

Abstract
High anisometropic myopia is a rare condition in twins. Genetic factors have been implicated in its development and there may be an association with vision-threatening complications. A pair of 11-year-old twins presented with poor distance vision in both eyes. Detailed ocular examination was performed including slit lamp examination, dilated funduscopy, cycloplegic refraction, keratometry and axial length measurement. The objective refraction was -6.50DS -2.00DC × 180 (right eye), -1.00DS (left eye) for the first twin; -13.75DS -2.25DC × 180 (right eye), -0.50DS -0.75DC × 04 (left eye) for the second twin. This case suggests an underlying genetic defect in the development of myopia.
Keywords: Anisometropia, Myopia, Twins
INTRODUCTION
Myopia has a multifactorial origin with interaction between genetic and environmental factors.1 Genetic factors play a major role in the development of myopia. For example, studies of twins indicate that genetic factors may account for up to 80% of the variance in myopia irrespective of the age of onset.2 The prevalence of myopia has been steadily increasing over the last few decades3,4 with wide racial differences.4,5 A study from England, reported the prevalence of myopia in 10-11 year-old children as 25.2%, 10.0%, and 3.4% in South Asians, African-Caribbeans and white Europeans, respectively.5 In developing countries in Asia, high myopia accounted for 10-20% of the over 80% of high school dropouts who were myopic.6 Fitgerald et al.7 evaluated 145 children with high myopia and found bilateral high myopia to be more common with a prevalence of 64%. Severe myopia is a significant public health problem because it may be associated with myopic macular degeneration, cataract, glaucoma, peripheral retinal changes (such as lattice degeneration), retinal tears and holes as well as retinal detachment.8
Anisometropia, by definition, exists when there is a difference in refractive status between an individual's eyes.9 Myopic anisometropia is rare in twins. In this case report, I present the presence of severe anisometropic myopia in a pair of 11-year-old female identical twins.
CASE REPORT
A pair of 11-year-old identical twin sisters were seen in the eye clinic in April, 2012 with poor distant vision of one year duration. They had no associated complaints such as deviation of the eyes and there was no history of prior spectacle use. Their past medical histories were unremarkable. They were delivered at full term and there was no history suggestive of myopia in the family. The first twin had a distance visual acuity (VA) of counting fingers at two meters (0.03) in the right eye and near vision of N14 (0.4) and the left eye had a distance VA of 6/18 (0.3) and near vision of N4.5 (1.0). Cycloplegic (cyclopentolate 0.5%) refraction revealed an error of -6.50DS -2.00DC × 180 in the right eye and -1.00DS in the left eye. Best corrected VA was 6/12 (0.5) and N5 (0.9) with -6.00DS -2.00DC × 180 for the right eye and 6/6 (1.0) and N4.5 (1.0) with -1.00DS for the left eye. The difference in the spherical equivalent between the two eyes was - 6.5 diopters (D). On ocular examination there was no abnormality in the anterior segment of either eye. Funduscopic examination revealed a pink disc with peripapillary chorioretinal atrophy in the right eye and a normal fundus in the left eye. The patient was prescribed spectacles with full correction for the left eye and slight under-correction in the right eye.
The second twin had a distance VA of counting fingers at one meter (0.02) in the right eye and a near VA of N36 (0.1) while the left eye had a distance VA of 6/18 (0.3) and near vision of N4.5 (1.0). Cycloplegic refraction revealed an error of - 13.75DS - 2.25DC × 180 in the right eye and - 0.50DS -0.75DC × 04 in the left eye. There was no improvement in the VA with refraction in the right eye while the best corrected VA was 6/6 (1.0) and N4.5 (1.0) with - 0.50DS -0.50DC × 030 in the left eye. The difference in the spherical equivalent between the two eyes was -14D. On ocular examination, the anterior segments in both eyes were normal. Funduscopy revealed a hypoplastic disc with peripapillary chorioretinal atrophy in the right eye while the left fundus was normal. The patient was prescribed spectacles with full correction for the left eye and balanced for the right eye. There was no strabismus, and systemic examination did not reveal features of any genetic defect suggestive of syndromic high myopia. Genetic studies could not be performed due to the lack of the necessary facilities.
