

Abstract
In this paper, we aim to systematically analyze the effectiveness of community-based interventions (CBIs) for the prevention and control of helminthiasis including soil-transmitted helminthiasis (STH) (ascariasis, hookworms, and trichuriasis), lymphatic filariasis, onchocerciasis, dracunculiasis, and schistosomiasis. We systematically reviewed literature published before May 2013 and included 32 studies in this review. Findings from the meta-analysis suggest that CBIs are effective in reducing the prevalence of STH (RR: 0.45, 95% CI: 0.38, 0.54), schistosomiasis (RR: 0.40, 95% CI: 0.33, 0.50), and STH intensity (SMD: −3.16, 95 CI: −4.28, −2.04). They are also effective in improving mean hemoglobin (SMD: 0.34, 95% CI: 0.20, 0.47) and reducing anemia prevalence (RR: 0.90, 95% CI: 0.85, 0.96). However, it did not have any impact on ferritin, height, weight, low birth weight (LBW), or stillbirths. School-based delivery significantly reduced STH (RR: 0.49, 95% CI: 0.39, 0.63) and schistosomiasis prevalence (RR: 0.50, 95% CI: 0.33, 0.75), STH intensity (SMD: −0.22, 95% CI: −0.26, −0.17), and anemia prevalence (RR: 0.87, 95% CI: 0.81, 0.94). It also improved mean hemoglobin (SMD: 0.24, 95% CI: 0.16, 0.32). We did not find any conclusive evidence from the quantitative synthesis on the relative effectiveness of integrated and non-integrated delivery strategies due to the limited data available for each subgroup. However, the qualitative synthesis from the included studies supports community-based delivery strategies and suggests that integrated prevention and control measures are more effective in achieving greater coverage compared to the routine vertical delivery, albeit it requires an existing strong healthcare infrastructure. Current evidence suggests that effective community-based strategies exist and deliver a range of preventive, promotive, and therapeutic interventions to combat helminthic neglected tropical diseases (NTDs). However, there is a need to implement and evaluate efficient integrated programs with the existing disease control programs on a larger scale throughout resource-limited regions especially to reach the unreachable.
Keywords: Neglected tropical diseases, Soil-transmitted helminthiasis, Community-based interventions
Multilingual abstracts
Please see Additional file 1 for translations of the abstract into the six official working languages of the United Nations.
Introduction
Helminths (Greek, meaning ‘worms’) are parasitic worms that have been harboring in humans throughout the ages. These are classified as nematodes or roundworms and include soil-transmitted helminths (ascariasis, hookworms, and trichuriasis) and filarial (causing lymphatic filariasis [LF] and onchocerciasis), whereas the platyhelminthes or flatworms include the flukes (schistosomes) and tapeworms. As discussed in Paper 1 [1], helminthic infections are a prominent subgroup within neglected tropical diseases (NTDs), primarily perpetuated due to a lack of access to safe water and sanitation. The most common helminths are the soil-transmitted helminthiasis (STH), followed by schistosomiasis and LF. These are often co-infectious, although the biology of each disease differs. These infections disproportionately affect children, pregnant women, and young adults resulting in serious chronic health conditions including malnutrition, physical and intellectual growth retardations in children, and adverse maternal, perinatal and delivery outcomes among pregnant women [2-4]. Onchocerciasis is a leading cause of blindness and skin disease, while LF is a major cause of limb and genital deformities. For a more thorough discussion on the epidemiology and burden of each of these diseases, please refer to our previous publication [1].
Mass drug administration (MDA) with anthelminthics has been a major approach to combat human helminthiasis while parallel interventions such as micronutrient supplementation, especially iron, to combat associated anemia has also been widely evaluated for effectiveness [5]. Sanitation and education are also recommended, however, these are not always feasible in resource-limited settings. All these strategies can be effectively administered via community delivery platforms. Child health days, micronutrient supplementation, vaccination programs, and school-based programs provide a potential entry point for periodic deworming and health education in a more cost-effective manner [6]. In this paper, we aim to systematically analyze the effectiveness of community-based interventions (CBIs) for the prevention and control of helminthiasis including STH (ascariasis, hookworms, and trichuriasis), LF, onchocerciasis, dracunculiasis, and schistosomiasis.
Methods
We systematically reviewed literature published before May 2013 to identify studies on the effectiveness of the community-based delivery of interventions highlighted in our conceptual framework [7] for the outlined helminthic diseases. Our priority was to select existing randomized, quasi-randomized, and before-and-after studies in which the intervention was delivered within community settings and the reported outcomes were relevant to the diseases under review. A separate search strategy was developed for each disease using appropriate keywords, medical subject headings (MeSH), and free text terms. Searches were conducted in the PubMed, Cochrane Libraries, Embase, and the World Health Organization (WHO) Regional Databases. Studies that met the inclusion criteria were selected and double data was abstracted on a standardized abstraction sheet. Quality assessment of the included randomized controlled trials (RCTs) was done using the Cochrane risk of bias assessment tool [8]. The outcomes of interest assessed for each of the above diseases are outlined in Table 1. We conducted a meta-analysis for individual studies using the software Review Manager 5.1. Pooled statistics were reported as the relative risk (RR) for categorical variables and standard mean difference (SMD) for continuous variables between the experimental and control groups with 95% confidence intervals (CIs). We also attempted to qualitatively synthesize the findings reported in the included studies for other pragmatic parameters identified in our conceptual framework including intervention coverage, challenges/barriers, enabling factors, aspects related to integrated delivery, monitoring, and evaluations and equity. The detailed methodology is described in Paper 2 of this series [7].
Table 1.
Outcomes analyzed
| Outcomes | Outcomes analyzed |
|---|---|
|
Morbidity |
• Hookworm prevalence and intensity |
| • Ascaris prevalence and intensity | |
| • Trichuris prevalence and intensity | |
| • Schistosoma haematobium prevalence | |
| • Schistosoma mansoni prevalence | |
| • Schistosoma japonicum prevalence | |
|
Anthropometry |
• Weight |
| • Height | |
|
Hematologic |
• Prevalence of anemia |
| • Mean hemoglobin | |
| • Serum ferritin | |
| Birth outcomes | • Birth weight |
| • Low birth weigh | |
| • Very low birth weight | |
| • Stillbirths |
Review
We identified 2,556 titles from the searches conducted in all databases. After screening titles and abstracts, 208 full texts were reviewed, of which 32 studies (17 RCTs, two quasi, and 13 before-and-after studies) were included in the review (see Figure 1). The characteristics of the included studies are summarized in Table 2. Of these 32 studies, four could not be included in the meta-analysis; one study [9] did not report any outcome of interest, poolable data was not available in two studies [10,11], while one [12] did not have a suitable control group for comparison. We did not find any quantifiable data from the studies on dracunculiasis, LF, and onchocerciasis to be included in the pooled analysis. For the 17 RCTs included in this review, randomization was adequate in 15 studies, allocation was concealed in six, and adequate sequence generation was also done in six. All studies provided insufficient information on selective reporting which limited us from making any judgment (see Table 3).
Figure 1.
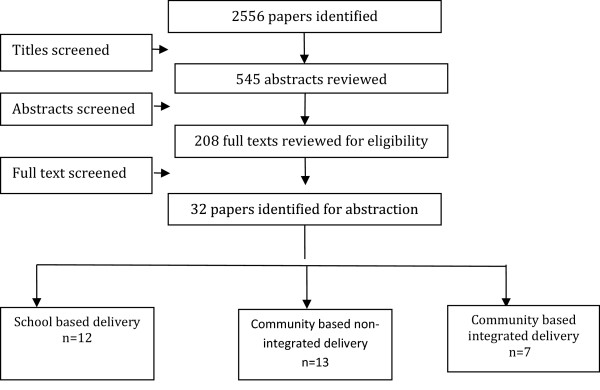
Search flow diagram.
Table 2.
