

Abstract
The purpose of this study was to assess whether cytochrome P450 enzyme 2A6 (CYP2A6) genotypes moderate the association between smoking and hypertension. In this study, 954 Chinese male current smokers from a community-based chronic disease screening project in Guangzhou were interviewed with a structured questionnaire about socio-demographic status, smoking and other health-related behaviors. Blood was collected for DNA extraction and CYP2A6 genotyping. Hypertension was defined according to 2007 ESH-ESC Practice Guidelines. A multivariate logistic regression was performed to examine the interaction between smoking quantity and CYP2A6 genotypes on hypertension after adjusting for age, education level and other potential confounders. Multivariate analyses indicated that smoking more than 15 cigarettes per day significantly increased the risk of hypertension (odds ratio (OR)=1.59, 95% confidence interval (CI)=1.21-2.10) compared with smoking 1-15 cigarettes per day, and further suggested that smoking interacted with normal CYP2A6 metabolizer genotype to increase the risk of hypertension. Smokers consuming more than 15 cigarettes per day with normal CYP2A6 metabolizer genotypes had the highest risk of hypertension (OR=2.04, 95% CI=1.11-3.75) compared with those consuming 1-15 cigarettes per day with slower CYP2A6 metabolizer genotypes. These findings demonstrated that smoking quantity was positively associated with hypertension and that CYP2A6 genotypes may moderate this relationship.
Keywords: cigarette smoking, CYP2A6, genetic polymorphisms, interaction
Introduction
Cigarette smoking is a well-documented risk factor for cardiovascular diseases, including atherosclerosis, coronary artery disease, acute myocardial infarction, hypertension and sudden cardiac death.1 - 3 Multiple prospective studies have consistently shown that cigarette smoking is associated with increased risk of hypertension.4 - 8 Cigarette smoking can stimulate sympathetic nervous activation,9 oxidative stress,10 vasopressor effects,11 cause endothelial dysfunction,12 vascular inflammation13 and injury,14 and increase arterial stiffness;15 factors that might contribute to the development of hypertension.16,17 However, the precise mechanisms underlying the etiological contribution of cigarette smoking to hypertension is still not well understood.
It has been well proved that nicotine is the main reason of smoking dependence, and approximately 80% of the inhaled nicotine from smoking is metabolized to cotinine by C-oxidation in liver, then the cotinine is further metabolized into trans-3-hydroxycotinine that is finally excreted in urine as the major nicotine metabolite.18 Almost all the process of nicotine metabolization is mediated by cytochrome P450 2A6 (CYP2A6) enzyme, which is mainly expressed in liver.18 The enzymatic activity of the CYP2A6 enzyme is moderated by variation in the CYP2A6 gene, which has in turn been associated with variation in smoking behaviors.19 To date, over 30 variants in the CYP2A6 gene have been identified (http://www.cypalleles.ki.se/cyp2a6.htm). Numerous studies have found an association of genetic variation in CYP2A6 with a number of aspects of smoking, including age of smoking onset, smoking duration,20,21 likelihood of smoking cessation,22 depth and amount of smoke inhalation,23 and the number of cigarettes smoked per day.24 - 26 Moreover, CYP2A6 genotype appears to moderate the relationship between cigarette smoking and smoking-related cancers, such as lung cancer,26 - 28 nasopharyngeal carcinoma,29 pancreatic cancer,30 bladder cancer,31 and head and neck cancer.32 However, little is known about the interactive effect between cigarette smoking and CYP2A6 genotype on the development of hypertension.
The present study aimed to assess the interaction between smoking quantity and CYP2A6 genotype on hypertension in Chinese male current smokers.
Methods
Subjects
Subjects were from a community-based chronic disease-screening project conducted in Guangzhou and Zhuhai of China from July 2006 to June 2007.32 In that project, a total of 7293 residents (2465 males and 4828 females) aged 20 years or above were randomly selected using a stratified multistage sampling method. In this population, 1440 participants were smokers (1059 current smokers and 381 former smokers, or 1327 male smokers and 113 female smokers). To minimize the confounding effect of smoking status and gender only, male current smokers were included in the analysis of interaction between amounts of daily cigarette consumption and CYP2A6 genotype on hypertension. Of the 1025 current male smokers, 71 refused to have blood samples drawn and were therefore excluded for a total of 954 male current smokers in these analyses (Figure 1). This study was approved by the Ethics Committees of Sun Yat-sen University in Guangzhou of China and a written informed consent was obtained from all study participants.
