

Abstract
Background:
Although alopecia areata (AA) is typically seen by medical staff as a benign, not life-threatening cosmetic disease, some studies have found significant impairment in quality of life (QL) in AA patients. There are no studies that assess QL in Brazilian AA patients.
Objectives:
To evaluate QL in AA patients, using the 36-item Short-Form Health Survey (SF-36). The most affected SF-36 dimensions were compared to two culturally different AA QL studies.
Materials and Methods:
We performed a case-control study with 37 AA patients and 49 age- and sex-matched volunteer blood donors. The results of a Turkish and a French study were compared to our results.
Results:
The dimensions social functioning (P = 0,001), role emotional (P = 0,019), and mental health (P = 0,000) scored statistically lower in the AA group in relation to controls, suggesting a worse QL. Incomparison to the Turkish and French studies, we found: (1) On the dimension role emotional, QL was equally impaired; (2) on the dimension social functioning, it was not different than the Turkish study; (3) social life of French AA patients was more affected; and (4) vitality and mental health dimensions were significantly more affected in French and Turkish patients.
Conclusions:
Impairment in QL in AA patients affected psychological, emotional, and social aspects of theirlives. Despite the scores of SF-36 dimensions varied significantly among different cultural groups, impairment of QL was found in all three studies; thus, we can suppose that these findings are not linked to a specific culture.
Keywords: Alopecia areata, case-control studies, quality of life
INTRODUCTION
Alopecia areata (AA) is an autoimmune disease of universal distribution[1,2] and the most frequent cause of inflammation-induced hair loss.[3] It occurs in virtually any hair-bearing area, including eyebrows and eyelashes, but is more common in the scalp.[4] The most severe forms include a complete absence of terminal scalp hair (alopecia totalis) and a total loss of terminal scalp and body hair (alopecia universalis).[5]
The disease affects patients relatively young, mostly before the 40s, and has a rapid onset and an unpredictable course.[2,3]
AA is associated with risk of vitiligo, lupus erythematosus, psoriasis, atopic dermatitis, thyroid disease, and allergic rhinitis;[6] but generally do not interfere with physical health. It is typically seen by medical staff as a benign, not life-threatening cosmetic disease. Also, the psychological impact of alopecia and the vulnerability of patients are often not recognized.[7] AA is a very difficult disease to treat; curative therapy does not exist and there is a lack of well-conducted long-term, controlled trials.[3,8,9]
Terminal scalp hairs, along with eyebrows and eyelashes, are very important features of human identity.[10] Humans have been using a wide range of time-consuming procedures to change the appearance of their hair since old times.[11,12,13]
Some studies have showed an impairment of quality of life (QL) in AA patients particular in the psychological, emotional, and social aspects of life.[14,15,16] There are no studies in the Brazilian population that assess QL in AA patients. The present study evaluated QL in AA patients attending a University Hospital in Rio de Janeiro, Brazil using the the Medical Outcomes Study (MOS) 36-item Short-form Health Survey (SF-36). To better figure out the level of QL in the AA group, we also compared the most affected SF-36 dimensions with two different AA QL studies that utilized the same measuring instrument but concerning different cultures: Turkish and French AA patients.
MATERIALS AND METHODS
Study population
This case-control study was performed in the Alopecia Clinic at Clementino Fraga Filho University Hospital, Rio de Janeiro, Brazil between January 2011 and October 2012 and included 37 AA patients and 49 controls.
The inclusion criteria for AA patients were: Diagnosis of AA as performed by a dermatologist, age ≥18 years, and no cognitive impairments. The exclusion criteria were: (1) Diagnosis of AA diffuse/incognita and (2) other active and/or noncontrolled diseases.
The control group was composed by volunteer blood donors at the same hospital. Inclusion criteria for the control group were: Age ≥18 years and no cognitive impairments. The exclusion criteria were: (1) Other active and/or noncontrolled diseases.
The study was approved by the hospital ethics committee and all subjects signed the informed consent.
Study procedures
Variables such as age, sex, marital status, educational level, employment situation, monthly income, and comorbidities were collected for both AA patients and control groups.