Characteristics of the included studies
| Study | Study design | Country | Intervention | Target population | Integrated/Non-Integrated |
|---|---|---|---|---|---|
| Adam 1995 [13] |
RCT |
Kenya |
Three doses of 400 mg ALB vs. identical placebo on three consecutive school days |
Children aged 5–10 years infected with hookworms or ascariasis |
School-based |
| Ageel 1997 [33] |
Pre/post |
Saudi Arabia |
One oral dose of PZQ (40 mg/kg) + snail/vector control + health education + community participation |
General population infected with schistosomiasis |
PHC |
| Albonico 2002 [14] |
RCT |
Tanzania |
MBZ 500 mg vs. pyrantel-oxantel (10 mg/kg) vs. placebo |
Children aged 6–9 years |
School-based |
| Bausch 1995 [35] |
Quasi |
Cameroon |
Health education + PZQ |
Children aged 5–15 years with schistosomiasis |
PHC + school-based |
| Beasely 1999 [25] |
RCT |
Tanzania |
Single dose of 400 mg ALB + PPZQ (40 mg/kg) vs. placebo |
Infected children aged 7–12 years |
Non-integrated |
| Bhargawa 2003 [15] |
RCT |
Tanzania |
ALB 400 mg + PZQ single 40 mg/kg vs. placebo |
Infected children aged 9–15 years |
School-based |
| Christian 2009 [36] |
RCT |
Nepal |
ALB 40 mg in 2nd + 3rd trimester |
Pregnant women |
Integrated with routine ANC |
| Dossa 2001 [26] |
RCT |
Benin |
Iron (Fe) (60 mg/day) + ALB (200 mg for 3 days) vs. FE + placebo vs. ALB + placebo vs. placebo 10 months F/V |
Children aged 3–5 years |
Non-integrated |
| Engels 1993 [11] |
Pre/post |
Burundi |
Single dose PZQ (40 mg/kg), 50–150 mg levamisole or 500 mg MBL or PZQ (20 mg/kg) + snail vector control + education |
General population |
PHC |
| Gryseels 1991 [23] |
Pre/post |
Burundi |
PZQ (40 mg/kg) |
General population |
Non-integrated |
| Gundersen 1990 [34] |
Pre/post |
Ethiopia |
Vector snail control + 20 mg oxamniquine followed by 40 mg the next day |
General population |
PHC |
| Guyatt 2001 [16] |
Pre/post |
Tanzania |
Single dose 400 mg ALB + PZQ 40 mg/kg |
School children aged 8–14 years |
School-based |
| Halwindi 2011 [27] |
RCT |
Zambia |
Facility vs. community detected and treatment + training + education + MBZ |
Children aged 12–months (preventive) |
Non-integrated |
| Haque 2010 [28] |
RCT |
Bangladesh |
400 mg ALB + B-carotene (2 doses) vs. ALB + placebo vs. B-carotene + placebo vs. placebo + placebo |
Infected children aged 24–60 months |
Non-integrated |
| Hathirat 1992 [24] |
RCT |
Thailand |
Fe 50 mg FeSo 4 daily for 2 weeks then 100 mg for 14wks vs. anthelminthic |
Children aged 9–11 years |
School-based |
| Kosinski 2012 [31] |
Pre/post |
Ghana |
Water recreation area + PZQ |
Children |
Non-integrated |
| Koukounari 2006 [17] |
Pre/post |
Uganda |
PZQ |
Children aged 7–14 years |
School-based |
| Koukounari 2007 [18] |
Pre/post |
Burkina Faso |
PZQ 40 mg/kg + ALB 400 mg |
Children aged 6–14 years |
School-based |
| Larocque 2006 [37] |
RCT |
Peru |
MBZ 500 mg single dose + 60 mg FE daily vs. placebo + FE |
Pregant women aged 18–44 years in the 2nd trimester |
Integrated with routine ANC |
| Ndibazza 2010 [38] |
RCT |
Uganda |
ALB (400 mg) vs. PZQ 40 mg/kg vs. ALB + PZQ vs. placebo |
Pregnant women |
Integrated with routine ANC |
| Nsowah-Nuamah 2001 [12] |
Pre/post |
Ghana |
PZQ 40 mg/kg + passive edu vs. PZQ + no education vs. PZQ + active edu vs. community mobilization |
Those aged 5 years and above |
Non-integrated |
| Olds 1999 [29] |
RCT |
China and Philippines |
ALB + PZQ vs. PZQ + ALB placebo vs. ALB + PZQ placebo vs. placebo + placebo |
Infected school aged children (4–18 years) |
Non-integrated |
| Palupi 1997 [30] |
RCT |
Indonesia |
FE + ALB 400 mg once a week vs. FE once a week + placebo vs. placebo alone |
Children aged 2–5 years |
Non-integrated |
| Phuc 2009 [40] |
Pre/post |
Vietnam |
IEC materials + staff training + Ferrous Sulphate/ folic acid (200 mg) + ALB (400 mg) |
Women of reproductive age (16–45 years) |
Non-integrated |
| Rohner 2010 [19] |
RCT |
Cote d’Ivoire |
Iron fortified biscuits (20 mg fe/day) + IPT-SP (500 mg sulphadoxine + 25 mg pyrimethamine) + anthelminthic (400 mg-single) + PZQ (single – 40 mg/kg) in different combinations |
School children aged 6–14 years |
School-based |
| Savioli 1989 [9] |
Pre/post |
Tanzania |
PZQ |
Children |
School-based |
| Sungthong 2002 [20] |
RCT |
Thailand |
Deworming (400 mg ALB single) + daily or weekly iron |
Children aged 6–13 years |
School-based |
| Sinoun 2007 [10] |
Pre/post |
Cambodia |
Universal chemotherapy with PZQ (40 mg/kg) |
General population |
Non-integrated |
| Taylor 2001 [21] |
RCT |
South Africa |
ALB (400 mg) + PZQ (40 mg/kg) + FE fumigate 200 mg weekly vs. ALB (400 mg) + PZQ (40 mg/kg) + placebo weekly vs. ALB (400 mg) daily + PZQ (40 mg/kg) + FE 200 mg weekly vs. ALB (400 mg) + PZQ (40 mg/kg) + placebo weekly vs. placebos + FE 200 mg weekly vs. placebos |
Children aged 6–15 years |
School-based |
| Torlesse 2001 [39] |
RCT |
Sierra Leone |
FE + ALB vs. FE alone vs. ALB alone vs. placebo |
Pregnant women (10–14 weeks) |
Integrated with routine ANC |
| Wang 2009 [32] |
Quasi |
China |
Health education + vector control + removing cattle + latrines + PZQ |
General population |
Non-integrated |
| Zhang 2007 [22] | Pre/post | Uganda | PZQ (40 mg/kg) + ALB(400 mg) + education | School children and adults | Non-integrated |
Table 3.
Quality assessment of the included RCTs
| Study | Randomization | Sequence generation | Allocation concealment | Blinding of participants | Blinding of assessors | Selective reporting |
|---|---|---|---|---|---|---|
| Larocque 2006 [37] |
Done |
Done |
Done |
Done |
Done |
No |
| Ndibazza 2010 [38] |
Done |
Done |
Done |
Done |
Done |
No |
| Torlesse 2001 [39] |
Done |
Done |
Not clear |
Not clear |
Not clear |
Yes |
| Haque 2010 [28] |
Done |
Not clear |
Not clear |
Done |
Not clear |
No |
| Albonico 2002 [14] |
Done |
Done |
Done |
Done |
Done |
No |
| Taylor 2001 [21] |
Done |
Not clear |
Not clear |
Done |
Done |
Not clear |
| Adams 1994 [13] |
Done |
Not clear |
Not clear |
Done |
Not clear |
No |
| Beasley 1999 [25] |
Done |
Not computerized but done |
Not clear |
Not done |
Done |
No |
| Christian 2009 [36] |
Not clear |
Not clear |
Not clear |
Not Clear |
Not Clear |
Not clear |
| Halwindi 2011 [27] |
Not clear |
Not clear |
Not applicable |
Not applicable |
Not clear |
No |
| Olds 1999 [29] |
Done |
Not clear |
Done |
Done |
Done |
Not clear |
| Rohner 2010 [19] |
Done |
Not clear |
Done |
Done |
Done |
No |
| Bhargava 2003 [15] |
Done |
Not clear |
Not clear |
Not clear |
Not clear |
No |
| Palupi 1997 [30] |
Done |
Not clear |
Not clear |
Not clear |
Not clear |
No |
| Dossa 2001 [26] |
Done |
Not clear |
Not clear |
Done |
Done |
Yes |
| Hathirat 1992 [24] |
Done |
Not clear |
Not clear |
Done |
Done |
No |
| Sungthong 2002 [20] | Done | Done | Done | Done | Done | No |
Included studies mainly focused on community-based MDA, which involved preventive chemotherapy in 19 of the studies and treatment after confirmed diagnosis in 11 studies. A school-based delivery strategy was the most common delivery strategy used in 12 [9,13-21,24,25] studies targeting children aged five to 15 years, thirteen [10,12,22,23,25-32,40] studies were non-integrated vertically delivered interventions, seven [11,33,34,36-39] were integrated with primary healthcare (PHC), and routine antenatal care (ANC) services. Almost all the studies had a component on health education to promote general hygiene and sanitation along with the drug administration. Other co-interventions included iron and β-carotene supplementation, snail control, constructing latrines, eliminating cattle from the residential areas, staff training, and community mobilization. One study [31] assessed the effectiveness of constructing a water recreation area in the community using a local lake to prevent transmission of schistosomiasis among school children. Most of the studies provided combined drug treatment for the prevention and treatment of hookworms, ascariasis, trichuriasis, and schistosomiasis with the treatment regimen including administration of albendazole (ALB) 400 mg for STH and praziquantel (PZQ) 40 mg/kg for schistosomiasis, while mebendazole (MBZ) 500 mg was used in four studies [11,14,27,37] and one study [14] also administered pyrantel-oxantel (10 mg/kg). The frequency of treatment varied according to the prevalence in the intervention area. We also attempted to conduct a subgroup analysis for the relative effectiveness of preventive and therapeutic drug administration, integrated and non-integrated delivery strategies, and evidence from RCTs/quasi and pre-post studies separately, where possible, and reported the results accordingly. The results are summarized in Tables 4 and 5.
