

Abstract
IMPORTANCE
The Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS) is a multicomponent study designed to generate actionable recommendations to reduce Army suicides and increase knowledge of risk and resilience factors for suicidality.
OBJECTIVES
To present data on prevalence, trends, and basic sociodemographic and Army experience correlates of suicides and accident deaths among active duty Regular Army soldiers between January 1, 2004, and December 31, 2009, and thereby establish a foundation for future Army STARRS investigations.
DESIGN, SETTING, AND PARTICIPANTS
Analysis of trends and predictors of suicide and accident deaths using Army and Department of Defense administrative data systems. Participants were all members of the US Regular Army serving at any time between 2004 and 2009.
MAIN OUTCOMES AND MEASURES
Death by suicide or accident during active Army service.
RESULTS
The suicide rate rose between 2004 and 2009 among never deployed and currently and previously deployed Regular Army soldiers. The accident death rate fell sharply among currently deployed soldiers, remained constant among the previously deployed, and trended upward among the never deployed. Increased suicide risk was associated with being a man (or a woman during deployment), white race/ethnicity, junior enlisted rank, recent demotion, and current or previous deployment. Sociodemographic and Army experience predictors were generally similar for suicides and accident deaths. Time trends in these predictors and in the Army’s increased use of accession waivers (which relaxed some qualifications for new soldiers) do not explain the rise in Army suicides.
CONCLUSIONS AND RELEVANCE
Predictors of Army suicides were largely similar to those reported elsewhere for civilians, although some predictors distinct to Army service emerged that deserve more in-depth analysis. The existence of a time trend in suicide risk among never-deployed soldiers argues indirectly against the view that exposure to combat-related trauma is the exclusive cause of the increase in Army suicides.
Although the suicide rate in the US military has historically been below the civilian rate, it climbed steadily since the beginning of the Iraq and Afghanistan conflicts to the point where by 2008 it exceeded the demographically matched civilian rate.1 The Department of the Army responded to this trend in 2008 by entering into an agreement with the National Institute of Mental Health to fund jointly a study that came to be called the Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS [www.armystarrs.org]). The 2 overarching goals of the Army STARRS are (1) to evaluate hypotheses about modifiable risk and resilience factors for suicidality that could be used to target effective preventive interventions for Army suicides and (2) to expand basic scientific understanding of psychosocial and neurobiological risk and resilience factors for suicidal behaviors and their psychopathologic correlates. The Army STARRS includes a number of coordinated component studies designed to facilitate non-experimental hypothesis generation and testing, intervention targeting, and intervention evaluation.2 The first of these is a Historical Administrative Data Study (HADS) that examines patterns and correlates of suicide in an integrated data system created by combining information from several Army and Department of Defense administrative databases on all soldiers who served in the Army between January 1, 2004, and December 31, 2009. Prior studies3–7 of military administrative records identified numerous sociodemographic characteristics, stressful life experiences, and treated psychiatric conditions that predict suicide, but none of these earlier studies assembled as comprehensive an assessment of these variables as the HADS.
The present study gives the first results of the preliminary HADS analysis designed to examine suicide and accident death rates among Regular Army soldiers between 2004 and 2009, along with basic sociodemographic and military career predictors. We examine accession waivers (acceptance of applicants who do not fully meet Army admission standards) and stop loss orders (requirement that soldiers serve past their original obligation) because these policies were used during the study period to meet operational requirements for the conflicts in Iraq and Afghanistan and questions have been raised whether they might have been associated with negative outcomes, including the rising Army suicide rate.6,8,9 We also investigate the extent to which changes in Army composition might account for the increase in suicides. Finally, we evaluate patterns and predictors of accident death rates in parallel to suicide rates to assess potential similarities in patterns and correlates.
Methods
Historical Administrative Data Study
Army STARRS components were approved by institutional review boards at the National Institute of Mental Health, Harvard University, Uniformed Services University School of the Health Sciences, University of Michigan, and University of California, San Diego, which determined that the present study did not constitute human participant research because it relies entirely on deidentified secondary data. We worked with the Army and Department of Defense to identify 39 nonclassified administrative data systems containing soldiers’ characteristics, exposures, and experiences considered potentially important predictors of suicides.3 Data from the first 7 such systems available for research use are considered herein (Table 1).
Table 1.
Selected Data Sources Contributing Data to the Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS) Historical Administrative Data Study
| Military Data System | Description |
|---|---|
| Defense Manpower Data Center (DMDC) Master Personnel | Includes basic demographics. Two measures of race/ethnicity are available based on soldier self-identification, with no obvious way to prioritize divergent values. Also, Hispanic race/ethnicity is recorded independently. There is also pre-enlistment information (eg, Armed Forces Qualification Test category, education) and career highlights such as assignments, promotions and demotions, and length of Army service) |
| DMDC Defense Enrollment and Eligibility Reporting System | Contains selected basic demographics and captures changes in family structure (eg, marital status and dependents) over time |
| DMDC Contingency Tracking System | Captures location and duration of deployments since September 2001 for soldiers supporting Operations Iraqi Freedom, New Dawn, and Enduring Freedom |
| Armed Forces Medical Examiner Tracking System | Primary source of the cause and manner of death for all deaths of active duty Army soldiers, determined directly by the Armed Forces Medical Examiner or in consultation with civilian authorities |
| Defense Casualty Information Processing System | Alternative source of cause and manner of death |
| Department of Defense Suicide Event Report | Registry of selected cases of suicidal behavior. Extensive information collected by behavioral health specialists following suicides, as well as suicide attempts or suicidal ideation requiring hospitalization or evacuation |
| Army Waiver Data | List of soldiers who did not meet ≥1 entry criterion but were granted a waiver and allowed to enlist. Includes the type of waiver (medical, conduct, education, etc) |
Sample
We focus on all 975 057 Regular Army soldiers (ie, excluding those in the Army National Guard and Army Reserve) on active duty between January 1, 2004, and December 31, 2009. The mean duration of active duty during this study period was approximately 38 months, for a total of approximately 37 million person-months. Of this total, there were 569 deaths classified as suicides by the Armed Forces Medical Examiner, and an additional 1331 deaths were classified as accidents. Data on patterns and correlates of these deaths were analyzed at the person-month level in a case-control framework,10 with cases consisting of the person-months of suicide or accident death and controls comprising a 1 per 400 stratified (by age, sex, rank, and historical time) probability sample of all other person-months. The latter were given a weight of 400 to account for their undersampling. Person-months associated with other types of death were censored.
Measures
Sociodemographics
The sociodemographic variables considered herein are sex, age, race/ethnicity, religion, education, and family status. The latter includes marital status and the presence vs the absence of dependents.
