

Abstract
Objective:
Persons experiencing homelessness are a vulnerable population and are at increased risk for morbidity and all-cause mortality compared to the general population. This study sought to evaluate medication use, regular physician visits, and identify health conditions among the homeless population of Long Beach, California.
Methods:
Two “brown bag” medication review events were held at homeless shelters in the Long Beach area. Demographic information, medication use, and comorbid disease states were obtained through surveys.
Findings:
Three-fourths of the cohort (95 participants) consisted of males, and the average age of participants was 48 years. Psychiatric disorders and cardiovascular disease were the most common disease states reported at 32% and 46%, respectively and so were medications used in treating these chronic diseases. Medication adherence was found to be a significant problem in this population, where more than 30% of patients were nonadherent to medications for chronic diseases. Furthermore, foot problems, hearing and vision difficulties constitute the most commonly overlooked health problems within the homeless population.
Conclusion:
Based on this and other similar finding, we must accept that the homeless represent a vulnerable population, and that because of this fact, more programs should be focused at improving availability and access to health care among the homeless. Regarding the high number of reported health problems in the study, more studies are needed and more studies should incorporate screening for foot, hearing, and vision issues, both to increase awareness and to provide an opportunity for devising possible solutions to these highly preventable conditions.
Keywords: Health access, homeless, medication review
INTRODUCTION
Homelessness is a major public health concern in Los Angeles County and throughout the United States. The term homelessness has a specific meaning, and a homeless individual is defined as “an individual who lacks housing (without regard to whether the individual is a member of a family), including an individual whose primary residence during the night is a supervised public or private facility (e.g. shelters) that provides temporary living accommodations, and an individual who is a resident in transitional housing”.[1] Nationally, approximately 650,000 individuals were homeless on any given night in 2009.[2] In Los Angeles County alone, it is estimated that 250,000 individuals experienced homelessness during some portion of 2009, and 82,000 people were homeless on any given night.[3] Specifically, in Long Beach, the city has the ninth largest population for large cities of chronically (≥12 months) homeless individuals, with 1061 chronically homeless living in shelters and on the streets and the 10th largest population of homeless veterans in the country according to the City of Long Beach 2013 Homeless Count Summary Report.[4] These homeless individuals include persons from diverse cultural backgrounds, and include men, women, and children. In addition, homeless populations often have multiple concurrent health care needs, including both chronic and acute conditions, which render them extremely vulnerable.[5,6]
Poverty is the main contributor to homelessness[2,7] and results in a lack of stable housing, poor nutrition, stress, inadequate hygiene, and increased contact with communicable diseases. Studies have found that substance abuse and mental illness rates are higher among homeless individuals.[8] It is estimated that one in three homeless individuals suffer from alcoholism compared to one in nine of the general population and that 20-25% of homeless suffer from mental illness compared to 4-6% of the general population.[2,9,10,11] The difficulties associated with both substance abuse and mental illness create a vicious cycle, which ultimately leads to poverty because these conditions often result in increased stress, loss of employment, and loss of housing. In addition, other health problems such as cardiovascular disease, diabetes, and skin disorders, are frequently reported among the persons experiencing homelessness. Unfortunately, despite the fact that the homeless are considered a vulnerable population in terms of the incidence of health-related illness, disabilities, and have higher age-adjusted mortality compared to the general population,[12,13] individuals experiencing homelessness are less likely to seek preventive and regular health care services and are more likely to encounter barriers to health care access.[14,15,16,17,18]
American University of Health Sciences (AUHS) understands that persons experiencing homelessness are less likely to seek health care at institutions unless it is absolutely necessary.[19,20,21] Therefore, the university regularly holds community health events incorporating pharmacist-conducted “brown bag” medication reviews to address health care concerns of the homeless and educate them about the importance of health care and any medications being taken. These community health events are consistent with the community engagement mission of AUHS and its School of Pharmacy and are part of a collaborative educational and outreach effort with the university's surrounding community to enhance community engagement and awareness of the needs of that experiencing homelessness in the vicinity. The University sponsors two gender-based programs known in the community as Women Inspired Self Health (WISH) and Men Achieving Self Health (MASH) outreach, each of which focus primarily on providing community-based services to the homeless population.