Table 4.
Results for the overall and subgroup analysis according to type of study and treatment
|
Outcomes |
Estimates (95% CI) |
|
|||
|---|---|---|---|---|---|
| Combined | RCTs | Pre-post studies | Preventive | Therapeutic | |
|
STH Prevalence (RR) |
0.47 [0.41, 0.54] |
0.47 [0.41, 0.55] |
0.51 [0.40, 0.65] |
0.43 [0.31, 0.59] |
0.52 [0.44, 0.61] |
| 45 datasets from 12 studies |
40 datasets from 9 studies |
5 datasets from 3 studies |
22 datasets from 7 studies |
23 datasets from 5 studies |
|
| Hookworm |
0.40 [0.31, 0.52] |
0.41 [0.32, 0.54] |
0.39 [0.23, 0.65] |
0.26 [0.14, 0.45] |
0.60 [0.46, 0.78] |
| 15 datasets, 10 studies |
13 datasets from 8 studies |
2 datasets from 2 studies |
8 datasets from 6 studies |
7 datasets from 4 studies |
|
| Ascariasis |
0.32 [0.20, 0.51] |
0.30 [0.18, 0.49] |
0.61 [0.41, 0.90] |
0.62 [0.38, 1.01] |
0.18 [0.08, 0.40] |
| 15 datasets, 9 studies |
14 datasets from 8 studies |
1 dataset from 1 study |
7 datasets from 4 studies |
8 datasets from 5 studies |
|
| Trichuriasis |
0.66 [0.55, 0.80] |
0.65 [0.53, 0.79] |
0.97 [0.68, 1.37] |
0.57 [0.22, 1.46] |
0.76 [0.66, 0.88] |
| 14 datasets, 8 studies |
13 datasets from 7 studies |
1 dataset from 1 study |
6 datasets from 3 studies |
8 datasets from 5 studies |
|
|
Schistosomiasis Prevalence (RR) |
0.41 [0.34, 0.50] |
0.42 [0.33, 0.54] |
0.37 [0.25, 0.55] |
0.39 [0.27, 0.55] |
0.41 [0.30, 0.55] |
| 25 datasets, 13 studies |
16 datasets from 6 studies |
9 datasets from 7 studies |
11 datasets from 7studies |
14 datasets from 6 studies |
|
|
Schistosoma Haematobium
|
0.41 [0.30, 0.57] |
0.43 [0.29, 0.64] |
0.33 [0.17, 0.65] |
0.59 [0.35, 1.02] |
0.31 [0.18, 0.52] |
| 10 datasets, 8 studies |
6 datasets from 4 studies |
4 datasets from 4 studies |
3 datasets from 3 studies |
7 datasets from 5 studies |
|
|
SchistosomaJaponicum |
0.24 [0.07, 0.80] |
0.24 [0.07, 0.80] |
No studies |
0.11 [0.05, 0.26] |
0.30 [0.07, 1.31] |
| 4 datasets, 2 studies |
4 datasets from 2 studies |
1 dataset from 1 study |
3 datasets from 1 study |
||
|
SchistosomaMansoni |
0.48 [0.36, 0.64] |
0.55 [0.38, 0.81] |
0.39 [0.25, 0.62] |
0.37 [0.24, 0.58] |
0.67 [0.45, 1.01] |
| 11 datasets, 7 studies |
6 datasets from 2 studies |
5 datasets from 5 studies |
7 datasets from 5 studies |
4 datasets from 2 studies |
|
|
STH intensity (SMD) |
−3.16 [−4.28, −2.04] |
−5.29 [−9.22, −1.36] |
−0.22 [−0.26, −0.17] |
−0.22 [−0.26, −0.17] |
−5.29 [−9.22, −1.36] |
| 5 datasets, 3 studies |
3 datasets from 1 study |
2 datasets from 2 studies |
2 datasets from 2 studies |
3 datasets from 1 study |
|
| Hookworm |
−2.22 [−3.27, −1.17] |
−6.79 [−7.44, −6.14] |
−0.22 [−0.26, −0.17] |
−0.22 [−0.26, −0.17] |
−6.79 [−7.44, −6.14] |
| 3 datasets, 03 studies |
1 dataset from 1 study |
2 datasets from 2 studies |
2 datasets from 2 studies |
1 dataset from 1 study |
|
| Ascariasis |
−7.25 [−7.93, −6.56] |
−7.25 [−7.93, −6.56] |
No studies |
No studies |
−7.25 [−7.93, −6.56] |
| 1 dataset, 1 study |
1 dataset from 1 study |
1 dataset from 1 study |
|||
| Trichuriasis |
−1.87 [−2.16, −1.57] |
−1.87 [−2.16, −1.57] |
No Studies |
No studies |
−1.87 [−2.16, −1.57] |
| 1 dataset, 01 study |
1 dataset from 1 study |
1 dataset from 1 study |
|||
|
Mean hemoglobin (SMD) |
0.34 [0.20, 0.47] |
0.43 [0.15, 0.71] |
0.22 [0.13, 0.31] |
0.19 [0.12, 0.26] |
1.28 [−0.53, 3.08] |
| 14 datasets, 12 studies |
9 datasets from 7 studies |
5 datasets from 5 studies |
12 datasets from 10 studies |
2 datasets from 2 studies |
|
|
Anemia |
0.90 [0.85, 0.96] |
0.92 [0.85, 1.00] |
0.87 [0.78, 0.97] |
0.90 [0.85, 0.96] |
0.85 [0.69, 1.06] |
| 9 datasets, 7 studies |
5 datasets from 3 studies |
4 datasets from 4 studies |
8 datasets from 6 studies |
1 dataset from 1 study |
|
|
Serum ferritin (SMD) |
2.30 [−1.13, 5.73] |
0.06 [−0.07, 0.18] |
0.10 [−0.16, 0.37] |
0.09 [−0.12, 0.29] |
0.07 [−0.07, 0.20] |
| 4 datasets, 4 studies |
2 dataset from 2 studies |
2 datasets from 2 studies |
3 datasets from 3 studies |
1 dataset from 1 study |
|
|
Height |
0.01 [−0.10, 0.12] |
−0.04 [−0.16, 0.08] |
0.23 [−0.02, 0.49] |
0.08 [−0.12, 0.28] |
−0.02 [−0.15, 0.11] |
| 4 datasets, 4 studies |
3 datasets from 3 studies |
1 dataset from 1 study |
2 datasets from 2 studies |
2 datasets from 2 studies |
|
|
Weight |
−0.13 [−0.42, 0.16] |
−0.28 [−0.66, 0.11] |
0.22 [−0.03, 0.47] |
−0.01 [−0.48, 0.46] |
−0.35 [−1.13, 0.42] |
| 4 datasets, 4 studies |
3 datasets from 3 studies |
1 dataset from 1 study |
2 datasets from 2 studies |
2 data sets from 2 studies |
|
|
Birth outcomes |
|
|
|
|
|
| Birth weight |
−9.52 [−13.86, −5.19] |
−9.52 [−13.86, −5.19] |
No studies |
−9.52 [−13.86, −5.19] |
No study |
| 6 datasets, 3 studies |
6 datasets from 3 studies |
6 datasets from 3 studies |
|||
| LBW |
0.96 [0.78, 1.18] |
0.96 [0.78, 1.18] |
No studies |
0.96 [0.78, 1.18] |
No studies |
| 4 datasets, 2 studies |
4 datasets from 2 studies |
4 datasets from 2 studies |
|||
| VLBW |
0.48 [0.19, 1.19] |
0.48 [0.19, 1.19] |
No studies |
0.48 [0.19, 1.19] |
No studies |
| 4 datasets, 2 studies |
4 datasets, 2 studies |
4 datasets, 2 studies |
|||
| Stillbirths | 1.54 [0.93, 2.58] |
1.54 [0.93, 2.58] |
No studies | 1.54 [0.93, 2.58] |
No studies |
| 3 datasets, 1 study | 3 datasets from 1 study | 3 datasets from 1 study | |||
*estimates in bold are statistically significant.
Table 5.
