

Abstract
Objective:
The aim of this investigation was to assess the efficacy of hydrochlorothiazide as a hypocalciuric diuretic on stone-free rate of renal pelvic calculi after extracorporeal shock wave lithotripsy (ESWL).
Materials and Methods:
A double-blind, placebo-controlled randomized clinical trial was conducted and 52 patients with renal pelvic calculi (diameter ≤2 cm) were enrolled from February 2010 to September 2010. ESWL protocol was performed by 2,500 shocks per session. The patients were randomized into two groups: (1) 26 patients who were given 25 mg hydrochlorothiazide twice daily; and (2) 26 patients who received placebo. The stone-free rate was defined as residual calculus size ≤4 mm in controlled ultrasound on 2nd week, 1 month and 3 months after ESWL.
Results:
19 (78%) of the first group and 9 (42.9%) of the second group were stone-free after one session of ESWL (P = 0.02). 88% of the group 1 and 47.8% of the group 2 were stone-free on 1 month after ESWL (P = 0.003); however, this effect of hydrochlorothiazide was not related to the patients' body mass index, age and gender. The accessory treatment procedures were applied in 24% of the group 1 compared with 19% of the group 2 during 3 months (P = 0.68). All patients in both groups were stone-free on 3 months following lithotripsy.
Conclusions:
Hydrochlorothiazide did not impact on the stone-free rate and using accessory procedure within 3 months; however, it decreased duration of stone-free status and number of ESWL sessions.
Keywords: Hydrochlorothiazide, kidney calculi, lithotripsy
INTRODUCTION
Urolithiasis represents as a health problem because of its high incidence and prevalence.[1] Residual fragments have been detected in 20-25% of the patients 3 months after lithotripsy treatment of the urolithiasis. It is found that a fragment has regrown if its size to be over one third of the original size. In addition, various data suggested that 10-20% of the fragmented calculi would increase in size.[2] In these patients, stone formation relapses were high, especially calcium stones[3] and predisposing factors of the stone formation must be detected and treated.[4]
Thiazide diuretics can reduce urinary excretion of calcium and are used to treat hypercalciuric calcium stones. On the other hand, adding a diuretic such a thiazide to extracorporeal shock wave lithotripsy (ESWL) may efficaciously improve ureteral stone fragmentation and its clearance rate.[5] Some authors believed that the hypocalciuric effect of the thiazides is not remarkable and also have an adverse impact including hypotension, hypocitraturia and hyperuricemia.[6]
In the present study, we intended to investigate the effect of adjunctive hydrochlorothiazide on renal pelvic calculi clearance rate and number of ESWL sessions following lithotripsy treatment.
MATERIALS AND METHODS
This prospective double-blind, placebo-controlled randomized clinical trial was conducted in the Urmia Imam-Khomeini Hospital, Iran. 61 patients were assessed for eligibility and a total of 52 patients with renal pelvic calculi (diameter ≤2 cm) were enrolled from February 2010 to September 2010. All patients were referred to our clinic of urology and were scheduled to undergo ESWL treatment. All of them signed informed consent forms prior to participating in the investigation.
They underwent taking history, complete physical examination and routine laboratory investigation including whole blood cell count, urinalysis, creatinine, prothrombin activity, bleeding time and coagulation time. In addition, all patients underwent ultrasonographic investigation and imaging with an X-ray intravenous urography or a computed tomography scan.
Inclusion criterion was single renal pelvic calculus ≤2 cm. Exclusion criteria included history of nephrolithiasis surgery, moderate to severe hydronephrosis and renal failure. The study was approved by our local ethics committee. We randomly assigned patients into two groups using the numbered envelopes. The groups were included: (1) 26 patients in the first group who received 25 mg of hydrochlorothiazide twice daily; (2) 26 patients who received placebo (same as main drug size, shape and taste). Patients, physicians who prescribed medications and biostatistician were blinded to the type of drugs. All patients took either hydrochlorothiazide or placebo from undergoing ESWL of kidney pelvic stone to 3 months after lithotripsy or time of stone clearance based on controlled ultrasonography. They were informed about drug adverse events without attention to the allocated group.