Army Entry Characteristics
All enlisted personnel take the Armed Forces Qualification Test (AFQT) during recruitment and are classified into categories between I (best) and V (worst). The AFQT distributions change over time because of fluctuations in the number and mix of applicants (eg, changes in the civilian employment rate and in national patriotism that increased after the September 11, 2001, terrorist attacks) and recruitment targets. Recruits not meeting Army entry criteria (either AFQT scores or other requirements such as those involving criminal records, substance use, or medical history) may request an accession waiver. Data on all such waivers by type (medical, substance use, or conduct) are available in the HADS. This information is important in that the Army accepted more candidates than usual who did not meet the Army’s usual admission standards during portions of the study period to meet operational requirements, raising concerns that increased accession waivers might help explain the increase in the Army suicide rate during that period.
Army Experiences
We also examine length of Army service, current rank, history of demotions, and stop loss orders. Stop loss refers to the involuntary extension of a soldier’s term of active Army service beyond its original end date because critical occupational special-ties are understaffed during times of war, deployment, or national emergencies. Recent examples include special forces medics, mortuary affairs specialists, and helicopter mechanics. Involuntary retention on active duty, especially if facing deployment to a combat zone or potentially missing out on a desirable civilian job opportunity, could be a significant stressor and a possible predictor of suicidal behavior.
Missing Values
Some item-level administrative data were missing for particular person-months, but in most cases these data could be recovered by cross-checking other data systems or other months in the records for the same soldiers. Remaining missing values, which were small in number, were assigned imputed values equal to subgroup modes.
Analysis Methods
Trends in Mortality Rates
Soldiers enter (enlist) or leave (separate or retire) the Army throughout the year, which means that not all soldiers on active duty in a given year serve the entire year. The ratio of suicides in a given year divided by the number of soldiers on active duty for any part of the year consequently underestimates the suicide rate by the fraction 1/p, where p is the mean proportion of the year during which all soldiers on active duty in the year served during the year. To remove this bias, we calculated the suicide rate as the number of suicides in the year divided by the mean number of soldiers serving in each month during that year. By convention, we report the suicide rate per 100 000 person-years (ie, per 1.2 million person-months). Because suicides are not homogeneously distributed throughout the calendar year, resulting in volatile monthly rates that are difficult to interpret, we calculated 12-month moving averages, where the rate reported for a given month represents the average of the current and previous 11-month rates.
Predictive Associations
Discrete time survival analysis with person-month as the unit of analysis11 was used to study associations of predictors with suicides and accident deaths, respectively. A logistic link function was used in the analysis. The dependent variables were dichotomous classifications of whether or not the person-month involved a suicide or accident death. Explanatory variables included sociodemographics, Army entry characteristics, and Army experiences. Time-varying characteristics such as length of Army service were defined in relation to the current person-month. Controls were included for calendar time. Only one substantive predictor was included in each equation to focus on overall associations. We recognize, of course, that more detailed multivariate analyses could have been performed to adjust for overlap among predictors and for interactions, but we wanted to focus on overall associations in this preliminary report. However, given a central interest in deployment, each association was also stratified by the 3 broad deployment history categories of never, currently, and previously deployed, and suicide rates were calculated per 100 000 person-years of active service for soldiers with each value of each predictor with each category of the deployment history variable. We also evaluated whether the associations of predictors with outcomes varied significantly by deployment history and calendar time.
To evaluate the possibility that the rise in the Army suicide rate since 2004 was related to increases in accession waivers or other changes in Army composition, we estimated multivariate models that included all predictors considered herein separately for subsets of person-months in 2004–2005, 2006–2007, and 2008–2009 and evaluated whether regression parameters varied significantly over these different periods. We then used simulation to estimate what the Army suicide rate would have been in 2006–2007 and 2008–2009 if Army composition in those years had been the same as in 2004–2005. This was done by applying the parameter estimates from the 2006–2007 and 2008–2009 equations to the 2004–2005 data, generating predicted probabilities of suicide and accident death for each observation in the 2004–2005 data using the 2006–2007 and 2008–2009 parameters, and then averaging the predicted probabilities of suicide death across the respective simulations to generate predicted mortality rates for 2006–2007 and 2008–2009, respectively, under the assumptions that the distributions of characteristics in those periods were the same as in 2004–2005 but the relationships between the predictors and death were as estimated for 2006–2007 or 2008–2009. Additional detail on the simulations is available in the eAppendix in the Supplement.
Results
Mortality Rates
The suicide rate among Regular Army soldiers increased between 2004 and 2009 not only for the currently and previously deployed but also for the roughly 40% of soldiers who had never deployed (Figure 1). As a point of comparison, the accident death rate among deployed soldiers fell dramatically during this same period, possibly reflecting changes in the nature of Army operations (Figure 2). No meaningful trend in accident deaths occurred among previously deployed soldiers, while the accident death rate trended upward among never-deployed soldiers.
Figure 1.
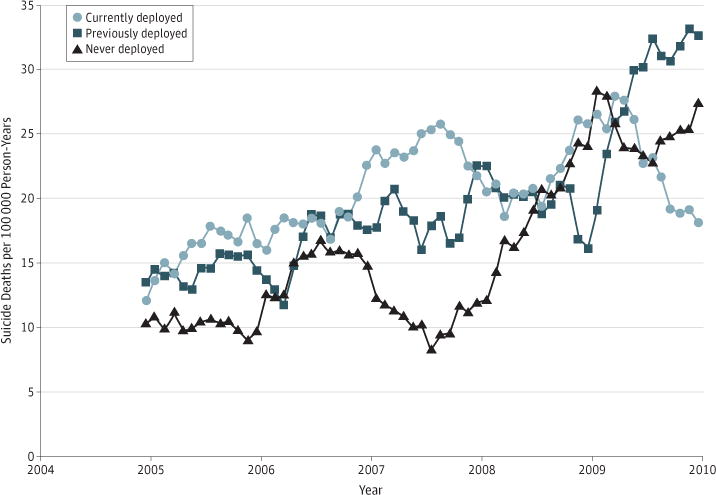
Suicide Deaths per 100000 Person-Years of Active Duty Army Service
Shown are Regular Army 12-month moving averages. Each line represents a 12-month moving average (ie, each respective dot reports the rate for the prior 12-month period).
Figure 2.
