

Abstract
Objective
This study investigated whether a universal school-based life skills program—IPSY (Information + Psychosocial Competence = Protection)—against substance misuse exerted the same effectiveness for young adolescents (10.5–13 years) from distinct alcohol use trajectories characterized by late childhood risk factors (temperament, self-worth, social problems with peers).
Method
Analyses were based on a German sample of school students (N = 1,484). A longitudinal quasi-experimental design (intervention/control) with schoolwise assignment to the respective groups was used. Data were gathered via self-report questionnaire. Two-part growth mixture modeling was applied.
Results
Two prototypical trajectory classes of early alcohol use were found: a problematic group with a sharp increase in prevalence and quantity of consumed alcohol (19.7%) and a normative group with a moderate increase in both outcomes (80.3%). The problematic trajectory class was associated with several risk factors. IPSY decreased the likelihood of membership in the problematic group. Furthermore, IPSY buffered the increase in prevalence and quantity for the normative group, whereas it had no effects on these indicators for the problematic group. Concerning quantity of alcohol use, the effect size in terms of a difference in estimated means between intervention and control group at the last measurement point in the normative group was d = 0.33 (95% CI [0.21, 0.44]).
Conclusions
Study findings indicate the usefulness of IPSY for reducing alcohol use especially in normative developing adolescents. However, the minority of adolescents consistently pursuing a problematic developmental pathway of alcohol use seem to be in need of earlier, more tailored treatments.
Keywords: preventive intervention, life skills, early adolescent substance use, two-part growth mixture model, risk factors
Although adolescence reflects a life period with a general increase in prevalence and consumption rates of alcohol, there appear to exist subgroups following prototypical developmental trajectories of alcohol use (Jackson, Sher, & Schulenberg, 2005; Zucker, Fitzgerald, & Moses, 1995). These subgroups differ by age at onset of alcohol use and/or by rates of increase in alcohol consumption. Recent research indicates that distinct trajectory classes of drinking behavior are already distinguishable during early adolescence (van der Vorst, Vermulst, Meeus, Deković, & Engels, 2009). Accordingly, the majority of youth develop a largely adaptive drinking pattern. They abstain from or merely experiment with alcohol in early adolescence, increase the amount of consumption during mid- and late adolescence (including occasional incidents of binge drinking), and become responsible users in adulthood. A substantial but minor proportion of youth, in contrast, pursue a problematic pathway of adolescent alcohol use characterized by early consumption of significant quantities and a rapid acceleration of frequency and amount consumed in early adolescence (Chassin, Pitts, & Prost, 2002; Flory, Lynam, Milich, Leukefeld, & Clayton, 2004). Interestingly, from a prevention point of view, these young adolescents often possess early identifiable predispositions toward chronic problematic alcohol use such as disinhibition (e.g., risk taking, impulsivity; Colder, Campbell, Ruel, Richardson, & Flay, 2002). The negative consequences of following a problematic developmental pathway of alcohol use originating in early adolescence are manifold. For instance, untimely onset of serious alcohol use often leads to subsequent adolescent and adult problem drinking (Clark, 2004) and increases the likelihood of other future adaptation problems, such as academic failure and delinquent behavior (Ellickson, Tucker, & Klein, 2003). However, adolescents on a normative pathway of alcohol use are not a group entirely without significance for the health care system because their heightened alcohol consumption during mid-to late adolescence often leads to serious short-term consequences, including accidents, vandalism, and unprotected sex (Weichold, Bühler, & Silbereisen, 2008).
Given the fact that the age of onset of substance use plays a crucial role in predicting subsequent alcohol use, it is not surprising that prevention efforts in early adolescence typically aim at delaying the initiation of alcohol use and reducing the normative increase in the amount of alcohol consumption. To achieve this aim, universal prevention programs (Mrazek & Haggerty, 1994) are implemented before the onset of alcohol use (average age of onset is 12–13 years for German adolescents, which is comparable, for instance, to that of the United States; cf. Currie et al., 2004) and are delivered to the general population (regardless of risk status) in relevant social contexts (e.g., school). These early interventions are derived from theories of developmental psychopathology focusing on risk and protective factors that promote or deter the onset and problematic progression of substance use in adolescence (e.g., Hawkins, Catalano, & Miller, 1992). According to the social influence hypothesis, one of the most prominent risk factors for substance use in adolescence is the influence of substance-using peers (e.g., Oetting & Beauvais, 1986). Prevention research has revealed that universal school-based prevention programs are more effective when they are based on the social influence approach, that is, when they focus on substance-related social norms and interactively train how to avoid social high-risk situations or how to resist peer pressure to use substances (Cuijpers, 2002; Donald-son et al., 1996). The promotion of protective factors has also turned out to be an important component of effective programs. Correspondingly, interventions that fostered rather substance-unspecific, comprehensive individual and social skills were more effective than other approaches, such as educational programs (Tobler, Roona, Marshall, Streke, & Stackpole, 2000). Such generic “life skills” (World Health Organization [WHO], 1997) as empathy, assertiveness, communication skills, thoughtful decision making, and problem solving can be seen as fundamental capabilities needed to deal adequately with age-typical challenges and developmental tasks (e.g., establishing amicable or intimate relationships with peers). Adolescents with poor personal and social skills are more likely to fail in these tasks and subsequently are at a heightened risk to use substances as an alternative way to achieve age-typical aims or to cope with failures (Weichold et al., 2008).
The two components that proved to be effective in preventing problematic substance use in adolescence (social influence approach, generic skills training) are combined in life skills programs (Botvin & Griffin, 2004; Cuijpers, 2002; WHO, 1997). This approach claims that changes in knowledge, attitudes, and values (cf. Ajzen & Fishbein, 1980); an enhancement in psychosocial competence; and enduring reinforcement of new behavioral alternatives all lead to better adaptation and healthy development in adolescents. School-based life skills programs have shown to be effective in preventing problematic substance use in adolescence, as revealed by well-designed evaluation studies based on U.S. samples (e.g., Botvin, 2000; Skara & Sussman, 2003). However, their effect sizes with regard to substance use outcomes have been rather small (Tobler et al., 2000). This might be due to moderator variables such as characteristics of the study participants (e.g., prior consumption experiences, vulnerability). For instance, it is often speculated that a universal prevention program might not work, by design, for subgroups characterized by various risk factors pointing to a heightened risk for developing early alcohol misuse (e.g., Spoth, Greenberg, & Turrisi, 2008; Springer et al., 2004). According to Kumpfer, Williams, and Baxley (1997), selective prevention programs aiming more intensively at target-group-specific risk and protective factors may be more appropriate.
Empirical findings regarding the differential effectiveness of universal prevention programs among subgroups of youth exhibiting different risk profiles before the onset of the intervention are rare and inconclusive. Some studies have shown that universal prevention programs can indeed delay the onset and regular use of substances, even among adolescents at high risk for developing problematic alcohol use patterns, with “high risk” being defined as, for instance, user status at pretest (Chou et al., 1998; Johnson et al., 1990). In addition, Griffin, Botvin, Nichols, and Doyle (2003) demonstrated that a school-based life skills program was effective even among students who were exposed to substance-using peers and did not perform very well in school. Contrary to that, Vitaro and Dobkin (1996) found that a slightly modified life skills training had no effects on adolescent substance use in a sample including participants showing problem behaviors at pre-test.
It is likely that some of the discrepant findings occurred because the studies differed in their definition of risk. The effects of risk factors such as substance-using peers might be easier to attenuate (e.g., via enhancement of life skills) compared with those of early, more general dispositional risk factors such as difficult temperament (Weichold, 2007). However, prevention research within this field has been informed only marginally by the literature about early psychologically predisposing factors for adolescent substance misuse (e.g., Swaim, 1991; Zucker, Donovan, Masten, Mattson, & Moss, 2008) and has largely relied on assessments of adolescent risk factors. This is a crucial limitation of the existing literature, considering that effective primary prevention programs should start in late childhood, before first experiences with substance use occur. Risk factors that become especially prominent during the adolescent years (such as peer substance use) might be of very limited use for creating subgroups with distinctive risk profiles during examinations of the differential effectiveness of universal prevention approaches. Additionally, in some of the above-mentioned evaluation studies, risk factors were not tested as predictors of subsequent substance use. When they were tested, knowledge about variability of drinking behavior during adolescence in terms of distinct trajectories was typically neglected. As already mentioned above, recent research has indicated the existence of at least two distinctive alcohol use pathways during adolescence (e.g., Li, Duncan, & Hops, 2001; van der Vorst et al., 2009), and there is some evidence that problematic alcohol use trajectories could be associated with predisposing factors assessed in late childhood or early adolescence (Chassin et al., 2002; Colder et al., 2002). Thus, a promising strategy to put the differential effectiveness of universal prevention programs to a test might be to create subgroups based on drinking patterns associated with levels of late childhood risk factors.
To the best of our knowledge, no study to date has accounted for heterogeneity in early alcohol use pathways (including trajectory specific risk factors) when evaluating the effectiveness of a universal school-based prevention approach. It is questionable whether a universal prevention program designed for the general population works for young adolescents on problematic pathways of alcohol use that are associated with early risk factors (Masterman & Kelly, 2003). For instance, a difficult temperament could contribute (in transaction with deficient socialization and via disruptive interactions with the environment) to an increasingly chronic problematic substance use pattern. Such a mechanism is described in work on the etiology of early-age-onset substance use disorders (e.g., Clark, 2004; Tarter et al., 1999) and also in theoretical models that pinpoint pathways of risk to chronic alcoholism in adulthood (Zucker et al., 1995). Although our study spans only 2.5 years at the beginning of adolescence (age 10.5–13), a disposition or liability toward substance use and steeply increasing alcohol use during this time window could reflect the beginning of a developmental trajectory toward chronic problematic drinking behavior. Universal school-based prevention approaches might be insufficient for the minority pursuing such a developmental pathway because these programs typically neglect predispositions toward problematic substance use and are largely restricted to resistance toward negative social influences during adolescence. For the problematic subgroup, earlier and rather selective interventions might be more appropriate (Tarter et al., 1999). To examine this research question, we adopted a stepwise approach (cf. van Lier, Muthén, van der Sar, & Crijnen, 2004) that involved the following sequence of five study goals.
