

Dear Editor-in-Chief
In professional soccer, the high rate of recurrence after a hamstring strain forces therapists to reflect about the most appropriate interventions in order to prevent subsequent occurrence of the same injury. In this context, the return-to-play (RTP) decision represents a key point. Even if there is little original RTP research, some authors proposed guidelines or suggestions to help clinicians to make an informed decision as to whether an injured athlete may safely return to practice and/or competition (Matheson et al., 2011; Herring et al., 2012). For example, a recent model developed by Creighton could clarify the processes that clinicians have to apply when making their decisions (Creighton et al., 2010).
The aim of this study was to analyse how clinicians decide, in their daily practice, when a hamstring injured professional soccer player is fully able to get back to competitive soccer activities.
In collaboration with the French and the Belgian Soccer Associations, 37 sports medicine physicians from French (League 1 and 2) and Belgian (1st division) male professional soccer clubs filled in a questionnaire. Physicians were asked to rank a list of RTP criteria after Hamstring Strain (HS) according to their actual daily medical practice and, for some criteria, to answer to detailed questions.
As represented in Table 1, a complete pain relief was considered as the most important criterion, presumably because pain would indicate incomplete healing. This strict rule of “no pain” is, in most cases, recommended by RTP experts, whatever the type of lesion (Kvist, 2004).
Table 1.
Answers to the following question: “Rank from 1 to 14 all the previous criteria according to the importance you assign to them in your daily medical practice (1 = the most important RTP criteria after hamstring strain – 14 = the less important RTP criteria after hamstring strain”).
| Ranking | Return-to-play criteria |
|---|---|
| 1 | Complete pain relief |
| 2 | Muscle strength performance |
| 3 | Subjective feeling reported by the player |
| 4 | Muscle flexibility |
| 5 | Specific soccer test performance |
| 6 | Respect of a theoretical period of competition break |
| 7 | Running analysis |
| 8 | Physical fitness |
| 9 | Balance control assessment |
| 10 | Medical imaging |
| 11 | Dynamic functional testing performance |
| 12 | Correction of potential sacroiliac or lumbar joint dysfunction |
| 13 | Other |
| 14 | Quadriceps – Hamstrings EMG analysis |
Muscle strength performance assessment was also considered as an essential RTP criterion. This result is not surprising, as it is proven that a muscle strength abnormality increases HS recurrence (Croisier et al., 2008). However, the way to highlight a muscular abnormality appears sometimes very different among professional soccer clubs physicians: as represented in Figure 1, there is a lack of consensus about the choice of the assessment device (isokinetics or other), the elements taken in consideration for determining that muscle strength is sufficient and the limits of strength differences between injured and uninjured sides.
Figure 1.
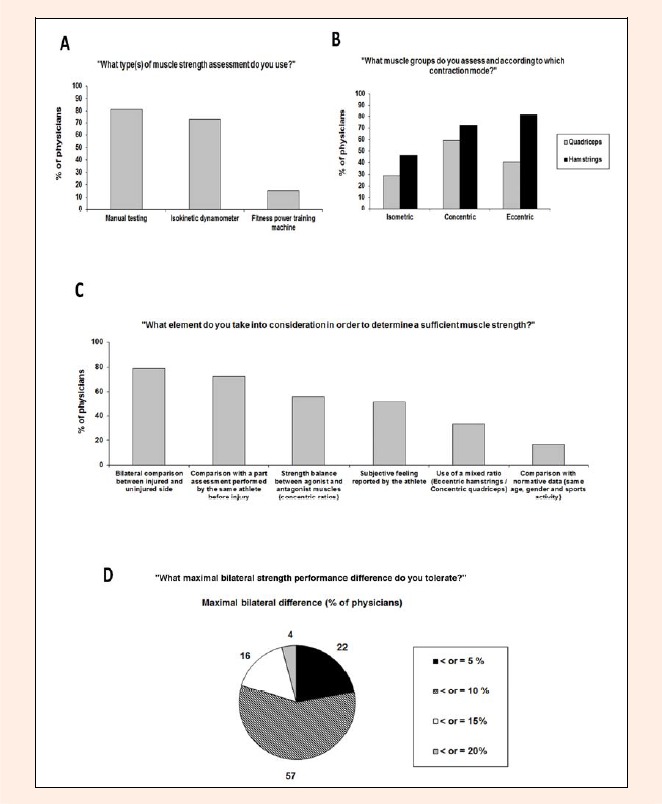
Muscle strength assessment - A) Type(s) of muscle strength assessment; B) Strength assessment: muscle groups and contraction modes; C) Elements taken in consideration for determining that muscle strength is sufficient; D) Limits of strength differences between injured and uninjured sides.
