

Abstract
Background:
Traffic-related air pollution (TRAP) is a major source of air pollution but the impact on health in Nigeria is not well described.
Patients and Methods:
A descriptive cross-sectional study of road traffic workers and university students in Lagos. Eligible, accessible and willing participants were included in the sample. Respiratory symptoms and anthropometry were obtained from all the participants using an adapted Medical Research Council (MRC) questionnaire and they all did a spirometry test and exhaled carbon monoxide (CO) test.
Results:
Fifty-nine individuals participated with complete data, including 47 traffic policemen and 12 students who acted as controls. The mean age (SD) was 35.1 (8.0) and 35.4 years (6.3) for the traffic workers and students, respectively. All the respondents were men. The mean (SD) duration of occupation as a traffic policeman was 4.4 (4.4) and a median of 4 years (range 1-25). There was no significant difference in the presentation of respiratory and non-respiratory symptoms between the two groups. Compared with the students, the traffic workers had higher age, height and sex adjusted forced expiratory volume in one second and forced vital capacity. Traffic policemen had significantly higher levels of exhaled CO than the students (1.18 vs 0.73 ppm, P < 0.006).
Conclusion:
There is a high prevalence of respiratory symptoms in both traffic policemen and non-traffic residents of Lagos metropolis, indicating widespread pollution.
Keywords: Lung function, pollution, traffic, traffic policemen
INTRODUCTION
A number of previous studies have shown that air pollution predict mortality independent of cigarette smoking, especially deaths due to cancers and cardiovascular diseases.1,2,3,4 Several studies have also shown that the ambient levels of indoor and outdoor pollutants in many developing urban cities is substantial5,6,7,8,9 and associated with huge cost in economic terms and mortality.5 There are various sources of environmental pollution including traffic-related air pollution (TRAP). TRAP is a major source of particulate matter (PM), nitrous oxide, carbon dioxide, ozone and carbon monoxide (CO) pollution.6,10 Though it is relatively well established that there are high levels of TRAP in the atmosphere in many developing cities,6 the impact on health in Nigeria is not well described.
In 2011, the third international ministerial conference tagged ‘Africa Environment Outlook’ (AEO), reported that environmental risks contribute 28% of Africa's disease burden.11 Lagos is a densely populated city in Africa, which has undergone astronomical growth in population over the last four decades from an estimated 1.7 million inhabitants in 1975 to 10.5 million in 2010, and a projected estimate of 12.4 million by 2015.12 Consequently, there has been corresponding increases in traffic, number of vehicles and associated environmental pollutants in the atmosphere.13 Traffic policemen and commercial motorists spend most of their working hours exposed to environmental pollutions including vehicular emissions that contain unhealthily high concentrations of aromatic hydrocarbons, particles and CO-rich air.14 We hypothesise that traffic workers may, as a result, have a high burden of respiratory disease compared with age and sex matched non-exposed individuals.
We examined the ventilatory function, levels of exhaled CO and prevalence of respiratory symptoms among traffic workers using a sample of traffic policemen in a densely polluted area in Lagos, Nigeria.
PATIENTS AND METHODS
The study was a cross-sectional descriptive survey of road traffic workers in January 2008. The participants included road traffic policemen who have been on the job for at least a year and age and sex-matched residential students in Akoka campus of the University of Lagos. These students were assumed to be less exposed to traffic pollutions as they live in a university campus environment, which has a relatively low vehicular traffic. Eligible, accessible and willing participants were included in the sample.
A modified British Medical Research Council (MRC) questionnaire was used to obtain relevant details including history of respiratory symptoms and disease, demographic and socio-economic details from all the participants (the exposed and non-exposed group) on-site at the study locations.
All the participants underwent a lung function (spirometry) test. The forced expiratory volume in one second (FEV1), and forced vital capacity (FVC) were measured with a standard portable Spirometer (Micro lab. UK ML3500, 2005). The peak expiratory flow was assessed using a mini Wright peak flow meter. A minimum of three and a maximum of eight spirometry manoeuvres were done.15 The best three acceptable and reproducible manoeuvres (within 200 ml) were recorded for each patient. The reference equation for the spirometry was derived from the African American norms of the third National Health and Nutrition Examination Survey (NHANES III).16
The CO in subjects’ breath was analysed using a CO Breathe Analyser. The device measures the amount of CO in exhaled air, in parts per million (ppm)
Height was measured without shoes to the nearest centimetre using a wall-mounted stadiometer while weight was measured without outer garment to the nearest 0.1 kg using a portable weight scale after zero calibration check.
Data analysis
Data were analysed using the Stata 11.2.17 Continuous variables like the spirometry indices were expressed as means and standard deviations while discrete variables like the presence of respiratory symptoms were expressed as frequencies and proportions. Students t-test was used in analysing continuous variables while the Pearson's chi-square test was used for analysing categorical variables.