AA severity of hair loss (percentage of the scalp surface covered by the sum of all alopecic areas) was evaluated and AA patients were classified into six groups: S0 (N = 4), no hair loss; S1 (N = 14), <25% hair loss; S2 (N = 5), 25-49% hair loss; S3 (N = 1), 50-74% hair loss; S4 (N = 3), 75-99% hair loss; and S5 (N = 10), 100% hair loss.[17] Among four S0 AA patients, two were males with patches of alopecia in beard and two were females who had been with AA for more than 5 years and were experiencing remission for the first time.
SF-36
The SF-36 is a multi-item scale designed to measure health-related QL. This generic instrument was constructed for use in the MOS.[18] It is composed of eight health dimensions or subscales: (1) Physical functioning (PF)-assesses limitations in physical activities including bathing or dressing because of health problems; (2) role physical (RP)-limitations with work or other daily activities as a result of physical health; (3) bodily pain (BP)-assessment of severity of pain and its effects in work; (4) general health (GH)-evaluates the individual's self-perception; (5) vitality (V)-level of energy and fatigue; (6) social functioning (SF)-limitations in social activities due to physical or emotional problems; (7) role emotional (RE)-limitations with work or other daily activities as a result emotional problems; and (8) mental health (MH)- psychological well-being, emotional distress, sadness, and happiness.
The eight subscales are hypothesized to form two distinct summary measures: The physical health component and the mental health component. Three subscales (physical functioning, role physical, and bodily pain) correlate most highly with the physical health component; whereas, social functioning, role emotional, and mental health subscales correlate mostly with the mental health component. Although general health, vitality, and social functioning have correlations with both components; vitality and social functioning still correlate more with the mental health component.
The mental health subscale contributes the most to the scoring of the mental health component and has been shown to be useful in screening for psychiatric disorders.[19]
This instrument is suitable for self-administration, computerized administration, or administration by a trained person or by telephone, to persons of 14 years of age and older. Each subscale's score varies in the range of 0 (lowest level of QL) to 100 (highest level of QL).[19] It was judged to be the most widely evaluated generic patient-assessed health outcome measure and can be used to compare different diseases and populations. It was adapted and translated for Brazilian Portuguese in 1999 by Ciconelli et al.[20] Both AA and control groups were interviewed by the same trained person.
Statistical analysis
Parametric and nonparametric tests (Chi-square, Kolmogorov–Smirnov, and t-test) were used to compare the groups.
The Mann-Whitney nonparametric test for two independent samples was used to compare SF-36 scores of AA patients and controls.
XLSTAT-PRO (win-upgrade) version 10 from ADDINSOFT was used for data analysis. P < 0.05 was considered to be statistically significant.
RESULTS
The 37 AA patients (23 females and 14 males) had a mean age of 35.89 ± 11.59 and the control group (23 females; 26 males), a mean age of 34.63 ± 12.49.
There were no statistical differences between AA group and the control group in relation to sex, age, marital status, education, employment situation, and monthly income.
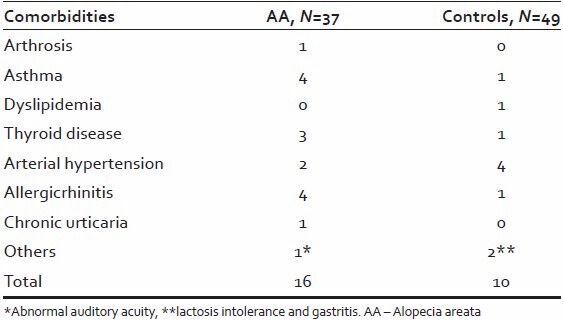
The AA group presented with a higher prevalence of comorbidities in relation to the control groups (P = 0.0015). All comorbidities were under control and/or not active.
The distribution of comorbidities between the groups is summarized in Table 1.
Table 1.