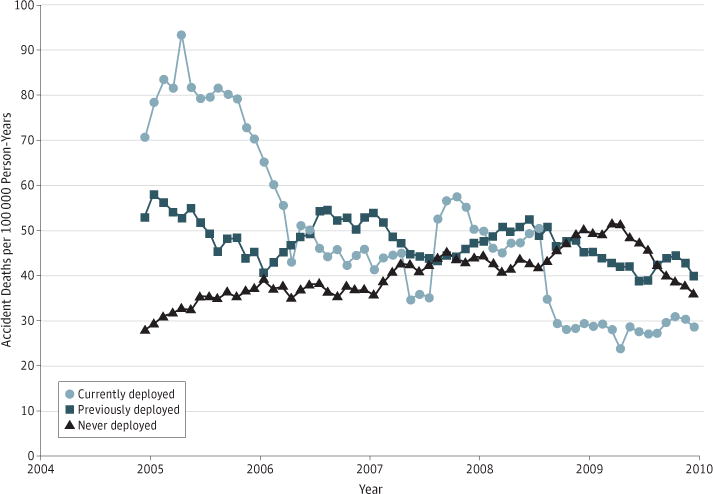
Accident Deaths per 100000 Person-Years of Active Duty Army Service
Shown are Regular Army 12-month moving averages. Each line represents a 12-month moving average (ie, each respective dot reports the rate for the prior 12-month period).
Bivariate Predictors of Suicide and Accident Deaths
Table 2 summarizes selected overall distributions and bivariate associations of predictors with suicide rates overall and by deployment history. (Information on distributions within deployment categories is available on request from the corresponding author.) We focus on overall suicide risk within categories of each predictor based on the fact that none of the interactions between predictors and time within deployment category in predicting suicide were statistically significant at the .05 level of significance.
Table 2.
Bivariate Predictors of Suicide Deaths Among Regular Army Soldiers, 2004–2009
| Predictor | Regular Army, % | Suicide Deaths per 100 000 Person-Years | Suicide Deaths per 100 000 Person-Years by Deployment Category |
|||||
|---|---|---|---|---|---|---|---|---|
| Never | No. | Current | No. | Previous | No. | |||
| Total | … | 18.5 | 15.6 | 193 | 20.0 | 140 | 20.5 | 236 |
| Sex | ||||||||
| Women | 14.0 | 6.5a | 5.9b | 14 | 13.2 | 9 | 4.0b | 5c |
| Men | 86.0 | 20.4 | 18.0 | 179 | 20.8 | 131 | 22.5 | 231 |
| Age, y | ||||||||
| 17–20 | 12.5 | 23.4b | 15.7 | 45 | 46.7b | 32 | 43.0b | 13d |
| 21–24 | 26.6 | 23.2 | 19.1 | 64 | 24.5 | 54 | 27.3 | 72 |
| 25–29 | 22.9 | 19.4 | 15.2 | 33 | 16.2 | 29 | 24.2 | 75c |
| 30–44 | 34.5 | 12.9 | 12.6 | 44 | 10.2 | 22 | 14.2 | 71 |
| ≥45 | 3.5 | 14.1 | 15.3 | 7 | 20.4 | 3 | 10.8 | 5 |
| Marital status | ||||||||
| Married | 57.1 | 16.6a | 16.1 | 94 | 12.7b | 51 | 19.1 | 148c |
| Unmarried with dependents | 7.1 | 15.6 | 12.3 | 11 | 9.5 | 4 | 21.9 | 19 |
| Unmarried without dependents | 35.8 | 21.9 | 15.7 | 88 | 33.2 | 85 | 24.0 | 69d |
|
Race/Ethnicity (Not Mutually Exclusive) | ||||||||
| White | ||||||||
| No | 30.1 | 14.3b | 12.0e | 43 | 15.5 | 31 | 16.0e | 59 |
| Yes | 69.9 | 20.2 | 17.1 | 150 | 21.9 | 109 | 22.6 | 177c |
| Black | ||||||||
| No | 78.3 | 20.0b | 17.1e | 166 | 22.0e | 122 | 22.0e | 195c |
| Yes | 21.7 | 12.8 | 10.3 | 27 | 12.6 | 18 | 15.5 | 41 |
| Native American | ||||||||
| No | 99.0 | 18.3e | 15.5 | 189 | 19.8 | 137 | 20.3 | 232c |
| Yes | 1.0 | 35.9 | 31.3 | 4 | 43.9 | 3 | 36.4 | 4 |
| Asian/Pacific | ||||||||
| No | 95.6 | 18.3 | 15.5 | 182 | 19.9 | 133 | 20.4 | 225c |
| Yes | 4.4 | 21.5 | 19.2 | 11 | 23.6 | 7 | 23.0 | 11 |
| Hispanic | ||||||||
| No | 89.4 | 18.7 | 15.9 | 176 | 20.4 | 126 | 20.8 | 215c |
| Yes | 10.6 | 16.0 | 13.4 | 17 | 17.5 | 14 | 17.6 | 21 |
| Religion | ||||||||
| Christian | ||||||||
| Catholic | 20.2 | 15.2b | 13.1a | 31 | 17.0e | 24 | 16.3b | 40 |
| Baptist | 18.2 | 11.6 | 9.5 | 20 | 12.4 | 15 | 13.0 | 30 |
| Other Protestant | 16.8 | 15.3 | 12.1 | 25 | 13.1 | 15 | 19.8 | 39 |
| Other Christian | 17.7 | 19.7 | 17.1 | 41 | 25.0 | 32 | 19.5 | 35 |
| Other religion | 1.9 | 28.4 | 22.9 | 6 | 31.5 | 4 | 33.5 | 7 |
| No religion | 20.6 | 25.5 | 21.2 | 53 | 26.9 | 40 | 29.3 | 69 |
| Religion unknown | 4.5 | 30.8 | 26.3 | 17 | 30.5 | 10 | 37.7 | 16 |
| Education | ||||||||
| <High school | 1.7 | 20.8b | 15.1b | 4 | 35.1 | 4 | 20.2b | 3 |
| High school diploma or GED | 65.5 | 19.3 | 15.6 | 120 | 20.4 | 99 | 22.1 | 170c |
| Some college | 5.2 | 11.8 | 9.7 | 6 | 13.1 | 4 | 13.2 | 9 |
| College graduate, masters, or PhD | 19.1 | 9.8 | 10.4 | 26 | 9.2 | 10 | 9.5 | 22 |
| Alternative educational certificate | 8.4 | 35.5 | 29.3 | 37 | 36.2 | 23 | 46.1 | 32 |
| AFQT Category | ||||||||
| I | 4.3 | 22.9b | 14.1a | 9 | 43.8 | 12 | 22.6b | 9c |
| II | 27.2 | 22.9 | 16.2 | 58 | 26.3 | 50 | 28.7 | 84f |
| IIIA | 22.4 | 18.8 | 15.5 | 42 | 16.6 | 27 | 23.6 | 61 |
| IIIB | 26.1 | 17.9 | 18.8 | 58 | 18.0 | 35 | 16.9 | 51 |
| IV/V | 2.8 | 15.1 | 6.1 | 2 | 19.0 | 4 | 21.4 | 7 |
| Missing | 0.8 | 33.5 | 11.9 | 1 | 52.0 | 3 | 41.4 | 4 |
| Officer (no AFQT) | 16.4 | 10.3 | 12.0 | 23 | 9.2 | 9 | 9.2 | 20 |
| Army Experiences | ||||||||
| Accession waiver status | ||||||||
| No | 57.6 | 23.0b | 18.5b | 138 | 23.6b | 104 | 28.3b | 167d |
| Yes | 5.3 | 25.8 | 18.0 | 16 | 38.6 | 14 | 31.7 | 12 |
| Missing waiver data | 37.1 | 10.3 | 9.7 | 39 | 10.0 | 22 | 10.9 | 57 |
| Current rank | ||||||||
| E1–E2 | 10.4 | 26.0b | 18.9a | 54 | 83.1b | 19 | 86.7b | 10d |
| E3 | 11.9 | 27.5 | 22.5 | 54 | 32.3 | 30 | 48.5 | 17c |
| E4 | 23.2 | 23.7 | 14.4 | 31 | 24.7 | 53 | 29.9 | 85f |
| E5–E9 | 38.2 | 13.9 | 10.2 | 31 | 10.7 | 29 | 17.2 | 104f |
| Warrant officer | 2.6 | 11.2 | 24.2 | 5 | 5.7 | 1 | 7.1 | 3 |
| Commissioned officer | 13.8 | 10.1 | 10.5 | 18 | 10.0 | 8 | 9.7 | 17 |
| History of demotions in past 2 y | ||||||||
| No | 95.3 | 17.4b | 15.1e | 178 | 18.2b | 120 | 19.4b | 213c |
| Yes | 4.7 | 40.1 | 27.5 | 15 | 50.6 | 20 | 45.4 | 23 |
| Stop loss orders | ||||||||
| Never | 89.5 | 18.1 | 15.1b | 181 | 20.6 | 117 | 20.3 | 201f |
