

Abstract
Background:
Contrast-induced acute kidney injury [contrast-induced nephropathy (CIN)] is one of the major causes of hospital-acquired acute renal failure. Volume supplementation is the most effective strategy to prevent acute renal failure caused by contrast; but the effects of sodium bicarbonate regimens are unknown in CIN prevention. The aim of this survey is to compare the efficacy of hydration with normal saline versus hydration with sodium bicarbonate in the prevention of the CIN in patients undergoing coronary angiography.
Materials and Methods:
In a clinical trial, 350 patients undergoing coronary interventions were randomized into two groups: One group received normal saline and another group received sodium bicarbonate before and after infusion of the contrast. Patients in both the groups had received N-acetylcysteine. CIN was defined as relative increase in serum creatinine equal to or more than 25% of baseline or increase to 0.5 mg/dl in 48 h after the injection of the contrast.
Results:
CIN was seen in 46 patients (13.1%) after coronary interventions. Incidence of CIN in patients receiving normal saline (19.4%) was more than in patients receiving sodium bicarbonate (6.9%) (P = 0.001). Hemodialysis was needed only in one patient who received saline normal. Relative risk to induce CIN in both groups was as 2.8 and was in the range of 1.50-5.25 with confidence interval of 95% and P = 0.001. Thus, the probability of CIN was significantly more in the usage of normal saline.
Conclusion:
This survey showed that hydration with sodium bicarbonate is superior to hydration with normal saline and has better protection effects.
Keywords: Contrast, nephropathy, sodium bicarbonate
INTRODUCTION
The rising usage of radiological procedures has resulted in an increasing incidence of procedure-related contrast-induced nephropathy (CIN).[1,2] The incidence from different studies varies significantly.[3,4]
Volume supplementation and dehydration treatment are the ways of preventing CIN.
However, there are limited data on the best choice for intravenous fluid supplementation. Evidence indicate that isotonic crystalloids such as normal saline and sodium bicarbonate are more effective than half saline.[5] The medical literature varies in the effects of sodium bicarbonate in preventing CIN.[4,6]
The primary aim of this survey was to compare the efficacy of hydration with normal saline versus hydration with sodium bicarbonate in the prevention of CIN, considering urea, creatinine, and glomerular filtration rate (GFR) before the procedure and 48 h after the percutaneous coronary intervention (PCI), among the patients undergoing coronary angiography.
MATERIALS AND METHODS
Between 19 March 2010 and 22 June 2010, 350 patients who underwent coronary interventions entered the clinical trial in Madani Heart Hospital, Tabriz, Iran.
The exclusion criteria were cardiogenic shock, recent exposure to radiographic media, serum creatinine (SCr) level above 4 mg/dl, and patients with pre-existing end-stage renal disease requiring dialysis. Eligible patients randomly received one of the hydration protocols.
Coronary angiography through the femoral artery was performed by the standard techniques.
All radiological procedures were done with non-ionic low-osmolar Omnipaque 300.
All the patients received a fixed dose of fluid 6 h before the procedure and 6 h after it.
Sodium bicarbonate solution was prepared by adding 154 ml of 1000 mEq/l sodium bicarbonate to 846 ml of 5% dextrose with water. Both groups had received 1200 mg N-acetylcysteine the day before and also on the angiography day. Before the intervention and 2 days after the injection of contrast, SCr level and blood urea nitrogen (BUN) level were measured, and creatinine clearance was estimated using the Cockcroft–Gault equation.
[(140−age) × weight (kg) × 0.85 (if female)]/72 × serum creatinine (mg/dl).
CIN was defined as an increase of ≥25% or 0.5 mg/dl in pre-procedure SCr at 48 h after the procedure.
Statistical analyses
The data were analyzed using SPSS16 software. Descriptive statistical analysis (frequency, percentage, mean ± SD) was used. Normal distribution of data was evaluated by Kolmogorov–Smirnov Test. Quantitative data, depending on the needs, were analyzed using Student's t-test or Mann–Whitney U test, and qualitative data were analyzed by Chi-square test (χ2) and, if needed, with Fisher exact test.
Using Medcalc software, relative risk (RR) was calculated for CIN. In this study, P < 0.05 were considered as significant.
RESULTS
In this survey, 350 patients were studied. The patients were divided randomly into two groups, those receiving normal saline (group A) and those receiving sodium bicarbonate (group B).
The mean age in group A was 64.48 ± 11.07 years and in group B was 64.96 ± 10.29 years (P = 0.67).