Community engagement through health and wellness events that include medication reviews conducted by pharmacists to educate participants, promote proper medication use, increase awareness about prevalent diseases affecting the homeless population, as well as identify health risks.[2] These community engagement events serve to increase health care access for the homeless, and foster a better understanding of this population and its needs. In this study, we sought to evaluate medication use, regular physician visits, and identify health conditions among the homeless population of the Long Beach, California vicinity through two such community “brown bag” medication review events.
METHODS
We performed a survey-based study of the homeless population within the Long Beach community using data collected from the community “brown bag” conducted during two, full-day WISH/MASH events, hosted by AUHS during December 2011 and February 2012. The study was approved by the AUHS Institutional Review Board. The events were advertised throughout the community and local homeless shelters by posting fliers detailing the location and services provided at each event and encouraging homeless to bring their medication containers. These fliers were placed 1-2 weeks prior to the events. A total of 95 self-reported homeless individuals participated in the two events held by AUHS. A questionnaire was provided to each homeless individual who attended and was completed at the time of meeting with the pharmacist to ensure the individual understood the overall meaning of the questions and avoid any misinterpretation. These individuals brought medication containers, completed a personal medical history questionnaire prior to the private pharmacist consultation, and participated in review of their medications. All participants who attended the two events were asked if they had a stable place of residence, if participants stated their residence was a shelter or stated they were homeless, they were included in the study analysis. Participants who stated they had a stable residence were excluded. For homeless participants who attended both sessions only data collected from the second session was included, thus avoiding duplicating participant numbers and data.
The questionnaire was designed to collect data, such as age, sex, family history, current medications taken, and date of last physician visit, comorbid conditions previously diagnosed, a subjective description of their health, and any complaints the individuals may have reported regarding their own health status. Patients were asked to report if they were healthy without health problems, not feeling well, have recurring health problems that recently started, or had recurring health problems for many years. During the interview, participants were asked if they knew why each medication was being taken, e.g. what conditions each one was being used to treat. Participants were also asked during the consultation, whether any nonprescription drugs or complementary medicines were being taken and any recent discontinuation of medications. Medication refill history and any issues related to compliance with the medication were asked individually based on the medication that participants were taking and on their health conditions.
Continuous variables were compared by Student's t-test. Dichotomous data were compared using χ2 with Yates correction or Fisher exact test where appropriate. All statistical analyses were performed using GraphPad Prism version 6.0 (San Diego, CA, USA). A P ≤ 0.05 denotes statistical significance.
RESULTS
A total of 95 unique homeless individuals participated in the “brown bag” events held in the Long Beach community. Seventy-four percent of the participants were male. The mean age of the homeless participants was 48 years old and ranged from 20 to 72 years of age. The mean age was similar between sexes. Most were aware and understood their health status and familiar with their respective medical conditions. Many of the homeless participants in our study also reported feeling shame, embarrassment, and prejudice when discussing their health care needs with providers.
Regarding, health status of participants, 25% of participants stated a feeling of well-being during the day of the survey with no immediate health care concerns, and 13% reported not being well. A much higher percentage (56%) of patients reported not being well due to having multiple concurrent acute and chronic health problems. Interestingly, 43% of the participants reported routinely seeing a regular primary care provider, and 54% had seen their physician or been to a hospital within the past year.