| Currently | 4.2 | 20.9 | 21.8 | 4 | 19.9 | 14 | 22.3 | 9 |
| Previously | 6.3 | 22.1 | 60.9 | 8 | 15.2 | 9 | 21.3 | 26f |
| Length of Army service, y | ||||||||
| ≤1 | 6.7 | 8.8b | 8.8b | 18 | 0.0b | 0 | NA | 0 |
| 2 | 6.4 | 25.3 | 20.1 | 36 | 73.7 | 13 | 100.0 | 1d |
| 3 | 12.0 | 25.0 | 23.5 | 53 | 28.6 | 32 | 23.5 | 8 |
| 4 | 11.1 | 24.2 | 17.8 | 20 | 29.3 | 33 | 25.4 | 30 |
| 5 | 16.1 | 23.1 | 15.9 | 17 | 17.8 | 26 | 29.4 | 72 |
| 6–10 | 19.9 | 17.9 | 13.8 | 18 | 11.3 | 17 | 22.6 | 75c |
| 11–19 | 22.1 | 11.4 | 10.7 | 22 | 9.7 | 13 | 12.6 | 43 |
| ≥20 | 5.7 | 12.6 | 12.8 | 9 | 24.0 | 6 | 8.8 | 7 |
| Deployment category | ||||||||
| Never | 40.0 | 15.6e | NA | NA | NA | NA | NA | NA |
| Currently | 22.6 | 20.0 | NA | NA | NA | NA | NA | NA |
| Previously | 37.3 | 20.5 | NA | NA | NA | NA | NA | NA |
| No.g | NA | 569 | 193 | 140 | NA | 236 | NA | |
Abbreviations: AFQT, Armed Forces Qualification Test; NA, not applicable; GED, general equivalency diploma.
Significant association between the predictor and suicide at the .01 level (2-sided test).
Significant association between the predictor and suicide at the .001 level (2-sided test).
Significant difference in the association between the predictor and suicide across the 3 deployment categories at the .05 level (2-sided test).
Significant difference in the association between the predictor and suicide across the 3 deployment categories at the .001 level (2-sided test).
Significant association between the predictor and suicide at the .05 level (2-sided test).
Significant difference in the association between the predictor and suicide across the 3 deployment categories at the .01 level (2-sided test).
The reported numbers are the numbers of suicide deaths among Regular Army soldiers, 2004–2009.
Women have consistently lower suicide risk than men; however, the sex difference narrows substantially during deployment because of a disproportionately greater increase in risk for deployed men than women soldiers. The youngest soldiers have markedly elevated suicide risk during and after deployment but not among those never deployed. Married soldiers and those with other dependents have significantly lower suicide risk than unmarried soldiers without dependents during deployment but not among either the never deployed or previously deployed. Suicide risk varies significantly by religious affiliation.
Suicide risk is inversely associated with educational attainment, with the highest risk among the small fraction of soldiers who did not receive either a high school diploma or general equivalency diploma and the somewhat larger group with an alternative education certificate, which includes vocational training and other alternate schooling. However, this association is not significant during deployment. Suicide risk is also inversely related to AFQT categories, but this association is most pronounced during deployment.
While accession waivers are significantly associated with suicide risk in the Army overall, this is mainly an artifact of missing waiver data for almost all officers and for most soldiers with more than 5 years of Army service, both groups with low suicide risk. Within the subsample of enlisted soldiers with 5 or fewer years of service, which covers the difficult recruiting periods associated with the “surge” in Iraq and for which waiver data were essentially complete, no statistically significant association was found between suicide risk and receiving a medical, substance use, or conduct waiver.
Among enlisted soldiers, suicide is inversely related to rank. Indeed, suicide rates among currently and previously deployed E1 and E2 (junior enlisted) soldiers are among the highest listed in Table 2. Suicide rates are also consistently elevated among soldiers who were demoted within the prior 2 years across all deployment categories. Suicide risk for soldiers serving under a current stop loss order does not differ consistently from that for other soldiers. However, the small number of never-deployed soldiers who previously served under a stop loss order, a group that by definition includes only soldiers who chose to reenlist after having been released from a stop loss order, have significantly elevated suicide risk. Finally, suicide risk is generally inversely related to length of Army service, with particularly high risk among currently and previously deployed soldiers in their first 2 years of service.
Correlates of accident death are similar to those for suicide death (Table 3). General patterns differ for suicide and accident deaths mainly with respect to the AFQT, where there is no consistent pattern in accident death risk across categories, and for soldiers currently serving under a stop loss order, which is associated with significantly elevated risk of accident death. The high risk of accident death among warrant officers during deployment is likely because of hazards associated with their duty assignments (eg, helicopter pilots).
Table 3.