Distribution of comorbidities between the groups
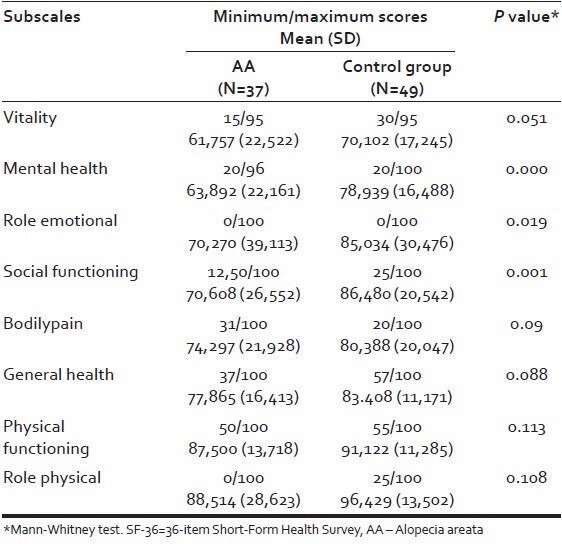
We found that, in the AA group, vitality, mental health, role emotional, and social functioning were the most affected subscales; whereas, bodily pain, general health, role physical, and physical functioning the least ones. Three subscales, social functioning (P = 0.001), role emotional (P = 0,019), and mental health (P = 0,000) displayed statistically significant difference in relation to the control group. These three subscales scored higher in the control group suggesting a better QL in these dimensions. The vitality subscale reached a P value very close to the significant level (P = 0.051) showing a trend for statistical significance. On the contrary, none of the subscales that correlate mostly with the physical component displayed differences between the two groups, showing that the groups did not differ in these dimensions. These results are summarized in Table 2.
Table 2.
Mean±SD of SF-36 subscales scores for AA patients and control group
In the AA group, mental health subscale's score was not influenced by sex (P = 0.139), age (P = 0.603), and severity of alopecia (P = 0.130).
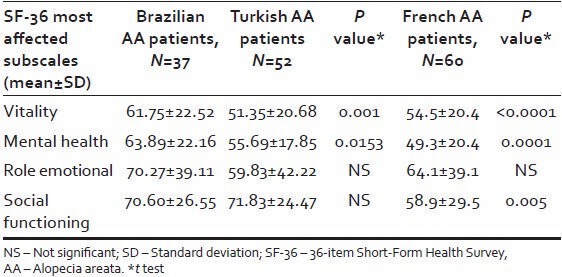
We examined our results in relation to two different AA QL studies that also used the SF-36.[14,16]
Our results showed that: (1) On the dimension role emotional, QL is impaired in our AA patients at the same level as in the Turkish and French studies; (2) on the dimension social functioning, our results donot differ from that of the Turkish study, suggesting that QL related to this specific dimension is equally impaired on both settings. Social life in French AA patients seems to be more affected; however, (3) vitality and mental health dimensions were significantly more affected in French and Turkish patients than in ours.
The comparison between our results and the Turkish and French studies results are shown in Table 3.
Table 3.
Quality of life indicative comparisons between AA patients from three different cultures
DISCUSSION
This is the first case-control study that evaluated QL in Brazilian AA patients.
QL is a rather new concept[21] and its assessment has recently gained importance in chronic non-life-threatening diseases such as skin diseases.[22] QL assessments help, in clinical practice, clinicians to make judgments about which aspects of daily life are most affected by the disease. This knowledge is beneficial in patient management.[23] The perception of patients about their diseases and consequences in life may differ from their healthcare providers as what constitutes QL is a personal and individual question. Therefore QL should, preferably, be measured by the patient.[24]
Our findings found that impairment in QL in AA patients occurredonly in the mental component of health; affecting patient's psychological, emotional, and social aspects of life.
Two other studies with AA patients using the generic instrument SF-36 also demonstrated impairment in QL.
Gulec et al., 2004, in a case-control study, found that vitality, mental health, and role emotional were the most altered dimensions in AA group. Physical functioning and role physical, on the contrary, displayed the highest scores. Vitality and mental health scored significantly higher in the control group. Role emotional did not differ from the control group. Surprisingly, social functioning was better in the patient group than in the controls. The authors attributed this finding to the fact that the control group was made up of staff from a very busy hospital with busy schedule and not much spare time for social activities.
A more recent study with French AA patients found mental health, vitality, and socialfunctioning to be the most affected dimensions. Again, the least affected dimensions were physical functioning, role physical, and bodily pain. Compared to general population, French age- and sex-matched controls, AA patients reported significantly worst QL in all dimensions of SF-36 except physical functioning and bodily pain.