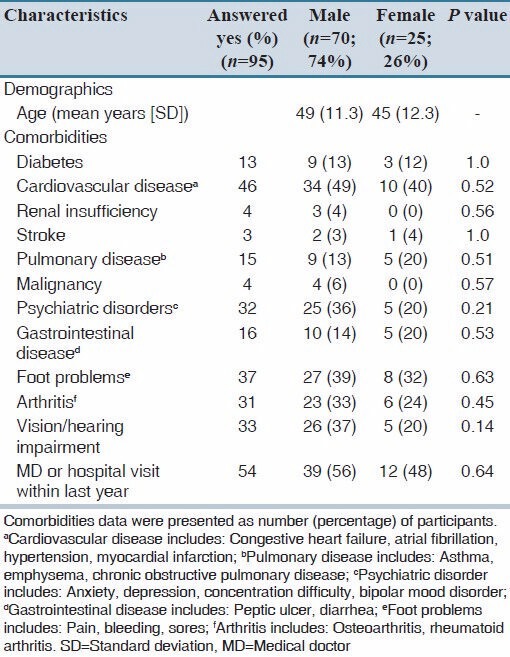
The data were then analyzed for specific health problems. The percentage of homeless participants with specific health problems are listed in Table 1. The most common chronic health problems among the participants were cardiovascular diseases followed by psychiatric disorders, with 46% and 32% of participants reporting them, respectively. Arthritis and visual/hearing impairment was reported by approximately 32% of participants, and of particular note, 37% of individuals reported having foot problems (pain, sores, or bleeding) [Table 1]. No statistically significant difference was observed when comparing health problems between male and female homeless individuals. Although, there was a numerically higher number of males reporting visual/hearing impairment compared to females (37% vs. 20%), although this did not reach statistical significance (P = 0.14) [Table 1].
Table 1.
Demographic and clinical characteristics (medical history questionnaire replies) of the study population
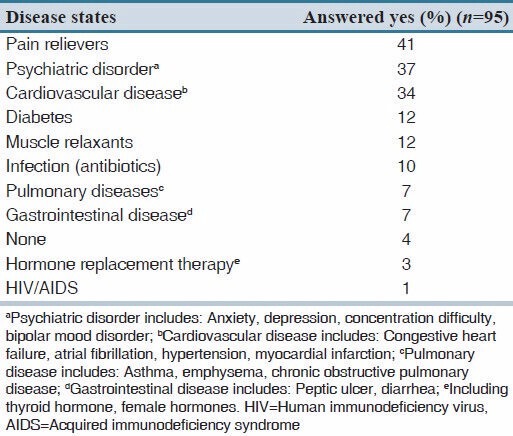
Consistent with the observations of cardiovascular and psychiatric diseases being highly reported among this cohort of individuals, medications for the treatment of these diseases were also highly reported. Angiotensin-converting enzyme inhibitors and diuretics were the highest reported blood pressure medications, which together accounted for 57% of blood pressure medications being taken. In participants with psychiatric disorders, 35% of participants were taking selective serotonin reuptake inhibitors as their primary treatment. However, the highest numbers of medications taken by our cohort were pain-relievers, which included hydrocodone/acetaminophen, nonsteroidal antiinflammatory drugs (NSAIDs), and acetaminophen. In our population 25% of patients reported taking over the counter NSAID medications and acetaminophen for pain. This observation is also consistent with diseases reported, as arthritis and foot problems were reported by a significant portion of the study population. Furthermore, of patients taking pain relievers and muscle relaxants nearly all had reported having arthritis or history of bodily injury [Table 2].
Table 2.
Medication use history for specific disease states and uses among the study population
Each patient's reported diagnosis and their current medication regimen were thoroughly examined. Unfortunately, while the type of medications being taken by our cohort was consistent with their reported disease states, we also found that a high percentage of patients were nonadherent [Table 3]. This was determined by comparing patient diagnosis to the medication regimen. It was found that a large portion of chronic diseases reported by patients were not being treated. More than 30% of patients were not compliant with their medications for any given chronic disease, with the highest on-adherence being found in patients with gastrointestinal, pulmonary, and psychiatric diseases [Table 3].
Table 3.
Medication non-adherence with chronic diseases among the study population

The number of comorbidities present in the homeless participants overall was stratified into four categories; zero, one, two, or greater than three comorbid conditions. The smallest groups were those that reported no comorbid conditions (13%) followed by those reporting one or two conditions, 21% and 22%, respectively. Forty-four percent of participants reported three or more comorbidities, making it the largest group. Ages of these groups did not differ, as the average age of each group was between 45 and 48 years of age. The only significant difference observed between comorbidity groups, and gender was a higher percentage of women reporting only one comorbid condition (female 36% vs. male 16%, P = 0.045). In line with the number of comorbidities present, we found that the number medications taken closely matched. The median number of medications taken by this population was two (interquartile range: 1, 3).
