

Abstract
Trichofolliculoma represents abortive differentiation of pluripotent skin cells toward hair follicles. We present a case of an adult female with lobulated mass involving the tip and dorsum of the nose for the last 15 years. The systemic and radiological examinations were noncontributory. The clinical diagnosis was thought to be dermoid cyst. The fine-needle aspiration cytology of the lobulated mass was performed, and the cytology smears showed anucleate squames admixed with sebaceous cells. The possibility of a benign skin adnexal lesion was suggested. The biopsy was done, and the final diagnosis of trichofolliculoma was made. The wide local excision of the mass was performed, and no recurrence was noted during the follow-up of 1 year.
Keywords: Cytology, hair follicle, nose, sebaceous cells, skin adnexal
INTRODUCTION
Trichofolliculoma is a rare pilar tumor and intermediate in differentiation between a hair follicle nevus, which is simple hyperplasia of the hair follicle, and a trichoepithelioma, which lacks maturation of the hair follicle. It usually presents as a solitary nodule approximately 0.5 cm in diameter in the head and neck region with central umbilication and a tuft of fine hairs protruding out of it.[1] The criteria for diagnosing benign primary epithelial skin tumors in cytology are not well-established and have been mainly described in a single case report to the best of our knowledge.[2] This report highlights its unusual lobulated appearance and aims to add information to the limited data available on the cytology of trichofolliculoma.
CASE REPORT
A 35-year-old female patient presented with gradually progressing lobulated mass for 15 years. On local examination, the mass was lobulated, skin colored, shiny, firm, nontender, involving the tip, and dorsum of the nose [Figure 1]. The systemic examination was noncontributory and radiological examination revealed no bony destruction or formation of sinus tract. The clinical diagnosis of dermoid cyst was made. The fine-needle aspiration cytology (FNAC) of lobulated mass was performed using 22 gauge needle and scant, blood mixed aspirate was obtained. The smears were air dried and stained with May-Grόnwald-Giemsa. The patient was advised for biopsy and histopathological examination.
Figure 1.

Skin colored, lobulated mass over the tip and dorsum of nose
The cytology smears showed mildly cellularity and cells were comprised of irregular clusters of anucleate squames admixed with singly lying cell and loose cluster of sebaceous cells having moderate amount of pale cytoplasm and round to oval nuclei. The possibility of a benign skin adnexal lesion was suggested [Figure 2a and b]. The biopsied tissue was single, firm, globular grey white and measured 1 cm × 1 cm × 0.5 cm in size. Histopathological examination revealed unremarkable epidermis and dermis showed strands of stratified squamous epithelium containing fragments of hair shafts along with many variables sized hair follicles exhibiting varying degree of maturation [Figure 2c and d]. The final diagnosis of trichofolliculoma was made. Wide local excision was done, and no recurrence was noted during the follow-up of 1 year.
Figure 2.
