

Abstract
Purpose:
A variety of fixation techniques for subpectoral biceps tenodeses have been described including interference screw and suture anchor fixation. Biomechanical data suggests that dual suture anchor fixation has equivalent strength compared to interference screw fixation. The purpose of the study is to determine the early complication rate after subpectoral biceps tenodesis utilizing a dual suture anchor technique.
Materials and Methods:
A total of 103 open subpectoral biceps tenodeses were performed over a 3-year period using a dual suture anchor technique. There were 72 male and 31 female shoulders. The average age at the time of tenodesis was 45.5 years. 41 patients had a minimum of 6 months clinical follow-up (range, 6 to 45 months). The tenodesis was performed for biceps tendonitis, superior labral tears, biceps tendon subluxation, biceps tendon partial tears, and revisions of prior tenodeses.
Results:
There were a total of 7 complications (7%) in the entire group. There were 4 superficial wound infections (4%). There were 2 temporary nerve palsies (2%) resulting from the interscalene block. One patient had persistent numbness of the ear and a second patient had a temporary phrenic nerve palsy resulting in respiratory dysfunction and hospital admission. One patient developed a pulmonary embolism requiring hospital admission and anticoagulation. There were no hematomas, wound dehiscences, peripheral nerve injuries, or ruptures. In the sub-group of patients with a minimum of 6 months clinical follow-up, the only complication was a single wound infection treated with oral antibiotics.
Conclusions:
Subpectoral biceps tenodesis utilizing a dual suture anchor technique has a low early complication rate with no ruptures or deep infections. The complication rate is comparable to those previously reported for interference screw subpectoral tenodesis and should be considered as a reasonable alternative to interference screw fixation.
Level of Evidence:
Level IV-Retrospective Case Series
Keywords: Biceps, complications, subpectoral, tenodesis Key Message: Subpectoral biceps tenodesis utilizing a dual suture anchor technique provides a low early complication rate comparable to previously reported rates for interference screw fixation. These early clinical findings are consistent with biomechanical data supporting that a dual suture anchor subpectoral technique has equivalent initial biomechanical strength compared to an interference screw.
INTRODUCTION
Optimal surgical management of long head biceps (LHB) tendon pathology remains controversial. The primary surgical options include biceps tenotomy and biceps tenodesis. Potential issues with biceps tenotomy include biceps muscle weakness or discomfort in addition to cosmetic concerns. Proximal biceps tenodesis has been shown to be a reliable treatment for tears, subluxation, and synovitis of the LHB. Tenodesis is preferred for managing LHB pathology in younger, more active patients and in those whom cosmetic deformity is a concern. Several techniques have been described for LHB tenodesis including arthroscopic and open techniques in both the suprapectoral and subpectoral regions. Advantages of the subpectoral tenodesis technique include the removal of the LHB from the bicipital groove potentially limiting the development of postoperative pain secondary to residual tenosynovitis within the biceps sheath. Subpectoral tenodesis (below the pectoralis major tendon) has been shown to provide excellent pain relief and functional improvement with limited residual biceps tendon symptoms.[1,2] While complications of biceps tenodesis in other locations have been studied extensively, limited data exist on the complications of a tenodesis in the subpectoral region.[3,4,5]
Several methods of fixation have been described for a subpectoral tenodesis including interference screws, suture anchors, and bone tunnels.[6,7] Several authors have performed biomechanical studies comparing interference screw fixation and suture anchor fixation for a proximal biceps tenodesis in both the suprapectoral and subpectoral regions.[6,8,9,10]
Subpectoral tenodesis utilizing a single-suture anchors has been shown to have inferior initial biomechanical properties (ultimate load-to-failure and stiffness) when compared to an interference screw construct.[6] Based upon this biomechanical data, Golish et al. have recommended the use of an interference screw instead of suture anchors for subpectoral tenodesis fixation.[6] We have recently shown that a dual suture anchor tenodesis and interference screw tenodesis have equivalent biomechanical strength when performed in the subpectoral region.[11] Clinically, outcomes of subpectoral proximal biceps tenodeses using interference screw fixation have been reported with excellent outcomes and rupture rates between 0.6% and 2%.[4,5] Limited data exist on the outcomes after subpectoral biceps tenodesis utilizing a suture anchor technique.[2]
The purpose of the present study is to evaluate the early postoperative complications of open subpectoral biceps tenodesis using a dual suture anchor technique. Our hypothesis is that the early complication rates after dual suture anchor fixation will be equivalent to those reported for interference screw fixation for a subpectoral tenodesis.