The subjective feeling reported by the player seemed important for the questioned physicians (third criterion in the ranking). Indeed, apprehension, fear and anxiety are associated with a higher risk of re-injury in addition to negative effects on performance (Glazer, 2009) and some authors insist on the importance of a conversation with the athlete about his mental readiness and confidence (fear of failure, fear of further injury) to return to play safely (Clover and Wall, 2010).
Hamstring muscle flexibility represented the fourth most important RTP criterion. Even if the relationship between a lack of flexibility and an increased risk of muscle injury remains unclear, some recent studies tended to establish a positive correlation between these two parameters. In a soccer players’ population, Witvrouw et al. (2003) demonstrated an association between a poor hamstring flexibility and the risk of developing a lesion on that muscle group.
In conclusion, we observed that nearly 80% of the questioned physicians used at least seven criteria to assess player’s ability to return to full sport. For some of these, notably muscle strength assessment, it appears that there is a lack of consensus about the choice of the assessment parameters and the limit values allowing doctors to authorize or forbid RTP. Even if the scientific evidence about this topic is not sufficient at the moment, some lines of thinking have been proposed, and their implementations are now possible. An effort could particularly be realized for applying, in actual medicine practice the elements which have been scientifically demonstrated to lower re-injury rate.
References
- Clover J., Wall J. (2010)Return-to-play criteria following sports injury. Clinics in Sports Medicine 29, 169-175 [DOI] [PubMed] [Google Scholar]
- Creighton D.W., Shrier I., Shultz R., Meeuwisse W.H., Matheson G.O. (2010)Return-to-play in sport: a decision-based model. Clinical Journal of Sports Medicine 20, 379-385 [DOI] [PubMed] [Google Scholar]
- Croisier J.L., Ganteaume S., Binet J., Genty M., Ferret J.M. (2008)Strength imbalances and prevention of hamstring injury in professional soccer players: a prospective study. American Journal of Sports Medicine 36, 1469-1475 [DOI] [PubMed] [Google Scholar]
- Glazer D.D. (2009)Development and preliminary validation of the Injury-Psychological Readiness to Return to Sport (I-PRRS) scale. Journal of Athletic Training 44, 185-189 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Herring S.A., Kibler W.B., Putukian M. (2012)The team physician and return-to-play issues: a consensus statement – 2012 update. Medicine and science in sports and exercise 44 (12), 2446-2448 [DOI] [PubMed] [Google Scholar]
- Kvist J. (2004)Rehabilitation following anterior cruciate ligament injury: current recommendations for sports participation. Sports Medicine 34, 269-280 [DOI] [PubMed] [Google Scholar]
- Matheson G.O., Shultz R., Bido J., Mitten M.J., Meeuwisse W.H., Shrier I. (2011)Return-to-play decisions: are they the team physician’s responsibility? Clinical Journal of Sports Medicine 21, 25-30 [DOI] [PubMed] [Google Scholar]
- Witvrouw E., Danneels L., Asselman P., D’Have T., Cambier D. (2003)Muscle flexibility as a risk factor for developing muscle injuries in male professional soccer players. A prospective study. American Journal of Sports Medicine 31, 41-46 [DOI] [PubMed] [Google Scholar]