As we compared our results with theirs, we found that despite the scores of vitality, mental health, role emotional, and social functioning subscales have varied significantly among different culturally background patients, QL impairment was found in all three studies. It is reasonable to suppose that these findings are not linked to a specific culture. AA seems to greatly affect patients worldwide. It is note worthy to mention about patients with AA who havegiven their testimony about difficulties in living with this disease as well as dermatology nurses who agreed about the devastating impact this disease may have on some patients' lives. Nurses also agreed about the role of patients support groups as places where patients can learn how to share with one another and to be part of a group that nurtures and heals them.[25,26,27]
The limitations of the study are the small number of patients and the sample selected from an Alopecia Clinic of a University Hospital. Patients attending an Alopecia Clinic are more likely to be affected by their disease as long as they are seeking for professional help. Our findings may not be representative of the general population of those with AA.
CONCLUSION
This study underscores the necessity of encouraging research on the psychological aspects of AA in order to better manage this disease. Healthcare providers should listen and support such patients. It would be very interesting to deepen the understanding about which factors influence AA patients QL in order to promote effective interventions in improving patients' well-being. Although AA is a “non-life-threating cosmetic disease”, patients may be suffering a great deal from it.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
REFERENCES
- 1.Sharma VK, Dawn G, Kumar B. Profile of alopecia areata in Northern India. Int J Dermatol. 1996;35:22–7. doi: 10.1111/j.1365-4362.1996.tb01610.x. [DOI] [PubMed] [Google Scholar]
- 2.Alkhalifah A, Alsantali A, Wang E, McElwee KJ, Shapiro J. Alopecia areata update Part I. Clinical picture, histopatology, and pathogenesis. J Am Acad Dermatol. 2010;62:177–88. doi: 10.1016/j.jaad.2009.10.032. [DOI] [PubMed] [Google Scholar]
- 3.Gilhar A, Etzioni A, Paus R. Alopecia areata. N Engl J Med. 2012;366:1515–25. doi: 10.1056/NEJMra1103442. [DOI] [PubMed] [Google Scholar]
- 4.Madani S, Shapiro J. Alopecia areata update. J Am Acad Dermatol. 2000;42:549–66. [PubMed] [Google Scholar]
- 5.Wasserman D, Guzman-Sanchez DA, Scott K, McMichael A. Alopecia areata. Int J Dermatol. 2007;46:121–31. doi: 10.1111/j.1365-4632.2007.03193.x. [DOI] [PubMed] [Google Scholar]
- 6.Chu SY, Chen YJ, Tseng WC, Lin MW, Chen TJ, Hwang CY, et al. Comorbidity profiles among patients with alopecia areata: The importance of onset age, a nationwide population-based study. J Am Acad Dermatol. 2011;65:949–56. doi: 10.1016/j.jaad.2010.08.032. [DOI] [PubMed] [Google Scholar]
- 7.Hunt N, McHale S. Reported experiences of persons with alopecia areata. J Loss Trauma. 2005;10:33–50. [Google Scholar]
- 8.Ito T. Advances in the management of alopecia areata. J Dermatol. 2012;39:11–7. doi: 10.1111/j.1346-8138.2011.01476.x. [DOI] [PubMed] [Google Scholar]
- 9.Messenger AG, McKillop J, Farrant P, McDonagh AJ, Sladdent M. British Association of Dermatologists' guidelines for the management of alopecia areata 2012. Br J Dermatol. 2012;166:916–26. doi: 10.1111/j.1365-2133.2012.10955.x. [DOI] [PubMed] [Google Scholar]
- 10.Bolduc C, Shapiro J. Hair care products: Waving, straightening, conditioning, and coloring. Clin Dermatol. 2001;19:431–6. doi: 10.1016/s0738-081x(01)00201-2. [DOI] [PubMed] [Google Scholar]
- 11.Oliveira MT. Hair: from etiologia to imaginarium. Rev Bras Psican. 2007;3:135–51. [Google Scholar]