Bivariate Predictors of Accident Deaths Among Regular Army Soldiers, 2004–2009
| Predictor | Regular Army, % | Accident Deaths per 100 000 Person-Years | Accident Deaths per 100 000 Person-Years by Deployment Category | |||||
|---|---|---|---|---|---|---|---|---|
| Never | No. | Current | No. | Previous | No. | |||
| Total | … | 43.2 | 37.9 | 468 | 47.0 | 328 | 46.5 | 535 |
| Sex | ||||||||
| Women | 14.0 | 15.0a | 18.5a | 44 | 11.7a | 8 | 10.3a | 13 |
| Men | 86.0 | 47.8 | 42.6 | 424 | 50.8 | 320 | 41.1 | 422b |
| Age, y | ||||||||
| 17–20 | 12.5 | 58.4a | 48.5a | 139 | 75.9a | 52 | 112.5a | 34c |
| 21–24 | 26.6 | 60.2 | 54.9 | 184 | 52.6 | 116 | 73.5 | 194d |
| 25–29 | 22.9 | 43.7 | 33.2 | 72 | 50.8 | 91 | 47.0 | 146d |
| 30–44 | 34.5 | 25.8 | 17.5 | 61 | 31.6 | 68 | 29.2 | 146d |
| ≥45 | 3.5 | 26.2 | 26.2 | 12 | 6.8 | 1 | 32.5 | 15 |
| Marital status | ||||||||
| Married | 57.1 | 34.3a | 26.9a | 157 | 38.9a | 156 | 37.5a | 291c |
| Unmarried with dependents | 7.1 | 43.5 | 30.2 | 27 | 50.1 | 21 | 54.1 | 47b |
| Unmarried without dependents | 35.8 | 57.2 | 50.6 | 284 | 59.0 | 151 | 68.4 | 197d |
|
Race/Ethnicity (Not Mutually Exclusive) | ||||||||
| White | ||||||||
| No | 30.1 | 33.2a | 30.4e | 109 | 31.9a | 64 | 36.7a | 135 |
| Yes | 69.9 | 47.5 | 41.0 | 359 | 53.0 | 264 | 51.1 | 400c |
| Black | ||||||||
| No | 78.3 | 45.1e | 39.8f | 386 | 50.7e | 282 | 47.3 | 420d |
| Yes | 21.7 | 36.3 | 31.2 | 82 | 32.2 | 46 | 43.5 | 115b |
| Native American | ||||||||
| No | 99.0 | 43.0 | 37.8 | 461 | 46.7 | 323 | 46.3 | 528d |
| Yes | 1.0 | 62.0 | 54.7 | 7 | 73.2 | 5 | 63.6 | 7 |
| Asian/Pacific | ||||||||
| No | 95.6 | 43.9e | 38.5 | 453 | 47.7 | 319 | 47.4f | 523c |
| Yes | 4.4 | 26.7 | 26.2 | 15 | 30.3 | 9 | 25.1 | 12 |
| Hispanic | ||||||||
| No | 89.4 | 43.7 | 38.6 | 427 | 46.2 | 286 | 47.7 | 492d |
| Yes | 10.6 | 38.7 | 32.4 | 41 | 52.6 | 42 | 36.0 | 43 |
| Religion | ||||||||
| Christian | ||||||||
| Catholic | 20.2 | 38.8e | 30.7 | 73 | 53.8 | 76 | 37.9e | 93d |
| Baptist | 18.2 | 42.4 | 40.5 | 85 | 40.6 | 49 | 45.1 | 104 |
| Other Protestant | 16.8 | 40.2 | 34.4 | 71 | 47.1 | 54 | 42.2 | 83 |
| Other Christian | 17.7 | 47.2 | 43.0 | 103 | 43.8 | 56 | 55.1 | 99 |
| Other religion | 1.9 | 16.7 | 19.1 | 5 | 15.7 | 2 | 14.4 | 3 |
| No religion | 20.6 | 47.7 | 44.0 | 110 | 46.4 | 69 | 52.6 | 124 |
| Religion unknown | 4.5 | 51.5 | 32.5 | 21 | 67.1 | 22 | 68.3 | 29b |
| Education | ||||||||
| <High school | 1.7 | 62.5a | 26.4a | 7 | 105.3a | 12 | 94.2 | 14d |
| High school diploma or GED | 65.5 | 47.5 | 42.3 | 325 | 51.2 | 248 | 50.3 | 386b |
| Some college | 5.2 | 34.9 | 29.0 | 18 | 32.9 | 10 | 41.1 | 28 |
| College graduate, masters, or PhD | 19.1 | 18.8 | 14.0 | 35 | 29.4 | 32 | 19.1 | 44d |
| Alternative educational certificate | 8.4 | 66.4 | 65.8 | 83 | 40.9 | 26 | 90.8 | 63d |
| AFQT Category | ||||||||
| I | 4.3 | 34.3 | 31.3 | 20 | 25.6 | 7 | 45.3 | 18d |
| II | 27.2 | 45.7 | 37.5 | 134 | 52.6 | 100 | 51.3 | 150b |
| IIIA | 22.4 | 48.4 | 44.9 | 122 | 40.0 | 65 | 57.3 | 148b |
| IIIB | 26.1 | 48.3 | 44.1 | 136 | 53.5 | 104 | 49.4 | 149 |
| IV/V | 2.8 | 37.1 | 49.2 | 16 | 28.6 | 6 | 30.5 | 10 |
| Missing | 0.8 | 67.0 | 71.1 | 6 | 34.7 | 2 | 82.8 | 8 |
| Officer (no AFQT) | 16.4 | 25.7 | 17.8 | 34 | 45.1 | 44 | 24.0 | 52c |
| Army Experiences | ||||||||
| Accession waiver | ||||||||
| No | 57.6 | 53.5a | 47.0a | 350 | 52.8e | 233 | 62.1a | 367c |
| Yes | 5.3 | 49.1 | 43.9 | 39 | 46.9 | 17 | 63.5 | 24 |
| Missing waiver data | 37.1 | 26.3 | 19.7 | 79 | 35.3 | 78 | 27.5 | 144c |
| Current rank | ||||||||
| E1–E2 | 10.4 | 71.7a | 65.3a | 186 | 74.3a | 17 | 225.4a | 26c |
| E3 | 11.9 | 55.2 | 46.3 | 111 | 64.6 | 60 | 91.3 | 32c |
| E4 | 23.2 | 53.3 | 33.9 | 73 | 49.9 | 107 | 70.7 | 201c |
| E5–E9 | 38.2 | 33.0 | 21.2 | 64 | 37.0 | 100 | 37.1 | 224c |
| Warrant officer | 2.6 | 72.1 | 53.1 | 11 | 130.9 | 23 | 57.0 | 24d |
| Commissioned officer | 13.8 | 16.9 | 13.5 | 23 | 26.3 | 21 | 16.0 | 28 |
| History of demotions in past 2 y | ||||||||
| No | 95.3 | 40.5a | 36.0a | 425 | 44.3a | 292 | 42.9a | 472d |
| Yes | 4.7 | 98.1 | 78.9 | 43 | 91.1 | 36 | 124.3 | 63 |
| Stop loss orders | ||||||||
| Never | 89.5 | 42.6e | 37.8 | 455 | 47.5 | 270 | 45.6e | 451d |
| Currently | 4.2 | 62.0 | 54.5 | 10 | 51.1 | 36 | 84.2 | 34 |
| Previously | 6.3 | 38.6 | 22.8 | 3 | 37.1 | 22 | 41.0 | 50 |
| Length of Army service, y | ||||||||
| ≤1 | 6.7 | 21.4a | 21.5a | 44 | 0.0f | 0 | NA | 0 |
| 2 | 6.4 | 61.3 | 61.5 | 110 | 56.7 | 10 | 100.0 | 1 |
| 3 | 12.0 | 61.4 | 59.9 | 135 | 56.3 | 63 | 88.2 | 30 |
| 4 | 11.1 | 63.0 | 53.5 | 60 | 53.3 | 60 | 81.4 | 96d |
| 5 | 16.1 | 50.4 | 30.8 | 33 | 52.8 | 77 | 57.6 | 141d |
| 6–10 | 19.9 | 42.3 | 25.4 | 33 | 47.8 | 72 | 46.4 | 154d |
| 11–19 | 22.1 | 25.7 | 21.0 | 43 | 30.5 | 41 | 26.6 | 91d |
| ≥20 | 5.7 | 21.2 | 14.3 | 10 | 20.0 | 5 | 27.7 | 22 |
| Deployment category | ||||||||
| Never | 40.0 | 37.9e | NA | NA | NA | NA | NA | NA |
| Currently | 22.6 | 47.0 | NA | NA | NA | NA | NA | NA |
| Previously | 37.3 | 46.5 | NA | NA | NA | NA | NA | NA |
| No.g | NA | 1331 | NA | NA | 328 | 535 | NA | |
Abbreviations: AFQT, Armed Forces Qualification Test; NA, not applicable; GED, general equivalency diploma.
Accident death rate differs significantly by deployment category for given value of characteristic (P ≤ .001, χ2 test).
Significant difference in the association between the characteristic and accident death rate across the 3 deployment categories at the .05 level (2-sided test).
Significant difference in the association between the characteristic and accident death rate across the 3 deployment categories at the .001 level (2-sided test).