Figure 1.

Study subjects selection diagram.
Data collection
A face to face interview was conducted by well-trained medical students or clinical doctors using a structured questionnaire inquiring about socio-demographic characteristics (for example, age, gender, income, education level, marital status, occupation) and smoking behaviors. The survey was completed at local health care centers, and a blood specimen was obtained from each subject for CYP2A6 genotyping.
Measurement of smoking behaviors
In the present study, smoking included current smoking and former smoking. A current smoker was defined by having smoked more than 100 cigarettes in one's lifetime and having smoked at least one cigarette daily at the time of the interview.33 A ‘former smoker’ was someone who had smoked more than 100 cigarettes in their lifetime, but reported that they had quit smoking. Former smokers included ex-daily smokers and ex-non-daily smokers.33 Current smokers reported their most recent average number of cigarettes consumed per day, and they were categorized into two groups according to the median of daily cigarette consumption: smokers who consumed 1 - 15 cigarettes per day and smokers who consumed more than 15 cigarettes per day.34
Definition of alcohol consumption and exercise
Alcohol consumption was divided into two categories (ever or never) based on whether a subject had at any time consumed alcohol at least three times a week for more than 6 months.35. Physical activity was also classified into two categories: regular physical activity, defined as leisure time physical activity engaged in any intensity for 30min at least three times a week, or no regular physical activity.36
Measurement and definition of obesity and abdominal obesity
Body mass index (BMI) was calculated as weight (kg) divided by the square of height (m). Participants with a BMI≥23 kg m−2 and <30 kg m−2 were classified as overweight, and those with a BMI≥30 kg m−2 were classified as obese.37 Waist-to-hip ratio (WHR) was calculated by dividing the waist circumference by the hip circumference. Abdominal obesity was defined by WHR≥0.90.38
CYP2A6 genotyping
Blood was collected from 954 male current smokers. The selection of CYP2A6 alleles assayed in the present study was based on two factors: (a) the impact of the variant on CYP2A6 enzyme function, and (b) the frequency of the variant in Chinese populations. The genotyping of CYP2A6*4, *5, *7, *9 and *10 were performed using the methods previously published by our group.38 Normal, intermediate, slow and poor CYP2A6 metabolizer genotypes are defined here on the basis of the predicted pharmacokinetic impact of genotypes resulting from the different variant alleles studied. The CYP2A6*9 allele was considered a ‘decrease of function’ allele (D), and *4, *5, *7 and *10 were considered ‘loss of function’ (L) alleles. ‘Normal metabolizers’ were defined as having neither a D nor an L allele (that is, *1/*1). ‘Intermediate metabolizers’ had only one D allele (for example, *1/*9), which was associated with approximately 75% of the activity of normal metabolizers. ‘Slow metabolizers’ had either one L allele or two D alleles (for example, *1/*4 or *9/*9), which were associated with 50% of the activity of normal metabolizers. ‘Poor metabolizers’ had either one L and one D allele or two L alleles (for example, *9/*4 or *4/*4), which were associated with <25% of the activity of normal metabolizers.25,39 In this study, the frequencies of normal, intermediate, slow and poor metabolizers in current smokers were 441 (46.2%), 137 (14.4%), 254 (26.6%) and 122 (12.8%), respectively.39 Considering the number of subjects with both heavy smoking and hypertension was few (11/122) in the current smokers with poor CYP2A6 metabolizer genotype, we combined poor CYP2A6 metabolizer genotype with slow CYP2A6 metabolizer genotype and named them the ‘slower CYP2A6 metabolizer genotype’, which may increase the statistical power.
Diagnostic criteria for hypertension
Systolic blood pressure and diastolic blood pressure were measured three times in each subject in the morning using a mercury sphygmomanometer in the sitting position after a 15-min rest, and the values were then averaged. Every smoker was asked not to smoke after getting up until finishing the blood pressure measurement. Hypertension was defined as systolic blood pressure ≥ 140 mm Hg and/or diastolic blood pressure ≥ 90 mm Hg according to the 2007 ESH-ESC Practice Guidelines,40 or as self-reported diagnosed hypertension requiring antihypertensive drugs.Family history of hypertension was defined as self-reported of one or more hypertensive parents or grandparents.