One hundred and eighty of the patients were males (51.4%) and 170 of the patients were females (48.6%). However, in group A, there were 104 males (59.4%) and 71 females (40.6%), while in group B, there were 76 males (43.4%) and 99 females (56.6%).
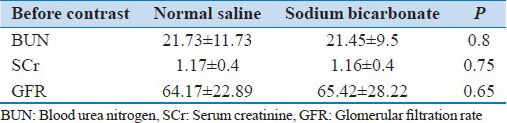
The mean BUN before the intervention in sodium bicarbonate group (group B) was 21.73 ± 11.73 mg/dl and in normal saline group (group A) was 21.45 ± 9.5 mg/dl (P = 0.8).
The SCr level in group A before the intervention was 1.17 ± 0.4 mg/dl and in group B it was 1.16 ± 0.4 mg/dl, with P = 0.75 [Table 1].
Table 1.
Renal indices before contrast injection in normal saline and sodium bicarbonate groups
There is significant difference in BUN, SCr, and GFR levels between the two groups, before and after [Table 2] the intervention [Table 3].
Table 2.
Renal function after the contrast has been compared in both groups considering BUN, SCr, and GFR
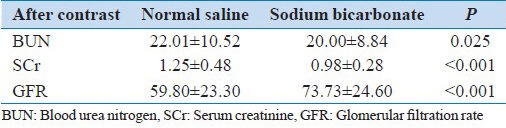
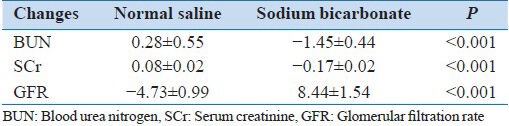
Table 3.
The measures of changes in renal function before and after the contrast
CIN was seen in 46 patients (13.1%) after the coronary interventions.
CIN was detected in 34 patients (19.4%) of normal saline receiving group (group A) and in 12 patients of bicarbonate receiving group (group B). As observed, the incidence of CIN was significantly higher in normal saline receiving patients (P = 0.001).
There were no major in-hospital events such as myocardial infarction (MI), stroke, and death due to heart problems in any of the patients.
The RR for CIN in both groups was 2.81 and was in the range of 1.50-5.25 with Confidence Interval (CI) = 95% (P = 0.001).
Due to the RR, the possibility of CIN was significantly higher in normal saline receiving patients.
DISCUSSION
The administration of radiocontrast media can give rise to a commonly reversible form of acute renal failure known as CIN that begins immediately after the contrast is administered.[5,6,7,8] Renal vasoconstriction resulting in medullary hypoxemia and direct cytotoxic effects of the contrast agents are the two major theories of the underlying mechanism of injury, though many strategies have been introduced to preserve renal function, which are mostly based on two general mechanisms: Preserving cell viability and preventing or reversing intratubular obstruction.
There are several limitations to investigating the prevention of post-ischemic acute tubular necrosis in humans. They include heterogeneous and complex patient factors (e.g., co-morbidities and concurrent multi-organ failure in critically ill patients), lack of a standardized definition of and diagnostic criteria for post-ischemic ATN, and the lack of clear and specific endpoints for clinical trials.[9,10] On the other hand, the optimal treatment or preventive regimen has not yet been introduced, making the necessity of such researches more overt in this regard.
Due to lack of convincing evidence of the potential risk of some approaches and given that the overall direction of the data is better to be toward beneficial, well-tolerated, and relatively inexpensive agents, we chose the administration of acetylcysteine, which must be accompanied by isotonic fluid hydration and use of a low or iso-osmolal contrast agent.[11,12,13]
The optimal hydration solution (isotonic saline, one-half isotonic saline, or isotonic sodium bicarbonate) for prevention of contrast nephropathy is unclear. Since alkalization may protect against free radical injury, the possibility that sodium bicarbonate may be superior to isotonic saline has been examined in a number of randomized trials and meta-analyses as ours. The results were conflicting as some showed a significantly lower rate of CIN with sodium bicarbonate,[14,15,16,17,18] while others found equivalent rates.[19,20,21]
The superiority of sodium bicarbonate regimen in our study was obvious in all the three evaluated parameters, suggesting it a safe and efficient protocol to be considered in patients receiving radiocontrast media. However, variations in outcomes with sodium bicarbonate may be due to the significant heterogeneity found in these studies. Several meta-analyses have noted differences due to wide variations in study size, treatment effect, and publication bias.[20,22,23] Yet, definition of contrast-induced acute renal failure, baseline risk for acute renal failure (e.g., severity of renal dysfunction and proportion with diabetes), acetylcysteine dose and route of administration (e.g., oral or intravenous), intravenous hydration protocols, amount and type of contrast given, and type of procedure performed (e.g., contrast CT, cardiac catheterization, or peripheral angiography) vary widely in such studies, which leads to substantial inconsistency in the reported results. However, in general, studies that have examined outcomes with isotonic sodium bicarbonate versus isotonic sodium chloride or normal saline have noted either equivalent or better outcomes with sodium bicarbonate than the other two, making it superior, as ours, to similar regimens.