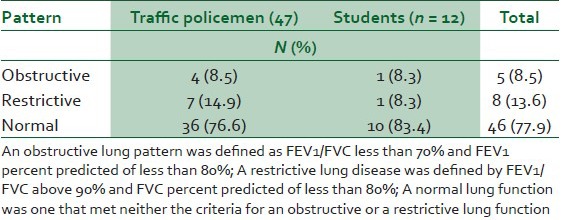
An obstructive lung function was defined by FEV1/FVC less than 70% and FEV1 percent predicted of less than 80%. A restrictive lung disease was defined by FEV1/FVC above 90% and FVC percent predicted of less than 80%. Other ventilatory functions that did not meet either of these criteria were regarded as normal.18 Statistical significance was considered at P value of < 0.05.
RESULTS
Out of 95 persons approached to be part of this survey, 59 individuals accepted to participate and provided complete data. Among these were 47 traffic policemen and 12 students who acted as controls. The mean age (SD) was 35.1 (8.0) and 35.4 years (6.3) for the traffic workers and students, respectively [Table 1]. The mean (SD) duration of occupation as a traffic policeman was 4.4 (4.4) and a median of 4 years (range 1-25). There was no significant difference in the height, age or body mass index of the traffic policemen and students who participated in the study. Table 2 shows the prevalence of symptoms between the traffic workers and students. There was no significant difference in the presentation of respiratory and non-respiratory symptoms between the two groups. Compared with the students, the traffic workers had higher age, height and sex adjusted forced expiratory volume in one second and FVC [Table 3]. In addition, the traffic policemen had significantly higher levels of exhaled CO than the students (1.18 vs 0.73 ppm P < 0.006). Out of the 47 policemen who provided spirometry data, 7 (14.9%) had a restrictive lung function while 4 (8.5%) had an obstructive lung function data [Table 4].
Table 1.
General characteristics of the study sample BMI- Body Mass index
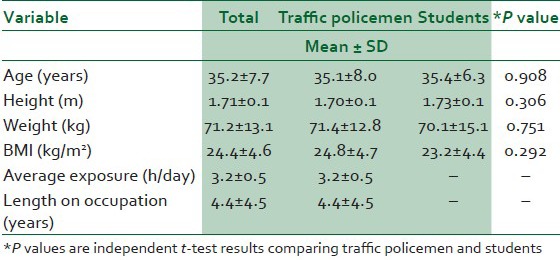
Table 2.
Self-reported respiratory symptoms among traffic policemen and students
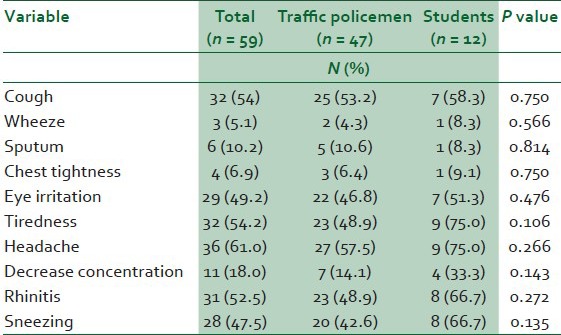
Table 3.
Lung function of traffic workers and students
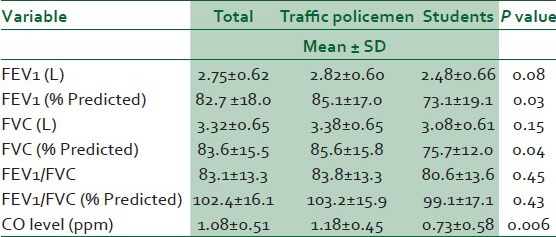
Table 4.
Patterns of lung function among the respondents
DISCUSSION
Our study showed that there is a general high prevalence of respiratory symptoms among the respondents in both groups, suggesting a widespread increased level of respiratory morbidity in Lagos metropolis. In addition, we observed paradoxically, higher FEV1 and FVC among traffic workers compared with the students.
Our study is a pilot survey of traffic policemen in Lagos who are exposed continuously to environmental pollutants especially traffic related air pollutants while they control and maintain the smooth flow of traffic in the metropolis.
