

Abstract
Background:
This study aims to investigate the effect of antioxidants supplement on clinical outcomes and antioxidant parameters in rheumatoid arthritis (RA).
Methods:
The pre-post study was conducted on 40 female patients with RA in 12 weeks that taken daily one Selenplus capsule contained 50 μg selenium, 8 mg zinc, 400 μg vitamin A, 125 mg vitamin C, and 40 mg vitamin E. About 5 mL venous blood sample was taken from all participants and disease activity score (DAS) was determined by DAS-28 formula and high-sensitive C-reactive protein (hs-CRP). Glutathione peroxidase (GPX) and superoxide dismutase (SOD) were measured by spectrophotometric kit and catalase (CAT) was measured by Abei method. Total antioxidant capacity (TAC) was determined by spectrophotometric kit. Distribution of the variables was assessed using histogram with normal curve as well as Kolmogorov-Smirnov test and data were analyzed with paired t-test for differences between pre-post data using SPSS software version 13.5.
Conclusions:
Our findings showed that antioxidants may improve disease activity significantly, but it did not affect the number of painful and swollen joints and increased erythrocyte antioxidant levels. Antioxidants may be useful for controlling of clinical outcomes and oxidative stress in RA.
Keywords: Antioxidants, dietary supplements, nutrition, oxidative stress, rheumatoid arthritis
INTRODUCTION
Rheumatoid arthritis (RA) is a chronic systemic autoimmune disease that about 0.5%-1% of world population are affected by its complaints.[1] The prevalence of RA in females is 3 times higher than males. The RA affects blood vessels, heart, lungs, muscles, and joints, resulting in bone deformity and osteoporosis.[2]
Several studies have reported that oxidative stress and production of oxygen-free radicals have important role in RA development[3,4] and epidemiologic studies have revealed a reverse relationship between dietary intake of antioxidants and RA incidence[5,6] and due to reduction of intake and absorption of dietary antioxidants in RA patients, the levels of blood antioxidants are decreased too. The antioxidants supplements such as vitamin E,[7,8] vitamin C,[4,9] and selenium[10,11] may control the disturbance of lipid peroxidation and loss of antioxidants markers in patients with RA. Vitamin E can interact with nitric oxide and may trigger the gene expression of catalase (CAT), glutathione peroxidase (GPX), and superoxide dismutase (SOD) enzymes,[12] vitamin C may demolish the peroxides of macrophage activities, zinc may strengthen the immune system,[13] and selenium has an important role as a cofactor of GPX enzyme in reduction of oxidative stress.[14]
In past 30 years, controlled trials have conducted to compare the effect of dietary antioxidants and antioxidant-rich diets in controlling of RA clinical outcomes;[15,16] however, they could not find a clear statement about antioxidants in RA prevention and treatment due to difference in study period, dose, and different types of antioxidants.[12] Regarding to integrity of antioxidant defense system and few clinical studies on combined antioxidant supplements in RA, the aim of this study is to evaluate the effect of combined antioxidant supplements as daily oral capsule on clinical outcomes and antioxidant parameters in female patients with RA for 3 months.
METHODS
Study design and patients
A pre-post clinical trial was conducted on female patients with RA for 12 weeks. The study group was selected from 400 registered RA patients in Sheikh-al-Rais and Sina clinics of Tabriz University of medical sciences, Iran according to inclusion criteria. The inclusion criteria were RA diagnosis by rheumatologist according to American College of Rheumatology guidelines-1987, 40-60 years old, no change in treatment approach in past 2 months. The exclusion criteria were diabetes mellitus, hypertension, thyroid disorders, liver and kidney failure, Cushing syndrome, severe infection, gastric illnesses, smoking, and exposure to daily smoking at home. We followed-up the intake of daily supplement use and type and dose of medications by regular phone calls, so change in type and dose of drugs and antioxidant supplement resulted in omission from study.
We asked from selected patients to take daily a “selenplus” capsule (Eurovital pharmaceutical company, Germany) that contained 50 μg selenium, 8 mg zinc, 400 μg vitamin A, 125 mg vitamin C, and 40 mg vitamin E. The supplement has been given to patients without trading label. After explanation of the study risks and benefits, written consent form was taken from all subjects. Registration code of the local ethics committee of Tabriz University of Medical Sciences is 8912 and registration number in the registration center for clinical trials in Iran is IRCT138901183655N1. In the case of any side effects, patients could leave the study and dose of each antioxidant nutrient was at the Recommended Dietary Allowances amount.