Summary estimates for the overall and subgroup analysis for school-based, non-integrated, and integrated delivery strategies
|
Outcomes |
Estimates (95% CI) |
|||
|---|---|---|---|---|
| Combined | School-based delivery | Community-based non-integrated delivery | Community-based integrated delivery | |
|
STH Prevalence (RR) |
0.45 [0.38, 0.54] |
0.49 [0.39, 0.63] |
0.52 [0.41, 0.67] |
0.30 [0.12, 0.78] |
| 45 datasets, 12 studies |
19 datasets from 6 studies |
16 datasets from 4 studies |
9 datasets from 1 study |
|
| Hookworm |
0.38 [0.27, 0.53] |
0.37 [0.22, 0.62] |
0.49 [0.29, 0.85] |
0.25 [0.04, 1.62] |
| 15 datasets, 10 studies |
7 datasets from 5 studies |
5 datasets from 3 studies |
3 datasets from 1 study |
|
| Ascariasis |
0.32 [0.19, 0.52] |
0.28 [0.09, 0.89] |
0.36 [0.18, 0.74] |
0.28 [0.09, 0.87] |
| 15 datasets, 9 studies |
4 datasets from 6 studies |
6 datasets from 4 studies |
3 datasets from 1 studies |
|
| Trichuriasis |
0.66 [0.53, 0.82] |
0.78 [0.67, 0.90] |
0.76 [0.62, 0.94] |
0.41 [0.07, 2.56] |
| 14 datasets, 8 studies |
4 datasets from 6 studies |
5 datasets from 3 study |
3 datasets from 1 studies |
|
|
Schistosomiasis Prevalence (RR) |
0.40 [0.33, 0.50] |
0.50 [0.33, 0.75] |
0.42 [0.31, 0.57] |
0.24 [0.11, 0.56] |
| 25 datasets, 13 studies |
7 datasets from 5 studies |
12 datasets from 4 studies |
6 datasets from 4 studies |
|
|
S. H
a
ematobium
|
0.40 [0.29, 0.57] |
0.59 [0.35, 1.02] |
0.42 [0.26, 0.70] |
0.05 [0.01, 0.45] |
| 10 datasets, 8 studies |
3 datasets from 3 studies |
5 datasets from 3 studies |
2 datasets from 2 studies |
|
|
S. Japonicum
|
0.24 [0.06, 0.87] |
No studies |
0.24 [0.06, 0.87] |
No studies |
| 4 datasets, 2 studies |
4 datasets from 2 studies |
|||
|
S. Mansoni
|
0.48 [0.35, 0.65] |
0.44 [0.27, 0.74] |
0.68 [0.42, 1.10] |
0.38 [0.16, 0.91] |
| 11 datasets, 7 studies |
4 datasets from 4 studies |
3 datasets from 1 study |
4 datasets from 2 studies |
|
|
STH intensity (SMD) |
−3.16 [−4.28, −2.04] |
−0.22 [−0.26, −0.17] |
−5.29 [−9.22, −1.36] |
No studies |
| 5 datasets, 3 studies |
2 datasets, 2 studies |
3 datasets from 1 study |
||
| Hookworm |
−2.22 [−3.27, −1.17] |
−0.22 [−0.26, −0.17] |
−6.79 [−7.44, −6.14] |
No studies |
| 3 datasets, 3 studies |
2 datasets, 2 studies |
1 dataset from 1 study |
||
| Ascariasis |
−7.25 [−7.93, −6.56] |
No studies |
−7.25 [−7.93, −6.56] |
No studies |
| 1 dataset, 1 study |
1 dataset from 1 study |
|||
| Trichuriasis |
−1.87 [−2.16, −1.57] |
No studies |
−1.87 [−2.16, −1.57] |
No studies |
| 1 dataset, 1 study |
1 dataset from 1 study |
|||
|
Mean hemoglobin (SMD) |
0.34 [0.20, 0.47] |
0.24 [0.16, 0.32] |
0.93 [−0.33, 2.18] |
0.09 [−0.01, 0.20] |
| 14 datasets, 12 studies |
7 datasets from 7 studies |
3 datasets from 3 studies |
4 datasets from 2 studies |
|
|
Anemia |
0.90 [0.85, 0.96] |
0.87 [0.81, 0.94] |
0.85 [0.69, 1.06] |
0.99 [0.90, 1.09] |
| 9 datasets, 7 studies |
5 datasets from 5 studies |
1 datasets from 1 study |
3 datasets from 1 study |
|
|
Serum ferritin (SMD) |
2.30 [−1.13, 5.73] |
0.10 [−0.04, 0.25] |
No studies |
−0.01 [−0.36, 0.34] |
| 4 datasets, 4 studies |
3 datasets from 3 studies |
1 dataset from 1 study |
||
|
Height |
0.01 [−0.10, 0.12] |
0.04 [−0.08, 0.15] |
−0.19 [−0.53, 0.14] |
No studies |
| 4 datasets, 4 studies |
3 datasets from 3 studies |
1 dataset from 1 study |
||
|
Weight |
−0.13 [−0.42, 0.16] |
−0.09 [−0.46, 0.27] |
−0.27 [−0.60, 0.07] |
No studies |
| 4 datasets, 4 studies |
3 datasets from 3 studies |
1 dataset from 1 study |
||
|
Birth outcomes |
|
|
|
|
| Birth weight |
−9.52 [−13.86, −5.19] |
No studies |
No studies |
−9.52 [−13.86, −5.19] |
| 6 datasets, 3 studies |
6 datasets from 3 studies |
|||
| LBW |
0.96 [0.78, 1.18] |
No studies |
No studies |
0.96 [0.78, 1.18] |
| 4 datasets, 2 studies |
4 datasets from 2 studies |
|||
| VLBW |
0.38 [0.16, 0.87] |
No studies |
No studies |
0.38 [0.16, 0.87] |
| 4 datasets, 2 studies |
4 datasets from 2 studies |
|||
| Stillbirths | 1.54 [0.93, 2.58] |
No studies | No studies | 1.54 [0.93, 2.58] |
| 3 datasets, 1 study | 3 datasets from 1 study | |||
*Estimates in bold are statistically significant.
Quantitative synthesis
Twelve studies reported STH prevalence, showing a significant 53% reduction in the overall STH prevalence (RR: 0.47, 95% CI: 0.41, 0.54) rate, 60% reduction in hookworm prevalence (RR: 0.40, 95% CI: 0.31, 0.52), 68% in ascariasis (RR: 0.32, 95% CI: 0.20, 0.51), and 34% (RR: 0.66, 95% CI: 0.55, 0.80) in trichuriasis prevalence (see Figure 2). Twenty-five studies pooled for schistosomiasis prevalence also showed a significant 59% overall reduction (RR: 0.41, 95% CI: 0.34, 0.50), with 59% (RR: 0.41, 95% CI: 0.30, 0.57), 76% (RR: 0.24, 95% CI: 0.07, 0.80) and 52% (RR: 0.48, 95% CI: 0.36, 0.64) reductions in the prevalence of Schistosoma haematobium, Schistosoma japonicum, and Schistosoma mansoni, respectively (see Figure 3). CBIs also significantly reduced the mean STH intensity (SMD: −3.16, 95 CI: −4.28, −2.04).Twelve studies reported on the hemoglobin (Hb) levels and showed significantly improved mean Hb in the intervention group (SMD: 0.34, 95% CI: 0.20, 0.47), while anemia significantly reduced by 10% (RR: 0.90, 95% CI: 0.85, 0.96) (see Figures 4 and 5). Impacts on serum ferritin, weight, height and delivery outcomes of stillbirth, low birth weight (LBW), and very LBW remained non-significant in the overall, as well as the subgroup, analyses.
Figure 2.
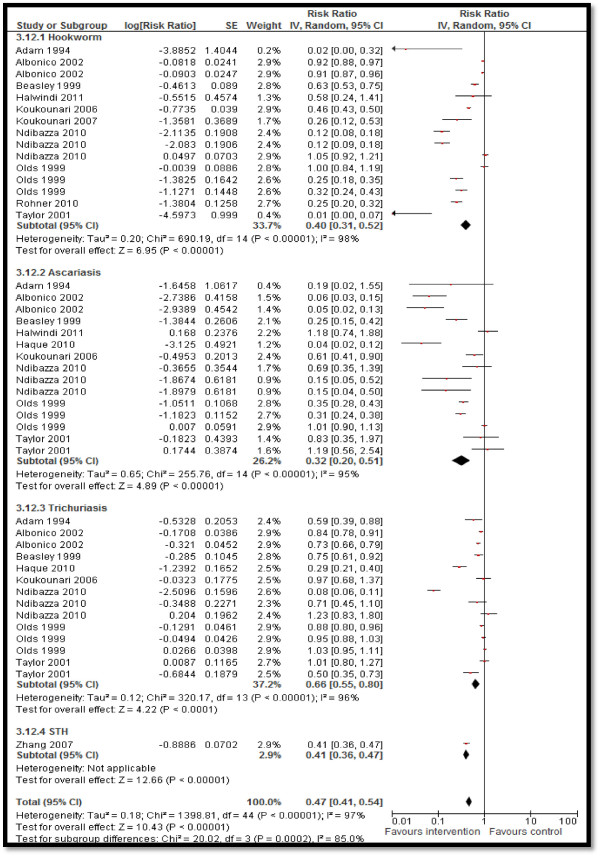
Forest plot for the impact of CBIs on STH prevalence.