Significant difference in the association between the characteristic and accident death rate across the 3 deployment categories at the .01 level (2-sided test).
Accident death rate differs significantly by deployment category for given value of characteristic (P ≤ .01, χ2 test).
Accident death rate differs significantly by deployment category for given value of characteristic (P ≤ .05, χ2 test).
The reported numbers are the numbers of accident deaths among Regular Army soldiers, 2004–2009.
Compositional Effects
Although levels of almost all predictors listed in Table 2 vary significantly across calendar time during the study period, there were no significant interactions between these predictors and calendar time in predicting suicide. (Detailed results are available on request from the corresponding author.) Multivariate analyses evaluated whether compositional changes in predictors (eg, the increasing proportions of soldiers having accession waivers) helped explain the rising Army suicide rate (Table 4). Because no corresponding trend was found in accident mortality during this period, we did not conduct simulations for that outcome. The first rows in Table 4 list the actual suicide rates and the numbers of suicides in 2004–2005, 2006–2007, and 2008–2009. The remainder of the table lists predicted suicide rates and the numbers in 2006–2007 and 2008–2009 under the assumption of compositional consistency with 2004–2005. The results show that only 11% of the increase in suicide rates between 2004–2005 and 2006–2007 and 10% of the increase between 2004–2005 and 2008–2009 can be attributable to increases in accession waivers or other compositional changes in the predictors considered herein.
Table 4.
Simulated Effect of Changes in Regular Army Composition on Suicide Rates
| Variable | 2004–2005 | 2006–2007 | 2008–2009 |
|---|---|---|---|
| Actual Suicide Death Rate | |||
| Rate per 100 000 person-years of active duty Regular Army service | 12.1 | 18.1 | 24.5 |
| No. | 120 | 182 | 267 |
| Predicted Suicide Death Rate Based on 2004–2005 Army Entry Characteristicsa | |||
| Simulated rate per 100 000 person-years of active duty Regular Army service | NA | 17.4 | 23.2 |
| Simulated No. | NA | 175 | 253 |
| Change vs actual, % | NA | −3.9 | −5.1 |
| Predicted Suicide Death Rate Based on 2004–2005 Army Entry and Experience Characteristicsb | |||
| Simulated rate per 100 000 person-years of active duty Regular Army service | NA | 16.9 | 23.5 |
| Simulated No. | NA | 170 | 256 |
| Change vs actual, % | NA | −6.7 | −4.0 |
Abbreviations: AFQT, Armed Forces Qualification Test; NA, not applicable.
Includes sex, age at Army entry, marital status, race/ethnicity, religion, education, accession waiver status, and AFQT category (based on Table 2 except for age at Army entry).
Includes sex, current age, marital status, race/ethnicity, religion, education, accession waiver status, AFQT category, current rank, recent demotions, length of Army service, and deployment category (based on Table 2).
Discussion
To our knowledge, this is the first report of suicide trends by deployment category during a period when the Army suicide rate increased above the civilian rate. While we found suicide risk to be highest during deployment, the rise in the suicide rate was found not only among the currently and previously deployed but also among the never deployed. We also found suicide risk to be significantly associated with a number of sociodemographic characteristics and Army experiences. Some of these associations replicate prior findings among military servicemembers such as the increased risk associated with being a man, white race/ethnicity, and junior enlisted rank.4,9,12–14 Other associations reported herein are new, including the disproportionate increase in suicide risk among deployed women soldiers, soldiers demoted in the past 2 years, and soldiers without either a high school diploma or general equivalency diploma. These associations merit additional study. Contrary to expectations, we found no consistent associations of either stop loss orders or accession waivers with suicide. The absence of an association of accession waivers with suicide is especially striking given that other research has shown that soldiers with accession waivers have elevated rates of a number of adverse behavioral outcomes (positive alcohol or drug test results and behavioral misconduct separations).9
There is only one result reported herein that would appear to differ from previous studies: our finding of elevated suicide risk among currently and previously deployed soldiers differs from the finding of no association between deployment history and suicide in a recent report from the Millennium Cohort Study (MCS).15 However, two differences between the MCS and HADS designs might account for this discrepancy in the results. First, the MCS is a study of all military services, while the HADS focuses on the Army. The failure to find an association between deployment history and suicide in the MCS was reported only for the total sample. This means that an association might have existed in the Army sub-sample, which was underpowered for separate analysis. Second, the MCS is based on a survey sample with a low response rate. No data were presented in the MCS report to show that the suicide rate in the sample was the same as in the population. This is an important limitation of the MCS report because the possibility of bias in this critical outcome variable is plausible based on prior research showing that people with emotional problems have low rates of participation in surveys.16,17 The HADS has no such limitation, in comparison, because it is based on population data rather than on survey data.