Procedure
At the beginning of the study, accurate clinical examination such as counting the swollen and painful joints was done by a rheumatologist and the validated DAS-28 form was filled to calculate disease activity index[17] according to following formula.[18]:

TYC28: Number of painful joints, SYC28: Number of swollen joints, Sqrt: Square, Ln: loge
Also, dietary intake questionnaire including food frequency questionnaire (FFQ) and 24 h recall questionnaire for 3 days (2 working days and 1 weekend) were completed by an expert nutritionist. The FFQ was composed of 168 food items that assessed the frequency of the intake in day, month, season, and year semiquantitavely. The recall questionnaire was a dietary detailed form in 6 parts: Breakfast, lunch, and dinner with three snacks that filled by face to face interview about the type and amount of the food items. Dietary intake of energy, macronutrients, and antioxidant micronutrients analyzed by nutritionist III software (MAM soft research Co, USA 1993). The weight of patients was measured by digital scale (after calibration and without shoes), the height was measured by stadiometer (after attachment of 4 points of body to the wall) and the body mass index calculated by Quetelet formula. The patients were followed-up every 2 weeks by phone calls and the measurements were repeated after 3 months.
Five milliliter fasting venous blood samples (8-12 h after fasting) were taken from all participants and were kept in -70°C freezer (Snider's, Germany) until conducting biochemical measurements. Biochemical measurements including GPX and SOD were measured by spectrophotometric kit (Ransel, Randox laboratories ltd, UK) and autoanalyzer apparatus (Abbott, model Alcyon 300, USA) and CAT was measured by Abei method.[19] TAC was determined by spectrophotometric kit (Randox TAC kit, Randox laboratories Ltd, UK). Serum high-sensitive C-reactive protein (hs-CRP) was quantified by photometric kit (Pars Azmoon Company Ltd, Iran).
Statistical analysis
SPSS software version 13 (SPSS for windows, Chicago, IL, USA) was used for statistical analysis. Distribution of data was tested by Q-Q plot and Kolmogorov-Smirnov test. For parametric data, paired t-test and in case of nonparametric data, Wilcoxon signed rank test was used. The linear regression model was used for adjusting confounding factors such as dietary intake of some selected nutrients. P < 0.05 was defined significant.
RESULTS
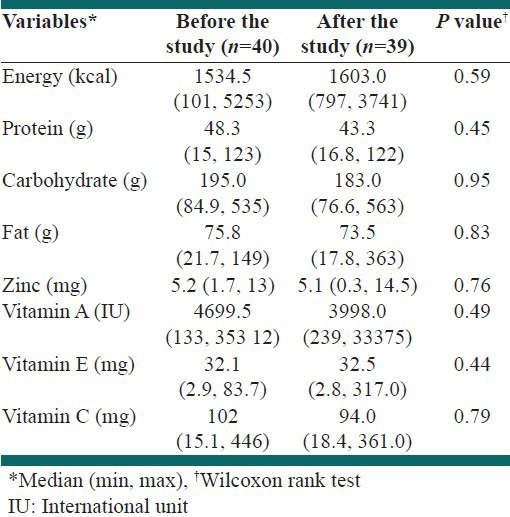
A total of 39 patients sustained in the study after 12 weeks. The baseline characteristics and dietary intake have been reported in reference no. 20.[20] One was left in reason of unrelated medical problem. Table 1 indicates basic characteristics of the subjects at the start point of trial and the median of the duration of the disease was 72 months [Table 1]. The pharmacotherapy regimen did not change during the period of the study in the selected patients and any changes in the dose and type of the drugs resulted in the omission of the study. Dietary intake of energy and selected nutrients during 12 weeks of intervention did not differ significantly [Table 2] and in the linear regression findings, no significant linear relationship between dietary antioxidants values with biochemical indices was observed.
Table 1.
The basic characteristics of subjects in the study
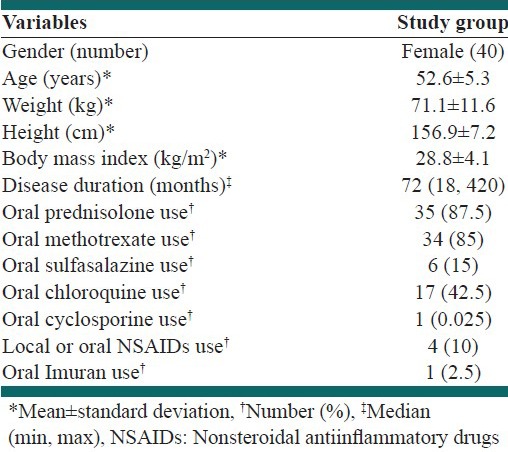
Table 2.