Figure 3.
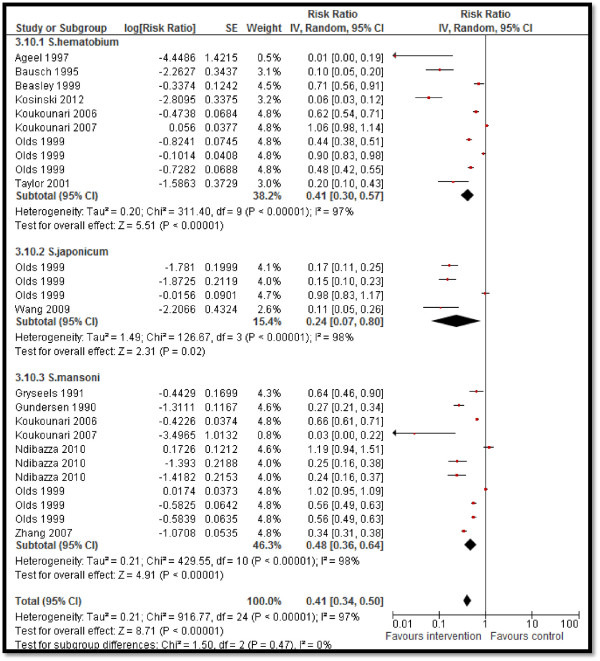
Forest plot for the impact of CBIs on schistosomiasis.
Figure 4.
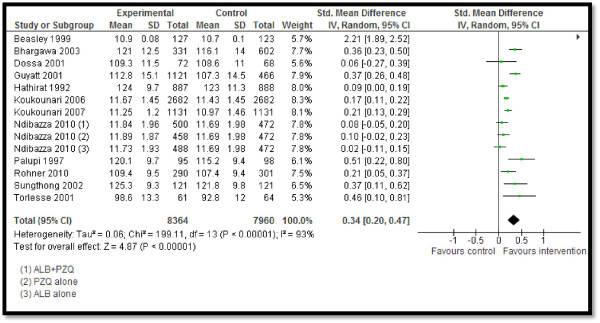
Forest plot for the impact of CBIs on hemoglobin.
Figure 5.
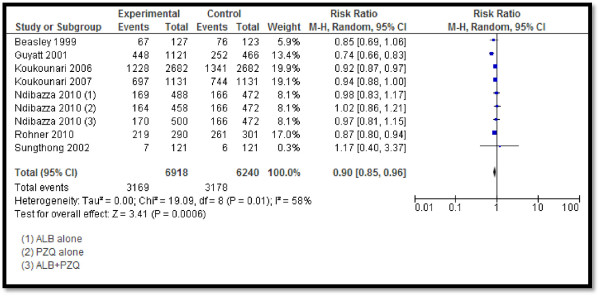
Forest plot for the impact of CBIs on anemia.
Our subgroup analysis for the preventive and therapeutic drug administration showed that preventive drug administration significantly reduced the overall prevalence of STH (RR: 0.43, 95% CI: 0.31, 0.59), STH intensity (SMD: −0.22, 95% CI: −0.26, −0.17), and schistosomiasis prevalence (RR: 0.39, 95% CI: 0.27, 0.55), with non-significant impacts on ascariasis, trichuriasis, and Schistosoma haematobium prevalence. It also significantly improved mean Hb (SMD: 0.19, 95% CI: 0.12, 0.26) and reduced anemia prevalence (RR: 0.90, 95% CI: 0.85, 0.96) and VLBW (RR: 0.38, 95% CI: 0.16, 0.87). Preventive chemotherapy did not have a significant impact on serum ferritin, height, weight, LBW, or stillbirths. Therapeutic drug administration showed significant reductions in STH prevalence (RR: 0.52, 95% CI: 0.44, 0.61), intensity (SMD: −5.29, 95% CI: −9.22, −1.36), and schistosomiasis prevalence (RR: 0.41, 95% CI: 0.30, 0.55). Our analysis did not show a significant impact of therapeutic chemotherapy on serum ferritin, Hb, weight, or height.
Findings from the subgroup analysis for school-based, non-integrated, and integrated delivery strategies suggest that school-based delivery significantly reduced STH prevalence (RR: 0.49, 95% CI: 0.39, 0.63) and intensity (SMD: −0.22, 95% CI: −0.26, −0.17), and the prevalence of all types of schistosomiasis (RR: 0.50, 95% CI: 0.33, 0.75), with a non-significant impact on Schistosoma mansoni. It also improved mean Hb (SMD: 0.24, 95% CI: 0.16, 0.32) and reduced anemia prevalence (RR: 0.87, 95% CI: 0.81-0.94) among school children. However, school-based delivery did not show any significant impact on serum ferritin, height, and weight. Non-integrated delivery reduced STH prevalence (RR: 0.52, 95% CI: 0.41, 0.67), intensity (SMD: −5.29, 95% CI: −9.22, −1.36), and schistosomiasis prevalence (RR: 0.42, 95% CI: 0.31, 0.57), with a non-significant impact on Schistosoma mansoni. Integrated delivery improved schistosomiasis prevalence (RR: 0.24, 95% CI: 0.11, 0.5) and overall STH prevalence (RR: 0.30, 95% CI: 0.12, 0.78), with non-significant impacts on the prevalence of hookworm or trichuriasis.
Qualitative synthesis
Since most of the quantitative outcomes reported pertained to disease specific indicators, we also attempted to qualitatively synthesize the findings reported in the included studies on other pragmatic parameters from our conceptual framework. CBIs have been reported to achieve large-scale nationwide coverage as seen in Burkina Faso, which was the first country in the WHO African Region to achieve nationwide coverage with anthelminthic drugs against three major NTDs: LF, schistosomiasis, and STH [18]. Furthermore, when delivered in integration with the existing health systems, these programs can achieve maximum coverage as seen in the Gizan region, where a vertically-oriented program, involving mobile teams for schistosome control, failed to achieve the target of 80% population coverage and was costly to sustain. The same program, when later on integrated with the existing PHC, led to a significant increase in the numbers of patients examined and chemotherapy coverage. Similarly in Zimbabwe and Burundi, schistosomiasis and other control programs for NTDs have increasingly been integrated into horizontal PHC systems [23]. The available health infrastructure allows the control strategy to be very well integrated into basic health services, enabling it to be sustained and making it affordable for the national health budget [11]. In a health system that generally enjoys a strong structure from the provincial level down to the community level, successful integration of these services are relatively easier and just require making small modifications to the existing system. However, this process may require more attention in countries where the health service structure is weak. The PHC approach has led to better coverage as compared to the vertical programs, and has been effective in reducing the overall prevalence of helminthic infections.
CBIs have achieved a higher coverage without any increase in implementation costs at the district and health facility levels. At the community level, there is an increase in ‘opportunity costs’ from community implementers who volunteer their time, thus forgoing other remunerative activities. Some of the studies reported no major direct additional costs incurred because the drugs, training materials, and stationary were provided by the PHC from their available resources, and the community health workers (CHWs) were not given any monetary incentives. Hence, the major additional costs included the indirect cost of labour hours for the CHWs and the PHC staff during training and implementation of the program. However, for national scale-up, the biggest challenge is likely to be the cost of training and incentives for the CHWs [27]. Similarly, school-based delivery of preventive and promotive interventions is also reported to be cost effective, however, its success depended on close supervision of the teachers’ compliance with the program implementation, collaboration of the educational authorities, and enthusiastic participation of the school personnel [24]. On the contrary, in some endemic areas, an integrated delivery strategy has not been successful in improving coverage because of the poor access to health services in remote areas. In view of the strong commitment of national health authorities and funding agencies to increase PHC coverage, rapid improvement of this situation can be expected. For sustained reduction in infection prevalence and complete eradication, periodic implementation is also necessary to ensure continuity of morbidity control and achieve universal coverage. In endemic areas, an intermittent intervention delivery has shown to reduce the prevalence but did not completely eradicate the infections. This might be attributable to the fact that chemotherapy reduces disease prevalence only at the time of its administration and does not prevent reinfection [32]. Hence, in endemic areas, periodic implementation along with efforts to prevent reinfection is required.
