

Abstract
AIM: To establish a rapid and accurate method for the detection of lamivudine-resistant mutations in hepatitis B virus and monitor of lamivudine resistance during lamivudine treatment in patients with chronic hepatitis B virus infection.
METHODS: We established a real-time PCR method using a universal template and TaqMan probe to detect YMDD mutants. Variants of YVDD and YIDD were tested by individual reactions (reaction V and reaction I) and total hepatitis B viruses were detected in another reaction for control (reaction C). Results were determined by ΔCt < 3.5 (ΔCt = Ct of reaction V or I - Ct of reaction C). Clones of the HBV polymerase gene containing different YMDD mutations were tested. Serum samples from 163 lamivudine-treated patients with chronic hepatitis B virus infection were detected using this method and the results were confirmed by DNA sequencing.
RESULTS: As many as 1 000 copies per milliliter of wide-type plasmid were detected and nonspecific priming was excluded. In the 163 samples from patients treated with lamivudine, lamivudine-resistant mutations were detected in 51 samples.
CONCLUSION: This universal real-time PCR is a rapid and accurate method for quantification of YMDD mutants of HBV virus in lamivudine-treated patients and can be used to monitor lamivudine-resistant mutations before and during lamivudine therapy.
Keywords: HBV, YMDD, Mutation, UT-PCR
INTRODUCTION
It is estimated that approximately 350 million persons worldwide are chronically infected with hepatitis B virus (HBV)[1,2]. HBV is the leading cause of liver cirrhosis and hepatocellular carcinima (HCC) and is responsible for 60 - 80% of all HCC cases[2,3]. Treatment of HBV infection has been revolutionized by the introduction of antiviral drugs such as lamivudine. However, long-term monotherapy commonly does not result in complete suppression of viral replication and is associated with the emergence of resistant mutants[4-7]. Specific mutations that result in replacement of methionine (M) in tyrosine-methionine-aspartate-aspartate (YMDD) motif of HBV reverse transcriptase (rt) by valine (V), isoleucine (I), or serine (S) confer resistance to lamivudine[8].
Mutations leading to lamivudine resistance can be detected by direct sequencing of HBV DNA after PCR amplification of a selected part of the viral polymerase gene. However, this is expensive, laborious and time-consuming with low level of sensitivity, usually detecting 20% the total virus population[9]. Other molecular techniques, such as restriction fragment length polymorphism (RFLP)[10], 5’ nuclease assay[11], line probe assay[12], peptide nucleic acid-mediated PCR clamping[13,14], and oligonucleotide chips[15], overcome some of the limitations of DNA sequencing, but they are also time-consuming and expensive. Recent studies using real-time PCR have obtained quantitative results but cannot avoid nonspecific amplification[16,17].
In the present study, we established a rapid and accurate method for the detection of lamivudine-resistant mutations in HBV based on real-time PCR using a universal template. Positive and negative controls were included to evaluate the quality of the assay.
MATERIALS AND METHODS
Patients and extraction of HBV DNA
Serum samples were collected from 163 patients with chronic HBV infection who had received lamivudine monotherapy for one to two years. The ethical committee of our hospital approved the study and oral consent was obtained from the patients. HBV DNA was extracted from serum samples using the QIAamp blood kit (Qiagen, Chatsworth, California) as described elsewhere[11].
Primers and probe
The primers and probe used in this study are summarized in Table 1. Two different reverse primers that would selectively amplify the YVDD (rtM204V) and YIDD (rtM204I) quasispecies and a common reverse primer to a highly conserved sequence within the polymerase open reading frame were used to discriminate different mutants. The amplicon was detected by real-time PCR with a TaqMan probe that annealed to the universal template linked to the primers. A universal forward primer was used in the control for amplification of all kinds of quasispecies. A universal template was linked to each primer as described previously[18]. In brief, the universal template (UT) sequence with a size of 21 bp was attached to the 5’ end of the primers specific to YMDD variants[17]. The UT probe was labeled with 6-carboxyfluorescein (FAM) at the 5’ end and DABCYL quencher at the 3’ end. During the annealing phase, the UT probe specifically annealed to the 5’ end of the UT-PCR primer and the 3’ end of the UT-PCR primer specifically annealed to the target sequence and was extended. Due to the 5’ exonuclease activity of DNA polymerase, the hybridized UT probe was hydrolyzed, leading to the separation of the reporter moiety from the quencher moiety and the generation of a fluorescent signal. The signal could be detected by ABI 7 000 real-time PCR system (Applied Biosystems Inc. California, USA).