First, we examined the overall effect of a universal school-based life skills program—IPSY (Information + Psychosocial Competence = Protection)—on alcohol use in early adolescence (indicated by both use vs. nonuse and quantity-of-use outcomes). Because the aim of life skills programs is to deter adolescents from using alcohol in early developmental stages and to encourage responsible use later on (Weichold, 2007), we expected to find a positive overall effect of IPSY on both the age-graded increase in the likelihood to use alcohol and the increase in the quantity of drinking among users.
Second, we examined heterogeneity in patterns of early alcohol use by means of identifying distinct alcohol use trajectories during early adolescence. On the basis of recent research, we anticipated at least a slowly increasing normative and a problematic trajectory of drinking behavior (e.g., Flory et al., 2004; van der Vorst et al., 2009). We expected any problematic pathways to be characterized by heightened baseline rates and/or a steep increase in likelihood to drink and amount of alcohol consumed.
Third, we investigated associations of the distinct alcohol use pathways with predisposing factors in late childhood (measured at age 10.5) to identify specific characteristics (besides levels of alcohol use) of the respective trajectory members.1 For instance, it was demonstrated in many studies that temperamental aspects in late childhood or early adolescence are related to substance use throughout adolescence. Accordingly, an active and approaching temperament served as a risk factor for heightened levels of consumption (Wills, DuHamel, & Vaccaro, 1995; Windle, 2000). A disinhibited temperament might contribute to dysregulated socioemotional behavior that underlies different (but cognate) patterns of behavior throughout the life span, including sensation seeking and conduct problems in childhood, early substance use in adolescence, and severe substance abuse in adulthood (Tarter et al., 1999). Furthermore, social problems with peers (social isolation, peer rejection, stigmata) and low self-worth may lead to a maladaptive developmental trajectory that manifests in substance misuse (Hops, Davis, & Lewin, 1999; Woodward & Fergusson, 1999; Zimmerman, Copeland, Shope, & Dielman, 1997). Lastly, being a male adolescent may increase the risk for early substance use relative to girls (Hops et al., 1999).
Fourth, we tested whether the life skills intervention IPSY was related to the probability of class membership (B. Muthén et al., 2002), that is, whether program participants, in general, were less likely to follow problematic pathways of drinking behavior. Despite the lack of evaluation studies that accounted for heterogeneity in alcohol use pathways during adolescence, findings from Botvin, Griffin, Diaz, and Ifill-Williams (2001) are consistent with the assumption that life skills programs might decrease the risk of initiating engagement in patterns of serious drinking behavior. The authors found that their life skills training reduced adolescent binge drinking up to 2 years after implementation.
Fifth, we examined the differential impact of IPSY on alcohol use progression within classes of students pursuing specific developmental pathways of alcohol use. We hypothesized that the school-based IPSY would exert no positive long-term effects (study span: 2.5 years) on the increase in alcohol use among those students classified as members of problematic developmental pathways of alcohol use. Advanced alcohol use experiences and more positive expectancies toward the effects of alcohol (Windle et al., 2008) imply that these adolescents are probably more resistant against a universal prevention. In addition, the predispositions in late childhood might constitute a common liability underlying substance misuse in adolescence and ultimately lead to even more severe and resistant alcohol use pathways during adolescence (e.g., Tarter et al., 1999). Such risk mechanisms are not accounted for by universal prevention programs such as IPSY. A normative moderate increase in alcohol use during adolescence, on the contrary, should be associated with rather regular developmental processes, such as the determination of identity or adaptation to peer substance use (Windle et al., 2008). Students belonging to such a pathway are the main target group of IPSY, as universal prevention efforts mostly focus on risk factors prevalent during adolescence (e.g., peer pressure). Accordingly, IPSY should be most effective in reducing the increase in alcohol consumption for those students pursuing a rather normative drinking pathway relatively free of predisposing factors in late childhood.
Method
Sample
The original sample consisted of 1,693 students in the fifth grade of schools located in the federal state of Thuringia, Germany. These students participated in at least the pretest. For the analyses of the current study, 33 students were excluded due to having constant missing data for alcohol use during Grades 5–7. Because the software package used for the analyses (Mplus 5.1; L. K. Muthén & Muthén, 2007) cannot model missing data in covariates within conditional models, the original sample was further reduced to 1,484. Via selection analyses, applying Bonferroni corrected tests, we compared the working sample with the original sample. These tests revealed no significant differences between both samples regarding covariates, outcome variables, and various sociodemographic variables. Thus, no selection effects were found. Likewise, in the unconditional two-part growth curve model, equality tests demonstrated that growth factor means and variances of the working sample did not differ significantly from those of excluded students with missing data on covariates.
From the working sample, 58% were in the intervention group and 42% in the control group. The intervention group consisted of 49% boys and 51% girls (control group: 44% boys and 56% girls; entire sample: 47% boys and 53% girls). The working sample had a mean age of 10.45 years (SD = 0.63) at pretest, and 61% of participants attended the college-bound track, whereas the rest attended the lower school track (i.e., “Regelschule”). Moreover, 73% of the students reported a good to very good financial background. In addition, we checked whether the intervention and control groups were comparable regarding outcome variables, covariates, and a variety of sociodemographic variables at pretest. These analyses revealed only one significant difference concerning outcomes and covariates; namely, the control group showed a significantly higher mean for the temperament scale Activity Level–General at pretest than the intervention group, t(1,482) = −2.71, p < .01, but the difference was very small in terms of effect size (d = 0.14). There were no significant baseline differences with respect to the other covariates (gender, approach–withdrawal, social problems, and self-worth) or alcohol use versus nonuse (intervention group: 43% user; control group: 44% user) and quantity of alcohol consumption among users (intervention group: M = 2.20 g/10, SD = 1.57; control group: M = 2.18 g/10, SD = 1.56). Regarding sociodemographic variables, students in the intervention group were more likely to come from rural rather than urban areas, χ2(1, N = 1,464) = 18.19, p < .001, d* = 0.26 (cf. Hasselblad & Hedges, 1995), and reported a better financial background compared with the control group, t(1,450) = 2.58, p = .01, but the latter group difference was very small (d = 0.13) as well. On various remaining sociodemographic variables, both groups were statistically equivalent at pretest (age, school type, number of siblings, persons per household, living situation, and marital and employment status of parents).
Intervention
IPSY (Weichold, 2007) is a universal school-based life skills program that aims to delay the onset and to reduce the regular consumption and misuse of alcohol and tobacco in early adolescence. The program is theoretically based on the model for life skills education (WHO, 1997), developmental psychological models, and empirical findings on risk and protective factors for substance misuse. IPSY is a comprehensive program that combines the training of general, intra- and interpersonal life skills (e.g., self awareness, stress- and problem-coping strategies, assertiveness, communication skills) with the acquisition of substance-specific skills (e.g., how to resist the offer of substances from peers). In addition, knowledge concerning alcohol and tobacco use (i.e., prevalence rates, short-term effects, advertising strategies) is transferred in an age-appropriate manner. The intervention uses interactive methods (i.e., role plays, group discussion) and is implemented by teachers after participating in a one-day facilitator workshop, based on a comprehensive training manual. Teachers are trained to be aware of the positive characteristics of each student and to work with reinforcement strategies in order to promote the acquisition of skills.
Because IPSY is a primary prevention program, it is designed to be implemented before adolescents start to experiment with the use of legal substances. The average age of substance use initiation in Germany is 12 years (Currie et al., 2004); therefore, the basic program was developed for fifth graders (aged 10–11 years), followed by booster sessions in Grades 6 and 7. More specifically, the intervention consists of 15 basic lessons (10 × 90 min and 5 × 45 min) in fifth grade and seven booster lessons (4 × 90 min and 3 × 45 min) in sixth and seventh grade each, to repeat contents and practice learned skills from basic sessions in an age-adequate manner (e.g., role plays). The focus of these booster sessions lies on the training of new acquired skills within age-typical critical situations (e.g., resisting peer pressure). These situations turned from low relevance for substance consumption in sixth grade (e.g., resist peer pressure to view movies not adequate for one’s age) to higher substance use relevance in seventh grade (e.g., resist peer pressure to get drunk at home).
Results of a process evaluation, based on a proprietary questionnaire (structured self-report) and referring to the basic program in Grade 5, revealed that in 80% of the lessons given, the teachers were able to cover the material as provided in the IPSY manual, and in about 80% of all implemented lessons the aim of the IPSY unit was achieved, indicating good fidelity (for more information, see Weichold, 2007). Already published findings of outcome evaluations demonstrate positive short-term effects on substance use outcomes, generic life skills, knowledge about substances, and school bonding (e.g., Weichold, Giannotta, Silbereisen, Ciairano, & Wenzel, 2006).
Design
This evaluation study used a quasi-experimental prospective intervention–control group design with four measurement points and schoolwise assignment to the respective groups. Between pretest (fall of 2003) and posttest (spring of 2004) there was an interval of approximately half a year. Two follow-up measurements were gathered within an interval of approximately 1 year each (spring of 2005 and spring of 2006).
As the study was to be implemented in schools, it first had to be approved by the Ministry of Culture and Education of the Thuringia, and schools were free to be involved. A letter was sent from the ministry to all schools (N = 403) offering them the opportunity to participate in a meeting about an intervention program against adolescent substance misuse. The letter did not contain any details about the program, and schools (at the principal’s discretion) could send one or two teacher representatives. As schools receive similar invitations on a regular basis, or may have been involved already in such activities, and as there are no negative consequences for schools that do not accept, the actual response rate is usually rather small (40 schools accepted the invitation). In this case, reasons given for participation varied and included such factors as a general interest in intervention programs, specific interest in substance misuse at schools, and the enhancement of school prestige. During the information meeting, teachers received a general outline of the IPSY program and of the evaluation study. They were then asked to decide (together with their principals) whether to implement the program in their schools and whether to take part in the evaluation study. Finally, all 40 schools (much more than expected) were willing to participate. As we could handle only a smaller number in the program, 23 schools were selected at random to be intervention schools for our evaluation study. It was not possible to use the remaining schools (N = 17) as control or intent-to-treat group because they expected to see the program implemented as soon as possible and were not prepared to wait until implementation (5 years in all). For this reason, control schools were recruited at random from the remaining 363 schools. One school refused participation in the study, and one did not comply with requirements for ensuring anonymity. Finally, 21 schools formed the control group. As expected, one third among them had taken part in interventions in the past as well. Interestingly enough, the share was the same among the intervention schools. Thus, intervention and control schools probably do not differ in their general interest in school-based interventions.