DISCUSSION
A total of 95 homeless individuals participated in the “brown bag” events. Consistent with literature, we found the mean age of participants was 48 years (range 20-72 years) and that males made up the majority of participants (74%). Furthermore, in-line with previous studies,[20,22,23] psychiatric disorders and cardiovascular disease were the most common comorbidities in both males and females [Table 1]. Nevertheless, females in the cohort studied reported more psychiatric disorders compared to males [Table 1]. Gelberg et al. have reported mental illness in 26% of their homeless population within the skid row, downtown Los Angeles area; however, they did not compare rates among males versus females.[22] Hearing problems and vision loss were also highly reported health problems among participants, with 33% reporting these issues. Furthermore, 44% of participants reported three or more comorbid conditions, further demonstrating that homeless persons suffer from high morbidity rates.
It was found that medication use was consistent with reported diagnosis; however, a large portion of patients were not one a medication regimen for a reported chronic disease. During consultation with the pharmacist, the importance of medication adherence was stressed and possible solutions and advice were given to address reasons for nonadherence. Consistent with literature and of particular concern, was the high number of patients diagnosed with psychiatric disorders, but were not taking maintenance medications for the disorder.[24] Addressing medication nonadherence is not simple as a number of factors can be involved, especially within the homeless population. For example, competing needs such as shelter and food may be seen as a priority compared to medication.[14,25] The availability to request refills for medications or make appointments for physician visits may also be a barrier to medication compliance.[26] Recent studies have explored addressing such issues. Coe et al. addressed psychiatric medication noncompliance and the usefulness of long acting injectable medications, and while positive effects were noted one limitation is that only a limited number of psychiatric medications come in long acting injectable form.[25] A study by Burda et al. found that providing cellular phones to homeless increased medication adherence and the ability to monitor and manage medication regimens in a small study population; however, the feasibility and cost to implement such a program is questionable.[26]
Another significant finding from our survey was the high number of participants (37%) that reported foot problems (included bleeding, pain, and foot sores). Foot problems are an often over-looked condition that is not reported by most studies on the homeless population; nonetheless, it is a problem that has been observed.[22,27] Chen et al. recently published a study that found foot health to be an often overlooked health problem and highlighted the health importance of foot care in homeless populations, particularly in preventing limb-threatening pathologies.[27] Thus, the foot problems reported in our study further highlight the increased risk that the homeless population has in developing lower-extremity pathologies. Aside from deformities or peripheral neuropathy, the acquisition of adequate shoes and socks can potentially have a major impact on this often-concealed problem.
Many of these participants reported embarrassment and shame when discussing health care needs with providers. This perceived prejudice observed in the population sample might also contribute to the competing priorities serving as a barrier to health care.[20,28] Thus, healthcare professionals who work with the homeless should be cognizant of these fears and attempt to foster an environment of open communication, two-way trust, and respect for the person if a positive outcome is to be obtained.
Our study has several limitations. First, the study is limited by its small sample size, which may or may not be an accurate representation of the entire homeless community within Long Beach, California. Second, the questionnaire used was based on self-reported homelessness and diagnosis of diseases, as well as subjective data, which may have resulted in reporting bias. Furthermore, the questionnaire provided to each participant did not collect information on duration of homelessness. Despite this second limitation, we confirmed the reported diagnoses to be accurate by comparing reported diseases with medications being taken. Thirdly, while each individual was consulted on the importance of medication adherence and possible solutions to help individuals stay adherent were provided by the pharmacist, data on specific barriers were not documented during consultations, thus barriers to adherence in our population was not reported. Future “brown bag” events are planned and documentation of barriers to medication adherence is planned. In addition, we were not able to observe or follow-up on adherence with recommended medication interventions and/or referrals. Finally, participants who attended the WISH/MASH events may have been more concerned with health and well-being; thus, it is possible that these individuals were more likely to consult with the pharmacist and resulting in possible selection bias.
It is our collective opinion that the pharmacist provided “brown bag” medication review held at community health events provided an effective way to engage the homeless community through proper medication use, emphasize the importance of medication adherence, answer health care related questions, and provide referrals to accessible health care institutions. These types of events not only reinforce the importance of medication adherence, but also provide referrals that will hopefully decrease the need and use of emergency departments, which are frequently used by this population as their primary care sources.[29] Future community health events should also include appropriate hearing and vision testing as well as podiatric care consultations. In addition, future studies should document perceived barriers to medication adherence in the homeless population in order to gain a better understanding of common obstacles, and lead to programs or interventions to increase medication adherence in this vulnerable patient population. Based on this and other similar finding, it must be accepted that the homeless represent a vulnerable population whose access to healthcare is impaired, thus supporting a need for enhanced awareness among health care providers to ensure increased allocation of attention and resources devoted to the homeless.
