacol. 2005;41:185–227. doi: 10.1016/j.yrtph.2004.12.002. [DOI] [PubMed] [Google Scholar]
- 40.Davies P, Levy S, Pahari A, Martinez D. Acute nicotine poisoning associated with a traditional remedy for eczema. Arch Dis Child. 2001;85:500–502. doi: 10.1136/adc.85.6.500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Dawkins L, Corcoran O. Acute electronic cigarette use: Nicotine delivery and subjective effects in regular users. Psychopharmacology. 2013 doi: 10.1007/s00213-013-3249-8. [DOI] [PubMed] [Google Scholar]
- 42.Dawkins L, Turner J, Crowe E. Nicotine derived from the electronic cigarette improves time-based prospective memory in abstinent smokers. Psychopharmacology. 2013;227:377–384. doi: 10.1007/s00213-013-2983-2. [DOI] [PubMed] [Google Scholar]
- 43.Dawkins L, Turner J, Hasna S, Soar K. The electronic-cigarette: Effects on desire to smoke, withdrawal symptoms, and cognition. Addictive Behaviors. 2012;37:970–973. doi: 10.1016/j.addbeh.2012.03.004. [DOI] [PubMed] [Google Scholar]
- 44.Dawkins L, Turner J, Roberts A, Soar K. 'Vaping' profiles and preferences: an online survey of electronic cigarette users. Addiction. 2013;108:1115–1125. doi: 10.1111/add.12150. [DOI] [PubMed] [Google Scholar]
- 45.Donny EC, Houtsmuller E, Stitzer ML. Smoking in the absence of nicotine: behavioral, subjective and physiological effects over 11 days. Addiction. 2007;102:324–334. doi: 10.1111/j.1360-0443.2006.01670.x. [DOI] [PubMed] [Google Scholar]
- 46.Dockrell M, Morrison R, Bauld L, McNeill A. E-cigarettes: prevalence and attitudes in Great Britain. Nicotine Tob Res. 2013;15:1737–1744. doi: 10.1093/ntr/ntt057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47.Douptcheva N, Gmel G, Studer J, Deline S, Etter JF. Use of electronic cigarettes among young Swiss men. J Epidemiol Community Health. 2013;67:1075–1076. doi: 10.1136/jech-2013-203152. [DOI] [PubMed] [Google Scholar]
- 48.Dutra LM, Glantz SA. Electronic Cigarettes and Conventional Cigarette Use Among US Adolescents: A Cross-sectional Study. JAMA Pediatr. 2014 doi: 10.1001/jamapediatrics.2013.5488. [Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Eisenbud DK. [Accessed December 1, 2013];Toddler who ingested liquid nicotine passes away [The Jerusalem Post website] 2013 May 29; Available at: http://www.jpost.com/Breaking-News/Toddler-who-ingested-liquid-nicotine-passes-away-314683.
- 50.Etter JF. The electronic cigarette: An alternative to tobacco? Geneva, Switzerland: Jean-François Etter; 2012a. [Google Scholar]
- 51.Etter JF. Commentary on Wagener et al. (2012): electronic cigarettes - the Holy Grail of nicotine replacement? Addiction. 2012b;107:1550–1552. doi: 10.1111/j.1360-0443.2012.03909.x. [DOI] [PubMed] [Google Scholar]
- 52.Etter JF. Should electronic cigarettes be as freely available as tobacco? Yes. BMJ. 2013;346:f3845. doi: 10.1136/bmj.f3845. [DOI] [PubMed] [Google Scholar]
- 53.Etter JF, Bullen C. A longitudinal study of electronic cigarette users. Addictive Behaviors. 2014;39:491–494. doi: 10.1016/j.addbeh.2013.10.028. [DOI] [PubMed] [Google Scholar]
- 54.Etter JF, Bullen C, Flouris AD, Laugesen M, Eissenberg T. Electronic nicotine delivery systems: A research agenda. Tob control. 2012;20:243–248. doi: 10.1136/tc.2010.042168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Farsalinos KE, Romagna G, Tsiapras D, Kyrzopoulos S, Voudris V. Evaluation of electronic cigarette use (vaping) topography and estimation of liquid consumption: Implications for research protocol standards definition and for public health authorities’ regulation. Int J of Environ Res Public Health. 2013;10:2500–2514. doi: 10.3390/ijerph10062500. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Farsalinos KE, Spyrou A, Tsimopoulou K, Stefopoulos C, Romagna G, Voudris V. Nicotine absorption from electronic cigarette use: comparison between first and new-generation devices. Sci Rep. 2014;4:4133. doi: 10.1038/srep04133. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Fiore M. Treating tobacco use and dependence: 2008 update: Clinical practice guideline. DIANE Publishing; 2008. [Google Scholar]