The IPSY program was implemented as part of the school curriculum; however, teachers were trained not to force students to take an active part in the IPSY sessions. Parents were informed in the run-up to the project via informative meetings and via letter. They were then asked to give active consent to their child’s study participation (evaluation part of the study). Only two students did not take part in the data collection, indicating that there was no active selection of the study participants. The students completed an anonymous questionnaire (length: 60 min) at each measurement point in the classroom administered by project staff or trained teachers. Questionnaires were identified and linked across waves of data collection by means of a self-generated code consisting of the day and month of birth, the last letter of the student’s first name, and the first three letters of the mother’s first name. At the first measurement point, project coworkers instructed the students on how to fill out the questionnaire and answered further questions. Study participants received small incentives (e.g., a key strap).
Measures
Alcohol use
Students reported at each assessment how many glasses of beer, wine, hard liquor, and mixed drinks they had consumed on a typical drinking occasion. On the basis of these data, the amount of ethanol in grams consumed by the students per typical drinking occasion was computed for each substance making use of German standard formulas. According to Simon, Tauscher, and Pfeiffer (1999), one standard glass of beer (0.5 L) contains 20 g ethanol, one standard glass of wine (0.225 L) 21.6 g ethanol, one standard glass of hard liquor (0.02 L) 6 g ethanol, and one standard glass of a mixed drink (0.29 L) 8.7 g ethanol (information is based on typical serving sizes in Germany). A total score was formed by summing up the amounts across the four types of alcoholic beverages. Prior to use in the analyses, total scores were divided by a constant (10) to facilitate computational processes in the statistical software package Mplus. Because of the young age of our sample, we reviewed literature pertaining to the ability of young adolescents to differentiate between alcoholic beverages. Liu (2003) demonstrated that elementary school children are already able to recognize different kinds of alcoholic beverages in survey questions. Additionally, the validity of self-reports of alcohol use has been supported in numerous studies with adolescents (e.g., Oetting & Beauvais, 1990). Further inspections of our own data showed that the amounts of ethanol consumed by the adolescents of the IPSY study were quite comparable to consumption patterns in nationally representative studies with approximately same-aged German adolescents (e.g., Bundeszentrale für gesund-heitliche Aufklärung [BZgA], 2007).
Intervention status and gender
Intervention status and gender were treated as dummy-coded variables. Students participating in the IPSY program were coded 0, and students belonging to the control group were coded 1. Male students were coded 0, and female students were coded 1.
Temperament
Temperament was assessed at pretest with two scales of the Revised Dimensions of Temperament Survey (Windle & Lerner, 1986), namely Activity Level–General (six items; e.g., “I can’t stay seated for a long time”) and Approach–Withdrawal (five items; e.g., “If there is something new, I have a closer look at it”).2 Response options for the items of both temperament scales consisted of a 4-point scale ranging from 0 (not true) to 3 (true). The average response to the items was computed for both scales (as for the following scales of the study). High mean scores in both scales reflect a high activity level and a strong tendency to approach (in novel situations). Means, standard deviations, and reliabilities (Cronbach’s alpha) of these and the following scales are presented in Table 1.
Table 1.
Descriptive Statistics for Continuous Covariates and Alcohol Use Outcomes (Quantity of Use Among Users)
| Variable | M | SD | Skewness | Kurtosis | α |
|---|---|---|---|---|---|
| Activity level (Time1) | 1.40 | 0.71 | 0.14 | −0.48 | .71 |
| Approach (Time 1) | 1.63 | 0.67 | −0.18 | −0.17 | .66 |
| Social problems (Time 1) | 0.35 | 0.34 | 1.28 | 1.52 | .69 |
| Self-worth (Time 1) | 4.62 | 0.90 | −0.71 | 0.23 | .77 |
| Ethanol in grams/10 | |||||
| Time 1 | 2.19 | 1.56 | 0.99 | 0.20 | |
| Time 2 | 2.50 | 2.31 | 1.07 | 0.67 | |
| Time 3 | 3.29 | 2.82 | 1.11 | 0.92 | |
| Time 4 | 4.94 | 3.79 | 0.88 | −0.02 |
Note. Observed means for ethanol in grams/10 were computed for those using alcohol at the current time point and having no missing data, resulting in the following sample sizes: Time 1, n = 602; Time 2, n = 555; Time 3, n = 592; Time 4, n = 659. Observed means for covariates are based on the full sample (N = 1,484).
Problems with peers
Problems with peers were measured at pretest by the scale Social Problems, taken from the German version (Döpfner, Berner, & Lehmkuhl, 1994) of the Child Behavior Checklist, Youth Self-Report Form (Achenbach, 1991). The scale comprised eight items (e.g., “I don’t get along with others at my age”). Response options consisted of a 3-point scale ranging from 0 (not true) to 2 (true). High mean scores indicate many problems with peers.
Self-worth
Self-worth was assessed at pretest with the scale Self-Concept of General Self-Worth, which is part of a German instrument measuring self-concept in a variety of domains (Frankfurt Self-Concept Scales; Deusinger, 1986). The scale comprised 10 items (e.g., “I am a nobody”), and response options consisted of a 6-point scale ranging from 1 (strongly agree) to 6 (strongly disagree). High mean scores therefore reflect a positive self-worth.
Statistical Analyses
In keeping with our sequence of study goals, we first applied a latent growth model (LGM) to determine overall effects of IPSY. In this method a single growth curve is estimated for the population, and individual differences in developmental trajectories are captured by estimates of growth factor variation (i.e., variation in the intercept and the slope). We then used a latent growth mixture model (LGMM; e.g., B. Muthén et al., 2002) to identify distinct trajectories of alcohol consumption among study participants. The LGMM approach, in contrast to LGM, assumes that the sample is a composite of several unobserved (“latent”) classes within the population, each following a prototypical growth curve. LGMM is well suited for the analysis of prevention trials. Because it allows for cross-group differences in the shape of developmental trajectories, it enables the user to investigate for whom a treatment is effective by allowing for different treatment effects in different latent trajectory classes.
To accommodate the large number of students who were not drinking at a given time point (i.e., had a value of zero regarding the alcohol use outcome), we extended the LGM and LGMM to a two-part LGM–LGMM (Brown, Catalano, Fleming, Haggerty, & Abbott, 2005; Witkiewitz, van der Maas, Hufford, & Marlatt, 2007). Two-part modeling allowed us to decompose the original distribution of the alcohol use outcome (i.e., amount of ethanol consumed on a typical drinking occasion) into a use versus nonuse part and a quantity-of-use part, each modeled by separate, but correlated, growth functions (Olsen & Schafer, 2001). The first part, the u part or prevalence part, consists of a logistic growth model that models the probability of nonzero (use) versus zero outcomes (nonuse). The second part, the y part or quantity part, consists of a continuous growth model that uses values of the nonzero outcomes. Alcohol nonuse at a given time point in the u part was treated as missing data in the y part, following common assumptions of data missing at random (Little & Rubin, 2002). The u and y parts were estimated simultaneously within the LGM and LGMM frameworks, but in LGMM one additional categorical latent class variable C was used to capture unobserved heterogeneity in both parts of the model (see Figure 1).
Figure 1.
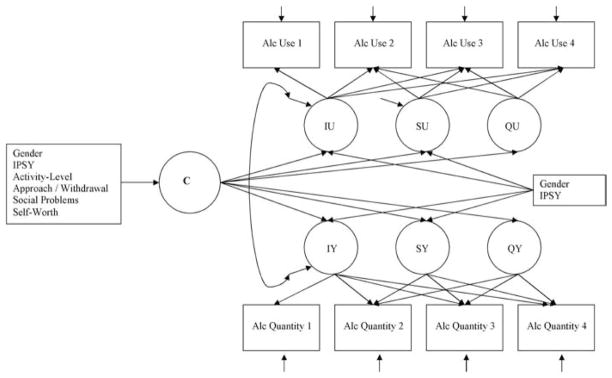
Path diagram describing the postulated effects of covariates on class membership and growth factors within a two-part latent growth mixture model of alcohol (Alc) use. Top portion of the diagram depicts the prevalence part (u part); the bottom portion depicts the quantity part of the model (y part). C is a latent class variable that influences the growth factors (intercept, linear slope, quadratic slope) of both model parts and is regressed on late childhood risk factors, gender, and intervention. Growth factors (intercept, linear slope) of both model parts are regressed on gender and intervention; however, the intercept of the prevalence part (IU) and the intercept of the quantity part (IY) are not regressed on intervention because of pretest equivalence (cf. Footnote 4). Because we found no effects of intervention and gender on the quadratic slope of the prevalence part (QU) and the quadratic slope of the quantity part (QY), these paths are fixed at zero. Linear and quadratic slope factor loadings for both model parts are fixed at 0, .20, .60, and 1 (linear trend) and 0, .04, .36, and 1 (quadratic trend), taking the uneven spacing between time points into account and representing the average linear and quadratic growth of alcohol use between ages 10.5 and 13. SU = linear slope prevalence part; SY = linear slope quantity part.
Two-part LGMs and two-part LGMMs were estimated with the software package Mplus 5.1 (L. K. Muthén & Muthén, 2007). It allows for missing data in all parts of LGM–LGMM except observed background variables. Missingness on outcomes was handled with full information maximum likelihood estimation under the assumption of missing at random. Furthermore, the software provided maximum likelihood parameter estimates with robust standard errors, employing numerical integration algorithms. Due to the use of the robust maximum likelihood estimator (MLR), adjusted chi-square difference tests were used throughout data analyses (Satorra, 2000). Because of the clustering of students within schools, all analyses were conducted with the Mplus command “Complex/Cluster,” which provides adjusted standard errors and chi-square values (cf. Stapleton, 2006).3
Using two-part growth mixture modeling requires an extensive, stepwise modeling process (B. Muthén, 2001). We first identified the growth functions (intercept only, linear and quadratic) of the unconditional u and y parts separately within a conventional LGM approach. We then investigated the influence of intervention and gender on growth factors in the entire two-part LGM. Note that the intercepts of both LGM model parts (both intercepts were centered at pretest) were not predicted by intervention status because we expected (and found) no differences between intervention and control group at Time 1 regarding outcome variables (cf. tests of pretest equivalence in Sample). This strategy is commonly used when pretest equivalence of outcomes is given (e.g., B. Muthén et al., 2002; van Lier et al., 2004).4 Afterward, an unconditional two-part LGMM was applied to identify distinct trajectory groups of alcohol use, followed by a conditional two-part LGMM to improve model specification and to determine the final two-part growth mixture solution (B. Muthén, 2004). Individuals were grouped according to their posterior probabilities of group membership, taking class uncertainty into account and leading to unbiased model estimates.