One surgeon performed ESWL procedure in all patients. The treatment protocol included about 2500 shock waves per patient in each session and energy of the shock was based on the patients' body mass index (BMI). A Dornier Sigma lithotripter (Dornier Med Tech, Munich, Germany) was used. All patients were advised to restrict dietary salt and increase intake fluids.
Stone-free status was defined as residual calculus size ≤4 mm in controlled ultrasonography at 2nd week, 1 month and 3 months after ESWL session. Moreover, based on our hypothesis, the stone-free rate at 3 months was considered as the primary endpoint. The data of the study were collected by a prepared questionnaire. A Chi-squared test and t-test were used as appropriate; P < 0.05 was considered statistically significant. Statistical analysis was performed using the SPSS Software, version 11.0 (SPSS Inc., Chicago, IL, USA).
RESULTS
From 52 patients who provided consent, 46 patients (88.5%) completed the study. Five patients (9.6%) of the placebo group discontinued the medication and lost during the follow-up period and one patient (1.9%) in thiazide group was excluded from the study due to discontinuing medication [Figure 1]. Therefore, we analyzed 25 patients and 21 patients in the hydrochlorothiazide and placebo groups, respectively. A total of 25 patients (54.3%) were male and others (45.7%) were female (P = 0.15). Mean of the patients' age was 42.73 ± 13.64 years and 38.76 ± 3.21 years in the groups 1 and 2, respectively (P = 0.32). The mean of stone size was not significantly different between both groups (P = 0.73).
Figure 1.
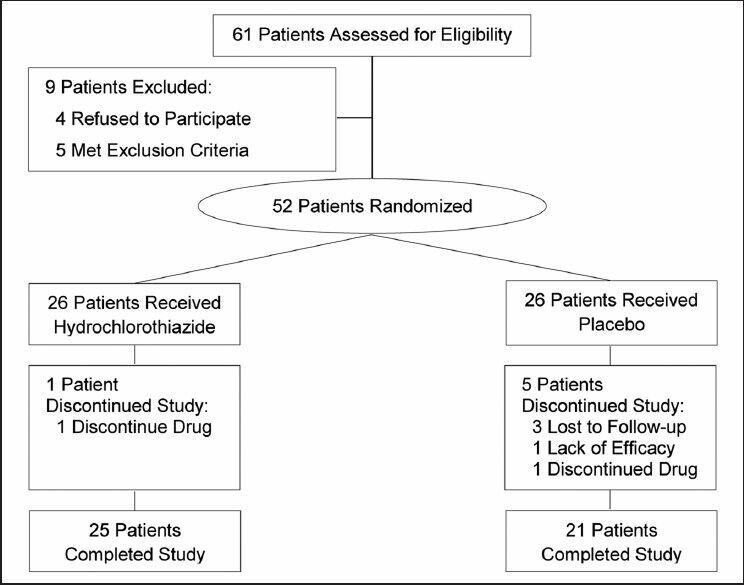
Study flowchart
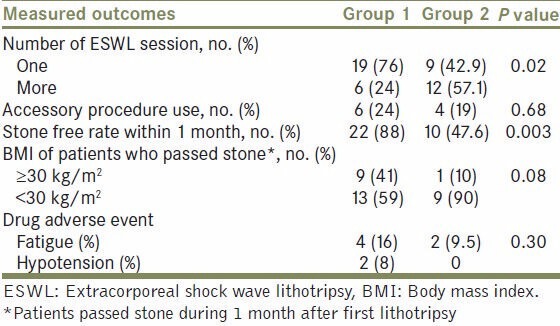
Moreover, 19 patients (76%) of the hydrochlorothiazide group underwent one session ESWL and 6 (24%) of them needed more than one session. In addition, in the placebo group, nine patients (42.9%) underwent a single session of ESWL and 12 patients (57.1%) needed more than one session of ESWL (P = 0.02). Six patients (24%) of the treatment group and four patients (19%) of the placebo group underwent accessory stone treatment procedures including further ureteroscopy or nephrolithotomy and there was no significant difference between groups [Table 1].