The rational approach for further investigation would better be based upon more homogeneous and larger-sized studies to diminish the effect of statistical bias on related issues.
CONCLUSIONS
Results of this survey show that hydration with sodium bicarbonate has more protective effects in comparison to hydration with normal saline in the incidence of contrast-induced acute kidney injury.
ACKNOWLEDGMENTS
The authors would like to acknowledge the kind cooperation extended by Dr. Morteza Ghojazadeh, researcher of Tabriz University of Medical Science.
Footnotes
Source of Support: This study was founded by cardiovascular research center of Tabriz
Conflict of Interest: None declared.
REFERENCES
- 1.McCullough PA. Contrast-induced acute kidney injury. J Am Coll Cardiol. 2008;51:1419–28. doi: 10.1016/j.jacc.2007.12.035. [DOI] [PubMed] [Google Scholar]
- 2.Finn WF. The clinical and renal consequences of contrast-induced nephropathy. Nephrol Dial Transplant. 2006;21:i2–10. doi: 10.1093/ndt/gfl213. [DOI] [PubMed] [Google Scholar]
- 3.Iakovou I, Dangas D, Mehran R, Lansky AJ, Ashby DT, Fahy M, et al. Impact of gender on the incidence and outcome of contrast-induced nephropathy after percutaneous coronary intervention. J Invasive Cardiol. 2003;15:18–22. [PubMed] [Google Scholar]
- 4.From AM, Bartholmai BJ, Williams AW, Cha SS, Pflueger A, McDonald FS. Sodium bicarbonate is associated with an increased incidence of contrast nephropathy: A retrospective cohort study of 7977 patients at mayo clinic. Clin J Am Soc Nephrol. 2008;3:10–8. doi: 10.2215/CJN.03100707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Davidson CJ, Hlatky M, Morris KG, Pieper K, Skelton TN, Schwab SJ, et al. Cardiovascular and renal toxicity of a nonionic radiographic contrast agent after cardiac catheterization. A prospective trial. Ann Intern Med. 1989;110:119–24. doi: 10.7326/0003-4819-110-2-119. [DOI] [PubMed] [Google Scholar]
- 6.Hogan SE, L’Allier P, Chetcuti S, Grossman PM, Nallamothu BK, Duvernoy C, et al. Current role of sodium bicarbonate–based preprocedural hydration for the prevention of contrast-induced acute kidney injury: A meta-analysis. Am Heart J. 2008;156:414–21. doi: 10.1016/j.ahj.2008.05.014. [DOI] [PubMed] [Google Scholar]
- 7.Rudnick M, Feldman H. Contrast-induced nephropathy: What are the true clinical consequences? Clin J Am Soc Nephrol. 2008;3:263–72. doi: 10.2215/CJN.03690907. [DOI] [PubMed] [Google Scholar]
- 8.Rudnick MR, Berns JS, Cohen RM, Goldfarb S. Nephrotoxic risks of renal angiography: Contrast media-associated nephrotoxicity and atheroembolism – A critical review. Am J Kidney Dis. 1994;24:713–27. doi: 10.1016/s0272-6386(12)80235-6. [DOI] [PubMed] [Google Scholar]
- 9.Groeneveld AB, Tran DD, van der Meulen J, Nauta JJ, Thijs LG. Acute renal failure in the medical intensive care unit: Predisposing, complicating factors and outcome. Nephron. 1991;59:602–10. doi: 10.1159/000186651. [DOI] [PubMed] [Google Scholar]
- 10.Star R. Design issues for clinical trials in acute renal failure. Blood Purif. 2001;19:233–7. doi: 10.1159/000046947. [DOI] [PubMed] [Google Scholar]
- 11.Fishbane S. N-acetylcysteine in the prevention of contrast-induced nephropathy. Clin J Am Soc Nephrol. 2008;3:281–7. doi: 10.2215/CJN.02590607. [DOI] [PubMed] [Google Scholar]
- 12.Kay J, Chow WH, Chan TM, Lo SK, Kwok OH, Yip A, et al. Acetylcysteine for prevention of acute deterioration of renal function following elective coronary angiography and intervention: A randomized controlled trial. JAMA. 2003;289:553–8. doi: 10.1001/jama.289.5.553. [DOI] [PubMed] [Google Scholar]