Model selection in LGMM requires determination of the number of trajectory classes that best describes the data. In this study, we theoretically assumed four trajectory classes as a maximum number of distinct classes (cf. Wiesner, Weichold, & Silbereisen, 2007). The 1-, 2-, 3-, and 4-class models were compared via the Bayesian information criterion (BIC; Schwarz, 1978) as a basic guide. Generally, the model with the smallest BIC is chosen. As further criteria, the adjusted Lo–Mendell–Rubin likelihood ratio test (Lo, Mendell, & Rubin, 2001) and the bootstrapped likelihood ratio test (McLachlan & Peel, 2000) were applied to test the fit of k-1 classes against k classes. In both tests a significant p value indicates that the null hypothesis of k-1 classes should be rejected in favor of at least k classes.5 Class prevalence (greater than 5% of the sample), class interpretability, and model stability were considered as additional criteria to correctly specify the number of distinct trajectory classes in the sample. Moreover, we used the entropy measure (Ramaswamy, Desarbo, Reibstein, & Robinson, 1993) and the average posterior group membership probabilities to evaluate classification quality. For both indices, scores close to one indicate an accurate classification of individuals into latent trajectory classes.
Results
Descriptive Statistics
Means, standard deviations, and values of skewness and kurtosis for the continuous covariates and alcohol use outcomes (quantity of use among users) appear in Table 1, and the proportions for the categorical alcohol use outcomes (use vs. nonuse) appear in Table 2. Intercorrelations among covariates ranged between .33 ( p < .001; activity level and approach) and −.36 ( p < .001; self-worth and social problems). In general, the likelihood to use alcohol (prevalence) and the amount of ethanol consumed among users (quantity of use) increased from age 10.5 to age 13, which is supported by significant slope growth factor means in the two-part growth curve analyses described below.
Table 2.
Proportions for the Categorical Alcohol Use Outcomes (Use vs. Nonuse)
| Alcohol use | Students (%) |
|---|---|
| Time 1 | 43 |
| Time 2 | 48 |
| Time 3 | 57 |
| Time 4 | 74 |
Note. Observed proportions of alcohol users were computed for those having no missing data at the current time point, resulting in the following sample sizes: Time 1, n = 1,398; Time 2, n = 1,163; Time 3, n = 1,038; Time 4, n = 894.
Two-Part LGM of Alcohol Use
Unconditional model
We first examined the growth function for each unconditional part of the two-part LGM separately (i.e., covariates were excluded). For the prevalence part (u part), it was demonstrated that a quadratic growth factor model improved model fit compared with a linear growth function, χdiff2 (1, N = 1,484) = 4.61, p < .05. The quantity part (y part) was also modeled best by a quadratic growth function, χ2(1, N = 1,125) = 0.77, p > .20, comparative fit index = 1.00, root-mean-square error of approximation = .00. Fit statistics of the linear model were inferior compared with the quadratic model, χ2(5, N = 1,125) = 23.19, p < .001, comparative fit index = .76, root-mean-square error of approximation = .06. In the entire two-part LGM, we found significant variation in intercept growth factors for both model parts (u part: variance = 3.50, SE = 0.36, p < .001; y part: variance = 1.27, SE = 0.18, p < .001). These intercept growth factors showed a significant positive covariation (r = .92, p < .001). In addition, the variance of the linear slope factors was significant for both model parts (u part: variance = 4.49, SE = 1.14, p < .001; y part: variance = 3.94, SE = 0.96, p < .001). However, we found no significant heterogeneity in quadratic growth factors for both model parts. Thus, these variances as well as the rest of nonsignificant covariances were fixed to zero to facilitate model convergence. The estimated latent growth factor means of the u part for intercept, linear slope, and quadratic slope were 0.00 (SE = 0.00; the mean of the intercept in the u part was set to zero for model identification purposes; cf. L. K. Muthén & Muthén, 2007), 0.42 (SE = 0.57, ns), and 1.98 (SE = 0.58, p < .001), respectively. The means of the intercept, linear, and quadratic factors for the y part were 1.55 (SE = 0.09, p < .001), 0.89 (SE = 0.51, p < .10), and 2.29 (SE = 0.56, p < .001), respectively.
Conditional model
In the conditional two-part LGM, growth factors of the y and u parts were regressed on intervention and gender. These analyses were performed to address our first study goal. Results revealed a positive intervention effect on linear growth factors of both model parts. Being a member of the control group was associated with a significantly greater rate of linear increase in the likelihood of alcohol use (B = 1.35, SE = 0.27, p < .001, 95% CI [0.83, 1.87]) and in the quantity of alcohol use (B = 0.91, SE = 0.36, p < .05, 95% CI [0.21, 1.61]) between Grade 5 and 7. The corresponding effect size (Cohen’s d) in terms of a difference in estimated means between intervention and control group at the last measurement point in the y part was 0.23 (95% CI [0.13, 0.34]), indicating a small effect (J. Cohen, 1988). Furthermore, boys had a significantly higher baseline of alcohol quantity consumed on a typical occasion than girls (B = −0.65, SE = 0.13, p < .001), but boys and girls did not differ with regard to the likelihood of using alcohol at pretest (B = −0.21, SE = 0.16, ns). Additionally, girls relative to boys showed a stronger linear increase in the likelihood of using alcohol between Grades 5 and 7 (B = 0.64, SE = 0.26, p < .05). There was no gender effect, however, on the linear increase within the quantity part of the model (B = 0.26, SE = 0.24, ns). In preliminary analyses of the conditional model, we found no effects of intervention and gender on quadratic growth factors. These paths were subsequently fixed to zero in the models reported above. The estimated growth curves for both model parts separated by intervention status (adjusted by gender) are depicted in Figure 2.6
Figure 2.

Estimated growth curves of alcohol use for the final conditional two-part latent growth model separated by intervention status: (A) prevalence part and (B) quantity part. Only the quantity part is adjusted by gender. See Footnote 6.
Two-Part LGMM of Alcohol Use
Unconditional model
Next, we addressed our second study goal and conducted a two-part LGMM without covariates to test for the existence of distinct developmental trajectories of alcohol use in young adolescents. In all models the group trajectories were identified by class-varying growth factor means and class-invariant but freely estimated growth factor (co)variances and residual variances. The variances of the quadratic growth factors were constrained to zero in both model parts (u and y parts), as in the previous LGM analyses. However, as we tried to extract more than one trajectory class of alcohol use, the variance of the linear slope factor in the y part became negative but insignificant. Thus, it was constrained to zero in two-part LGMMs to facilitate model convergence (cf. Witkiewitz et al., 2007).
The model fit statistics spoke for at least two distinct trajectory classes (see Table 3). The adjusted Lo–Mendell–Rubin likelihood ratio test was not significant for three groups, favoring a solution including two groups. The BIC was still decreasing even when a four-group model was presumed. Finally, an insignificant bootstrapped likelihood ratio test in the four-group model suggested a three-class model. Contradictory fit statistics in LGMM are not a rarity. In such situations, theoretical considerations, practical implications, reasonable group sizes, and the stability of the class solutions should play a crucial role besides the examination of fit statistics (e.g., Hipp & Bauer, 2006; Nagin, 2005). With regard to the latter criterion, we found that the three- and four-class solutions were unstable, which can be interpreted as a warning sign for trying to extract too many groups from the data. Log likelihood and entropy values are presented in Table 3. Average posterior probabilities (.91 and .88) indicated a sufficient classification quality of the two-class model (Nagin, 2005). After considering the various decision criteria discussed above, we favored the two-class trajectory model as the most parsimonious description of the data. It was further tested against the competing three-class model in the following analysis of conditional trajectory models to minimize the possibility of distorted trajectory class solutions because of an underspecified model (B. Muthén, 2004).
Table 3.
Fit Statistics and Classification Quality of Two-Part Latent Growth Mixture Models Assuming up to Four Trajectory Classes of Alcohol Use (Unconditional and Conditional Models)
| Class | Unconditional model
|
Conditional model
|
||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| BIC | LL | E | BLRT | Adj. LMR LRT | BIC | LL | E | BLRT | Adj. LMR LRT | |
| 1 | 16687 | −8289 | 16652 | −8249 | ||||||
| 2 | 16563 | −8205 | .65 | p < .001 | p < .01 | 16575 | −8145 | .69 | p < .001 | p < .05 |
| 3 | 16507 | −8151 | .62 | p < .001 | p = .27 | 16589 | −8083 | .75 | p = .12 | p = .95 |
| 4 | 16473 | −8109 | .65 | p = .27 | p = .76 | |||||
Note. BIC = Bayesian information criterion; LL = log likelihood; E = entropy; BLRT = bootstrapped likelihood ratio test; Adj. LMR LRT = adjusted Lo–Mendell–Rubin likelihood ratio test.
Conditional model
As a next step, covariates were entered into the two-part LGMM presuming two or three classes, respectively. This allowed us to address the third, fourth, and fifth study goals simultaneously. By using a multinomial logistic regression, class membership (i.e., the latent class variable C) was regressed on temperament variables, social problems, self-worth, gender, and prevention. In addition, growth factors were regressed on prevention and gender, as in the two-part LGM (see Figure 1). Variances for the quadratic slopes in both u and y parts, as well as the residual variance of the linear slope of the y part, were set to zero. All other significant residual (co)variances were freely estimated but held invariant across classes. These settings were needed to avoid model nonconvergence.