- 12.Lascaratos J, Tsiamis C, Lascaratos G, Stavrianeas NG. The roots of cosmetic medicine: Hair comestics in Bizantine times (AD 324-1453) Int J Dermatol. 2004;43:397–401. doi: 10.1111/j.1365-4632.2004.02131.x. [DOI] [PubMed] [Google Scholar]
- 13.Haas N. Hair over the ages and in art. The culture, and social history of hair and its depiction in art. In: Em Blume-Peytavi U, Tosti A, Whiting D, Trueb R, editors. Hair Growth and Disorders. Ch. 27. Berlin: Springer; 2008. pp. 526–37. [Google Scholar]
- 14.Gulec AT, Tanriverdi N, Dürü Ç, Saray Y, Akçali C. The role of psychological factors in alopecia areata and the impact of the disease on the quality of life. Int J Dermatol. 2004;43:352–6. doi: 10.1111/j.1365-4632.2004.02028.x. [DOI] [PubMed] [Google Scholar]
- 15.Sampogna F, Picardi A, Chren MM, Melchi CF, Pasquini P, Masini C, et al. Association between poorer quality of life and psychiatric morbidity in patients with different dermatological conditions. Psychosom Med. 2004;66:620–4. doi: 10.1097/01.psy.0000132869.96872.b2. [DOI] [PubMed] [Google Scholar]
- 16.Dubois M, Baumstarck-Barrau K, Gaudy-Marqueste C, Richard MA, Loundou A, Auquier P, et al. Quality of Life Group of the French Society of Dermatology. Quality of life in alopecia areata: A study of 60 cases. J Invest Dermatol. 2010;130:2830–3. doi: 10.1038/jid.2010.232. [DOI] [PubMed] [Google Scholar]
- 17.Olsen EA, Hordinsky MK, Price VH, Roberts JL, Shapiro J, Canfield D, et al. National Alopecia Areata Foundation. Alopecia areata investigacional assessment guidelines..Part II. National Alopecia Areata Foundation. J Am Acad Dermatol. 2004;51:440–7. doi: 10.1016/j.jaad.2003.09.032. [DOI] [PubMed] [Google Scholar]
- 18.Ware JE, Jr, Sherbourne CD. The MOS 36-Item short-form health survey (SF-36) I. Conceptual framework and item selection. Med Care. 1992;30:473–83. [PubMed] [Google Scholar]
- 19.The Sf Community-Sf-36 R survey update. Ware JR, JE. [Last accessed on 2013 Apr 18]. Available from: http://www.sf-36.org/tools/SF.shtml .
- 20.Ciconelli RM, Ferraz MB, Santos W, Meinão I, Quaresma MR. Translation for the Portuguese Language and validation of the generic questionnaire for evaluation of quality of life SF-36 (Brazil SF-36) Rev Bras Reumatol. 1999;39:143–1150. [Google Scholar]
- 21.Seidl EM, Zannon CM. Quality of life and health: Conceptual and methodological issues. Cad Saúe Pública. 2004;20:580–8. doi: 10.1590/s0102-311x2004000200027. [DOI] [PubMed] [Google Scholar]
- 22.Both H, Essink-Bot ML, Busschbach J, Nijsten T. Critical review of generic and dermatology-specific health-related quality of life instruments. J Invest Dermatol. 2007;127:2726–39. doi: 10.1038/sj.jid.5701142. [DOI] [PubMed] [Google Scholar]
- 23.Najafi M, Sheikhvatan M, Montazeri A, Hesameddin S, Sheikh Fatollahi M. Quality of life in coronary artery disease: SF-36 compared to WHOQOL-BREF. J Teh Univ Heart Ctr. 2008:101–6. [Google Scholar]
- 24.Slevin ML, Plant H, Lynch D, Drinkwater J, Gregory WM. Who should measure quality of life, the doctor or the patient? Br J Cancer. 1988;57:109–12. doi: 10.1038/bjc.1988.20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Beard HO. Social and psychological implications of alopecia areata. J Am Acad Dermatol. 1986;14:697–700. doi: 10.1016/s0190-9622(86)80482-0. [DOI] [PubMed] [Google Scholar]
- 26.McGettigan ML. Ahead with no hair. J Am Acad Dermatol. 2004;51:S18–9. doi: 10.1016/j.jaad.2004.01.012. [DOI] [PubMed] [Google Scholar]
- 27.Prickitt J, McMichael AJ, Gallagher L, Kalabokes V, Boeck C. Helping patients cope with chronic alopecia areata. Dermatol Nurs. 2004;16:237–41. [PubMed] [Google Scholar]