MATERIALS AND METHODS
All surgical cases from one surgeon (RZT) were reviewed from 12/2009 to 12/2012. Institutional review board (IRB) approval was obtained prior to initiating the study. We utilized the surgeon's personal surgical log to identify all patients who underwent an open subpectoral biceps tenodesis utilizing a dual suture anchor repair technique during the study period. Any patient between the ages of 18 and 80 years who underwent an open subpectoral biceps tenodesis utilizing a dual suture anchor fixation technique by the primary surgeon (RZT) between 12/09 and 12/12 was eligible for inclusion in the study. Exclusion criteria included all patients undergoing a biceps tenotomy or tenodesis utilizing another technique besides the dual suture anchor subpectoral technique.
Preoperative imaging included shoulder radiographs (AP, true AP, scapular Y and axillary views) and a shoulder magnetic resonance imaging (MRI) of every patient undergoing a biceps tenodesis. The decision to treat patients was based upon preoperative history and physical examination, MRI findings, and an arthroscopic evaluation. In the group of patients treated for biceps tendonitis, the decision to treat was made preoperatively based upon a history of bicipital pain and tenderness on physical examination independent of the MRI or arthroscopic findings. In the group treated for superior labral tears, the decision to treat was made at the time of surgery based upon a clinical history consistent with a superior labral tear (traumatic onset), positive physical exam findings (positive active compression test), an MRI confirming type II, III, or IV superior labral tear, and an arthroscopic evaluation consistent with a type II, III, or IV superior labral tear.[12,13] In the group of patients treated for biceps tendon partial tears, the decision to treat was made at the time of surgery where a tenodesis was performed if there was a partial tear greater than 25% of the biceps tendon. Finally, in the group treated for a failed proximal biceps tenodesis, the decision to treat was made preoperatively based upon proximal biceps groove pain and tenderness after a proximal tenodesis. No arthroscopy was performed prior to these surgical cases rather the biceps was cut proximally through the subpectoral tenodesis site surgical exposure and then tenodesed in the same wound.
The surgical technique utilized for dual suture anchor tenodesis has been previously described.[11] A glenohumeral arthroscopy was initially performed on all patients at which time the biceps tendon was evaluated as well as the labrum, glenohumeral cartilage, and rotator cuff. The biceps were then cut using electrocautery through an anterior rotator cuff interval portal. All other arthroscopic procedures were then performed, if any. After the arthroscopy, the scope instruments were removed and a 3- to 4-cm longitudinal incision is made centered over the inferior border of the pectoralis major tendon. The pectoralis major is retracted laterally, the conjoint tendon is retracted medially, and the previously cut biceps tendon is delivered into the wound. The biceps groove is removed of soft tissue and periosteum down to bleeding cortical bone using a currette and two drill holes are created for placement of two Mitek G4 Suture Anchors (Mitek, Norwood, MA). The superior drill hole is placed 3 cm proximal to the inferior border of the pectoralis tendon and the inferior hole is placed 1 cm proximal to the inferior border of the pectoralis tendon. Two Mitek G4 Suture Anchors (Mitek, Norwood, MA) are each loaded with a single No 2 Fiberwire (Arthrex, Naples, FL) stitch. The biceps tendon is then re-cut 20 mm proximal to the musculotendinous junction. A No. 2 Fiberwire (Arthrex, Naples, FL) suture from one anchor is then placed in the distal 15 mm of the proximal biceps tendon from proximal to distal using Krackow technique. The second suture on the other anchor is placed in the same region of the biceps tendon from distal to proximal using Bunnell technique. The Krackow stitch anchor is then impacted into the proximal hole and the Bunnell stitch anchor is impacted into the distal hole. The sutures from each anchor are then tied using 2 half hitches followed by a reverse half hitch, followed by 3 half hitches on opposite posts thrown in opposite directions after each hitch [Figure 1].
Figure 1.