We did not observe notable differences in the prevalence of respiratory and non-respiratory symptoms between the traffic policemen and the students. This observation can be viewed in various ways. It may suggest that the study was not powered enough to detect this effect because of the small sample. It could be due to inadvertent and inherent misclassification between the traffic workers and students due to unmeasured residual exposures in the students from sources other than traffic pollution. Alternatively it probably and more likely could indicate that there is a general high level of pollution in the metropolis, which impacts on both traffic workers and ordinary people in the society. Though the present study did not obtain PM data in the city, high levels of pollution have been reported in previous environmental studies in Lagos. In a study that assessed levels of particulate pollution in Lagos metropolis and elemental pollutants using laboratory analysis of leaf samples along major traffic corridors and control points over a period of 2 years, the authors found that the levels of total suspended PM, sulphur dioxide and ozone were far above the World Health Organisation (WHO's) Air Quality Standard (AQS). The key independent predictors of air pollution were traffic density, air temperature and land-use.8
In 2008, Efe et al., reported that the mean annual ambient PM of 10 µg or less (PM10) in over 70% of Nigerian cities was over 120 µg/m3 as against the WHO threshold of 70 µg/m3.19
These high particulates pollutions may be important predictive factors of the health condition and burden of respiratory illnesses in the general population.
We also found significantly higher level of exhaled CO in the traffic policemen compared with students. Similar observations have been found in other studies in developing countries, which assessed personal, in-vehicle and ambient levels of CO.20,21,22,23 There are daily and seasonal variations in ambient CO concentrations, in-vehicle and personal exposures.20 CO levels are also influenced by such factors like traffic congestion, density and meteorological conditions. CO is highly soluble and are easily absorbed in the blood to form carboxyhaemoglobin. Blood CO levels even at low concentrations can decrease exercise time to angina, increase the risk of arrhythmias, lead to difficulty in visual perception and negatively affect mental ability, dexterity, attention and concentration.20,24 These effects, however, were not assessed in the present pilot study.
Interestingly, we also found that the traffic workers had higher lung function values (FEV1% and FVC %) than the students [Table 3], though 15% of them had an obstructive lung function pattern [Table 4]. This could be an indication of a sampling limitation especially in the selection of the students or a ‘healthy worker’ phenomenon; implying the vulnerable workers may have been retired, off duty or screened out during pre-employment assessments leading to inadvertent selection of only those with better lung function. However, in the absence of pre-employment lung function records, it is difficult to provide the best interpretation of this observation. In the same vein, we place less emphasis on the lung function pattern because this pilot study is limited by its small sample size and few controls. Large environmental health impact studies are needed in many developing African cities to inform policy. In addition, this study did not assess blood levels of lead, volatile aromatic hydrocarbons or the amount of CO and other pollutants attributable to vehicular emissions. We did not assess the pre-morbid health and lung function of the participants or the levels of indoor pollutants participants may be exposed to at home through use of biomass fuels for cooking or heating. As such, there may be confounding of this result. Notwithstanding, the present survey adds to the body of literature available in this scarcely researched topic and stimulates the need for a more elaborate research on the health impact of environmental and outdoor pollution in Nigeria and other developing countries in Africa.
Our study highlights the need for health policy makers to undertake health risk assessments of the impacts of urbanisation and industrialisation of major cities in Nigeria and the African continent. It is important to critically assess the associated health effects on the populace and develop adequate strategies to mitigate them.
In conclusion, we found widespread high levels of respiratory and non-respiratory symptoms among the traffic and non-traffic workers in Lagos metropolitan area and significantly higher levels of exhaled CO among the traffic workers.
ACKNOWLEDGEMENT
The authors wish to express their gratitude to all who participated in this study and to the departmental support staff.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Dockery DW, Pope CA, 3rd, Xu X, Spengler JD, Ware JH, Fay ME, et al. An association between air pollution and mortality in six US cities. N Engl J Med. 1993;329:1753–9. doi: 10.1056/NEJM199312093292401. [DOI] [PubMed] [Google Scholar]