Table 1.
Primers and probe used in universal RT-PCR
| Primers or probe | Sequence |
| Reverse primers | |
| Reaction V | 5’-CCCCCAATACCACATCATCC-3’ |
| Reaction I | 5’-CCCCCAATACCACATCATCA-3’ |
| Reaction C | 5’-CCCCCAATACCACATCATC-3’ |
| Forward primers | 5’-tgaggagcacgagacggaagtATACAA CACCTGTATTCCCATCCCAT-3’ |
| Probe | 5’-FAM ACTTCCGTCTCGTGCTCCTCA TAMRA-3’ |
Real-time PCR
The amplification was performed on ABI 7 000 with a final volume of 50 μl by incubating the reaction mixture at 50 °C for 2 min and at 95 °C for 5 min, followed by 40 cycles of PCR amplification at 94 °C for 20 s and at 55 °C for 30 s. The reaction mixture contained the following components: 1×PCR buffer, 100 nmol/L primers and probes, 400 μmol/L each of dATP, dGTP, dCTP and dUTP, 1.5 units of hot-start Taq DNA polymerase, 0.2 units of Amperase uracil N-glycosylase (UNG), 3 mmol/L MgCl2, 20 mmol/L KCl. The amplification was optimized in Fosun Diagnostics (Fosun Diagnostics, Shanghai, China). Variants of YVDD and YIDD and total HBV virus were amplified in individual reactions (reactions V, I and C for YVDD, YIDD and HBV virus respectively). The positive results were determined by ΔCt < 3.5. ΔCt = Ct of reaction V or I - Ct of reaction C.
DNA sequencing
The DNA sequence of the domain C of HBV polymerase gene was analyzed as described elsewhere[11]. In brief, HBV DNA extracted from serum samples was amplified by PCR. PCR products were purified and sequenced by ABI 310 sequencer (Applied Biosystems Inc., California, USA)
RESULTS
Specificity of primers and probe
Mismatched templates and primers (mutant primers to wild-type templates and vice versa) were used to validate this assay. Dilution series of 108, 106, 104 copies per milliliter were used and PCR was performed with the mismatched primers. Nonspecific priming to the alternate template was observed at the template concentrations of 106 and 108 copies per milliliter but not at 104 copies per milliliter. Similar to previous study[17], the degree of cross-priming was at least 4 logs. For exclusion of nonspecific priming, the positive results were determined by ΔCt < 3.5. ΔCt = Ct of reaction V or I - Ct of reaction C.
Sensitivity and limit of detection
Mixing experiments were performed to determine the sensitivity of the assay. Mutant and wild-type plasmids were mixed with the ratio of 0:1, 1:1, 1:10, 1:100 and 1:1000 at end concentrations of 105, 106, 107 and 108 copies per milliliter respectively (five replicates for each mixture). In all the mixtures, the detection limit of the assay was 1 000 copies per milliliter.
Comparison of real-time UT-PCR and sequencing
The assay was evaluated using serum from 163 lamivudine-treated patients with chronic HBV infection. All the patients treated with lamivudine alone for one to two years were HBV DNA positive by real-time PCR. Real-time UT-PCR was performed with all the samples together with positive and negative controls. Fifty-one (31%) of 163 samples were detected with YVDD (Figure 1) or YIDD mutants (YMDD in 112, YIDD in 21, YVDD in 27 and YIDD + YVDD in 3). YMDD mutations were detected in 19% (14 of 73) of the patients treated with lamivudine for one year and in 40% (37 of 90) of the patients treated for two years. The results of real-time UT-PCR and sequencing were concordant in 15 randomly selected samples (Table 2).