Most of the studies support a multi-component strategy involving chemotherapy, health education, improved water supply and sanitation, and snail control. Health education and community involvement have been highlighted as essential components in any strategy for helminthic infection control and have been used in many countries [12,22,33]. Examples of such successful programs are the chemotherapy program in Sudan where village health committees served as facilitators, and in Zimbabwe where CHWs were involved in the implementation of improvements to the water supply, sanitation, and in health education programs. Similarly in Ethiopia and Egypt, local health personnel, farmers, school health visitors, and teachers assisted in the implementation of successful control programs. Knowledge and education plays an important role as, apparently, the information motivates the participants and consequently ensures a higher level of compliance [30,40]. The process of designing the program, from its very initiation, should include open discussions and involvement of all partners from the international to the local level. This will ensure that everyone understands the goals, benefits and underlying principles of the project, and have the flexibility needed to adapt to particular local conditions in order to achieve these goals [40]. Strong commitment of all partners to the intervention has reportedly led to excellent participation levels and a significant clinical impact [34,40]. Besides health education and community participation, the socioeconomic development leading to a general rise in living standards, improved sanitation and water supplies, construction of drilled wells in rural areas, and a significant increase in medical care also played a large part in the control of helminthic NTDs [33]. Another important enabling factor was free distribution of drugs and supplies to ensure equitable distribution to poor and marginalized groups, which also helped avoid a complicated system of cost recovery and achieve high compliance levels.
Financial, logistical, and organizational limitations were the major reported constraints in the long-term sustainability of such programs. Despite considerable efforts and their high costs, the results of some of the vector control programs have been disappointing, largely because of poor weed control, lack of maintenance, and the operational difficulty of covering entire networks, which leads to rapid recolonization of treated sites. Large-scale health education programs will not serve their purpose if alternatives to traditional water contact activities are not available. Maintenance is still reported as a major hindrance and local authorities should try to find adequate solutions. Annual tax payments, private latrine programs, subsidized prices, and credit facilities are some of the counter strategies devised to overcome these issues and ensure sustainability of such programs after withdrawal of external funds [11]. Another major challenge is to maintain a high level of participation and enthusiasm as the project is integrated into the routine provincial health program [40]. Although maximum coverage has been achieved in the school-based programs, frequent migration of people (particularly from the fishing communities), influx from neighboring countries, and absence from school of some school-aged children remain to be significant hurdles to the successful implementation of the program [23]. Although often disregarded, religious, economic, and educational heterogeneity within communities may also impair disease control efforts and, hence, these subtle demographic variables must be taken into account.
Discussion
The evidence in this review comes from efficacy and effectiveness studies on CBIs for helminthic NTDs compared to routine facility-based care or no intervention. Our review findings suggest that CBIs are effective in reducing the prevalence of STH and schistosomiasis, and STH intensity. They are also effective in improving mean Hb and reducing anemia prevalence, but there was non-significant impact on serum ferritin, height and weight gain, LBW, and stillbirths. School-based delivery was identified as a potential medium of delivery as it significantly reduced STH and schistosomiasis prevalence, STH intensity, and anemia prevalence, however, there was limited data available on the effectiveness of the integrated and non-integrated delivery strategies. The qualitative synthesis from the included studies supports community-based delivery strategies and suggests that integrated infection prevention and control measures are more effective in achieving greater coverage compared to the routine vertical delivery, albeit it requires an existing strong healthcare infrastructure. Systematic reviews have been conducted on helminthic NTDs previously, however, their scopes were either limited to a particular infection, drug efficacy or intervention, or the review did not evaluate the effectiveness of community delivery strategies [41-45].
The WHO recommends periodic administration of anthelminthic medicines, mainly ALB and MBZ for STH, PZQ for schistosomiasis, and ivermectin or diethylcarbamazine citrate (DEC) for LF once or twice a year depending on the baseline prevalence of the infection to control morbidity among the population at risk [46].
Health education is an essential component in the prevention and control of helminthiasis. Almost all the studies in this review had a health education component focusing on general hygiene and sanitation along with the recommended drug administration. We did not find any quantifiable data from studies on dracunculiasis, LF, and onchocerciasis to be included in the pooled analysis. Among these diseases, much progress has been made for dracunculiasis and a significant reduction in dracunculiasis prevalence of more than 99% has been achieved since 1989 [47]. Dracunculiasis is successfully at the verge of eradication due to a combination of interventions including community-based surveillance systems, intensified case-containment measures, and access to safe drinking water. Globally, 1.39 billion people still require preventive chemotherapy for LF while 123 million people are at risk of becoming infected with onchocerciasis [46,48]. Programs targeting LF and onchocerciasis are in place in endemic countries, for example, the Global Programme to Eliminate LF and the African Programme for Onchocerciasis. These programs enable resource-limited countries to make medicines freely available and allow easy access to healthcare with a consequent reduction in infection prevalence [49].
Community delivery platforms are increasingly being advocated for the prevention and control of major health issues such as nutrition and childhood infection, and hence could be feasible for helminthic NTDs [50,51]. Under these community platforms, integration of various disease specific programs is being encouraged for onchocerciasis, LF, schistosomiasis, STH, and trachoma [52,53]. The integrated delivery of interventions to control these diseases is more feasible and cost effective as these diseases are endemic in specific geographical pockets where population are mostly co-infected and control mainly involves regular MDA of effective preventive chemotherapy. Therefore, a package of drugs for more than one NTD can be feasibly delivered. Critical factors for successful integration include active support of relevant political and health authorities, a clear understanding by all parties of the health issues, and a simple distribution process. However, there is limited data available to gauge the effectiveness of integrated delivery of these programs along with other health programs including routine ANC and PHC setups [54,55]. School-based delivery has proven to be effective for the management and control of helminthic diseases as it requires a minimum amount of training for school teachers to aid implementation and hence doesn’t require an added workforce, whilst providing vast coverage at low costs [56].
Conclusion
Current evidence emphasizes that effective community-based strategies exist and deliver a range of preventive, promotive, and therapeutic interventions to combat helminthic NTDs. However, there is a need to conduct high-quality studies on the process of developing and implementing an efficient integrated program as previous global programs have focused on the control of a single NTD through a comprehensive approach. These interventions exist within the current health systems in most of the low- and middle-income countries, but there is a need to implement them on a larger scale especially to reach the unreachable.
Abbreviations
ANC: Antenatal care; CBI: Community based intervention; CHW: Community health worker; IDoP: Infectious diseases of poverty; LF: Lymphatic filariasis; MDA: Mass drug administration; NTD: Neglected tropical disease; PHC: Primary healthcare; STH: Soil-transmitted helminthiasis; WHO: World health organization
Competing interests
The authors declare that they have no financial or non-financial competing interests.
Authors’ contributions
ZAB was responsible for designing and coordinating the review. ZSL and HM were responsible for the data collection, screening of the search results, screening of the retrieved papers against the inclusion criteria, appraising the quality of papers, and abstracting the data. RAS, JKD, and ZSL were responsible for data interpretation and writing the review. ZAB critically reviewed and modified the manuscript. All authors read and approved the final manuscript.
Authors’ information
Zulfiqar A Bhutta: Founding Director, Center of Excellence in Women & Child Health, The Aga Khan University, Karachi, Pakistan and Robert Harding Chair in Global Child Health & Policy, Center for Global Child Health, Hospital for Sick Children, Toronto, Canada
Supplementary Material
Multilingual abstracts in the six official working languages of the United Nations.
Contributor Information
Rehana A Salam, Email: rehana.salam@aku.edu.
Hasina Maredia, Email: hasinamaredia@gmail.com.
Jai K Das, Email: jai.das@aku.edu.
Zohra S Lassi, Email: zohra.lassi@aku.edu.
Zulfiqar A Bhutta, Email: zulfiqar.bhutta@aku.edu.
Acknowledgements
The collection of scoping reviews in this special issue of Infectious Diseases of Poverty was commissioned by the UNICEF/UNDP/World Bank/WHO Special Programme for Research and Training in Tropical Diseases (TDR) in the context of a Contribution Agreement with the European Union for “Promoting research for improved community access to health interventions in Africa”.