Fit indices of the conditional models (see Table 3) were not contradictory anymore and, in sum, supported a two-class solution as the best fitting model. Entropy values improved compared with the unconditional LGMM’s suggesting a better classification quality when covariates were included in the model. More specifically, as in the unconditional model, the adjusted Lo–Mendell–Rubin likelihood ratio test was not significant when testing for three trajectories. However, unlike in the unconditional model, the BIC did not decrease when modeling three classes. Also, the bootstrapped likelihood ratio test was not significant anymore when testing a three-group model. Hence, we finally decided to assume two trajectory classes of alcohol use in early adolescence (see Figure 3 and Table 4).7 The classification quality of this model, based on average posterior probabilities (.92 and .86), was remarkable (Nagin, 2005).
Figure 3.

Estimated growth curves of alcohol use for the final conditional two-part latent growth mixture model assuming two trajectory classes of alcohol use: (A) prevalence part and (B) quantity part. Growth curves are separated by intervention status. Only the quantity part is adjusted by gender. See Footnote 6.
Table 4.
Growth Factor Means of Two-Part Latent Growth Mixture Model Assuming Two Trajectory Classes of Alcohol Use
| Growth factor | Normative group (n = 1,191)
|
Problematic group (n = 293)
|
||
|---|---|---|---|---|
| M | SE | M | SE | |
| IU | 0.00 | 0.00 | 0.65† | 0.35 |
| SU | −0.33 | 0.55 | 4.15† | 1.55 |
| QU | 2.22** | 0.56 | 1.04 | 1.60 |
| IY | 1.60** | 0.11 | 2.32** | 0.28 |
| SY | 0.70 | 0.57 | 0.48 | 2.00 |
| QY | 0.65 | 0.55 | 7.62** | 1.93 |
Note. IU = intercept prevalence part; SU = linear slope prevalence part; QU = quadratic slope prevalence part; IY = intercept quantity part; SY = linear slope quantity part; QY = quadratic slope quantity part.
p < .10.
p < .01.
p < .001.
The first trajectory class, labeled as a “normative class,” consisted of 80.3% of the students (n = 1,191) and was characterized by a moderate increase in the likelihood to use alcohol in the u part and a flat increase in quantity consumed in the y part (restricting both linear and quadratic growth factor means of the y part to zero worsened the model fit, indicating substantial growth despite insignificant linear and quadratic trends). The second class, labeled as a “problematic class,” consisted of 19.7% of the sample (n = 293). The growth curves in the prevalence and quantity parts of this group were characterized by a sharp increase, but this increase began later (and progressed even more markedly) in the quantity part. The problematic class, compared with the normative class, had a higher intercept growth factor mean in the y part, χdiff2(1, N = 1,484) = 4.64, p < .05, and a marginally higher intercept growth factor mean in the u part, χdiff2(1, N = 1,484) = 3.45, p < .10.
As we inspected the parameter estimates of the final conditional two-class two-part LGMM, we found various effects of covariates on trajectory class membership (C) and on class-specific growth factors (intercept and linear slope of the u and y parts). Pertaining to the third study goal, it was found that, of the late childhood risk factors, social problems with peers (B = 0.65, SE = 0.30, p < .05, OR = 1.92), a high activity level (B = 0.33, SE = 0.17, p < .05, OR = 1.39), and a strong tendency to approach (B = 0.43, SE = 0.18, p < .05, OR = 1.54) significantly increased the likelihood of pursuing a problematic pathway of alcohol use. By contrast, gender (B = 0.14, SE = 0.23, ns, OR = 1.15) and self-worth (B = −0.11, SE = 0.12, ns, OR = 0.90) did not influence the likelihood of belonging to the problematic class. With regard to the fourth study goal, binomial logistic regression also revealed that the odds of belonging to the problematic class significantly increased for the control group (B = 0.48, SE = 0.24, p < .05, OR = 1.62, 95% CI [1.01, 2.59]), indicating that participants of the IPSY program were underrepresented among members of the problematic user group. Hence, the intervention, in general, decreased the likelihood of following a problematic developmental trajectory of drinking behavior.
When examining the possible differential effectiveness of IPSY among the two alcohol use trajectories (our fifth and most important study goal), the within-class effects of the intervention status on slope growth factors are of primary interest (B. Muthén et al., 2002). We found that within the normative class, the control group, compared with the IPSY group, had a significantly stronger linear increase in the prevalence part as well as in the quantity part (see Figure 3 and Table 5).8 Thus, IPSY successfully buffered the increase in alcohol use on a typical occasion (in terms of both likelihood and quantity of use) for those students who followed a normative alcohol use trajectory in early adolescence. The corresponding effect size (Cohen’s d) in terms of a difference in estimated means between intervention and control group at the last measurement point in the y part was 0.33 (95% CI [0.21, 0.44]), indicating a small effect (J. Cohen, 1988). Within the problematic class, however, IPSY did not have significant effects on the linear increase in both outcomes. Moreover, with respect to the effects of gender on growth factors within classes, it was found that boys relative to girls started on significantly higher initial levels regarding the quantity part in both trajectory classes. However, girls in the normative class (compared with boys in the normative class) displayed a significantly stronger linear increase in the prevalence part, and girls in the problematic alcohol use class (compared with boys in the problematic class) had a significantly stronger linear increase in the quantity part. The latter pattern of effects on growth factors speaks for a gender-related catch-up effect in both trajectory classes, but pertaining to different outcomes (prevalence vs. quantity) depending on group membership.
Table 5.
Growth Factor Regression Coefficients of Two-Part Latent Growth Mixture Model Assuming Two Trajectory Classes of Alcohol Use
| Regression | Normative group (n = 1,191)
|
Problematic group (n = 293)
|
||||
|---|---|---|---|---|---|---|
| B | SE | 95% CI | B | SE | 95% CI | |
| IU on gender | −0.33 | 0.21 | [−0.73, 0.07] | 0.27 | 0.41 | [−0.53, 1.06] |
| SU on IPSY | 1.17** | 0.27 | [0.64, 1.71] | 0.07 | 1.39 | [−2.66, 2.80] |
| SU on gender | 0.74* | 0.29 | [0.18, 1.30] | −0.06 | 1.42 | [−2.85, 2.73] |
| IY on gender | −0.45** | 0.13 | [−0.71, −0.20] | −1.34* | 0.50 | [−2.31, −0.36] |
| SY on IPSY | 0.75* | 0.25 | [0.27, 1.24] | −0.16 | 0.55 | [−1.23, 0.92] |
| SY on gender | −0.09 | 0.23 | [−0.54, 0.35] | 1.41* | 0.55 | [0.34, 2.49] |
Note. CI = confidence interval; IU = intercept prevalence-part; SU = linear slope prevalence-part; IY = intercept quantity part; SY = linear slope quantity part.
p < .01.
p < .001.
Discussion
The impact of the universal school-based life skills program IPSY on alcohol use in early adolescence (age 10.5–13 years) was examined in a large German sample. By using a two-part LGM, it was shown that IPSY had a positive overall effect. The program decreased the likelihood to drink (prevalence) and reduced the quantity of drinking per occasion during early adolescence. Moreover, considerable interindividual variability in developmental courses of drinking behavior was detected in the data. By means of a two-part LGMM, two trajectory classes of alcohol use were identified in early adolescence, namely, a problematic class with a sharp increase in prevalence and quantity and a normative class characterized by a relatively moderate increase in both outcomes. Additionally, the normative class had a lower initial level with respect to quantity of alcohol use. Trajectory class membership was significantly predicted by risk factors in late childhood and intervention status. Pursuing a problematic pathway of alcohol use during early adolescence was associated with an approaching, active temperament and social problems with peers. Participation in the IPSY program, in general, decreased the likelihood of membership in the problematic trajectory class. However, further analyses showed that IPSY was not effective in reducing the acceleration of alcohol consumption for those students on the problematic developmental pathway but significantly buffered the increase in alcohol consumption for the majority of adolescents following a normative alcohol use trajectory. All analyses were controlled for gender and clustering of data within schools.
Although the main goal of our study was to determine the differential impact of IPSY on distinct developmental pathways of alcohol use, we first tested whether the intervention exerted positive effects within a conventional single-class two-part LGM of alcohol use (B. Muthén et al., 2002). Results of this analysis provided evidence for the general efficacy of the universal life skills program IPSY in reducing alcohol consumption during early adolescence. This finding is in line with prior evaluation studies of life skills programs (e.g., Skara & Sussman, 2003). Interestingly, the overall effectiveness applied to both outcomes of interest. The IPSY program decreased the likelihood of alcohol use throughout early adolescence (age 10.5–13) and thus encouraged abstinence. Also, the program buffered the normative increase in ethanol dosages consumed on a typical occasion. The positive effect of the intervention on ethanol intake among users can be interpreted as fostering a responsible use of alcohol, which is considered an explicit goal of modern primary prevention approaches (Franzkowiak, 2002). Having some experiences with alcohol use is normative even in early adolescence, and the acquisition of risk-related expertise is often considered a crucial developmental task (Paglia & Room, 1999). The effect size of IPSY (d = 0.23) was at the top of the range of what can typically be achieved by universal life skills programs (Tobler et al., 2000).
On the basis of recent research, however, we anticipated prototypical groups of young adolescents with different levels and/or different growth rates of alcohol use for whom the intervention might work differently. Hence, the second goal of this study was to explore unobserved heterogeneity in drinking pathways during early adolescence via LGMM methods. To the best of our knowledge, this was the first study addressing the above-mentioned research question by means of a two-part LGMM approach. Our findings indicated that the heterogeneity in drinking pathways found during mid- and late adolescence in many prior studies (e.g., Wiesner et al., 2007) might also apply to the developmental period of early adolescence. This assumption is corroborated by empirical evidence derived from other studies. For instance, a recent study (van der Vorst et al., 2009) pointed to the existence of four distinct alcohol use classes in early adolescence (abstainers, light drinkers, increasers, heavy drinkers). These trajectory classes might resemble the more parsimonious description of early drinking behavior in our study (abstainers + light drinkers = normative group; increasers + heavy drinkers = problematic group). Moreover, LGMM analyses of Li et al. (2001) revealed two latent classes of alcohol use trajectories during adolescence, and both trajectory groups already had clearly distinguishable levels of alcohol use in early adolescence (cf. Flory et al., 2004). Other studies identified more than two distinct alcohol use trajectories, but their focus was the time window of mid- to late adolescence (e.g., Colder et al., 2002; Wiesner et al., 2007). Although it is likely to find additional decreasing or stable consumption trajectories among samples of older adolescents, this is less likely during early adolescence, as the majority of youth just initiated their substance use. In the same vein, Weber, Graham, Hansen, Flay, and Johnson (1989) suggested that there exist, in principle, a moderate increasing normative and a rapidly increasing problematic pathway of alcohol use onset during adolescence, with the latter trajectory being associated with problem behavior proneness. Finally, approximately 20% of the study sample being classified on a problematic alcohol use pathway during early adolescence seems a plausible proportion when compared with evidence from other growth mixture studies (Flory et al., 2004; van der Vorst et al., 2009) and epidemiological studies (BZgA, 2007; Johnston, O’Malley, Bachman, & Schulenberg, 2006). However, more research with diverse samples (e.g., from different countries and of varying socioeconomic background) is required before firm conclusions about the number and shape of distinct alcohol use trajectories during early adolescence can be drawn.