Figure 1.
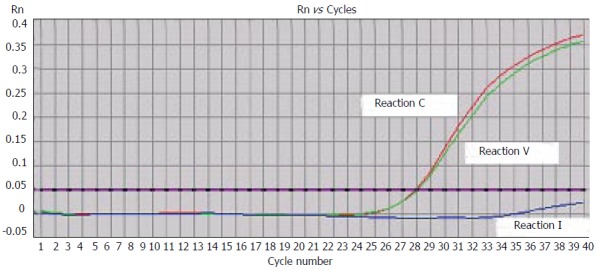
Detection of YMDD mutants using real-time UT-PCR. Three parallel reactions showed YVDD mutant.
Table 2.
Comparison of results obtained by real-time PCR and sequencing
| Samples | HBV DNA (Copies/mL) | Result of UT-PCR | Result of sequencing |
| 1 | 2.49 × 105 | YMDD | 5′ -TATATGGATGAT-3′ |
| 2 | 4.73 × 107 | YIDD | 5′ -TATATTGATGAT-3′ |
| 3 | 6.10 × 103 | YMDD | 5′ -TATATGGATGAT-3′ |
| 4 | 6.24 × 106 | YIDD | 5′ -TATATTGATGAT-3′ |
| 5 | 2.98 × 109 | YIDD | 5′ -TATATTGATGAT-3′ |
| 6 | 8.13 × 106 | YMDD | 5′ -TATATGGATGAT-3′ |
| 7 | 1.35 × 104 | YMDD | 5′ -TATATGGATGAT-3′ |
| 8 | 3.57 × 103 | YMDD | 5′ -TATATGGATGAT-3′ |
| 9 | 2.74 × 106 | YVDD | 5′ -TATGTGGATGAT-3′ |
| 10 | 9.10 × 104 | YVDD | 5′ -TATGTGGATGAT-3′ |
| 11 | 7.02 × 104 | YMDD | 5′ -TATATGGATGAT-3′ |
| 12 | 5.18 × 105 | YMDD | 5′ -TATATGGATGAT-3′ |
| 13 | 3.51 × 103 | YMDD | 5′ -TATATGGATGAT-3′ |
| 14 | 8.04 × 104 | YMDD | 5′ -TATATGGATGAT-3′ |
| 15 | 4.29 × 106 | YMDD | 5′ -TATATGGATGAT-3′ |
DISCUSSION
A more accurate and rapid method than DNA sequencing and RFLP is needed to detect and quantify the YMDD mutants in sera of chronic HBV infection patients before and during lamivudine therapy. A real-time UT-PCR assay has been developed for detection of YMDD mutations in a large number of patients. The detection limit of this assay is 1000 copies per milliliter of mutants and 1% within a mixed virus population at a concentration of 105 copies per milliliter of serum. This real-time UT-PCR assay is more sensitive than DNA sequencing. In addition, the result of the assay can be easily determined by the difference between Ct values of the mutant and the control and no quantitative standards are needed.
Real-time UT-PCR has two major advantages, namely the universal probe can be used for many target sequences and it is less expensive compared with other sequence-specific fluorescent PCR techniques[18]. In the present study, different YMDD variants were detected using different primers specific to the target DNA and a probe specific to the universal template, showing that it is cost-effective and convenient to detect different sequences simultaneously.
The overall prevalence of the YMDD mutations in the patients treated with lamivudine for one and two years in this study was 19% (14 of 73) and 40% (37 of 90), respectively, which is consistent with prevalence reported by previous studies[4,5,19]. Mixture of YIDD and YVDD variants was observed in three samples.
In the present study, the primer used to detect rtM204I was specific to sequence ATT. Sequences of ATG and ATC could not be detected by this assay. However, this could be improved by adding two reverse primers specific to ATG and ATC into the reaction used to detect YIDD (data not shown).