- 58.Flouris AD, Oikonomou DN. Electronic cigarettes: miracle or menace? BMJ. 2010;340:c311. doi: 10.1136/bmj.c311. [DOI] [PubMed] [Google Scholar]
- 59.Flouris AD, Chorti MS, Poulianiti KP, et al. Acute impact of active and passive electronic cigarette smoking on serum cotinine and lung function. Inhal Toxicol. 2013;25:91–101. doi: 10.3109/08958378.2012.758197. [DOI] [PubMed] [Google Scholar]
- 60.Foulds J, Veldheer S. Commentary on Etter & Bullen (2011): could E-cigs become the ultimate nicotine maintenance device? Addiction. 2011;106:2029–2030. doi: 10.1111/j.1360-0443.2011.03532.x. [DOI] [PubMed] [Google Scholar]
- 61.Foulds J, Veldheer S, Berg A. Electronic cigarettes (e-cigs): views of aficionados and clinical/public health perspectives. Int J Clin Pract. 2011;65:1037–1042. doi: 10.1111/j.1742-1241.2011.02751.x. [DOI] [PubMed] [Google Scholar]
- 62.Goniewicz ML, Lingas EO, Hajek P. Patterns of electronic cigarette use and user beliefs about their safety and benefits: an Internet survey. Drug Alcohol Rev. 2013;32:133–140. doi: 10.1111/j.1465-3362.2012.00512.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Goniewicz ML, Knysak J, Gawron M, et al. Levels of selected carcinogens and toxicants in vapor from electronic cigarettes. Tob Control. 2013 doi: 10.1136/tobaccocontrol-2012-050859. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 64.Goniewicz ML, Kuma T, Gawron M, Knysak J, Kosmider LK. Nicotine levels in electronic cigarettes. Nicotine Tob Res. 2012;15:158–166. doi: 10.1093/ntr/nts103. [DOI] [PubMed] [Google Scholar]
- 65.Grana RA. Electronic cigarettes: a new nicotine gateway? J Adolesc Health. 2013;52:135–136. doi: 10.1016/j.jadohealth.2012.11.007. [DOI] [PubMed] [Google Scholar]
- 66.Grana RA, Glantz SA, Ling PM. Electronic nicotine delivery systems in the hands of Hollywood. Tob Control. 2011;20:425–426. doi: 10.1136/tc.2011.043778. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Hadwiger ME, Trehy ML, Ye W, Moore T, Allgire J, Westenberger B. Identification of amino-tadalafil and rimonabant in electronic cigarette products using high pressure liquid chromatography with diode array and tandem mass spectrometric detection. J Chromatogr. 2010;1217:7547–7555. doi: 10.1016/j.chroma.2010.10.018. [DOI] [PubMed] [Google Scholar]
- 68.Hajek P. Commentary on Wagener et al. (2012): E-cigarettes: a vulnerable promise. Addiction. 2012;107:1549. doi: 10.1111/j.1360-0443.2012.03899.x. [DOI] [PubMed] [Google Scholar]
- 69.Hastings G, de Andrade M, Moodie C. Tobacco harm reduction: the devil is in the deployment. BMJ. 2012;345:e8412. doi: 10.1136/bmj.e8412. [DOI] [PubMed] [Google Scholar]
- 70.Heishman SJ, Kleykamp BA, Singleton EG. Meta-analysis of the acute effects of nicotine and smoking on human performance. Psychopharmacology. 2010;210:453–469. doi: 10.1007/s00213-010-1848-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Henningfield JE, Zaatari GS. Electronic nicotine delivery systems: emerging science foundation for policy. Tob Control. 2010;19:89–90. doi: 10.1136/tc.2009.035279. [DOI] [PubMed] [Google Scholar]
- 72.Hua M, Yip H, Talbot P. Mining data on usage of electronic nicotine delivery systems (ENDS) from YouTube videos. Tob Control. 2013;22:723–728. doi: 10.1136/tobaccocontrol-2011-050226. [DOI] [PubMed] [Google Scholar]
- 73.Kamerow D. Big Tobacco lights up e-cigarettes. BMJ. 2013;346:f3418. doi: 10.1136/bmj.f3418. [DOI] [PubMed] [Google Scholar]
- 74.Kim HJ, Shin HS. Determination of tobacco-specific nitrosamines in replacement liquids of electronic cigarettes by liquid chromatography–tandemmass spectrometry. J Chromatogr. 2013;1291:48–55. doi: 10.1016/j.chroma.2013.03.035. [DOI] [PubMed] [Google Scholar]