The third central finding of the present study pertained to risk factors in late childhood and associations with the identified problematic (i.e., escalating) pathway of alcohol use. Consistent with the alcohol research literature, a dysregulated approaching, active temperament served as predictor of this early problematic trajectory class of drinking behavior (Clark, 2004; Tarter et al., 1999). Interestingly, having social problems in late childhood also was an important risk factor. This might be due to several reasons. On the one hand, social problems with peers might be symptomatic of a generalized pattern of psychosocial and developmental disadvantage (e.g., low socioeconomic status, less intellectual abilities, more conduct problems), which places adolescents at a higher risk for problematic substance use (Woodward & Fergusson, 1999). On the other hand, creating relationships with peers becomes increasingly important in early adolescence. In the case of strained relationships with peers, the use of alcohol may provide social support in a social niche consisting of other deviant peers (Simons, Whitbeck, Conger, & Melby, 1991). Likewise, the consumption of alcohol might help to cope with experiences of peer rejection and loneliness (Laurent, Catanzaro, & Callan, 1997). Conversely, self-worth in late childhood was not related to trajectory class membership. A possible explanation could be that general self-worth might be too global to predict concrete drinking behavior. For instance, Rosenberg, Schooler, Schoenbach, and Rosenberg (1995) found that global self-esteem was more relevant to psychological well-being compared with behavior. In addition, Wild, Flisher, Bhana, and Lombard (2004) demonstrated that family and school self-esteem were more strongly related to risk behaviors than global self-esteem. Notably, gender was not related to trajectory class membership. This finding contradicts some previous studies (e.g., Chassin et al., 2002), where being male was associated with heavy drinking trajectories from adolescence to early adulthood. However, none of these studies investigated alcohol use from a very early age onward (age 10.5) and exclusively in early adolescence, where drinking might also be related to onset of puberty (Windle et al., 2008). Puberty begins a few years earlier for girls than for boys. Thus, during early adolescence, girls might catch up with heightened initial alcohol use levels of boys, which are, in turn, possibly caused by the heightened proneness to problem behavior in late childhood for boys (P. Cohen et al., 1993). As a result, there might be no gender difference in the likelihood to follow a problematic drinking pathway. Albeit the latter hypotheses are highly speculative, a catch-up effect in the above-mentioned direction was indeed consistent with our data.
Concerning the fourth study goal, IPSY participants were underrepresented among members of the problematic pathway of alcohol use. Thus, overall, the intervention seemed to reduce the likelihood to engage in severe drinking patterns in early adolescence, albeit the effect size (odds ratio) was rather small. Nevertheless, this finding points to the general usefulness of life skills programs in reducing serious levels of alcohol use (cf. Botvin et al., 2001).
The fifth and main objective of this study was an examination of the differential effectiveness of IPSY against the background of distinct developmental pathways of alcohol use during early adolescence. In general, the usefulness and necessity of accounting for more person-centered analysis strategies in evaluation research (e.g., growth mixture approaches) was demonstrated. If we had solely relied on the initial two-part LGM, it would not have been revealed that the universal life skills program IPSY indeed works for the majority of young adolescents, but not for a small subgroup consistently pursuing a problematic, probably more resistant developmental pathway of alcohol use. More specifically, we found that IPSY buffered the increase in both the likelihood to use alcohol and the amount of alcohol consumed on a typical occasion in those 80% of the students who belonged to the normative trajectory class. Hence, this finding enriched the conclusions derived from the single-class two-part LGM and revealed that the school-based life skills program exerted positive effects, in particular, on the normative increase in alcohol consumption during early adolescence. This is consistent with numerous studies demonstrating the effectiveness of universal life skills programs against substance misuse for adolescents on average risk for substance misuse (e.g., Botvin, 2000). It was shown that the effect size of IPSY in the normative group was even higher compared with the overall analysis (d = 0.33). Buffering the age-graded increase in alcohol use of this rather unproblematic group is not without significance for the health care system due to various negative consequences even of substance use within the normative range. In contrast, the analyses of the intervention effects within the problematic trajectory class (20% of the sample) revealed no impact of IPSY on the increase in both the likelihood to use alcohol and the amount of alcohol consumed on a typical occasion. This finding supports the common assumption in evaluation research that a universal prevention program might not meet the needs of a minority of young adolescents who possess an early liability to a problematic substance use pathway and, additionally, use alcohol from early age onward at a serious level (Masterman & Kelly, 2003). Such concerns have been frequently raised in the literature, and our study is one of the first to provide empirical support for this contention.
Although this is speculative, some components of universal interventions might be inappropriate for high-risk youth. IPSY, for instance, uses an interactive teaching approach that enables adolescents to actively exercise the new skills acquired within the classroom (i.e., role plays, small group activities). Our findings suggest that this approach might be ineffective for adolescents who are on a problematic developmental pathway of alcohol use associated with a difficult temperament and problems with peers in late childhood. In addition, a program component that has been originally designed to alter substance-related norms in an alcohol-naive population, like that provided in IPSY, might not work for a subpopulation already showing advanced alcohol use. Possibly, this subgroup is in need of an earlier, more intensive and tailored treatment compared with IPSY (e.g., interventions involving the family; cf. Spoth et al., 2008; Tarter et al., 1999). The specific reasons behind the ineffectiveness of IPSY for the problematic subgroup, however, cannot be clearly identified in the present study and merit further research. We also want to remind the reader that IPSY reduced the risk of membership in the problematic-escalating trajectory class at least to some extent (cf. study Goal 4). This finding, interpreted in the context of results related to study Goal 5, points to a partial effectiveness of universal life skills programs in reducing problematic alcohol use in early adolescence. At this point we can only speculate why IPSY lowered the likelihood of pursuing a problematic drinking pathway. Perhaps the program’s focus on rather normative risk factors (e.g., negative peer influences) and protective factors (e.g., self-management skills and social skills) might have exerted some limited beneficial impact on incidents of serious alcohol use over the course of the study period (e.g., binge drinking; cf. Botvin et al., 2001). This, in turn, might have resulted in the positive overall effect on trajectory class membership. However, for those who consistently followed a problematic developmental pathway of alcohol use, which was associated with late childhood risk factors (active and approaching temperament, social problems with peers), the intervention seemed to have no effect on the progression of alcohol use.
Findings should be interpreted in light of several study limitations. First, given the quasi-experimental design, the risk of any selection bias has to be considered when interpreting study findings, even though, with regard to the sampling procedure chosen, this seems unlikely. In line with this assumption, several analyses showed that students of the intervention and control groups were comparable concerning all outcome variables and most covariates and sociodemographic variables at pretest. Second, in mixture modeling, mixtures can be extracted even when no true distinct classes exist. More specifically, instead of having been drawn from mixture of normal subpopulations, data might also have come from a single nonnormal population distribution (Bauer & Curran, 2003; but see B. Muthén, 2003). The latter scenario, though, seems rather unlikely in our study. Both trajectory classes fit well to theories dealing with substance use in early adolescence, are predicted by covariates in meaningful ways, and are supported by similar findings from other studies. Moreover, the two-part approach has considerably reduced the distributional complexity of the alcohol use outcomes, possibly leading to more trustworthy classes based on true mixtures. Nevertheless, cross-validation of our findings is important. Third, the measures used in this study were based on adolescent self-reports. It is possible that reliance on a single informant has introduced some bias into the study findings. Fourth, the follow-up was limited to 2 years after the posttest. Additional follow-up data are needed to determine the long-term durability of the positive program effects on alcohol use and should include measures of other dimensions of drinking behavior more germane to older adolescents (e.g., binge drinking). Furthermore, a broader range of risk factors should be assessed to examine possible causes of differential program effectiveness more thoroughly.
Nevertheless, this study made a significant contribution to the knowledge concerning heterogeneity in drinking behavior in early adolescence. Study results highlighted the importance of accounting for early developmental pathways of alcohol use, including related late childhood risk factors when evaluating existing interventions and designing future universal or selective treatments. The usefulness of methods that integrate variable- and person-centered analyses (e.g., two-part growth mixture models) was thereby demonstrated.
Footnotes
This and the following steps were handled simultaneously in the final conditional two-part growth mixture model (see Statistical Analyses and Results). However, we elected to present the study goals in a stepwise fashion for didactic purposes.
The original scale comprised six items. We excluded Item 2, “My first reaction is to reject something new or unfamiliar to me,” to substantially improve Cronbach’s alpha.
We also tried to specify two-part LGMs and LGMMs as multilevel models including prevention versus control as a school-level predictor. However, these models turned out to be too complex because of intractable numeric integration. Perhaps multilevel two-part growth (mixture) modeling would represent an appealing approach when hardware and software are ready for such complex specifications in the future. Apart from that, clustering of data within schools was probably not an important issue in our study. Intraclass correlations across time points were low for both alcohol use outcomes (.01–.05), and design effects fell mostly below the threshold of concern (range: 1.35–2.33; design effects below 2.00 are considered as negligible; cf. B. Muthén & Satorra, 1995).
In addition, we tentatively estimated paths from the intervention variable to growth factor intercepts of both model parts. In both the two-part LGM and the two-part LGMM (assuming two trajectory classes), none of these regression coefficients was statistically significant. Thus, we fixed paths from the intervention variable to intercepts to zero.
The bootstrapped likelihood ratio test in Mplus cannot be used in conjunction with the command “TYPE = Complex.” The test was therefore used without any adjustments for clustering of data within schools and should be interpreted cautiously, in a more explorative manner.