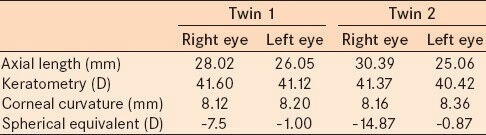
The refraction, radius of anterior corneal curvature and corneal refractive power were measured using the autorefractokeratometer (Accuref–K 9001; Ajinomoto Trading, Inc., Tokyo, Japan). Axial length was measured with an A-scan ultrasonographer (Storz Alpha II; Bausch and Lomb Storz® Instruments, Rochester, NY, USA). The results of these measurements are presented in Table 1.
Table 1.
Biometry and refraction results
DISCUSSION
The occurrence of anisometropic myopia in identical twins with degenerative myopia in the same eye and simple myopia in the other suggests an underlying genetic defect in this condition. Genetic factors have been shown to have a major role to play in the development of myopia. Twin studies in European-derived populations have reported high heritability for myopia, in the 90% range, with similar figures for the various biometric factors that control refractive error, such as axial length, anterior chamber depth and corneal curvature.10 Recently, a genome-wide association study identified a susceptibility locus for myopia on chromosome 15q14.11 The genetic basis for the dissimilar growth between eyes in cases of unilateral high myopia has been attributed to the skewed lyonization in females heterozygous for X-linked myopia.12 Skewed X-chromosome inactivation in the eye has been found in monozygotic twins and eye pairs of individuals discordant for color vision deficiency.13 The difference in the right eyes of the sisters in this report may be due to variable expression of the underlying genetic defect. Myopia can occur as an isolated finding or as a part of specific genetic syndromes.14 These syndromes include the syndromic high myopias, in which high myopia is associated with other symptoms that define the disease, such as connective tissue disorders (e.g., Marfan and Stickler syndromes), and complete and incomplete congenital stationary night blindness.3 Unlike these syndromes, however, the vast majority of individuals with moderate or severe myopia, have no associated defects.14 The absence of associated defects in these sisters suggests a non-syndromic high myopia.
Myopic anisometropia is a rare type of anisometropia.9 If it occurs with intact near vision it seldom results in amblyopia. When ordinary vision is however defocused due to high myopia, refractive amblyopia may occur.9 Mild myopic anisometropia (less than -3D) usually does not cause amblyopia but unilateral high myopia (-6D or more) often results in severe amblyopic visual loss.15 Unilateral high myopia with a difference of over -6D between the two eyes of the sisters in this report would account for the occurrence of amblyopia in the right eyes.
Severe myopia may be associated with posterior segment pathology. There was chorioretinal atrophy in the right eyes of both sisters with optic disc hypoplasia in the twin with the greater axial length. This could also have been a contributory factor in the development of amblyopia. Weiss12 evaluated 48 children with anisometropic myopia and reported a high prevalence of unilateral optic nerve hypoplasia with associated visual deficits.
Amblyopia due to anisometropia is difficult to detect and is essentially asymptomatic unless accompanied by a squint.16,17 Diagnosis is therefore usually late16 as in the current case report. The standard treatment for anisometropic amblyopia is correction of any refractive error with occlusion therapy.16 Refractive correction is performed first using spectacles and/or contact lenses with subsequent patching and near activities once visual acuity plateaus.18 High anisometropic amblyopia is however challenging to manage16,18 and has been reported to be the least responsive subtype of anisometropic amblyopia to treatment.19 As a result, many clinicians would undercorrect the more myopic eye of these patients in order to allow the lenses to be more balanced optically and cosmetically, and do not pursue further treatment.18
Contact lenses with occlusion therapy can be used safely in children with amblyopia due to high anisometropia.16 This would have been the preferred treatment option in this case but compliance and regular follow-up were identified as likely problems. Contact lenses may also be problematic.20 Contacts can be difficult to insert and remove, are frequently lost, can be irritating to the eye or may be too costly.21 Both sisters were boarding students and adequate supervision to ensure compliance could not be guaranteed in the absence of their parents. Compliance with amblyopia treatment has been found to be the most critical factor for predicting a successful outcome.22
Conventional treatment with glasses and occlusion therapy is usually unsuccessful but may be worth instituting as initial management.16 Refractive correction alone using spectacles was performed for both sisters with undercorrection of the more myopic eye. Full refractive correction was not possible as the difference in the spherical equivalents would result in aniseikonia.