- 75.King BA, Alam S, Promoff G, Arrazola R, Dube SR. Awareness and ever-use of electronic cigarettes among U.S. adults, 2010–2011. Nicotine Tob Res. 2013;15:1623–1627. doi: 10.1093/ntr/ntt013. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 76.Kralikova E, Novak J, West O, Kmetova A, Hajek P. Do e-Cigarettes Have the Potential to Compete With Conventional Cigarettes?: A Survey of Conventional Cigarette Smokers' Experiences With e-Cigarettes. Chest. 2013;144:1609–1614. doi: 10.1378/chest.12-2842. [DOI] [PubMed] [Google Scholar]
- 77.Kubica P, Wasik AK, Wasik A, Namiesnik J. “Dilute & Shoot” approach for rapid determination of trace amounts of nicotine in zero-level e-liquids by reversed phase liquid chromatography and hydrophilic interactions liquid chromatography coupled with tandem mass spectrometry-electrospray ionization. J Chromatogr. 2013;1289:13–18. doi: 10.1016/j.chroma.2013.02.078. [DOI] [PubMed] [Google Scholar]
- 78.Laugesen M. [Accessed November 7, 2013];Safety report on the ruyan e-cigarette cartridge and inhaled aerosol [Health New Zealand web site] 2008 Oct 30; (2008). Available at: http://www.healthnz.co.nz/RuyanCartridgeReport30-Oct-08.pdf.
- 79.Laugesen M, Thornley S, McRobbie H, Bullen C. The results of independent chemical and microbiological analysis. Christchurch, New Zealand: Health New Zealand; 2008. How safe is an e-cigarette? [Google Scholar]
- 80.Li J, Bullen C, Newcombe R, Walker N, Walton D. The use and acceptability of electronic cigarettes among New Zealand smokers. N Z Med J. 2013;126:48–57. [PubMed] [Google Scholar]
- 81.McAuley TR, Hopke PK, Babaian S. Comparison of the effects of e-cigarette vapor and cigarette smoke on indoor air quality. Inhal Toxicol. 2012;24:850–857. doi: 10.3109/08958378.2012.724728. [DOI] [PubMed] [Google Scholar]
- 82.McCauley L, Markin C, Hosmer D. An unexpected consequence of electronic cigarette use. Chest. 2012;141:110–113. doi: 10.1378/chest.11-1334. [DOI] [PubMed] [Google Scholar]
- 83.McMillen R, Maduka J, Winickoff J. Use of emerging tobacco products in the United States. J Environ Public Health. 2012;2012:989474. doi: 10.1155/2012/989474. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.McQueen A, Tower S, Sumner W. Interviews with"vapers": implications for future research with electronic cigarettes. Nicotine Tob Res. 2011;13:860–867. doi: 10.1093/ntr/ntr088. [DOI] [PubMed] [Google Scholar]
- 85.Noel JK, Rees VW, Connolly GN. Electronic cigarettes: a new 'tobacco' industry? Tob Control. 2011;20:81. doi: 10.1136/tc.2010.038562. [DOI] [PubMed] [Google Scholar]
- 86.Pearson JL, Richardson A, Niaura RS, Vallone DM, Abrams DB. E-Cigarette awareness use, harm perceptions in US adults. Am J Public Health. 2012;102:1758–1766. doi: 10.2105/AJPH.2011.300526. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Pellegrino RM, Tinghino B, Mangiaracina G, et al. Electronic cigarettes: An evaluation of exposure to chemicals and fine particulate matter (PM) Annali Di Igiene. 2012;24:279–288. [PubMed] [Google Scholar]
- 88.Pepper JK, Brewer NT. Electronic nicotine delivery system (electronic cigarette) awareness use, reactions and beliefs: a systematic review. Tob Control. 2013 doi: 10.1136/tobaccocontrol-2013-051122. [Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- 89.Pepper JK, Reiter PL, McRee AL, Cameron LD, Gilkey MB, Brewer NT. Adolescent males' awareness of and willingness to try electronic cigarettes. J Adolesc Health. 2013;52:144–150. doi: 10.1016/j.jadohealth.2012.09.014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 90.Phillips CV. Debunking the claim that abstinence is usually healthier for smokers than switching to a low-risk alternative, and other observations about anti-tobacco-harm-reduction arguments. Harm Reduct J. 2009;6:29. doi: 10.1186/1477-7517-6-29. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 91.Pokhrel P, Fagan P, Little MA, Kawamoto CT, Herzog TA. Smokers who try e-cigarettes to quit smoking: findings from a multiethnic study in Hawaii. Am J Public Health. 