Several real-time PCR methods are availabe for the detection of YMDD mutations[16,17,20,21]. Selective primers have been used[16,17]. One of the most important advantages of this study is that the result of mutants could be easily determined by the difference between Ct values of the mutant and the control without additional quantitative standards. Furthermore, nonspecific priming could be excluded by the cut-off of ΔCt < 3.5 because the degree of cross-priming was at least 4 logs in this study and elsewhere[17]. The impact of the intra-assay variability is reduced in this assay. However, this arbitrarily determined cut-off value reduces the sensitivity of the assay. The real-time UT-PCR is cost effective and convenient for large scale screening in clinical practices.
In conclusion, the real-time PCR assay established in this study is a rapid and accurate tool for detection of lamivudine-resistant mutations before and during lamivudine therapy.
Footnotes
S- Editor Wang J L- Editor Zhang JZ E- Editor Ma WH
References
- 1.1 Maddrey WC. Hepatitis B--an important public health issue. Clin Lab. 2001;47:51–55. [PubMed] [Google Scholar]
- 2.Lai CL, Ratziu V, Yuen MF, Poynard T. Viral hepatitis B. Lancet. 2003;362:2089–2094. doi: 10.1016/S0140-6736(03)15108-2. [DOI] [PubMed] [Google Scholar]
- 3.Manigold T, Rehermann B. Chronic hepatitis B and hepatocarcinogenesis: does prevention of "collateral damage" bring the cure. Hepatology. 2003;37:707–710. doi: 10.1002/hep.510370328. [DOI] [PubMed] [Google Scholar]
- 4.Lai CL, Chien RN, Leung NW, Chang TT, Guan R, Tai DI, Ng KY, Wu PC, Dent JC, Barber J, et al. A one-year trial of lamivudine for chronic hepatitis B. Asia Hepatitis Lamivudine Study Group. N Engl J Med. 1998;339:61–68. doi: 10.1056/NEJM199807093390201. [DOI] [PubMed] [Google Scholar]
- 5.Leung NW, Lai CL, Chang TT, Guan R, Lee CM, Ng KY, Lim SG, Wu PC, Dent JC, Edmundson S, et al. Extended lamivudine treatment in patients with chronic hepatitis B enhances hepatitis B e antigen seroconversion rates: results after 3 years of therapy. Hepatology. 2001;33:1527–1532. doi: 10.1053/jhep.2001.25084. [DOI] [PubMed] [Google Scholar]
- 6.Yuen MF, Lai CL. Treatment of chronic hepatitis B. Lancet Infect Dis. 2001;1:232–241. doi: 10.1016/S1473-3099(01)00118-9. [DOI] [PubMed] [Google Scholar]
- 7.Hu KQ. A Practical Approach to Management of Chronic Hepatitis B. Int J Med Sci. 2005;2:17–23. doi: 10.7150/ijms.2.17. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Allen MI, Deslauriers M, Andrews CW, Tipples GA, Walters KA, Tyrrell DL, Brown N, Condreay LD. Identification and characterization of mutations in hepatitis B virus resistant to lamivudine. Lamivudine Clinical Investigation Group. Hepatology. 1998;27:1670–1677. doi: 10.1002/hep.510270628. [DOI] [PubMed] [Google Scholar]
- 9.Günthard HF, Frost SD, Leigh-Brown AJ, Ignacio CC, Kee K, Perelson AS, Spina CA, Havlir DV, Hezareh M, Looney DJ, et al. Evolution of envelope sequences of human immunodeficiency virus type 1 in cellular reservoirs in the setting of potent antiviral therapy. J Virol. 1999;73:9404–9412. doi: 10.1128/jvi.73.11.9404-9412.1999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Jardi R, Buti M, Rodriguez-Frias F, Cotrina M, Costa X, Pascual C, Esteban R, Guardia J. Rapid detection of lamivudine-resistant hepatitis B virus polymerase gene variants. J Virol Methods. 1999;83:181–187. doi: 10.1016/s0166-0934(99)00125-1. [DOI] [PubMed] [Google Scholar]