Refractive surgery, although controversial, is another option in the management of pediatric refractive errors.23 The main indications are bilateral high ametropia and anisometropia where conventional treatment with spectacles or contact lens is not tolerated.24 The most commonly performed procedures currently are surface ablation procedures using excimer laser.24 The major drawback of surface ablation procedures is refractive regression, which is more pronounced in higher degrees of ametropia.21,24 When corneal refractive surgery is not possible, such as in extremely high myopia, phakic intraocular lens may be an option.23,25 Long-term endothelial cell loss remains a source of concern with phakic intraocular lens.24 The advantages of these lenses are reversibility, predictability, and lack of regression.24 Refractive surgery however has a limited role to play in the management of refractive errors in our environment as the equipment required are very expensive and are not readily available.
Regular monitoring of refraction in these sisters is mandatory as the myopia may still progress with an increase in the axial length of the eyes. For children between the ages of 6 and 15 years with myopia, increased progression in younger children and in those with greater myopia at the baseline examination has been a consistent finding.26
In conclusion, high anisometropic myopia may result in severe amblyopia especially when there is an associated abnormality of the eye. This case report is highly suggestive of an underlying genetic defect in its development.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Mehdizadeh M, Jalaeian H, Kashef MA. Effects of various risk factors on myopia progression. Iran J Med Sci. 2006;31:204–7. [Google Scholar]
- 2.Dirani M, Chamberlain M, Garoufalis P, Chen C, Guymer RH, Baird PN. Refractive errors in twin studies. Twin Res Hum Genet. 2006;9:566–72. doi: 10.1375/183242706778024955. [DOI] [PubMed] [Google Scholar]
- 3.Morgan IG, Ohno-Matsui K, Saw SM. Myopia. Lancet. 2012;379:1739–48. doi: 10.1016/S0140-6736(12)60272-4. [DOI] [PubMed] [Google Scholar]
- 4.Bar Dayan Y, Levin A, Morad Y, Grotto I, Ben-David R, Goldberg A, et al. The changing prevalence of myopia in young adults: A 13-year series of population-based prevalence surveys. Invest Ophthalmol Vis Sci. 2005;46:2760–5. doi: 10.1167/iovs.04-0260. [DOI] [PubMed] [Google Scholar]
- 5.Rudnicka AR, Owen CG, Nightingale CM, Cook DG, Whincup PH. Ethnic differences in the prevalence of myopia and ocular biometry in 10- and 11-year-old children: The Child Heart and Health Study in England (CHASE) Invest Ophthalmol Vis Sci. 2010;51:6270–6. doi: 10.1167/iovs.10-5528. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Lin LL, Shih YF, Hsiao CK, Chen CJ. Prevalence of myopia in Taiwanese school children: 1983 to 2000. Ann Acad Med Singapore. 2004;33:27–33. [PubMed] [Google Scholar]
- 7.FitzGerald DE, Chung I, Krumholtz I. An analysis of high myopia in a pediatric population less than 10 years of age. Optometry. 2005;76:102–14. doi: 10.1016/s1529-1839(05)70263-3. [DOI] [PubMed] [Google Scholar]
- 8.Saw SM, Katz J, Schein OD, Chew SJ, Chan TK. Epidemiology of myopia. Epidemiol Rev. 1996;18:175–87. doi: 10.1093/oxfordjournals.epirev.a017924. [DOI] [PubMed] [Google Scholar]