Dietary intake of selected nutrients before and after 12 weeks intervention
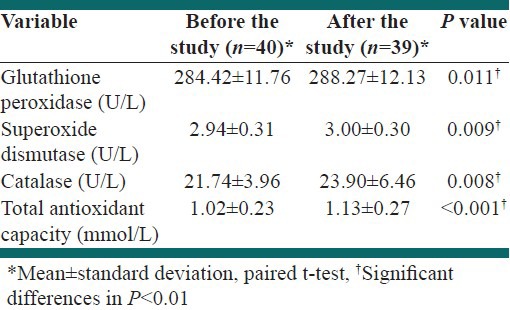
In our study, DAS-28 score and serum hs-CRP have changed during 12 weeks of intervention (P < 0.01), while the number of swollen and painful joints did not change significantly [Table 3]. The antioxidant markers of patients including TAC, GPX, SOD, and CAT increased significantly after 12 weeks supplementation (P < 0.01) [Table 4].
Table 3.
The changes of clinical outcomes in subjects of study before and after 12 weeks intervention
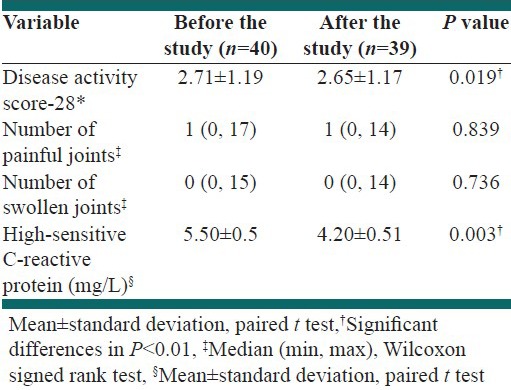
Table 4.
The changes of erythrocyte antioxidant parameters in subjects of study before and after 12 weeks intervention
DISCUSSION
In our study, antioxidants supplement for 12 weeks reduced significantly serum hs-CRP and DAS-28 score. The literature review indicates that zinc and selenium supplementation have been used in RA remission and prevention for several years[21] and the similar results of these studies were resulted from multicomponent antioxidants and nutrients as Koracevic et al.,[22] showed concurrent supplementation with 37.5 mg vitamin E, 150 mg vitamin C, 1.4 g eicosapentaenoic acid, 0.2 g docosaenoic acid, and 0.5 g gamma linolenic acid could not significantly reduce the number of swollen and painful joints.[22] As the results of alike studies revealed intake of simultaneous antioxidant micronutrients can have a helpful effect against RA progress.[22] In another similar study, 300 mg vitamin C, 5 mg zinc, 25000 International Unit vitamin A for 12 weeks reduced the disease activity (P < 0.0001).[23] Also, Pretez et al.,[10] study showed that 12 weeks selenium supplementation decreased the number of swollen and painful joints; however, the results were not statistically significant. Some studies have used higher doses of one antioxidant although they did not observe significant improvement in clinical outcomes.[24] It seems that the reason of these findings is due to no increase in antioxidants levels in polymorphonuclear leukocytes and antioxidant defense system in blood cells.[25] As Onal et al.,[26] study indicated the pharmacotherapy in patients with RA results in lower levels of zinc and selenium and higher levels of copper in red blood cells, so intake of oral drugs such as corticosteroids and chloroquine elevates the required amount of the antioxidants to suppress inflammatory-like substances.
In our study, erythrocyte antioxidant markers including TAC, GPX, SOD, and CAT increased significantly during 12 weeks supplementation due to probable direct effect of oral antioxidants on antioxidants levels. Similarly, Shinde et al.,[27] have shown that 400 mg vitamin E and 500 mg vitamin C could increase the reduced form of erythrocyte glutathione (P < 0.001), probably because vitamin E is the most important fat-soluble antioxidant and protects the cell membranes against oxidative stress just as vitamin C preserves cytosol and membranes of free radicals activity.[28] Furthermore, the results of VanVugt et al.,[29] study indicated that 400 mg alpha-tocopherol, 10 mg lycopene, 5 mg alpha carotene, 10 mg lutein, and 200 mg vitamin C for 12 weeks increased plasma levels of vitamin E, lycopene, lutein, alpha-carotene, and vitamin C and reduced F2-isoprstanes as the oxidative stress marker. Shah et al.,[30] illustrated that there is a strong association among the disease activity with antioxidant enzymes markers and they have showed that production of reactive oxygen substances can disturb the immune defense system and modulate inflammation processes to reduce the antioxidant molecules in blood cells. It seems that mixture of antioxidants help to reduce required dose of pain killer drugs and diminish the complaints of disease.