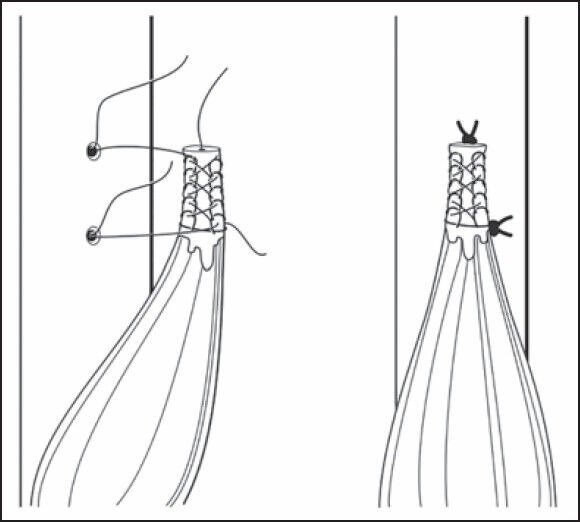
Dual suture anchor biceps tenodesis construct (Two Mitek G4 suture anchors (Mitek, Norwood, MA) each loaded with a No. 2 Fiberwire (Arthrex, Naples, FL) suture with one in Krackow stitch pattern and the other in a Bunnell stitch pattern)
The electronic medical record for all patients was retrospectively reviewed for early postoperative complications within the first 12 months of surgery including wound infection, hematoma, wound dehiscence, rupture, hardware failure, and requirement for re-operation. Patient demographics recorded included age, sex, hand dominance, surgical side, associated surgical procedures, biceps tendon diagnosis, and diagnoses requiring other surgical procedures.
RESULTS
A total of 103 open subpectoral biceps tenodeses were performed utilizing the same dual suture anchor technique by the primary surgeon (RZT) during the study period. There were 72 male and 31 female shoulders. The average age at time of tenodesis was 45.5 years. Tenodesis was performed on the dominant side in 55% of shoulders. Tenodeses were performed for five diagnoses: Biceps tendonitis (60), superior labral tears (21), biceps subluxation (8), biceps partial tears (12), and revision of prior tenodesis (2). Other surgical procedures performed at the time of tenodesis included Arthroscopic subacromial/glenohumeral debridement (40), arthroscopic rotator cuff repair (40), and distal clavicle excision (8).
The average length of follow-up was 7 months (range, 1 to 45 months). There were a total of 7 complications (7%). There were 4 superficial wound infections (stitch abscesses) (4%) of which 2 were treated with oral antibiotics alone and 2 required superficial debridement in the operating room and oral antibiotics. There were 2 temporary nerve palsies (2%) resulting from an interscalene block. One patient had persistent numbness of her ear and a second patient had a temporary phrenic nerve palsy resulting in respiratory dysfunction and hospital admission. One patient with no prior history of prior thrombosis and no overt risk factors for hypercoagulability developed a pulmonary embolism requiring hospital admission and anticoagulation. There were no hematomas, wound dehiscences, peripheral nerve injuries, or ruptures. Looking at the subgroup of patients with at least 6 months follow-up, there were a total of 41 patients. In this sub-group of patients with longer follow-up, there was only a single complication (superficial wound infection treated with oral antibiotics).
DISCUSSION
Open subpectoral biceps tenodesis utilizing a dual suture anchor technique has a low early complication rate. Superficial wound infection and interscalene block-related complications were the only significant surgery-related complications within 6 months of the surgical procedure. We reported no deep infections, hematomas, peripheral nerve injuries, fractures, or ruptures utilizing this technique. Complication rates are equivalent to those previously reported for interference screw fixation and should be considered as a reasonable alternative.
Various fixation techniques have been utilized for proximal biceps tenodeses with varying, but in general, low failure rates. Koh et al. reported on 43 patients undergoing proximal biceps tenodesis using suture anchors and noted 7% of patients had a clinically apparent traumatic failure.[14] Scheibel et al. performed 27 proximal biceps tenodeses using a suture anchor and evaluated the repair integrity with an MRI.[15] They reported that 35% of patients had a failure of the tenodesis followed by an autotenodesis more distally in the groove. Millet et al. are the only authors who have reported the results of subpectoral tenodesis utilizing a suture anchor technique.[2] They reported on 54 patients and reported no complications in this group. 89% of patients in this series had a single anchor tenodesis, while 11% had a two anchor tenodesis. Our series is the largest group of patients reported undergoing a suture anchor subpectoral tenodesis.