Observed and estimated categorical data proportions for prevalence of alcohol use were not available when predicting growth factors. We therefore derived this information from models that did not control for the effect of gender on growth factors to get an approximation.
See Footnote 6.
See Footnote 6.
Parts of this article were presented at the 27th Annual Meeting of the Society for Prevention Research, May, 26–29, 2009, in Washington, D.C.
Contributor Information
Michael Spaeth, Friedrich-Schiller University of Jena.
Karina Weichold, Friedrich-Schiller University of Jena.
Rainer K. Silbereisen, Friedrich-Schiller University of Jena
Margit Wiesner, University of Houston.
References
- Achenbach TM. Manual for the Youth Self-Report and 1991 Profile. Burlington, VT: University of Vermont, Department of Psychiatry; 1991. [Google Scholar]
- Ajzen I, Fishbein M. Understanding attitudes and predicting social behavior. Englewood Cliffs, NJ: Prentice Hall; 1980. [Google Scholar]
- Bauer DJ, Curran PJ. Distributional assumptions of growth mixture models: Implications of overextraction of latent trajectory classes. Psychological Methods. 2003;8:338–363. doi: 10.1037/1082-989X.8.3.338. [DOI] [PubMed] [Google Scholar]
- Botvin GJ. Preventing drug abuse in schools: Social and competence enhancement approaches targeting individual-level etiologic factors. Addictive Behaviors. 2000;25:887–897. doi: 10.1016/s0306-4603(00)00119-2. [DOI] [PubMed] [Google Scholar]
- Botvin GJ, Griffin KW. Life skills training: Empirical findings and future directions. Journal of Primary Prevention. 2004;25:211–232. [Google Scholar]
- Botvin GJ, Griffin KW, Diaz T, Ifill-Williams M. Preventing binge drinking during early adolescence: One- and two-year follow-up of a school-based preventive intervention. Psychology of Addictive Behaviors. 2001;15:360–365. doi: 10.1037//0893-164x.15.4.360. [DOI] [PubMed] [Google Scholar]
- Brown EC, Catalano RF, Fleming CB, Haggerty KP, Abbott RD. Adolescent substance use outcomes in the Raising Healthy Children project: A two-part latent growth curve analysis. Journal of Consulting and Clinical Psychology. 2005;73:699–710. doi: 10.1037/0022-006X.73.4.699. [DOI] [PubMed] [Google Scholar]
- Bundeszentrale für gesundheitliche Aufklärung. Alkoholkonsum der Jugendlichen in Deutschland 2004–2007—Kurzbericht. Köln, Germany: Author; 2007. Alcohol consumption among adolescents in Germany 2004–2007—Abridged report. [Google Scholar]
- Chassin L, Pitts SC, Prost J. Binge drinking trajectories from adolescence to emerging adulthood in a high-risk sample: Predictors and substance abuse outcomes. Journal of Consulting and Clinical Psychology. 2002;70:67–78. [PubMed] [Google Scholar]
- Chou CP, Montgomery S, Pentz MA, Rohrbach LA, Johnson CA, Flay BR, MacKinnon DP. Effects of a community-based prevention program on decreasing drug use in high-risk adolescents. American Journal of Public Health. 1998;88:944–948. doi: 10.2105/ajph.88.6.944. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clark DB. The natural history of adolescent alcohol use disorders. Addiction. 2004;99:5–22. doi: 10.1111/j.1360-0443.2004.00851.x. [DOI] [PubMed] [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. 2. Hillsdale, NJ: Erlbaum; 1988. [Google Scholar]
- Cohen P, Cohen J, Kasen S, Velez CM, Hartmark C, Johnson J, Streuning EL. An epidemiological study of disorders in late childhood and adolescence: I. Age- and gender-specific prevalence. Journal of Child Psychology and Psychiatry. 1993;34:851–867. doi: 10.1111/j.1469-7610.1993.tb01094.x. [DOI] [PubMed] [Google Scholar]
- Colder CR, Campbell RT, Ruel E, Richardson JL, Flay BR. A finite mixture model of growth trajectories of adolescent alcohol use: Predictors and consequences. Journal of Consulting and Clinical Psychology. 2002;70:976–985. doi: 10.1037//0022-006x.70.4.976. [DOI] [PubMed] [Google Scholar]
- Cuijpers P. Effective ingredients of school-based drug prevention programs. A systematic review. Addictive Behaviors. 2002;27:1009–1023. doi: 10.1016/s0306-4603(02)00295-2. [DOI] [PubMed] [Google Scholar]
- Currie C, Roberts C, Morgan A, Smith R, Settertobulte W, Samdal O, Rasmussen VB, editors. Young people’s health in context: Health Behaviour in School-aged Children (HBSC) study: International report from the 2001/2003 survey (Health Policy for Children and Adolescents, No. 4) Copenhagen, Denmark: World Health Organization; 2004. [Google Scholar]
- Deusinger IM. Frankfurter Selbstkonzeptskalen (FSKN). Handanweisung. Göttingen, Germany: Hogrefe; 1986. Frankfurt Self-Concept Scales. Manual. [Google Scholar]
- Donaldson SI, Sussman S, MacKinnon DP, Severson HH, Glynn T, Murray DM, Stone EJ. Drug abuse prevention programming: Do we know what content works? American Behavioral Scientist. 1996;39:868–883. [Google Scholar]
- Döpfner M, Berner W, Lehmkuhl G. Handbuch: Fragebogen für Jugendliche. Forschungsergebnisse zur deutschen Fassung der Youth Self-Report Form (YSR) der Child Behavior Checklist. Köln, Germany: Arbeitsgruppe Kinder-, Jugend- und Familiendiagnostik; 1994. Manual: Questionnaire for adolescents. Research findings pertaining to the German version of the Youth Self-Report Form (YSR)/Child Behavior Checklist. [Google Scholar]
- Ellickson PL, Tucker JS, Klein DJ. Ten-year prospective study of public health problems associated with early drinking. Pediatrics. 2003;111:949–955. doi: 10.1542/peds.111.5.949. [DOI] [PubMed] [Google Scholar]
- Flory K, Lynam D, Milich R, Leukefeld C, Clayton R. Early adolescent through young adult alcohol and marijuana use trajectories: Early predictors, young adult outcomes, and predictive utility. Development and Psychopathology. 2004;16:193–213. doi: 10.1017/s0954579404044475. [DOI] [PubMed] [Google Scholar]
- Franzkowiak P. Primary drug prevention: Developments in Germany since the 1970s. Journal of Drug Issues. 2002;32:491–502. [Google Scholar]
- Griffin KE, Botvin GJ, Nichols TR, Doyle MM. Effectiveness of a universal drug abuse prevention approach for youth at high risk for substance use initiation. Preventive Medicine. 2003;36:1–7. doi: 10.1006/pmed.2002.1133. [DOI] [PubMed] [Google Scholar]
- Hasselblad V, Hedges LV. Meta-analysis of screening and diagnostic tests. Psychological Bulletin. 1995;117:167–178. doi: 10.1037/0033-2909.117.1.167. [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Catalano RF, Miller JY. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: Implications for substance abuse prevention. Psychological Bulletin. 1992;112:64–105. doi: 10.1037/0033-2909.112.1.64. [DOI] [PubMed] [Google Scholar]
- Hipp JR, Bauer DJ. Local solutions in the estimation of growth mixture models. Psychological Methods. 2006;11:36–53. doi: 10.1037/1082-989X.11.1.36. [DOI] [PubMed] [Google Scholar]
- Hops H, Davis B, Lewin LM. The development of alcohol and other substance use: A gender study of family and peer context. Journal of Studies on Alcohol. 1999;(Suppl 13):22–31. doi: 10.15288/jsas.1999.s13.22. [DOI] [PubMed] [Google Scholar]
- Jackson KM, Sher KJ, Schulenberg JE. Conjoint developmental trajectories of young adult alcohol use and tobacco use. Journal of Abnormal Psychology. 2005;114:612–626. doi: 10.1037/0021-843X.114.4.612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Johnson CA, Pentz MA, Weber MD, Dwyer JH, Baer N, MacKinnon DP, Flay BR. Relative effectiveness of comprehensive community programming for drug abuse prevention with high-risk and low-risk adolescents. Journal of Consulting and Clinical Psychology. 1990;58:474–456. doi: 10.1037//0022-006x.58.4.447. [DOI] [PubMed] [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE. Monitoring the Future national survey results on drug use, 1975–2005: Vol. 1. Secondary school students. Bethesda, MD: National Institute on Drug Abuse; 2006. NIH Publication No. 07–6205. [Google Scholar]
- Kumpfer KL, Williams MK, Baxley GB. Drug abuse prevention for at-risk groups. Rockville, MD: National Institute on Drug Abuse; 1997. [Google Scholar]
- Laurent J, Catanzaro SJ, Callan KM. Stress, alcohol-related expectancies and coping preferences: A replication with adolescents of the Cooper et al. (1992) model. Journal of Studies on Alcohol. 1997;58:644–651. doi: 10.15288/jsa.1997.58.644. [DOI] [PubMed] [Google Scholar]
- Li F, Duncan TE, Hops H. Examining developmental trajectories in adolescent alcohol use using piecewise growth mixture modeling analysis. Journal of Studies on Alcohol. 2001;62:199–210. doi: 10.15288/jsa.2001.62.199. [DOI] [PubMed] [Google Scholar]
- Little RJA, Rubin DB. Statistical analysis with missing data. 2. New York, NY: Wiley; 2002. [Google Scholar]
- Liu LY. Texas school survey of substance use among students: Grades 4–6, 2002. Austin, TX: Texas Commission on Alcohol and Drug Abuse; 2003. Retrieved from http://www.tcada.state.tx.us. [Google Scholar]
- Lo Y, Mendell NR, Rubin DB. Testing the number of components in a normal mixture. Biometrika. 2001;88:767–778. [Google Scholar]
- Masterman PW, Kelly AB. Reaching adolescents who drink harmfully: Fitting intervention to developmental reality. Journal of Substance Abuse Treatment. 2003;24:347–355. doi: 10.1016/s0740-5472(03)00047-3. [DOI] [PubMed] [Google Scholar]
- McLachlan GJ, Peel D. Finite mixture models. New York, NY: Wiley; 2000. [Google Scholar]
- Mrazek PJ, Haggerty RJ, editors. Reducing risks for mental disorders: Frontiers for preventive intervention research. Washington, DC: National Academies Press; 1994. [PubMed] [Google Scholar]
- Muthén B. Two-part growth mixture modeling. 2001 (Unpublished manuscript). Retrieved from http://www.statmodel.com.