- 9.Park SJ, Kim JY, Baek SH, Kim ES, Kim US. One sister and brother with mirror image myopic anisometropia. Korean J Ophthalmol. 2010;24:62–4. doi: 10.3341/kjo.2010.24.1.62. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Lyhne N, Sjølie AK, Kyvik KO, Green A. The importance of genes and environment for ocular refraction and its determiners: A population based study among 20-45 year old twins. Br J Ophthalmol. 2001;85:1470–6. doi: 10.1136/bjo.85.12.1470. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Verhoeven VJ, Hysi PG, Saw SM, Vitart V, Mirshahi A, Guggenheim JA, et al. Large scale international replication and meta-analysis study confirms association of the 15q14 locus with myopia. The CREAM consortium. Hum Genet. 2012;131:1467–80. doi: 10.1007/s00439-012-1176-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Weiss AH. Unilateral high myopia: Optical components, associated factors, and visual outcomes. Br J Ophthalmol. 2003;87:1025–31. doi: 10.1136/bjo.87.8.1025. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Jørgensen AL, Philip J, Raskind WH, Matsushita M, Christensen B, Dreyer V, et al. Different patterns of X inactivation in MZ twins discordant for red-green color-vision deficiency. Am J Hum Genet. 1992;51:291–8. [PMC free article] [PubMed] [Google Scholar]
- 14.Young TL. Dissecting the genetics of human high myopia: A molecular biological approach. Trans Am Ophthalmol Soc. 2004;102:423–45. [PMC free article] [PubMed] [Google Scholar]
- 15.Sethi S, Sethi MJ, Hussain I, Kundi NK. Causes of amblyopia in children coming to ophthalmology out patient department, Khyber Teaching Hospital, Peshawar. J Pak Med Assoc. 2008;58:125–8. [PubMed] [Google Scholar]
- 16.Roberts CJ, Adams GG. Contact lenses in the management of high anisometropic amblyopia. Eye (Lond) 2002;16:577–9. doi: 10.1038/sj.eye.6700159. [DOI] [PubMed] [Google Scholar]
- 17.Cobb CJ, Russel K, Cox A, MacEwen CJ. Factors influencing visual outcome in anisometropic amblyopes. Br J Ophthalmol. 2002;86:1278–81. doi: 10.1136/bjo.86.11.1278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Pang Y, Allison C, Frantz KA, Block S, Goodfellow GW. A prospective pilot study of treatment outcomes for amblyopia associated with myopic anisometropia. Arch Ophthalmol. 2012;130:579–84. doi: 10.1001/archopthalmol.2011.1203. [DOI] [PubMed] [Google Scholar]
- 19.Kutschke PJ, Scott WE, Keech RV. Anisometropic amblyopia. Ophthalmology. 1991;98:258–63. doi: 10.1016/s0161-6420(91)32307-8. [DOI] [PubMed] [Google Scholar]
- 20.Paysse EA. Refractive surgery in children: Is it ready for prime time? Am Orthopt J. 2007;57:79–88. doi: 10.3368/aoj.57.1.79. [DOI] [PubMed] [Google Scholar]
- 21.Tychsen L. Refractive surgery for children: Laser, implants, current results and future directions. Expert Rev Ophthalmol. 2008;3:635–43. [Google Scholar]
- 22.Lithander J, Sjöstrand J. Anisometropic and strabismic amblyopia in the age group 2 years and above: a prospective study of results of treatment. Br J Ophthalmol. 1991;75:111–6. doi: 10.1136/bjo.75.2.111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Daoud YJ, Hutchinson A, Wallace DK, Song J, Kim T. Refractive surgery in children: Treatment options, outcomes, and controversies. Am J Ophthalmol. 2009;147:573–82. doi: 10.1016/j.ajo.2008.12.028. [DOI] [PubMed] [Google Scholar]
- 24.Moran S, O'Keefe M. Refractive surgery in children. Asia Pac J Ophthalmol. 2012:235–9. doi: 10.1097/APO.0b013e31825ffff1. [DOI] [PubMed] [Google Scholar]
- 25.Chipont EM, García-Hermosa P, Alió JL. Reversal of myopic anisometropic amblyopia with phakic intraocular lens implantation. J Refract Surg. 2001;17:460–2. doi: 10.3928/1081-597X-20010701-08. [DOI] [PubMed] [Google Scholar]
- 26.Jensen H. Myopia progression in young school children. A prospective study of myopia progression and the effect of a trial with bifocal lenses and beta blocker eye drops. Acta Ophthalmol. 1991;69:1–79. [PubMed] [Google Scholar]