Several complications have been reported after interference screw biceps tenodesis including tenodesis failure.[1,5,16] Mazzocca et al. reported a 2% failure rate in his initial series of 50 patients after subpectoral interference screw biceps tenodesis.[1] Koch et al. reported a case series of 3 patients who sustained a rupture after proximal biceps tenodesis utilizing an interference screw resulting in an 8% failure rate.[16] Nho et al. reported on 353 patients undergoing a subpectoral biceps tenodesis using an interference screw.[5] The authors reported a 2% complication rate with 0.57% rupture rate, 0.28% deep infection rate, 0.28% peripheral nerve palsy rate, and a .028% reflex sympathetic dystrophy rate. Finally, Sears et al. reported on 2 patients who sustained a humeral shaft fracture after subpectoral tenodesis utilizing an interference screw.[17] While our series is not as large as the series by Nho et al., we did not have any failures, deep infections, fractures, or neurologic injuries.[5] One potential reason for the absence of clinically evident early failures in our series compared to previously reported series using interference screws may be the lack of a sharp transition in stress at the site of fixation with the suture anchor construct compared with the tenodesis screw. We previously identified, in a biomechanical study, that fixation using an interference screw has significantly increased stiffness compared with a suture anchor construct.[11] While the increased stiffness prevents any minor elongations in the construct as it heals, it may place the construct at more risk for catastrophic failure. The risk for fracture is also likely lower with the suture anchor technique as the drill holes made in the humerus are only 1-2 mm compared to the much smaller 7-8 mm drill hole commonly required for an interference screw.
The only significant complication in the current series was four superficial wound infections. The incidence of wound infections is higher than expected and may be secondary to the location of the incision relatively close to the axilla. We utilize vicryl suture to close the subcutaneous layer and this may have precipitated an increased superficial infection rate. All infections were treated with oral antibiotics alone or superficial debridement and oral antibiotics. No superficial infections led to deep infections or other significant morbidity.
One limitation of this study is that this is a retrospective review of a large number of patients and a prospective evaluation was not performed. Consequently, outcome data was not obtained. Another potential limitation is that only early complications were evaluated and it is likely that some re-ruptures were missed. Our average length of follow-up was only 7 months. Nevertheless, most patients after a subpectoral tenodesis are allowed to return to all activities without restriction at 3 months if a concomitant rotator cuff repair was not performed and 6 months if a rotator cuff repair was performed. Consequently, it is likely that most traumatic failures would occur within the first 6 months as has been shown in other series.[5] Looking specifically at the sub-group with greater than 6 month follow-up, we found no increased incidence of complications, specifically re-rupture. There was only one superficial wound infection in this sub-group with an overall complication rate of 2%. Finally, healing data was not obtained and we are therefore unable to confirm that no sub-clinical ruptures occurred.
CONCLUSIONS
Dual suture anchor subpectoral biceps tenodesis leads to a low early complication rate with no deep wound infections, neurologic injuries, or clinically evident ruptures although follow-up in this series is very short. Dual suture anchor subpectoral tenodesis should be considered as a safe and reliable alternative to interference screw fixation with a low overall risk for the development of major postoperative complications although longer follow-up outcome studies are needed to confirm the results.
Footnotes
Source of Support: Nil
Conflict of Interest: The authors and their immediate family or the institution did not receive any financial payments or other benefits from any commercial entity related to the subject of this article.