2013;103:e57–e62. doi: 10.2105/AJPH.2013.301453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 92.Polosa R, Caponnetto P, Morjaria JB, Papale G, Campagna D, Russo C. Effect of an electronic nicotine delivery device (e-Cigarette) on smoking reduction and cessation: a prospective 6-month pilot study. BMC Public Health. 2011;11:786. doi: 10.1186/1471-2458-11-786. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 93.Popova L, Ling PM. Alternative tobacco product use and smoking cessation: a national study. Am J Public Health. 2013;103:923–930. doi: 10.2105/AJPH.2012.301070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 94.Puustinen P, Olkkonen H, Kolonen S, Tuomisto J. Microcomputer-aided measurement of puff parameters during smoking of low- and medium-tar cigarettes. Scand J of Clin Lab Invest. 1987;47:655–660. doi: 10.1080/00365518709168925. [DOI] [PubMed] [Google Scholar]
- 95.Regan AK, Promoff G, Dube SR, Arrazola R. Electronic nicotine delivery systems: adult use and awareness of the 'e-cigarette' in the USA. Tob Control. 2013;22:19–23. doi: 10.1136/tobaccocontrol-2011-050044. [DOI] [PubMed] [Google Scholar]
- 96.Rhee MY, Na SH, Lee MM, Kim HY. Acute effects of cigarette smoking on arterial stiffness and blood pressure in male smokers with hypertension. Am J of Hypertens. 2007;6:637–641. doi: 10.1016/j.amjhyper.2006.12.017. [DOI] [PubMed] [Google Scholar]
- 97.Richardson A, Xiao H, Vallone DM. Primary and dual users of cigars and cigarettes: profiles, tobacco use patterns and relevance to policy. Nicotine Tob Res. 2012;14:927–932. doi: 10.1093/ntr/ntr306. [DOI] [PubMed] [Google Scholar]
- 98.Rohbemed N. E-cigarette sales surpass $1 billion as big tobacco moves in. Forbes. 2013 Sep 7; [Google Scholar]
- 99.Romanga G, Allifranchini E, Bocchietto E, Todeschi S, Esposito M, Farsalinos K. Cytotoxicity evaluation of electronic cigarette vapor extract on cultured mammalian fibroblasts (ClearStream-LIFE): comparison with tobacco cigarette smoke extract. Inhal Toxicol. 2013;25:354–361. doi: 10.3109/08958378.2013.793439. [DOI] [PubMed] [Google Scholar]
- 100.Rooke C, Amos A. News media representations of electronic cigarettes: an analysis of newspaper coverage in the UK and Scotland. Tob Control. 2013 doi: 10.1136/tobaccocontrol-2013-051043. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 101.Schneiderhan ME. A case report of patient-initiated e-cigarette use and resulting 5-months smoking cessation; Poster presented at the 2012 College of Psychiatric and Neurologic Pharmacists. [Google Scholar]
- 102.Schripp T, Markewitz D, Uhde E, Salthammer T. Does e-cigarette consumption cause passive vaping? Indoor Air. 2012 doi: 10.1111/j.1600-0668.2012.00792.x. [DOI] [PubMed] [Google Scholar]
- 103.Shihadeh A, Salman R, Balhas Z, Karaoghlanian N, Melvani R, Eissenberg T. Factors influencing the toxicant content of electronic cigarette vapor: Device characteristics and puff topography. Poster Presented at: (SRNT 19th Annual Meeting); March, 2013; Boston, Massachusetts. [Google Scholar]
- 104.Siegel MB, Tanwar KL, Wood KS. Electronic cigarettes as a smoking-cessation: tool results from an online survey. Am J Prev Med. 2011;40:472–475. doi: 10.1016/j.amepre.2010.12.006. [DOI] [PubMed] [Google Scholar]
- 105.Sutfin EL, McCoy TP, Morrell HE, Hoeppner BB, Wolfson M. Electronic cigarette use by college students. Drug Alcohol Depend. 2013;131:214–221. doi: 10.1016/j.drugalcdep.2013.05.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 106.Trehy ML, Ye W, Hadwiger ME, et al. Analysis of electronic cigarette cartridges, refill solutions, and smoke for nicotine and nicotine related impurities. J Liquid Chromatogr Related Technol. 2011;34:1442–1458. [Google Scholar]
- 107.Trtchounian A, Talbot P. Electronic nicotine delivery systems: is there a need for regulation? Tob Control. 2011;20:47–52. doi: 10.1136/tc.2010.037259. [DOI] [PubMed] [Google Scholar]