- 13.Shyu KG, Cheng JJ, Kuan P. Acetylcysteine protects against acute renal damage in patients with abnormal renal function undergoing a coronary procedure. J Am Coll Cardiol. 2002;40:1383–8. doi: 10.1016/s0735-1097(02)02308-2. [DOI] [PubMed] [Google Scholar]
- 14.Briguori C, Airoldi F, D’Andrea D, Bonizzoni E, Morici N, Focaccio A, et al. Renal Insufficiency Following Contrast Media Administration Trial (REMEDIAL): A randomized comparison of 3 preventive strategies. Circulation. 2007;115:1211–7. doi: 10.1161/CIRCULATIONAHA.106.687152. [DOI] [PubMed] [Google Scholar]
- 15.Hoste EA, De Waele JJ, Gevaert SA, Uchino S, Kellum JA. Sodium bicarbonate for prevention of contrast-induced acute kidney injury: A systematic review and meta-analysis. Nephrol Dial Transplant. 2010;25:747–58. doi: 10.1093/ndt/gfp389. [DOI] [PubMed] [Google Scholar]
- 16.Merten GJ, Burgess WP, Gray LV, Holleman JH, Roush TS, Kowalchuk GJ, et al. Prevention of contrast-induced nephropathy with sodium bicarbonate: A randomized controlled trial. JAMA. 2004;291:2328–34. doi: 10.1001/jama.291.19.2328. [DOI] [PubMed] [Google Scholar]
- 17.Ozcan EE, Guneri S, Akdeniz B, Akyildiz IZ, Senaslan O, Baris N, et al. Sodium bicarbonate, N-acetylcysteine, and saline for prevention of radiocontrast-induced nephropathy. A comparison of 3 regimens for protecting contrast-induced nephropathy in patients undergoing coronary procedures. A single-center prospective controlled trial. Am Heart J. 2007;154:539–44. doi: 10.1016/j.ahj.2007.05.012. [DOI] [PubMed] [Google Scholar]
- 18.Recio-Mayoral A, Chaparro M, Prado B, Cozar R, Mendez I, Banerjee D, et al. The reno-protective effect of hydration with sodium bicarbonate plus N-acetylcysteine in patients undergoing emergency percutaneous coronary intervention: The reno study. J Am Coll Cardiol. 2007;49:1283–8. doi: 10.1016/j.jacc.2006.11.034. [DOI] [PubMed] [Google Scholar]
- 19.Alonso A, Lau J, Jaber BL, Weintraub A, Sarnak MJ. Prevention of radiocontrast nephropathy with N-acetylcysteine in patients with chronic kidney disease: A meta-analysis of randomized, controlled trials. Am J Kidney Dis. 2004;43:1–9. doi: 10.1053/j.ajkd.2003.09.009. [DOI] [PubMed] [Google Scholar]
- 20.Brar SS, Hiremath S, Dangas G, Mehran R, Brar SK, Leon MB. Sodium bicarbonate for the prevention of contrast induced-acute kidney injury: A systematic review and meta-analysis. Clin J Am Soc Nephrol. 2009;4:1584–92. doi: 10.2215/CJN.03120509. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Vasheghani-Farahani A, Sadigh G, Kassaian SE, Khatami SM, Fotouhi A, Razavi SA, et al. Sodium bicarbonate plus isotonic saline versus saline for prevention of contrast-induced nephropathy in patients undergoing coronary angiography: A randomized controlled trial. Am J Kidney Dis. 2009;54:610–8. doi: 10.1053/j.ajkd.2009.05.016. [DOI] [PubMed] [Google Scholar]
- 22.Joannidis M, Schmid M, Wiedermann CJ. Prevention of contrast media-induced nephropathy by isotonic sodium bicarbonate: A meta-analysis. Wien Klin Wochenschr. 2008;120:742–8. doi: 10.1007/s00508-008-1117-z. [DOI] [PubMed] [Google Scholar]
- 23.Zoungas S, Ninomiya T, Huxley R, Cass A, Jardine M, Gallagher M, et al. Systematic review: Sodium bicarbonate treatment regimens for the prevention of contrast-induced nephropathy. Ann Intern Med. 2009;151:631–8. doi: 10.7326/0003-4819-151-9-200911030-00008. [DOI] [PubMed] [Google Scholar]