References
- Bhutta ZA, Sommerfeld J, Lassi ZS, Salam RA, Das JK. Global Burden, Distribution and Interventions for the Infectious Diseases of Poverty. Infect Dise of Pov. 2014;3:21. doi: 10.1186/2049-9957-3-21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hotez PJ, Bundy DAP, Beegle K, Brooker S, Drake L, de Silva N, Montresor A, Engels D, Jukes M, Chitsulo L. Helminth infections: soil-transmitted helminth infections and schistosomiasis. 2006. [PubMed]
- Crompton DWT, Nesheim MC. Nutritional impact of intestinal helminthiasis during the human life cycle. Annu Rev Nutr. 2002;22(1):35–59. doi: 10.1146/annurev.nutr.22.120501.134539. [DOI] [PubMed] [Google Scholar]
- Miguel E, Kremer M. Worms: identifying impacts on education and health in the presence of treatment externalities. Econometrica. 2004;72(1):159–217. [Google Scholar]
- Hotez PJ, Molyneux DH, Fenwick A, Kumaresan J, Sachs SE, Sachs JD, Savioli L. Control of neglected tropical diseases. N Engl J Med. 2007;357(10):1018–1027. doi: 10.1056/NEJMra064142. [DOI] [PubMed] [Google Scholar]
- Hawley WA, Phillips-Howard PA, Kuile FO, Terlouw DJ, Vulule JM, Ombok M, Nahlen BL, Gimnig JE, Kariuki SK, Kolczak MS. Community-wide effects of permethrin-treated bed nets on child mortality and malaria morbidity in western Kenya. Am J Trop Med Hyg. 2003;68(4):121–127. [PubMed] [Google Scholar]
- Lassi ZS, Salam RA, Das JK, Bhutta ZA. Conceptual framework and assessment methodology for the systematic review on community based interventions for the prevention and control of IDoP. Infect Dise of Pov. 2014;3:22. doi: 10.1186/2049-9957-3-22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- H. JPT and G. S, editor. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. [updated March 2011] The Cochrane Collaboration; 2011. [Google Scholar]
- Savioli L, Dixon H, Kisumku UM, Mott KE. Control of morbidity due to Schistosoma haematobium on Pemba island; selective population chemotherapy of schoolchildren with haematuria to identify high-risk localities. Trans R Soc Trop Med Hyg. 1989;83(6):805–810. doi: 10.1016/0035-9203(89)90336-2. [DOI] [PubMed] [Google Scholar]
- Sinuon M, Tsuyuoka R, Socheat D, Odermatt P, Ohmae H, Matsuda H, Montresor A, Palmer K. Control of Schistosoma mekongi in Cambodia: results of eight years of control activities in the two endemic provinces. Trans R Soc Trop Med Hyg. 2007;101(1):34–39. doi: 10.1016/j.trstmh.2006.04.011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Engels D, Ndoricimpa J, Gryseels B. Schistosomiasis mansoni in Burundi: progress in its control since 1985. Bull World Health Organ. 1993;71(2):207–214. [PMC free article] [PubMed] [Google Scholar]
- Nsowah-Nuamah NN, Mensah G, Aryeetey ME, Wagatsuma Y, Bentil G. Urinary schistosomiasis in southern Ghana: a logistic regression approach to data from a community-based integrated control program. Am J Trop Med Hyg. 2001;65(5):484–490. doi: 10.4269/ajtmh.2001.65.484. [DOI] [PubMed] [Google Scholar]
- Adams EJ, Stephenson LS, Latham MC, Kinoti SN. Physical activity and growth of Kenyan school children with hookworm, Trichuris trichiura and Ascaris lumbricoides infections are improved after treatment with albendazole. J Nutr. 1994;124(8):1199. doi: 10.1093/jn/124.8.1199. [DOI] [PubMed] [Google Scholar]
- Albonico M, Bickle Q, Haji HJ, Ramsan M, Khatib KJ, Montresor A, Savioli L, Taylor M. Evaluation of the efficacy of pyrantel-oxantel for the treatment of soil-transmitted nematode infections. Trans R Soc Trop Med Hyg. 2002;96(6):685–690. doi: 10.1016/s0035-9203(02)90352-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bhargava A, Jukes M, Lambo J, Kihamia CM, Lorri W, Nokes C, Drake L, Bundy D. Anthelmintic treatment improves the hemoglobin and serum ferritin concentrations of Tanzanian schoolchildren. Food Nutr Bull. 2003;24(4):332–342. doi: 10.1177/156482650302400403. [DOI] [PubMed] [Google Scholar]
- Guyatt HL, Brooker S, Kihamia CM, Hall A, Bundy DAP. Evaluation of efficacy of school-based anthelmintic treatments against anaemia in children in the United Republic of Tanzania. Bull World Health Organ. 2001;79(8):695–703. [PMC free article] [PubMed] [Google Scholar]
- Koukounari A, Fenwick A, Whawell S, Kabatereine NB, Kazibwe F, Tukahebwa EM, Stothard JR, Donnelly CA, Webster JP. Morbidity indicators of Schistosoma mansoni: relationship between infection and anemia in Ugandan schoolchildren before and after praziquantel and albendazole chemotherapy. Am J Trop Med Hyg. 2006;75(2):278–286. [PubMed] [Google Scholar]
- Koukounari A, Gabrielli AF, Toura S, BosquaOliva E, Zhang Y, Sellin B, Donnelly CA, Fenwick A, Webster JP. Schistosoma haematobium infection and morbidity before and after large-scale administration of praziquantel in Burkina Faso. J Infect Dis. 2007;196(5):659. doi: 10.1086/520515. [DOI] [PubMed] [Google Scholar]
- Rohner F, Zimmermann MB, Amon RJ, Vounatsou P, Tschannen AB, N’Goran EK, Nindjin C, Cacou MC, TaBonla MD, Aka H. In a randomized controlled trial of iron fortification, anthelmintic treatment, and intermittent preventive treatment of malaria for anemia control in Ivorian children, only anthelmintic treatment shows modest benefit. J Nutr. 2010;140(3):635–641. doi: 10.3945/jn.109.114256. [DOI] [PubMed] [Google Scholar]
- Sungthong R, Mo-suwan L, Chongsuvivatwong V, Geater AF. Once weekly is superior to daily iron supplementation on height gain but not on hematological improvement among schoolchildren in Thailand. J Nutr. 2002;132(3):418–422. doi: 10.1093/jn/132.3.418. [DOI] [PubMed] [Google Scholar]
- Taylor M, Jinabhai CC, Couper I, Kleinschmidt I, Jogessar VB. The effect of different anthelmintic treatment regimens combined with iron supplementation on the nutritional status of schoolchildren in KwaZulu-Natal, South Africa: a randomized controlled trial. Trans R Soc Trop Med Hyg. 2001;95(2):211–216. doi: 10.1016/s0035-9203(01)90171-3. [DOI] [PubMed] [Google Scholar]
- Zhang Y, Koukounari A, Kabatereine N, Fleming F, Kazibwe F, Tukahebwa E, Stothard JR, Webster J, Fenwick A. Parasitological impact of 2-year preventive chemotherapy on schistosomiasis and soil-transmitted helminthiasis in Uganda. BMC Med. 2007;5(1):27. doi: 10.1186/1741-7015-5-27. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gryseels B, Nkulikyinka L, Engels D. Repeated community-based chemotherapy for the control of Schistosoma mansoni: effect of screening and selective treatment on prevalences and intensities of infection. Am J Trop Med Hyg. 1991;45(4):509–517. doi: 10.4269/ajtmh.1991.45.509. [DOI] [PubMed] [Google Scholar]
- Hathirat P, Valyasevi A, Kotchabhakdi NJ, Rojroongwasinkul N, Pollitt E. Effects of an iron supplementation trial on the Fe status of Thai schoolchildren. Br J Nutr. 1992;68(1):245–252. doi: 10.1079/bjn19920081. [DOI] [PubMed] [Google Scholar]
- Beasley NMR, Tomkins AM, Hall A, Kihamia CM, Lorri W, Nduma B, Issae W, Nokes C, Bundy DAP. The impact of population level deworming on the haemoglobin levels of schoolchildren in Tanga, Tanzania. Trop Med Int Health. 1999;4(11):744–750. doi: 10.1046/j.1365-3156.1999.00486.x. [DOI] [PubMed] [Google Scholar]
- Dossa RAM, Ategbo EAD, De Koning F, Van Raaij JMA, Hautvast J. Impact of iron supplementation and deworming on growth performance in preschool Beninese children. Eur J Clin Nutr. 2001;55(4):223–228. doi: 10.1038/sj.ejcn.1601126. [DOI] [PubMed] [Google Scholar]
- Halwindi H, Magnussen P, Siziya S, Handema RAY, Meyrowitsch D, Olsen A. Impact of community-directed treatment on soil transmitted helminth infections in children aged 12 to 59 months in Mazabuka District, Zambia. Parasitology. 2011;138(12):1578. doi: 10.1017/S0031182011000059. [DOI] [PubMed] [Google Scholar]