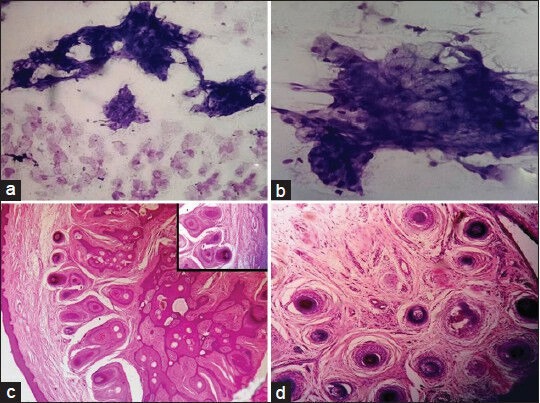
(a) Clusters of anucleate squames admixed with sebaceous cells (Giemsa, ×100). (b) Loose cluster of sebaceous cells (Giemsa, ×400). (c) Unremarkable epidermis along with dermis showing lobules of hair follicle structure (H and E, ×100). (d) Hair follicles showing varying degree of maturation (H and E, ×400)
DISCUSSION
Trichofolliculoma is common in adulthood with no definitive racial or gender predilection.[3] The unusual locations reported for trichofolliculoma are external auditory meatus, intranasal area, genitalia, lip, and vulva.[4] The exact etiology is still not known, and no proven association has been found with any dermatological or systemic diseases. However, it has been found that the pluripotent skin cells undergo unsuccessful differentiation toward hair follicles.[3] The presentation of trichofolliculoma as large lobulated mass or cystic lesion is rare as seen in our case.[5] The lesion mimics basal cell carcinoma, dermal nevus, epidermoid cyst and trichoepithelioma.[3,5] Tumor undergoes changes similar to the regressing hair follicle in its well-known cycle.[6] Trichofolliculoma were characterized by the proliferation of abnormal cytokeratin 15-positive hair follicle stem cells, differentiating toward the outer root sheath with an attempt to make hair without proper differentiation.[7] FNAC has helped identifying uncommon cutaneous cystic lesions, benign and malignant tumors of epidermal appendages such as chondroid syringomas, cylindromas, pilomatrixomas, sebacecous carcinoma, and primary adenoid cystic carcinoma, as well as tumors of the dermis and subcutaneous fat.[8] In our case, the differential diagnosis of sebaceous adenoma and steatocystoma simplex was considered on cytology; however, histopathological examination helped in exclusion of these entity. On an extensive search FNAC findings of trichofolliculoma has been described only once in the literature.[9] This case report highlights the atypical presentation of trichofolliculoma presenting as large lobulated mass and aims to add information to the limited data available on the cytology of trichofolliculoma. FNAC findings, however, has to be supported by histopathological examination to know the hair follicular origin for definitive diagnosis.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Weedon D. Weedon's skin pathology. 3rd ed. China: Elsevier; 2010. p. 758. [Google Scholar]
- 2.Orell SR, Domanski H. Skin and subcutis. In: Orell SR, Sterrett GF, editors. Fine Needle Aspiration Cytology. 4th edition. New Delhi: Churchill Livingstone Elsevier; 2005. p. 373. [Google Scholar]
- 3.Howard MS, Smoller BR. Trichofolliculoma. e–Medicine Dermatology. [Last accessed on 2010 Aug 02]. Available from: http://www.emedicine.medscape.com .
- 4.Choi CM, Lew BL, Sim WY. Multiple trichofolliculomas on unusual sites: A case report and review of the literature. Int J Dermatol. 2013;52:87–9. doi: 10.1111/j.1365-4632.2011.05120.x. [DOI] [PubMed] [Google Scholar]
- 5.McCalmoont TH. Adnexal neoplasm. In: Bolognia JL, Jorrijo JL, Rapini RP, editors. Dermatology. 2nd ed. Philadelphia: Mosby Elsevier; 2008. pp. 1693–712. [Google Scholar]
- 6.Schulz T, Hartschuh W. The trichofolliculoma undergoes changes corresponding to the regressing normal hair follicle in its cycle. J Cutan Pathol. 1998;25:341–53. doi: 10.1111/j.1600-0560.1998.tb01757.x. [DOI] [PubMed] [Google Scholar]
- 7.Misago N, Kimura T, Toda S, Mori T, Narisawa Y. A revaluation of trichofolliculoma: The histopathological and immunohistochemical features. Am J Dermatopathol. 2010;32:35–43. doi: 10.1097/DAD.0b013e3181a77414. [DOI] [PubMed] [Google Scholar]
- 8.Daskalopoulou D, Galanopoulou A, Statiropoulou P, Papapetrou S, Pandazis I, Markidou S. Cytologically interesting cases of primary skin tumors and tumor-like conditions identified by fine-needle aspiration biopsy. Diagn Cytopathol. 1998;19:17–28. doi: 10.1002/(sici)1097-0339(199807)19:1<17::aid-dc5>3.0.co;2-l. [DOI] [PubMed] [Google Scholar]
- 9.Alexander MP, Makhija P, Jayaseelan E. Fine needle aspiration cytology of trichofolliculoma: A case report. Indian J Pathol Microbiol. 2007;50:870–2. [PubMed] [Google Scholar]