REFERENCES
- 1.Mazzocca AD, Cote MP, Arciero CL, Romeo AA, Arciero RA. Clinical outcomes after subpectoral biceps tenodesis with an interference screw. Am J Sports Med. 2008;36:1922–9. doi: 10.1177/0363546508318192. [DOI] [PubMed] [Google Scholar]
- 2.Millett PJ, Sanders B, Gobezie R, Braun S, Warner JJ. Interference screw vs. suture anchor fixation for open subpectoral biceps tenodesis: Does it matter? BMC Musculoskelet Disord. 2008;15:121. doi: 10.1186/1471-2474-9-121. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Hsu AR, Ghodadra NS, Provencher MT, Lewis PB, Bach BR. Biceps tenotomy versus tenodesis: A review of clinical outcomes and biomechanical results. J Shoulder Elbow Surg. 2011;20:326–32. doi: 10.1016/j.jse.2010.08.019. [DOI] [PubMed] [Google Scholar]
- 4.Mazzocca AD, Cote MP, Arciero CL, Romeo AA, Arciero RA. Clinical outcomes after subpectoral biceps tenodesis with an interference screw. Am J Sports Med. 2008;36:1922–9. doi: 10.1177/0363546508318192. [DOI] [PubMed] [Google Scholar]
- 5.Nho SJ, Reiff SN, Verma NN, Slabaugh MA, Mazzocca AD, Romeo AA. Complications associated with subpectoral biceps tenodesis: Low rates of incidence following surgery. J Shoulder Elbow Surg. 2010;19:764–8. doi: 10.1016/j.jse.2010.01.024. [DOI] [PubMed] [Google Scholar]
- 6.Golish SR, Caldwell PE, Miller MD, Singanamala N, Ranawat AS, Treme G, et al. Interference screw versus suture anchor fixation for subpectoral tenodesis of the proximal biceps tendon: A cadaveric study. Arthroscopy. 2008;24:1103–8. doi: 10.1016/j.arthro.2008.05.005. [DOI] [PubMed] [Google Scholar]
- 7.Mazzocca AD, Rios CG, Romeo AA, Arciero RA. Subpectoral biceps tenodesis with interference screw fixation. Arthroscopy. 2005;21:896. doi: 10.1016/j.arthro.2005.04.002. [DOI] [PubMed] [Google Scholar]
- 8.Mazzocca AD, Bicos J, Santangelo S, Romeo AA, Arciero RA. The biomechanical evaluation of four fixation techniques for proximal biceps tenodesis. Arthroscopy. 2005;21:1296–306. doi: 10.1016/j.arthro.2005.08.008. [DOI] [PubMed] [Google Scholar]
- 9.Papp DF, Skelley NW, Sutter EG, Ji JH, Wierks CH, Belkoff SM, et al. Biomechanical evaluation of open suture anchor fixation versus interference screw for biceps tenodesis. Orthopedics. 2011;34:e275–8. doi: 10.3928/01477447-20110526-04. [DOI] [PubMed] [Google Scholar]
- 10.Patzer T, Santo G, Olender GD, Wellmann M, Hurschler C, Schofer MD. Suprapectoral or subpectoral position for biceps tenodesis: Biomechanical comparison of four different techniques in both positions. J Shoulder Elbow Surg. 2012;21:116–25. doi: 10.1016/j.jse.2011.01.022. [DOI] [PubMed] [Google Scholar]
- 11.Tashjian RZ, Henninger HB. Biomechanical evaluation of subpectoral biceps tenodesis: dual suture anchor versus interference screw fixation. J Shoulder Elbow Surg. 2013;22(10):1408–12. doi: 10.1016/j.jse.2012.12.039. [DOI] [PubMed] [Google Scholar]
- 12.Snyder SJ, Banas MP, Karzel RP. An analysis of 140 injuries to the superior glenoid labrum. J Shoulder Elbow Surg. 1995;4:243–8. doi: 10.1016/s1058-2746(05)80015-1. [DOI] [PubMed] [Google Scholar]
- 13.O'Brien SJ, Pagnani MJ, Fealy S, McGlynn SR, Wilson JB. The active compression test: A new and effective test for diagnosing labral tears and acromiooclavicular joint abnormality. Am J Sports Med. 1998;26:610–3. doi: 10.1177/03635465980260050201. [DOI] [PubMed] [Google Scholar]
- 14.Koh KH, Ahn JH, Kim SM, Yoo JC. Treatment of biceps tendon lesions in the setting of rotator cuff tears: Prospective cohort study of tenotomy versus tenodesis. Am J Sports Med. 2010;38:1584–90. doi: 10.1177/0363546510364053. [DOI] [PubMed] [Google Scholar]
- 15.Scheibel M, Schroder RJ, Chen J, Bartsch M. Arthroscopic soft tissue tenodesis versus bony fixation anchor tenodesis of the biceps tendon. Am J Sports Med. 2011;39:1046–52. doi: 10.1177/0363546510390777. [DOI] [PubMed] [Google Scholar]
- 16.Koch BS, Burks RT. Failure of biceps tenodesis with interference screw fixation. Arthroscopy. 2012;28:735–40. doi: 10.1016/j.arthro.2012.02.019. [DOI] [PubMed] [Google Scholar]
- 17.Sears BW, Spencer EE, Getz CL. Humeral fracture following subpectoral biceps tenodesis in 2 active, healthy patients. J Shoulder Elbow Surg. 2011;20:e7–11. doi: 10.1016/j.jse.2011.02.020. [DOI] [PubMed] [Google Scholar]