Table 1.
Basic characteristics
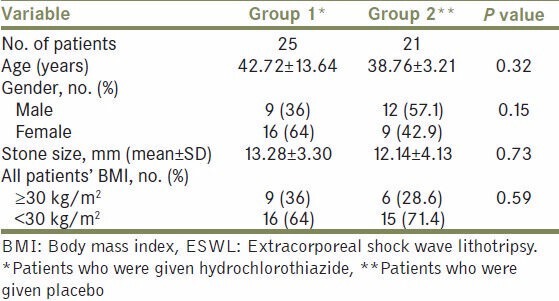
BMI values was not significantly different between groups (P = 0.59). Patients who passed the stone within 1 month after lithotripsy with BMI ≥30 kg/m2 were less than patients with BMI <30 kg/m2 in the hydrochlorothiazide group (41% vs. 59%, respectively) and placebo group (10% vs. 90%, respectively). However, this difference was not statistically significant between groups (P = 0.08). While 22 patients (88%) of those who were given hydrochlorothiazide passed the stone within 1 month following ESWL, 10 patients (47.6%) of those who received placebo passed stones at the same duration and there was a significant difference between the both groups (P = 0.003). All patients were free of calculus (size of the residual stone ≤4 mm) using ultrasonography following lithotripsy at 3 months after ESWL treatment. Moreover, drug side-effects that contributed to study withdrawal did not occurred in any patients [Table 2]. Hypotension and fatigue were reported by patients and there was no significant difference between groups in terms of drug adverse events.
Table 2.
Study outcomes
DISCUSSION
Since the introduction of ESWL it has become most using treatment option in urolithiasis setting;[5] however, medical therapy is needed to improve results of the urolithiasis treatment even using the lithotripsy.[4] One of the medications is alpha-blocker such as tamsulosin that was effective for improving ESWL outcomes.[7] Thiazides are another agent that results in reabsorption of sodium and calcium in distal tube. In addition, its hypocalciuric impact is the most important therapeutic effect of such diuretics in urolithiasis setting.[8]
Some authors explained other effects of the thiazides consist of urine oxalate reduction after long-term use (more than 12 months).[9] Moreover, it enhances urinary excretion of zinc and magnesium ions, which they have crystallization inhibitory role.[10] Other studies showed that the beneficial effect of thiazides on calcium stones is low and it is associated with adverse events including hypotension, fatigue, hypercalcemia, hyperuricemia and hyperuricosuria.[11] To the best of our knowledge, this is the first investigation showing that using the hydrochlorothiazide as a diuretic combined with ESWL treatment of renal pelvic calculi improved the stone-free rate and the number of ESWL sessions.
Azm and Higazy evaluated the effect of thiazide on stone passing after ESWL of ureteral stone and they showed that using diuresis adjunct to ESWL resulted in less number of lithotripsy sessions and more clearance success rate at 3rd month.[12] Moreover, Zomorrodi et al. assessed the impact of furosemide on ureteral stone passing after ESWL. They concluded that diuresis is useful for improving outcomes of ESWL of ureteric stones, especially, the middle ureteral calculi.[5] These findings are similar to our results, although, we could not show a significant difference between groups in the stone-free rate at 3 months following lithotripsy. However, we found that hydrochlorothiazide combined with ESWL treatment had more stone-free rate at 1 month than when using placebo along with lithotripsy. Moreover, the need for accessory treatment including further ureteroscopy or nephrolithotomy was not different between groups.
In addition, we found that the outcome of ESWL was affected by BMI of patients, because a higher proportion of patients who passed stones during 1 month after ESWL had BMI <30 kg/m2 than those who had BMI ≥30 kg/m2; however, this difference was not statistically significant (P = 0.08). We believe that BMI may act as a potential factor to augment outcomes of ESWL even using adjunct medication. Hereby, conducting an investigation in terms of weight indices (e.g., BMI, skin fold measurement and skin to stone distance) effect on outcomes can be impressive.