- Haque R, Ahmed T, Wahed MA, Mondal D, Rahman ASMH, Albert MJ. Low-dose Î2-carotene supplementation and deworming improve serum vitamin A and Î2-carotene concentrations in preschool children of Bangladesh. J Health Popul Nutr. 2010;28(3):230. doi: 10.3329/jhpn.v28i3.5549. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Olds GR, King C, Hewlett J, Olveda R, Wu G, Ouma J, Peters P, McGarvey S, Odhiambo O, Koech D. Double-blind placebo-controlled study of concurrent administration of albendazole and praziquantel in schoolchildren with schistosomiasis and geohelminths. J Infect Dis. 1999;179(4):996–1003. doi: 10.1086/314686. [DOI] [PubMed] [Google Scholar]
- Palupi L, Schultink W, Achadi E, Gross R. Effective community intervention to improve hemoglobin status in preschoolers receiving once-weekly iron supplementation. Am J Clin Nutr. 1996;65(4):1057–1061. doi: 10.1093/ajcn/65.4.1057. [DOI] [PubMed] [Google Scholar]
- Kosinski KC, Adjei MN, Bosompem KM, Crocker JJ, Durant JL, Osabutey D, Plummer JD, Stadecker MJ, Wagner AD, Woodin M, Gute D. Effective control of Schistosoma haematobium infection in a Ghanaian community following installation of a water recreation area. PLoS Negl Trop Dis. 2012;6(7):e1709. doi: 10.1371/journal.pntd.0001709. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wang LD, Chen HG, Guo JG, Zeng XJ, Hong XL, Xiong JJ, Wu XH, Wang XH, Wang LY, Xia G, Hao Y, Chin D, Zhou XN. A strategy to control transmission of Schistosoma japonicum in China. N Engl J Med. 2009;360(2):121–128. doi: 10.1056/NEJMoa0800135. [DOI] [PubMed] [Google Scholar]
- Ageel ARM, Amin MA. Integration of schistosomiasis control activities into the primary health care system in the Gizan region, Saudi Arabia. Ann Trop Med Parasitol. 1997;91(8):907–916. doi: 10.1080/00034989760293. [DOI] [PubMed] [Google Scholar]
- Gundersen SG, Birrie H, Torvik HP, Scherbaum H. Control of Schistosoma mansoni in the Blue Nile Valley of western Ethiopia by mass chemotherapy and focal snail control: a primary health care experience. Trans R Soc Trop Med Hyg. 1990;84(6):819–825. doi: 10.1016/0035-9203(90)90095-v. [DOI] [PubMed] [Google Scholar]
- Bausch D, Cline BL. The impact of control measures on urinary schistosomiasis in primary school children in northern Cameroon: a unique opportunity for controlled observations. Am J Trop Med Hyg. 1995;53(6):577–580. doi: 10.4269/ajtmh.1995.53.577. [DOI] [PubMed] [Google Scholar]
- Christian P, Stewart CP, LeClerq SC, Wu L, Katz J, West KP, Khatry SK. Antenatal and postnatal iron supplementation and childhood mortality in rural Nepal: a prospective follow-up in a randomized, controlled community trial. Am J Epidemiol. 2009;170(9):1127–1136. doi: 10.1093/aje/kwp253. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Larocque R, Casapia M, Gotuzzo E, MacLean JD, Soto JC, Rahme E, Gyorkos TW. A double blind randomized controlled trial of antenatal mebendazole to reduce low birthweight in a hookworm endemic area of Peru. Trop Med Int Health. 2006;11(10):1485–1495. doi: 10.1111/j.1365-3156.2006.01706.x. [DOI] [PubMed] [Google Scholar]
- Ndibazza J, Muhangi L, Akishule D, Kiggundu M, Ameke C, Oweka J, Kizindo R, Duong T, Kleinschmidt I, Muwanga M. Effects of deworming during pregnancy on maternal and perinatal outcomes in Entebbe, Uganda: a randomized controlled trial. Clin Infect Dis. 2010;50(4):531–540. doi: 10.1086/649924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Torlesse H, Hodges M. Albendazole therapy and reduced decline in haemoglobin concentration during pregnancy (Sierra Leone) Trans R Soc Trop Med Hyg. 2001;95(2):195–201. doi: 10.1016/s0035-9203(01)90164-6. [DOI] [PubMed] [Google Scholar]
- Phuc T, Mihrshahi S, Casey G, Phu L, Tien N, Caruana S, Thach T, Montresor A, Biggs BA. Lessons learned from implementation of a demonstration program to reduce the burden of anemia and hookworm in women in Yen Bai Province, Viet Nam. BMC Public Health. 2009;9(1):266. doi: 10.1186/1471-2458-9-266. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dickson R, Awasthi S, Williamson P, Demellweek C, Garner P. Effects of treatment for intestinal helminth infection on growth and cognitive performance in children: systematic review of randomised trials. BMJ. 2000;320:1697–1701. doi: 10.1136/bmj.320.7251.1697. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Uneke CJ. Soil transmitted helminth infections and schistosomiasis in school age children in sub-Saharan Africa: efficacy of chemotherapeutic intervention since World Health Assembly Resolution 2001. Tanzan J Health Res. 2010;12(1):86–99. doi: 10.4314/thrb.v12i1.56366. [DOI] [PubMed] [Google Scholar]
- Ziegelbauer K, Speich B, Mausezahl D, Bos R, Keiser J, Utzinger J. Effect of sanitation on soil-transmitted helminth infection: systematic review and meta-analysis. PLoS Med. 2012;9(1):e1001162. doi: 10.1371/journal.pmed.1001162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Keiser J, Utzinger J. Efficacy of current drugs against soil-transmitted helminth infections: systematic review and meta-analysis. JAMA. 2008;299(16):1937–1948. doi: 10.1001/jama.299.16.1937. [DOI] [PubMed] [Google Scholar]
- Taylor-Robinson DC, Maayan N, Soares-Weiser K, Donegan S, Garner P. Deworming drugs for soil-transmitted intestinal worms in children: effects on nutritional indicators, haemoglobin and school performance. Cochrane Database Syst Rev. 2012;7(11):CD000371. doi: 10.1002/14651858.CD000371.pub4. [DOI] [PubMed] [Google Scholar]
- World Health, Organization. Sustaining the drive to overcome the global impact of neglected tropical diseases. Geneva, Switzerland: World Health Organization; 2013. (Second WHO report on neglected tropical diseases). [Google Scholar]
- World Health, Organization. Dracunculiasis eradication-global surveillance summary, 2009. Wkly Epidemiol Rec. 2010;85:165–176. [PubMed] [Google Scholar]
- Hotez PJ. Forgotten people, forgotten diseases: the neglected tropical diseases and their impact on global health and development. Amer Society for Microbiology. 2008.
- Crompton DWT, Daumerie D, Peters P, Savioli L, World Health Organization. Working to overcome the global impact of neglected tropical diseases: first WHO report on neglected tropical diseases. Geneva, Switzerland: World Health Organization; 2010. [Google Scholar]
- Bhutta ZA, Das JK, Rizvi A, Gaffey MF, Walker N, Horton S, Webb P, Lartey A, Black RE. Evidence-based interventions for improvement of maternal and child nutrition: what can be done and at what cost? Lancet. 2013;382(9890):452–477. doi: 10.1016/S0140-6736(13)60996-4. [DOI] [PubMed] [Google Scholar]
- Bhutta ZA, Das JK, Walker N, Rizvi A, Campbell H, Rudan I, Black RE. Interventions to address deaths from childhood pneumonia and diarrhoea equitably: what works and at what cost? Lancet. 2013;381(9875):1417–1429. doi: 10.1016/S0140-6736(13)60648-0. [DOI] [PubMed] [Google Scholar]
- Brady MA, Hooper PJ, Ottesen EA. Projected benefits from integrating NTD programs in sub-Saharan Africa. Trends Parasitol. 2006;22(7):285–291. doi: 10.1016/j.pt.2006.05.007. [DOI] [PubMed] [Google Scholar]
- Hotez P, Raff S, Fenwick A, Richards F Jr, Molyneux DH. Recent progress in integrated neglected tropical disease control. Trends Parasitol. 2007;23(11):511–514. doi: 10.1016/j.pt.2007.08.015. [DOI] [PubMed] [Google Scholar]
- Grepin KA, Reich MR. Conceptualizing integration: a framework for analysis applied to neglected tropical disease control partnerships. PLoS Negl Trop Dis. 2008;2(4):e174. doi: 10.1371/journal.pntd.0000174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lammie PJ, Fenwick A, Utzinger J. A blueprint for success: integration of neglected tropical disease control programmes. Trends Parasitol. 2006;22(7):313–321. doi: 10.1016/j.pt.2006.05.009. [DOI] [PubMed] [Google Scholar]
- Molyneux DH. Combating the “other diseases” of MDG 6: changing the paradigm to achieve equity and poverty reduction? Trans R Soc Trop Med Hyg. 2008;102(6):509–519. doi: 10.1016/j.trstmh.2008.02.024. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Multilingual abstracts in the six official working languages of the United Nations.