- 11.Allen MI, Gauthier J, DesLauriers M, Bourne EJ, Carrick KM, Baldanti F, Ross LL, Lutz MW, Condreay LD. Two sensitive PCR-based methods for detection of hepatitis B virus variants associated with reduced susceptibility to lamivudine. J Clin Microbiol. 1999;37:3338–3347. doi: 10.1128/jcm.37.10.3338-3347.1999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Stuyver L, Van Geyt C, De Gendt S, Van Reybroeck G, Zoulim F, Leroux-Roels G, Rossau R. Line probe assay for monitoring drug resistance in hepatitis B virus-infected patients during antiviral therapy. J Clin Microbiol. 2000;38:702–707. doi: 10.1128/jcm.38.2.702-707.2000. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Kirishima T, Okanoue T, Daimon Y, Itoh Y, Nakamura H, Morita A, Toyama T, Minami M. Detection of YMDD mutant using a novel sensitive method in chronic liver disease type B patients before and during lamivudine treatment. J Hepatol. 2002;37:259–265. doi: 10.1016/s0168-8278(02)00145-9. [DOI] [PubMed] [Google Scholar]
- 14.Ogata N, Ichida T, Aoyagi Y, Kitajima I. Development of peptide nucleic acid mediated polymerase chain reaction clamping (PMPC)--direct sequencing method for detecting lamivudine-resistant hepatitis B virus (HBV) variants with high sensitivity and specificity. Rinsho Byori. 2003;51:313–319. [PubMed] [Google Scholar]
- 15.Jang H, Cho M, Heo J, Kim H, Jun H, Shin W, Cho B, Park H, Kim C. Oligonucleotide chip for detection of Lamivudine-resistant hepatitis B virus. J Clin Microbiol. 2004;42:4181–4188. doi: 10.1128/JCM.42.9.4181-4188.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Punia P, Cane P, Teo CG, Saunders N. Quantitation of hepatitis B lamivudine resistant mutants by real-time amplification refractory mutation system PCR. J Hepatol. 2004;40:986–992. doi: 10.1016/j.jhep.2004.02.009. [DOI] [PubMed] [Google Scholar]
- 17.Wightman F, Walters T, Ayres A, Bowden S, Bartholomeusz A, Lau D, Locarnini S, Lewin SR. Comparison of sequence analysis and a novel discriminatory real-time PCR assay for detection and quantification of Lamivudine-resistant hepatitis B virus strains. J Clin Microbiol. 2004;42:3809–3812. doi: 10.1128/JCM.42.8.3809-3812.2004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Zhang Y, Zhang D, Li W, Chen J, Peng Y, Cao W. A novel real-time quantitative PCR method using attached universal template probe. Nucleic Acids Res. 2003;31:e123. doi: 10.1093/nar/gng123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Lai CL, Dienstag J, Schiff E, Leung NW, Atkins M, Hunt C, Brown N, Woessner M, Boehme R, Condreay L. Prevalence and clinical correlates of YMDD variants during lamivudine therapy for patients with chronic hepatitis B. Clin Infect Dis. 2003;36:687–696. doi: 10.1086/368083. [DOI] [PubMed] [Google Scholar]
- 20.Cane PA, Cook P, Ratcliffe D, Mutimer D, Pillay D. Use of real-time PCR and fluorimetry to detect lamivudine resistance-associated mutations in hepatitis B virus. Antimicrob Agents Chemother. 1999;43:1600–1608. doi: 10.1128/aac.43.7.1600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Whalley SA, Brown D, Teo CG, Dusheiko GM, Saunders NA. Monitoring the emergence of hepatitis B virus polymerase gene variants during lamivudine therapy using the LightCycler. J Clin Microbiol. 2001;39:1456–1459. doi: 10.1128/JCM.39.4.1456-1459.2001. [DOI] [PMC free article] [PubMed] [Google Scholar]