Since autoimmune diseases such as RA are accompanying with reduction of cellular immune level that results in high coincidence of other chronic diseases, healthy antioxidant-rich diet can improve immune system and compensate the inadequate intake of micronutrients, especially antioxidant-rich supplies of RA patients in northwest of Iran.[27,28] Also, consumption of antioxidant micronutrients in the form of dietary items or supplements may be helpful in enhancement of enzymatic and nonenzymatic antioxidants due to strengthen the antioxidant defense system of the body.[29,30] Lack of the control group is the major limitation in this pre-post clinical trial due to limited financial support. One of the strengths is the high response rate of participants (97.5%) and low loss to follow-up during the intervention. Also, mild to moderate severity of RA was considered as a criterion of the study and the dietary intake of antioxidants was supposed as confounding factors.
CONCLUSIONS
The combined antioxidant supplement may improve DAS-28 score significantly, but it did not change the number of painful and swollen joints statistically significant during 12 weeks, while it could increase TAC, GPX, SOD, and CAT levels. It seems that supplementation with antioxidants may be useful as a complementary treatment in control of clinical outcomes and oxidative stress in patients with RA.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
REFERENCES
- 1.Gill TM, Feinstein AR. A critical appraisal of quality of life measurement. JAMA. 1995;272:619–29. [PubMed] [Google Scholar]
- 2.Westaway MS, Rheeder P, Guloba G. Rheumatoid arthritis functional disability in a public health care clinic. S Afr Med J. 2008;98:706. [PubMed] [Google Scholar]
- 3.Karatas F, Ozates I, Canatan H, Halifeogly I, Karatepe M, Colak R. Antioxidant status and lipid peroxidation in patients with rheumatoid arthritis. Indian J Med Res. 2003;118:178–81. [PubMed] [Google Scholar]
- 4.Pattison DJ, Silman AJ, Goodson NJ, et al. Vitamin C and the risk of developing inflammatory polyarthritis: Prospective nested case-control study. Ann Rheum Dis. 2004;63:843–7. doi: 10.1136/ard.2003.016097. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Rennie KL, Hughes J, Lang R, Jebb SA. Nutritional management of rheumatoid arthritis: A review of the evidence. J Hum Nutr Diet. 2003;16:97–109. doi: 10.1046/j.1365-277x.2003.00423.x. [DOI] [PubMed] [Google Scholar]
- 6.El-barbary AM, Khalek MAA, Elsalawy AM, Hazaa SM. Assessment of lipid peroxidation and antioxidant status in rheumatoid arthritis and osteoarthritis patients. The Egyptian Rheumatologist. 2011;33:179–85. [Google Scholar]
- 7.Helmy M, Shahayeb M, Helmy MH, El-Bassiouni EA. Antioxidants as adjuvant therapy in rheumatoid disease: A preliminary study. Arzneimittelforschung. 2001;51:293–8. doi: 10.1055/s-0031-1300040. Abs. [DOI] [PubMed] [Google Scholar]
- 8.Karlson EW, Shadick NA, Cook NR, Buring JE, Lee IM. Vitamin E in the primary prevention of rheumatoid arthritis: The Women's Health Study. Arthritis and rheumatism. 2008;59:1589–95. doi: 10.1002/art.24194. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Meki AR, Hamed EA, Ezam KA. Effect of green tea extract and vitamin C on oxidant or antioxidant status of rheumatoid arthritis rat model. Indian journal of clinical biochemistry: IJCB. 2009;24:280–7. doi: 10.1007/s12291-009-0053-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Pretez A, Siderova V, Neve J. Selenium supplementation in rheumatoid arthritis investigated in a double blind, placebo-controlled trial. Scand J Rheumatol. 2001;30:208–12. doi: 10.1080/030097401316909549. [DOI] [PubMed] [Google Scholar]
- 11.Vieira AT, Silveira KD, Arruda MC, et al. Treatment with Selemax (R), a selenium-enriched yeast, ameliorates experimental arthritis in rats and mice. The British journal of nutrition. 2012;108:1829–38. doi: 10.1017/S0007114512000013. [DOI] [PubMed] [Google Scholar]
- 12.Evans P, Halliwell B. Micronutrients: Oxidant/antioxidant status. The British journal of nutrition. 2001;85:67–74. [PubMed] [Google Scholar]
- 13.Cerhan J, Saag K, Merlino L, Mikuls T, Criswell L. Anti-oxidant micronutrients and risk of rheumatoid arthritis in a cohort of older women. American journal of epidemiology. 2003;157:345–54. doi: 10.1093/aje/kwf205. [DOI] [PubMed] [Google Scholar]
- 14.Canter PH, Wider B, Ernst E. The antioxidant vitamins A, C, E and selenium in the treatment of arthritis: A systematic review of randomized clinical trials. Rheumatology. 2007;116:1–11. doi: 10.1093/rheumatology/kem116. [DOI] [PubMed] [Google Scholar]
- 15.Martin HR. The role of nutrition and diet in rheumatoid arthritis. Proc Nutr Soc. 2004;63:137–43. doi: 10.1079/pns19980036. [DOI] [PubMed] [Google Scholar]
- 16.Hagfors L, Leanderson P, Skoldstam L, Andersson J, Johansson G. Antioxidant intake, plasma antioxidants and oxidative stress in a randomized, controlled, parallel, Mediterranean dietary intervention study on patients with rheumatoid arthritis. Nutrition journal. 2003;2:5. doi: 10.1186/1475-2891-2-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Sarban S, Kocyigi A, Yazar M, Isikan UE. Plasma total antioxidant capacity, lipid peroxidation, and erythrocyte antioxidant enzyme activities in patients with rheumatoid arthritis and osteoarthritis. Clinical biochemistry. 2005;38:981–6. doi: 10.1016/j.clinbiochem.2005.08.003. [DOI] [PubMed] [Google Scholar]
- 18.DAS-score.nl. 2009. [Accessed february 2010]. http://www.das-score.nl/www.das.score.nl: ref/index.html .