We found that temporal patterns in accident mortality differed from those for suicide but that the individual-level sociodemographic and Army career predictors of accident death and suicide death were generally similar. This may seem surprising because accident typically connotes exogenous factors. However, the similar findings raise the possibility of some common etiology. This possibility is being investigated in ongoing Army STARRS analyses.
While variation across individuals in sociodemographics and Army experiences helped explain overall suicide risk between 2004 and 2009, compositional changes in these predictors and in accession waivers over time explained little of the rise in Army suicides. However, the exploratory models reported herein were limited in the scope and granularity of the domains of risk and resilience that they included. As a result, we plan to expand the set of predictors considerably in future analyses as additional types of data become available. We will be particularly interested in information on mental and physical health care treatment data obtained from the Military Health System.
The present study was limited not only in working with an incomplete set of the administrative systems that will eventually be included in the HADS but also in excluding activated US Army National Guard (USARNG) and US Army Reserve (USAR) soldiers. This was necessary because the military data systems feeding the HADS contain data only for USARNG and USAR soldiers related to their periods of active duty military service. The HADS consequently contains virtually no data about risk and resilience factors related to the civilian life experiences of USARNG and USAR soldiers. However, the Army and Department of Defense have initiatives under way to expand the scope of data available on USARNG and USAR soldiers. A final noteworthy limitation is that the analyses reported herein were all based on bivariate associations involving rather coarse measures (eg, a simple 3-category measure of deployment history rather than more fine-grained measures that distinguish the number of deployments, recency of deployments, and time between deployments). This was done to provide preliminary data on overall associations of potentially important variables before attempting to adjust for associations among predictors and for variation in associations of some predictors with suicide as a function of other predictors. Future HADS analyses will investigate multivariate associations and will consider much more fine-grained variables.
Conclusions
Despite these limitations, the results reported herein provide useful preliminary information about patterns and basic sociodemographic and Army experience predictors of Army suicides in the years leading up to the initiation of the Army STARRS. The results debunk several hypotheses that previously were considered plausible about the effects of waivers, stop loss orders, and compositional changes in the characteristics of soldiers in accounting for the suicide trend observed during the study. They demonstrate clearly the existence of important sociodemographic and Army career correlates of suicide risk, some of them not previously documented, that remained stable in their associations with suicide during this period, despite the rising suicide rate over the first decade of the new millennium. These results set the stage for more in-depth analyses aimed at helping the Army target both high-risk soldiers and high-risk situations, as well as at developing, implementing, and evaluating preventive interventions to reverse the rising Army suicide rate.
Supplementary Material
Acknowledgments
Funding/Support: The Army STARRS was sponsored by the Department of the Army and funded under cooperative agreement U01MH087981 with the National Institute of Mental Health, National Institutes of Health, US Department of Health and Human Services.
Role of the Sponsor: As a cooperative agreement, scientists employed by the National Institute of Mental Health (Drs Schoenbaum and Colpe) and Army liaisons and consultants (Dr Cox and Steven Cersovsky, MD, MPH) collaborated to develop the study protocol and data collection instruments, supervise data collection, plan and supervise data analyses, interpret results, and prepare reports. Although a draft of this manuscript was submitted to the Army and the National Institute of Mental Health for review and comment before submission, this was with the understanding that comments would only be advisory.
Author Contributions
Dr Schoenbaum had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Study concept and design: Schoenbaum, Heeringa, Ursano.
Acquisition, analysis, or interpretation of data: All authors.
Drafting of the manuscript: Schoenbaum, Ursano, Cox.
Critical revision of the manuscript for important intellectual content: Schoenbaum, Kessler, Gilman, Colpe, Heeringa, Stein, Cox.
Statistical analysis: Schoenbaum, Heeringa.
Obtained funding: Schoenbaum, Kessler, Heeringa, Ursano.
Administrative, technical, or material support: Schoenbaum, Kessler, Colpe, Heeringa, Stein, Ursano.
Study supervision: Schoenbaum, Kessler.
Conflict of Interest Disclosures
In the past 5 years, Dr Kessler has been a consultant for Eli Lilly & Company, Glaxo Inc, Integrated Benefits Institute, Ortho-McNeil Janssen Scientific Affairs, Pfizer Inc, sanofi-aventis, Shire US Inc, and Transcept Pharmaceuticals Inc and has served on advisory boards for Johnson & Johnson. Dr Kessler has had research support for his epidemiologic studies during this period from Eli Lilly & Company, EPI-Q, GlaxoSmithKline, Ortho-McNeil Janssen Scientific Affairs, sanofi-aventis, Shire US Inc, and Walgreens Co. Dr Kessler owns a 25% share in DataStat Inc. In the past 3 years, Dr Stein has been a consultant for Healthcare Management Technologies and had research support for pharmacologic imaging studies from Janssen. No other disclosures were reported.