- 2.Pope CA, 3rd, Thun MJ, Namboodiri MM, Dockery DW, Evans JS, Speizer FE, et al. Particulate air pollution as a predictor of mortality in a prospective study of U.S adults. Am J Respir Crit Care Med. 1995;151:669–74. doi: 10.1164/ajrccm/151.3_Pt_1.669. [DOI] [PubMed] [Google Scholar]
- 3.Pope CA, 3rd, Burnett RT, Thun MJ, Calle EE, Krewski D, Ito K, et al. Lung cancer, cardiopulmonary mortality, and long-term exposure to fine particulate air pollution. JAMA. 2002;287:1132–41. doi: 10.1001/jama.287.9.1132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Hoek G, Brunekreef B, Goldbohm S, Fischer P, van den Brandt PA. Association between mortality and indicators of traffic-related air pollution in the Netherlands: A cohort study. Lancet. 2002;360:1203–9. doi: 10.1016/S0140-6736(02)11280-3. [DOI] [PubMed] [Google Scholar]
- 5.Yaduma N, Kortelainen M, Wossink A. Estimating mortality and economic costs of particulate air pollution in developing countries: The case of Nigeria. (361-87).Environ Resour Econ. 2013:54–3. [Google Scholar]
- 6.Han X, Naeher LP. A review of traffic-related air pollution exposure assessment studies in the developing world. Environ Int. 2006;32:106–20. doi: 10.1016/j.envint.2005.05.020. [DOI] [PubMed] [Google Scholar]
- 7.Bruce N, Perez-Padilla R, Albalak R. Indoor air pollution in developing countries: A major environmental and public health challenge. Bull World Health Organ. 2000;78:1078–92. [PMC free article] [PubMed] [Google Scholar]
- 8.Akanni CO. Spatial and seasonal analysis of traffic-related pollutant concentrations in lagos metropolis, Nigeria. Afr J Agric Res. 2010;5:1264–72. [Google Scholar]
- 9.Efe S, Efe A. Spatial distribution of particulate matter (PM10) in warri metropolis, Nigeria. Environmentalist. 2008;28:385–94. [Google Scholar]
- 10.Ndoke P, Jimoh O. Impact of traffic emission on air quality in a developing city of Nigeria. Assumpt Univ J Technol. 2005;4:222–7. [Google Scholar]
- 11.Africa environment outlook 3 — authors guide | GRID-arendal - publications — AEO 3 [Internet] [Last accessed on 2013 Sep 7]. Available from: http://www.grida.no/publications/aeo3/
- 12.The state of African cities 2010: Governance, inequalities and urban land market. [Last accessed 2013 Jul 31]. Available from: http://www.google.com.ng/search?site=&source=hp&q=The+State+of+African+Cities+2010:+Governance,+Inequalities+and+Urban+Land+Market,&btnK=Google+Find .
- 13.Petkova EP, Jack DW, Volavka-Close NH, Kinney PL. Particulate matter pollution in african cities. Air Qual Atmos Health. 2013:1–12. [Google Scholar]
- 14.Ekpenyong CE, Ettebong EO, Akpan EE, Samson TK, Daniel NE. Urban city transportation mode and respiratory health effect of air pollution: A cross-sectional study among transit and non-transit workers in Nigeria. BMJ Open. 2012;2 doi: 10.1136/bmjopen-2012-001253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Miller MR, Hankinson J, Brusasco V, Burgos F, Casaburi R, Coates A, et al. ATS/ERS Task Force. Standardisation of spirometry. Eur Respir J. 2005;26:319–38. doi: 10.1183/09031936.05.00034805. [DOI] [PubMed] [Google Scholar]
- 16.Hankinson JL, Odencrantz JR, Fedan KB. Spirometric reference values from a sample of the general US population. Am J Respir Crit Care Med. 1999;159:179–87. doi: 10.1164/ajrccm.159.1.9712108. [DOI] [PubMed] [Google Scholar]
- 17.StataCorp L. College Station, TX: StataCorp LP; 2009. Stata version 11.0. [Google Scholar]
- 18.GOLD - the global initiative for chronic obstructive lung disease [Internet] [Last cited on 2013 May 29]. Available from: http://www.goldcopd.org/guidelines-global-strategy-for-diagnosis-management.html .
- 19.Home J. Spatial distribution of particulate air pollution in Nigerian cities: Implications for human health. Geography. 2008;7 [Google Scholar]
- 20.Atimtay AT, Emri S, Bagci T, Demir AU. Urban CO exposure and its health effects on traffic policemen in Ankara. Environ Res. 2000;82:222–30. doi: 10.1006/enrs.1999.4031. [DOI] [PubMed] [Google Scholar]
- 21.Chan L, Lau W, Zou S, Cao Z, Lai S. Exposure level of carbon monoxide and respirable suspended particulate in public transportation modes while commuting in urban area of guangzhou, China. Atmos Environ. 2002;36:5831–40. [Google Scholar]
- 22.Shendell DG, Naeher LP. A pilot study to assess ground-level ambient air concentrations of fine particles and carbon monoxide in urban guatemala. Environ Int. 2002;28:375–82. doi: 10.1016/s0160-4120(02)00057-0. [DOI] [PubMed] [Google Scholar]
- 23.Gomez-Perales J, Colvile R, Nieuwenhuijsen M, Fernandez-Bremauntz A, Gutierrez-Avedoy V, Paramo-Figueroa V, et al. Commuters’ exposure to PM <sub> 2.5</sub>, CO, and benzene in public transport in the metropolitan area of mexico city. Atmos Environ. 2004;38:1219–29. [Google Scholar]
- 24.Marshall MD, Kales SN, Christiani DC, Goldman RH. Are reference intervals for carboxyhemoglobin appropriate? A survey of Boston area laboratories. Clin Chem. 1995;41:1434–8. [PubMed] [Google Scholar]