AUTHORS' CONTRIBUTION
Conception and design: MT Chong
Development of methodology: MT Chong
Acquisition of data: MT Chong, M. Harwood, R. d'Assalenaux, E. Rosenberg, O. Aruoma, and A. Bishayee
Analysis and interpretation of data: MT Chong, J. Yamaki and A. Bishayee
Writing, review and/or revision of the manuscript: MT Chong J. Yamaki, M. Harwood, R. d'Assalenaux, E. Rosenberg, O. Aruoma and A. Bishayee
Study supervision: MT Chong
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Section 330 of the Public Health Service Act (42 U.S.C., 254b) [Last accessed 2014 Mar 02]. http://www.hrsa.gov/advisorycommittees/shortage/Meetings/20100922/section330mua.pdf .
- 2.Bralock AR, Farr NB, Kay J, Lee MJ, Smythe-Padgham C, Scherlin DD, et al. Issues in community-based care among homeless minorities. J Natl Black Nurses Assoc. 2011;22:57–67. [PubMed] [Google Scholar]
- 3.Homelessness in Los Angeles County. 2011. [Last accessed on 2014 Mar 02]. Available from: http://www.laalmanaccom/social/so14htm .
- 4.City of Long Beach 2013 Homeless Count Summary Report. 2013. [Last accessed on 2014 Jun 01]. Available from: http://www.downtownlongbeach.org/Uploads/2013-Homeless-Count-o_1GjKd2.pdf .
- 5.Montauk SL. The homeless in America: Adapting your practice. Am Fam Physician. 2006;74:1132–8. [PubMed] [Google Scholar]
- 6.Aday LA. Health status of vulnerable populations. Annu Rev Public Health. 1994;15:487–509. doi: 10.1146/annurev.pu.15.050194.002415. [DOI] [PubMed] [Google Scholar]
- 7.Baumohl J. Addiction and the American debate about homelessness. Br J Addict. 1992;87:7–10. doi: 10.1111/j.1360-0443.1992.tb01889.x. [DOI] [PubMed] [Google Scholar]
- 8.North CS, Eyrich KM, Pollio DE, Spitznagel EL. Are rates of psychiatric disorders in the homeless population changing? Am J Public Health. 2004;94:103–8. doi: 10.2105/ajph.94.1.103. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Gelberg L, Linn LS. Social and physical health of homeless adults previously treated for mental health problems. Hosp Community Psychiatry. 1988;39:510–6. doi: 10.1176/ps.39.5.510. [DOI] [PubMed] [Google Scholar]
- 10.Nielsen SF, Hjorthøj CR, Erlangsen A, Nordentoft M. Psychiatric disorders and mortality among people in homeless shelters in Denmark: A nationwide register-based cohort study. Lancet. 2011;377:2205–14. doi: 10.1016/S0140-6736(11)60747-2. [DOI] [PubMed] [Google Scholar]
- 11.Toro PA, Hobden KL, Wyszacki Durham K, Oko-Riebau M, Bokszczanin A. Comparing the characteristics of homeless adults in Poland and the United States. Am J Community Psychol. 2014;53:134–45. doi: 10.1007/s10464-014-9632-8. [DOI] [PubMed] [Google Scholar]
- 12.Hibbs JR, Benner L, Klugman L, Spencer R, Macchia I, Mellinger A, et al. Mortality in a cohort of homeless adults in Philadelphia. N Engl J Med. 1994;331:304–9. doi: 10.1056/NEJM199408043310506. [DOI] [PubMed] [Google Scholar]
- 13.Morrison DS. Homelessness as an independent risk factor for mortality: Results from a retrospective cohort study. Int J Epidemiol. 2009;38:877–83. doi: 10.1093/ije/dyp160. [DOI] [PubMed] [Google Scholar]
- 14.Wood D, Valdez RB. Barriers to medical care for homeless families compared with housed poor families. Am J Dis Child. 1991;145:1109–15. doi: 10.1001/archpedi.1991.02160100041021. [DOI] [PubMed] [Google Scholar]
- 15.Lewis JH, Andersen RM, Gelberg L. Health care for homeless women. J Gen Intern Med. 2003;18:921–8. doi: 10.1046/j.1525-1497.2003.20909.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Miller DS, Lin EH. Children in sheltered homeless families: Reported health status and use of health services. Pediatrics. 1988;81:668–73. [PubMed] [Google Scholar]