- 19.Aebi HE. Derfield Beach: Verlag Chemie; 1980. Enzymes 1: Oxidoreductases, transferases. [Google Scholar]
- 20.Jalili M, Hosseini S-RA, Kolahi S, Ebrahimi-Mamegani M, Sabour S. The Effect of Antioxidants Supplement on Lipid Peroxidation and Serum Aryl Esterase Enzyme in Rheumatoid Arthritis Patients. American Medical Journal. 2011;2:119–24. [Google Scholar]
- 21.Drafi F, Bauerova K, Kuncirova V, et al. Pharmacological influence on processes of adjuvant arthritis: Effect of the combination of an antioxidant active substance with methotrexate. Interdisciplinary toxicology. 2012;5:84–91. doi: 10.2478/v10102-012-0015-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Koracevic D, Koracevic G, Djordjevic V. Method for the measurement of antioxidant activity in human. J Clin Pathol. 2001;54:356–61. doi: 10.1136/jcp.54.5.356. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Nourmohammadi I, Athari-Nikazm S, Vafa MR, et al. Effects of antioxidant supplements on oxidative stress in rheumatoid arthritis patients. J Biol Sci. 2010:1–3. [Google Scholar]
- 24.Springer D. Rheumatoid arthritis: Pain Suppresion effect of vitamin E versus analgestics. Natura Med. 1998;13:30–2. [Google Scholar]
- 25.Tarp U, Stengaard-Pederson K, Hansen JC, Thorling EB. Glutathione redox cycle enzymes and selenium in severe rheumatoid arthritis: Lack of antioxidative response to selenium supplementation in polymorphonuclear leucocytes. Ann Rheum Dis. 1992;51:1044–9. doi: 10.1136/ard.51.9.1044. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Sang-Cheol B, Won-Jin J, Eun-Ju L, Rina Y, Mi-kyung S. Effects of antioxidant supplements intervention on the level of plasma inflammatory molecules and disease severity od rheumatoid arthritis patients. Am Coll Nutr. 2009;28:56–62. doi: 10.1080/07315724.2009.10719762. [DOI] [PubMed] [Google Scholar]
- 27.Bae SC, Kim SJ, Sung MK. Inadequate antioxidant nutrient intake and altered plasma antioxidant status of rheumatoid arthritis patients. Journal of the American College of Nutrition. 2003;22:311–5. doi: 10.1080/07315724.2003.10719309. [DOI] [PubMed] [Google Scholar]
- 28.Hejazi J, Mohtadinia J, Kolahi S, Bakhtiyari M, Delpisheh A. Nutritional status of Iranian women with rheumatoid arthritis: An assessment of dietary intake and disease activity. Women's health (London, England) 2011;7:599–605. doi: 10.2217/whe.11.41. [DOI] [PubMed] [Google Scholar]
- 29.Staron A, Makosa G, Koter-Michalak M. Oxidative stress in erythrocytes from patients with rheumatoid arthritis. Rheumatology international. 2012;32:331–4. doi: 10.1007/s00296-010-1611-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Al-Okbi SY. Nutraceuticals of anti-inflammatory activity as complementary therapy for rheumatoid arthritis. Toxicology and industrial health. 2012 doi: 10.1177/0748233712462468. [DOI] [PubMed] [Google Scholar]