- Muthén B. Statistical and substantive checking in growth mixture modeling: Comment on Bauer and Curran (2003) Psychological Methods. 2003;8:369–377. doi: 10.1037/1082-989X.8.3.369. [DOI] [PubMed] [Google Scholar]
- Muthén B. Latent variable analysis: Growth mixture modeling and related techniques for longitudinal data. In: Kaplan D, editor. The Sage handbook of quantitative methodology for the social sciences. Newbury Park, CA: Sage; 2004. pp. 354–368. [Google Scholar]
- Muthén B, Brown CH, Masyn K, Jo B, Khoo ST, Yang CC, Liao J. General growth mixture modeling for randomized preventive interventions. Biostatistics. 2002;3:459–475. doi: 10.1093/biostatistics/3.4.459. [DOI] [PubMed] [Google Scholar]
- Muthén B, Satorra A. Complex sample data in structural equation modeling. In: Marsden PV, editor. Sociological methodology. Washington, DC: American Sociological Association; 1995. pp. 267–316. [Google Scholar]
- Muthén LK, Muthén BO. Mplus user’s guide: Statistical analysis with latent variables. 5. Los Angeles, CA: Author; 2007. [Google Scholar]
- Nagin DS. Group-based modeling of development. Boston, MA: Harvard University Press; 2005. [Google Scholar]
- Oetting ER, Beauvais F. Peer cluster theory: Drugs and the adolescent. Journal of Counseling & Development. 1986;65:17–22. [Google Scholar]
- Oetting ER, Beauvais F. Adolescent drug use: Findings of national and local surveys. Journal of Consulting and Clinical Psychology. 1990;58:385–394. doi: 10.1037//0022-006x.58.4.385. [DOI] [PubMed] [Google Scholar]
- Olsen MK, Schafer JL. A two-part random-effects model for semicontinuous longitudinal data. Journal of the American Statistical Association. 2001;96:730–745. [Google Scholar]
- Paglia A, Room R. Preventing substance use problems among youth: A literature review and recommendations. Journal of Primary Prevention. 1999;20:3–50. [Google Scholar]
- Ramaswamy V, Desarbo WS, Reibstein DJ, Robinson WT. An empirical pooling approach for estimating marketing mix elasticities with PIMS data. Marketing Science. 1993;12:103–124. [Google Scholar]
- Rosenberg M, Schooler C, Schoenbach C, Rosenberg F. Global self-esteem and specific self-esteem: Different concepts, different outcomes. American Sociological Review. 1995;60:141–156. [Google Scholar]
- Satorra A. Scaled and adjusted restricted tests in multiple-sample analysis of moment structures. In: Heijmans RDH, Pollock DSG, Satorra A, editors. Innovations in multivariate statistical analysis. A Festschrift for Heinz Neudecker. London, England: Kluwer Academic; 2000. pp. 233–247. [Google Scholar]
- Schwarz G. Estimating the dimension of a model. Annals of Statistics. 1978;6:461–464. [Google Scholar]
- Simon R, Tauscher M, Pfeiffer T. Suchtbericht Deutschland 1999. Hohengehren, Germany: Schneider-Verlag; 1999. Report on addictions in Germany 1999. [Google Scholar]
- Simons LS, Whitbeck LB, Conger RD, Melby JN. The effect of social skills, values, peers, and depression on adolescent substance use. Journal of Early Adolescence. 1991;11:466–481. [Google Scholar]
- Skara S, Sussman S. A review of 25 long-term adolescent tobacco and other drug use prevention program evaluations. Preventive Medicine. 2003;37:451–474. doi: 10.1016/s0091-7435(03)00166-x. [DOI] [PubMed] [Google Scholar]
- Spoth R, Greenberg M, Turrisi R. Preventive interventions addressing underage drinking: State of the evidence and steps toward public health impact. Pediatrics. 2008;121:S311–S336. doi: 10.1542/peds.2007-2243E. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Springer JF, Sale E, Hermann J, Sambrano S, Kasim R, Nistler M. Characteristics of effective substance abuse prevention programs for high-risk youth. Journal of Primary Prevention. 2004;25:171–194. [Google Scholar]
- Stapleton LM. An assessment of practical solutions for structural equation modeling with complex sample data. Structural Equation Modeling. 2006;13:28–58. [Google Scholar]
- Swaim RC. Childhood risk factors and adolescent drug and alcohol abuse. Educational Psychology Review. 1991;3:363–398. [Google Scholar]
- Tarter RE, Vanyukov M, Giancola P, Dawes M, Blackson T, Mezzich A, Clark DB. Etiology of early age onset substance use disorder: A maturational perspective. Development and Psychopathology. 1999;11:657–683. doi: 10.1017/s0954579499002266. [DOI] [PubMed] [Google Scholar]
- Tobler NS, Roona MR, Marshall DG, Streke AV, Stackpole KM. School-based adolescent drug prevention programs: 1998 meta-analysis. Journal of Primary Prevention. 2000;20:275–336. [Google Scholar]
- van der Vorst H, Vermulst AA, Meeus WHJ, Deković M, Engels RCME. Identification and prediction of drinking trajectories in early and mid-adolescence. Journal of Clinical Child & Adolescent Psychology. 2009;38:329–341. doi: 10.1080/15374410902851648. [DOI] [PubMed] [Google Scholar]
- van Lier PAC, Muthén BO, van der Sar RM, Crijnen AAM. Preventing disruptive behavior in elementary schoolchildren: Impact of a universal classroom-based intervention. Journal of Consulting and Clinical Psychology. 2004;72:467–748. doi: 10.1037/0022-006X.72.3.467. [DOI] [PubMed] [Google Scholar]
- Vitaro F, Dobkin PL. Prevention of substance use/abuse in early adolescents with behavior problems. Journal of Alcohol and Drug Education. 1996;41:11–38. [Google Scholar]
- Weber MD, Graham JW, Hansen WB, Flay BR, Johnson CA. Evidence for two paths of alcohol use onset in adolescents. Addictive Behaviors. 1989;14:399–408. doi: 10.1016/0306-4603(89)90027-0. [DOI] [PubMed] [Google Scholar]
- Weichold K. Prevention against substance misuse: Life skills and positive youth development. In: Silbereisen RK, Lerner RM, editors. Approaches to positive youth development. London, England: Sage; 2007. pp. 293–310. [Google Scholar]
- Weichold K, Bühler A, Silbereisen RK. Konsum von Alkohol und illegalen Drogen im Jugendalter [Consumption of alcohol and illegal drugs in adolescence] In: Silbereisen RK, Hasselhorn M, editors. Enzyklopädie der Psychologie, Serie V: Entwicklung. Göttingen, Germany: Hogrefe; 2008. pp. 537–586. [Google Scholar]
- Weichold K, Giannotta F, Silbereisen RK, Ciairano S, Wenzel V. Cross-cultural evaluation of a life-skills program to combat adolescent substance misuse. Sucht. 2006;52:268–278. [Google Scholar]
- Wiesner M, Weichold K, Silbereisen RK. Trajectories of alcohol use among adolescent boys and girls: Identification, validation, and sociodemographic characteristics. Psychology of Addictive Behaviors. 2007;21:62–75. doi: 10.1037/0893-164X.21.1.62. [DOI] [PubMed] [Google Scholar]
- Wild LG, Flisher AJ, Bhana A, Lombard C. Associations among adolescent risk behaviours and self-esteem in six domains. Journal of Child Psychology and Psychiatry. 2004;45:1454–1467. doi: 10.1111/j.1469-7610.2004.00851.x. [DOI] [PubMed] [Google Scholar]
- Wills TA, DuHamel K, Vaccaro D. Activity and mood temperament as predictors of adolescent substance use: Test of a self-regulation mediational model. Journal of Personality and Social Psychology. 1995;68:901–916. doi: 10.1037//0022-3514.68.5.901. [DOI] [PubMed] [Google Scholar]
- Windle M. Parental, sibling and peer influences on adolescent substance use and alcohol problems. Applied Developmental Science. 2000;4:98–110. [Google Scholar]
- Windle M, Lerner RM. Reassessing the dimensions of temperamental individuality across the life span: The Revised Dimensions of Temperament Survey (DOTS-R) Journal of Adolescent Research. 1986;1:213–229. [Google Scholar]
- Windle M, Spear LP, Fuligni AJ, Angold A, Brown JD, Pine D, Dahl RE. Transitions into underage and problem drinking: Developmental processes and mechanisms between 10 and 15 years of age. Pediatrics. 2008;121:S273–S289. doi: 10.1542/peds.2007-2243C. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Witkiewitz K, van der Maas HLJ, Hufford MR, Marlatt GA. Nonnormality and divergence in posttreatment alcohol use: Reexamining the Project MATCH data “another way. Journal of Abnormal Psychology. 2007;116:378–394. doi: 10.1037/0021-843X.116.2.378. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Woodward LJ, Fergusson DM. Childhood peer relationship problems and psychosocial adjustment in late adolescence. Journal of Abnormal Child Psychology. 1999;27:87–104. doi: 10.1023/a:1022618608802. [DOI] [PubMed] [Google Scholar]
- World Health Organization. Life skills education in schools. Geneva, Switzerland: Author; 1997. [Google Scholar]
- Zimmerman MA, Copeland LA, Shope JT, Dielman TE. A longitudinal study of self-esteem: Implications for adolescent development. Journal of Youth and Adolescence. 1997;26:117–141. [Google Scholar]
- Zucker RA, Donovan JE, Masten AS, Mattson ME, Moss HB. Early developmental processes and the continuity of risk of underage drinking and problem drinking. Pediatrics. 2008;121:S252–S272. doi: 10.1542/peds.2007-2243B. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zucker RA, Fitzgerald HE, Moses HD. Emergence of alcohol problems and the several alcoholisms: A developmental perspective on etiologic theory and life course trajectory. In: Cicchetti D, Cohen DJ, editors. Developmental psychopathology: Vol. 2. Risk, disorder and adaptation. New York, NY: Wiley; 1995. pp. 677–711. [Google Scholar]