- 17.Grant R, Shapiro A, Joseph S, Goldsmith S, Rigual-Lynch L, Redlener I. The health of homeless children revisited. Adv Pediatr. 2007;54:173–87. doi: 10.1016/j.yapd.2007.03.010. [DOI] [PubMed] [Google Scholar]
- 18.Stein JA, Andersen RM, Robertson M, Gelberg L. Impact of hepatitis B and C infection on health services utilization in homeless adults: A test of the Gelberg-Andersen Behavioral Model for Vulnerable Populations. Health Psychol. 2012;31:20–30. doi: 10.1037/a0023643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Kushel MB, Vittinghoff E, Haas JS. Factors associated with the health care utilization of homeless persons. JAMA. 2001;285:200–6. doi: 10.1001/jama.285.2.200. [DOI] [PubMed] [Google Scholar]
- 20.Gelberg L, Gallagher TC, Andersen RM, Koegel P. Competing priorities as a barrier to medical care among homeless adults in Los Angeles. Am J Public Health. 1997;87:217–20. doi: 10.2105/ajph.87.2.217. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Hammond WP, Matthews D, Corbie-Smith G. Psychosocial factors associated with routine health examination scheduling and receipt among African American men. J Natl Med Assoc. 2010;102:276–89. doi: 10.1016/s0027-9684(15)30600-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Gelberg L, Andersen RM, Leake BD. The behavioral model for vulnerable populations: Application to medical care use and outcomes for homeless people. Health Serv Res. 2000;34:1273–302. [PMC free article] [PubMed] [Google Scholar]
- 23.Jones CA, Perera A, Chow M, Ho I, Nguyen J, Davachi S. Cardiovascular disease risk among the poor and homeless-what we know so far. Curr Cardiol Rev. 2009;5:69–77. doi: 10.2174/157340309787048086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Sajatovic M, Levin J, Ramirez LF, Hahn DY, Tatsuoka C, Bialko CS, et al. Prospective trial of customized adherence enhancement plus long-acting injectable antipsychotic medication in homeless or recently homeless individuals with schizophrenia or schizoaffective disorder. J Clin Psychiatry. 2013;74:1249–55. doi: 10.4088/JCP.12m08331. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Coe AB, Moczygemba LR, Gatewood SB, Osborn RD, Matzke GR, Goode JV. Medication adherence challenges among patients experiencing homelessness in a behavioral health clinic. Res Social Adm Pharm. 2012 Dec 5; doi: 10.1016/j.sapharm.2012.11.004. Published online. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Burda C, Haack M, Duarte AC, Alemi F. Medication adherence among homeless patients: A pilot study of cell phone effectiveness. J Am Acad Nurse Pract. 2012;24:675–81. doi: 10.1111/j.1745-7599.2012.00756.x. [DOI] [PubMed] [Google Scholar]
- 27.Chen B, Mitchell A, Tran D. Podiatric health needs of homeless populations as a public health concern. J Am Podiatr Med Assoc. 2012;102:54–6. doi: 10.7547/1020054. [DOI] [PubMed] [Google Scholar]
- 28.Davis E, Tamayo A, Fernandez A. “Because somebody cared about me. That's how it changed things”: Homeless, chronically ill patients' perspectives on case management. PLoS One. 2012;7:e45980. doi: 10.1371/journal.pone.0045980. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Little GF, Watson DP. The homeless in the emergency department: A patient profile. J Accid Emerg Med. 1996;13:415–7. doi: 10.1136/emj.13.6.415. [DOI] [PMC free article] [PubMed] [Google Scholar]