- 108.Trtchounian A, Williams M, Talbot P. Conventional and electronic cigarettes (e-cigarettes) have different smoking characteristics. Nicotine Tob Res. 2010;12:905–912. doi: 10.1093/ntr/ntq114. [DOI] [PubMed] [Google Scholar]
- 109.Trumbo CW, Harper R. Use and perception of electronic cigarettes among college students. J Am Coll Health. 61:149–155. doi: 10.1080/07448481.2013.776052. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 110.Uchiyama S, Inaba Y, Kunugita N. Determination of acrolein and other carbonyls in cigarette smoke using coupled silica cartridges impregnated with hydroquinone and 2, 4-dinitrophenylhydrazine. J Chromatogr. 2010;1217:4383–4388. doi: 10.1016/j.chroma.2010.04.056. [DOI] [PubMed] [Google Scholar]
- 111.Uryupin AB, Peregudov AS, Kochetkov KA, Bulatnikova LN, Kiselev SS, Nekrasov YS. Qualitative and quantitative compositions of fluids for electronic cigarettes. Pharm Chem J. 2013;46:44–49. [Google Scholar]
- 112.Vansickel AR, Cobb CO, Weaver MF, Eissenberg T. A clinical laboratory model for evaluating the acute effects of electronic cigarettes: Nicotine delivery profile and cardiovascular and subjective effects. Cancer Epidemiol Biomarkers. 2010;19:1945–1953. doi: 10.1158/1055-9965.EPI-10-0288. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 113.Vansickel AR, Eissenberg T. Electronic cigarettes: Effective nicotine delivery after acute administration. Nicotine Tob Res. 2013;15:267–270. doi: 10.1093/ntr/ntr316. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 114.Vansickel AR, Weaver MF, Eissenberg T. Clinical laboratory assessment of the abuse liability of an electronic cigarette. Addiction. 2012;107:1493–1500. doi: 10.1111/j.1360-0443.2012.03791.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 115.VaporBrands International. [Accessed April 21,. 2014];VaporBrands Interantional, Inc. to market hemp oil in electronic cigarettes. 2014 Feb 6; http://www.marketwired.com/press-release/vaporbrands-international-inc-to-market-hemp-oil-in-electronic-cigarettes-pinksheets-vapr-1876292.htm.
- 116. [Accessed November 30, 2013];Vaperzone Inc [Vaperzone’s website for e-cigarettes and e-liquids] Available at: http://www.vaporzone.com/
- 117.Vardavas CI, Anagnostopoulos N, Kougias M, Evangelopoulou V, Connolly GN, Behrakis PK. Short-term pulmonary effects of using an electronic cigarette: Impact on respiratory flow resistance, impedance, and exhaled nitric oxide. Chest. 2012;141:1400–1406. doi: 10.1378/chest.11-2443. [DOI] [PubMed] [Google Scholar]
- 118.Vickerman KA, Carpenter KM, Altman T, Nash CM, Zbikowski SM. Use of electronic cigarettes among state tobacco cessation quitline callers. Nicotine Tob Res. 2013;15:1787–1791. doi: 10.1093/ntr/ntt061. [DOI] [PubMed] [Google Scholar]
- 119.Wagener TL, Siegel M, Borrelli B. Electronic cigarettes: achieving a balanced perspective. Addiction. 2012;107:1545–1548. doi: 10.1111/j.1360-0443.2012.03826.x. [DOI] [PubMed] [Google Scholar]
- 120.Wagener TL, Siegel M, Borrelli B. Let's keep our 'eye on the ball': reducing tobacco-related harm. Addiction. 2012;107:1554–1555. doi: 10.1111/j.1360-0443.2012.04012.x. [DOI] [PubMed] [Google Scholar]
- 121.Wagener TL, Meier E, Hale JJ, et al. Pilot Investigation of Changes in Readiness and Confidence to Quit Smoking After E-cigarette Experimentation and 1 Week of Use. Nicotine Tob Res. 2013 doi: 10.1093/ntr/ntt138. [Epub ahead of print] [DOI] [PubMed] [Google Scholar]
- 122.Warren GW, Singh AK. Nicotine and lung cancer. J Carcinog. 2013;12:1. doi: 10.4103/1477-3163.106680. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 123.Westenberger BJ. Center for Drug Evaluation and Research, Division of Pharmaceutical Analysis. Rockville, MD: US Food and Drug Administration; 2009. US Food and Drug Administration evaluation of e-cigarettes. [Google Scholar]
- 124.Yamin CK, Bitton A, Bates DW. E-cigarettes: a rapidly growing Internet phenomenon. Ann. Intern Med. 2010;153:607–609. doi: 10.7326/0003-4819-153-9-201011020-00011. [DOI] [PubMed] [Google Scholar]