This study had some limitations. First, the sample size was small and it may contributed to the lack of showing other effects of hydrochlorothiazide. Second, we did not measure the urine level of calcium and acid-uric those are useful for evaluating hydrochlorothiazide complications. Third, we only considered patients with kidney stones to investigate. Finally, we need to further prospective and large-scale studies to assess the effects of diuresis on outcomes of ESWL treatment.
CONCLUSIONS
Administering 25 mg of hydrochlorothiazide twice daily adjunct to ESWL of nephrolithiasis improves the stone-free rate at 1 month following a single session of ESWL than ESWL alone. Moreover, it decreases the risk of requiring further ESWL sessions.
Footnotes
Source of Support: Nil
Conflict of Interest: None.
REFERENCES
- 1.Arrabal Martín M. Grupo de Litiasis de la Associación Española de Urología. Extracorporeal lithotripsy in Spain in the 20 th .Century. Actas Urol Esp. 2000;24:699–708. doi: 10.1016/s0210-4806(00)72531-9. [DOI] [PubMed] [Google Scholar]
- 2.Grases F, Costa-Bauzá A, Isern B, Sanchis P, Perelló J, Hierro F, et al. Evolution of post-ESWL residual lithiasis depending on the type of calculus and urine composition. Arch Esp Urol. 2009;62:473–82. [PubMed] [Google Scholar]
- 3.Norlin A, Lindell B, Granberg PO, Lindvall N. Urolithiasis. A study of its frequency. Scand J Urol Nephrol. 1976;10:150–3. doi: 10.3109/00365597609179677. [DOI] [PubMed] [Google Scholar]
- 4.Pak CY. Prevention and treatment of kidney stones. Role of medical prevention. J Urol. 1989;141:798–801. doi: 10.1016/s0022-5347(17)41013-5. [DOI] [PubMed] [Google Scholar]
- 5.Zomorrodi A, Golivandan J, Samady J. Effect of diuretics on ureteral stone therapy with extracorporeal shock wave lithotripsy. Saudi J Kidney Dis Transpl. 2008;19:397–400. [PubMed] [Google Scholar]
- 6.Costanzo LS, Weiner IM. On the hypocalciuric action of chlorothiazide. J Clin Invest. 1974;54:628–37. doi: 10.1172/JCI107800. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Losek RL, Mauro LS. Efficacy of tamsulosin with extracorporeal shock wave lithotripsy for passage of renal and ureteral calculi. Ann Pharmacother. 2008;42:692–7. doi: 10.1345/aph.1K546. [DOI] [PubMed] [Google Scholar]
- 8.Ettinger B, Citron JT, Livermore B, Dolman LI. Chlorthalidone reduces calcium oxalate calculous recurrence but magnesium hydroxide does not. J Urol. 1988;139:679–84. doi: 10.1016/s0022-5347(17)42599-7. [DOI] [PubMed] [Google Scholar]
- 9.Elomaa I, Ala-Opas M, Porkka L. Five years of experience with selective therapy in recurrent calcium nephrolithiasis. J Urol. 1984;132:656–61. doi: 10.1016/s0022-5347(17)49809-0. [DOI] [PubMed] [Google Scholar]
- 10.Laerum E. Metabolic effects of thiazide versus placebo in patients under long-term treatment for recurrent urolithiasis. Scand J Urol Nephrol. 1984;18:143–9. doi: 10.3109/00365598409182182. [DOI] [PubMed] [Google Scholar]
- 11.Yendt ER, Guay GF, Garcia DA. The use of thiazides in the prevention of renal calculi. Can Med Assoc J. 1970;102:614–20. [PMC free article] [PubMed] [Google Scholar]
- 12.Azm TA, Higazy H. Effect of diuresis on extracorporeal shockwave lithotripsy treatment of ureteric calculi. Scand J Urol Nephrol. 2002;36:209–12. doi: 10.1080/003655902320131893. [DOI] [PubMed] [Google Scholar]