Group Information
The Army STARRS coprincipal investigators were Robert J. Ursano, MD, Uniformed Services University of the Health Sciences, Bethesda, Maryland; and Murray B. Stein, MD, MPH, University of California, San Diego, La Jolla, and Veterans Affairs San Diego Healthcare System, San Diego. The site principal investigators were Steven G. Heeringa, PhD, University of Michigan, Ann Arbor; and Ronald C. Kessler, PhD, Harvard Medical School, Boston, Massachusetts. The National Institute of Mental Health (Bethesda, Maryland) collaborating scientists were Lisa J. Colpe, PhD, MPH, and Michael Schoenbaum, PhD. United States Army Public Health Command (Aberdeen Proving Ground, Maryland) Army liaisons and consultants were Steven Cersovsky, MD, MPH, and Kenneth L. Cox, MD, MPH. Other team members were Pablo A. Aliaga, MA, Uniformed Services University of the Health Sciences; David M. Benedek, MD, Uniformed Services University of the Health Sciences; Susan Borja, PhD, National Institute of Mental Health; Gregory G. Brown, PhD, University of California, San Diego; Laura Campbell-Sills, PhD, University of California, San Diego; Catherine L. Dempsey, PhD, MPH, Uniformed Services University of the Health Sciences; Richard Frank, PhD, Harvard Medical School; Carol S. Fullerton, PhD, Uniformed Services University of the Health Sciences; Nancy Gebler, MA, University of Michigan; Joel Gelernter, MD, Yale University, New Haven, Connecticut; Robert K. Gifford, PhD, Uniformed Services University of the Health Sciences; Stephen E. Gilman, ScD, Harvard School of Public Health; Marjan G. Holloway, PhD, Uniformed Services University of the Health Sciences; Paul E. Hurwitz, MPH, Uniformed Services University of the Health Sciences; Sonia Jain, PhD, University of California, San Diego; Tzu-Cheg Kao, PhD, Uniformed Services University of the Health Sciences; Karestan C. Koenen, PhD, Columbia University, New York, New York; Lisa Lewandowski-Romps, PhD, University of Michigan; Holly Herberman Mash, PhD, Uniformed Services University of the Health Sciences; James E. McCarroll, PhD, MPH, Uniformed Services University of the Health Sciences; Katie A. McLaughlin, PhD, Harvard Medical School; James A. Naifeh, PhD, Uniformed Services University of the Health Sciences; Matthew K. Nock, PhD, Harvard University; Rema Raman, PhD, University of California, San Diego; Nancy A. Sampson, BA, Harvard Medical School; Patcho Santiago, MD, MPH, Uniformed Services University of the Health Sciences; Michaelle Scanlon, MBA, National Institute of Mental Health; Jordan Smoller, MD, ScD, Harvard Medical School; Nadia Solovieff, PhD, Harvard Medical School; Michael L. Thomas, PhD, University of California, San Diego; Christina Wassel, PhD, University of Pittsburgh, Pittsburgh, Pennsylvania; and Alan M. Zaslavsky, PhD, Harvard Medical School.
Disclaimer
The contents are solely the responsibility of the authors and do not necessarily represent the views of National Institute of Mental Health, the US Department of Health and Human Services, the Department of the Army, or the Department of Defense.
Additional Information
Additional information on the Army STARRS, including a complete list of publications from the study, can be found at http://www.armystarrs.org.
Additional Contributions
Monica M. Wahi, MPH, CPH (US Army Research Institute of Environmental Medicine), assisted with the use of Army and Department of Defense data via the Total Army Injury and Health Outcomes Database (http://www.usariem.army.mil/index.cfm/about/divisions/mpd/taihod). We thank the other staff members of the institute (http://www.usariem.army.mil).
References
- 1.Kuehn BM. Soldier suicide rates continue to rise: military, scientists work to stem the tide. JAMA. 2009;301(11):1111. doi: 10.1001/jama.2009.342. 1113. [DOI] [PubMed] [Google Scholar]
- 2.Kessler RC, Colpe LJ, Fullerton CS, et al. Design of the Army Study to Assess Risk and Resilience in Servicemembers (Army STARRS) Int J Methods Psychiatr Res. 2013;22(4):267–275. doi: 10.1002/mpr.1401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Bachynski KE, Canham-Chervak M, Black SA, Dada EO, Millikan AM, Jones BH. Mental health risk factors for suicides in the US Army, 2007–8. Inj Prev. 2012;18(6):405–412. doi: 10.1136/injuryprev-2011-040112. [DOI] [PubMed] [Google Scholar]
- 4.Black SA, Gallaway MS, Bell MR, Ritchie EC. Prevalence and risk factors associated with suicides of Army soldiers 2001–2009. Mil Psychol. 2011;23(4):433–451. [Google Scholar]
- 5.Braswell H, Kushner HI. Suicide, social integration, and masculinity in the U.S. military. Soc Sci Med. 2012;74(4):530–536. doi: 10.1016/j.socscimed.2010.07.031. [DOI] [PubMed] [Google Scholar]
- 6.Nock MK, Deming CA, Fullerton CS, et al. Suicide among soldiers: a review of psychosocial risk and protective factors. Psychiatry. 2013;76(2):97–125. doi: 10.1521/psyc.2013.76.2.97. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Trofimovich L, Skopp NA, Luxton DD, Reger MA. Health care experiences prior to suicide and self-inflicted injury, active component, US Armed Forces, 2001–2010. Med Surveill Monthly Rep. 2012;19(2):2–6. [PubMed] [Google Scholar]
- 8.Committee on Youth. Population and Military Recruitment: Physical, Medical, and Mental Health Standards, National Research Council: Assessing Fitness for Military Enlistment: Physical, Medical, and Mental Health Standards. Washington, DC: National Academy Press; 2006. [Google Scholar]
- 9.Gallaway MS, Bell MR, Lagana-Riordan C, Fink DS, Meyer CE, Millikan AM. The association between US Army enlistment waivers and subsequent behavioral and social health outcomes and attrition from service. Mil Med. 2013;178(3):261–266. doi: 10.7205/MILMED-D-12-00316. [DOI] [PubMed] [Google Scholar]
- 10.Schlesselman JJ. Case-Control Studies: Design, Conduct, Analysis. Oxford, England: Oxford University Press; 1982. [Google Scholar]
- 11.Cox DR. Regression models and life-tables. J R Stat Soc B. 1972;34(2):187–220. [Google Scholar]
- 12.Bush NE, Reger MA, Luxton DD, et al. Suicides and suicide attempts in the U.S. military, 2008–2010. Suicide Life Threat Behav. 2013;43(3):262–273. doi: 10.1111/sltb.12012. [DOI] [PubMed] [Google Scholar]
- 13.Hyman J, Ireland R, Frost L, Cottrell L. Suicide incidence and risk factors in an active duty US military population. Am J Public Health. 2012;102(suppl 1):S138–S146. doi: 10.2105/AJPH.2011.300484. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Logan J, Skopp NA, Karch D, Reger MA, Gahm GA. Characteristics of suicides among US army active duty personnel in 17 US states from 2005 to 2007. Am J Public Health. 2012;102(suppl 1):S40–S44. doi: 10.2105/AJPH.2011.300481. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.LeardMann CA, Powell TM, Smith TC, et al. Risk factors associated with suicide in current and former US military personnel. JAMA. 2013;310(5):496–506. doi: 10.1001/jama.2013.65164. [DOI] [PubMed] [Google Scholar]
- 16.Badawi MA, Eaton WW, Myllyluoma J, Weimer LG, Gallo J. Psychopathology and attrition in the Baltimore ECA 15-year follow-up 1981–1996. Soc Psychiatry Psychiatr Epidemiol. 1999;34(2):91–98. doi: 10.1007/s001270050117. [DOI] [PubMed] [Google Scholar]
- 17.Eaton WW, Anthony JC, Tepper S, Dryman A. Psychopathology and attrition in the epidemiologic catchment area surveys. Am J Epidemiol. 1992;135(9):1051–1059. doi: 10.1093/oxfordjournals.aje.a116399. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.