Statistical analysis
For continuous variables, mean ± s.d. was calculated. Categorical variables were given as percentage of subjects with the respective attribute. χ2 tests were performed to test the differences of these attributes between male current smokers with and without blood samples.
A binary logistic regression was performed to assess the interaction between smoking quantity (1 = smoking 1-15 cigarettes per day, 2 = smoking more than 15 cigarettes per day) and CYP2A6 genotypes (1 = slower, 2 = intermediate, 3 = normal metabolizers) on hypertension. In this binary logistic regression, age, education level, alcohol consumption, physical exercise, family history of hypertension, BMI and WHR were first entered into the model for adjusting for their potential confounding effect; smoking quantity and CYP2A6 genotypes were then entered into the model to test for their main effects, and an interaction term between smoking quantity and CYP2A6 genotypes was then added into the model to test their interaction effect. In addition, according to smoking quantity and CYP2A6 genotypes, the subjects were divided into six groups taking smokers who consumed 1-15 cigarettes per day with slower CYP2A6 metabolizer genotype as the reference group; the effect sizes on hypertension of the other five groups were assessed by a binary logistic regression with adjusting for age, education level, alcohol consumption, physical exercise, family history of hypertension, and BMI and WHR. The six odds ratios (ORs) are presented graphically.
The frequencies of CYP2A6 *4, *5, *7, *9 and *10 alleles were in Hardy-Weinberg equilibrium (P>0.05). All P values were two-sided and statistical significance was P = 0.05. All the analyses were conducted with SPSS 13.0 (SPSS, Inc., Chicago, IL, USA).
Results
A comparison of the characteristics of male current smokers with different smoking quantities
There were significant differences of education level, alcohol consumption, exercise, abdominal obesity, hypertension and CYP2A6 genotypes between the two groups (details are presented in Table 1).
Table 1. Comparisons of study subject characteristics with different smoking quantity.
| Variables | Current smokers with 1-15 cigarettes per day (n = 545) | Current smokers with more than 15 cigarettes per day (n = 409) | χ2 | P value | ||
|---|---|---|---|---|---|---|
|
|
|
|||||
| No | % | No | % | |||
| Age (years) | 7.17 | 0.208 | ||||
| 20 - 29 | 43 | 7.9 | 18 | 4.4 | ||
| 30-39 | 65 | 11.9 | 49 | 12.0 | ||
| 40-49 | 85 | 15.6 | 80 | 19.6 | ||
| 50-59 | 181 | 33.2 | 140 | 34.2 | ||
| 60-69 | 131 | 24.0 | 97 | 23.7 | ||
| 70-86 | 40 | 7.4 | 25 | 6.1 | ||
| Occupation | 7.56 | 0.373 | ||||
| Worker | 131 | 24.0 | 104 | 25.4 | ||
| Farmer | 69 | 12.7 | 46 | 11.2 | ||
| Person in charge | 32 | 5.9 | 20 | 4.9 | ||
| Technician | 31 | 5.7 | 12 | 2.9 | ||
| Service personnel | 73 | 13.4 | 47 | 11.5 | ||
| Retired personnel | 121 | 22.2 | 101 | 24.7 | ||
| Jobless | 64 | 11.7 | 57 | 13.9 | ||
| Others | 24 | 4.4 | 22 | 5.4 | ||
| Education | 11.04 | 0.026 | ||||
| Illiteracy | 12 | 2.2 | 9 | 2.2 | ||
| Elementary school | 83 | 15.2 | 66 | 16.1 | ||
| Junior middle school | 185 | 33.9 | 153 | 37.4 | ||
| Senior middle school or vocational secondary school | 174 | 31.9 | 143 | 35.0 | ||
| College or above | 91 | 16.7 | 38 | 9.3 | ||
| Family monthly income (yuan) | 2.83 | 0.586 | ||||
| <1000 | 75 | 13.8 | 53 | 13.0 | ||
| 1000-2999 | 172 | 31.6 | 145 | 35.5 | ||
| 3000-4999 | 148 | 27.2 | 114 | 27.9 | ||
| ≥5000 | 95 | 17.4 | 59 | 14.2 | ||
| Do not know or refuse to answer | 55 | 10.1 | 39 | 9.5 | ||
| Family history of hypertension | 0.17 | 0.680 | ||||
| No | 377 | 69.2 | 288 | 70.4 | ||
| Yes | 168 | 30.8 | 121 | 29.6 | ||
| Alcohol consumption | 7.02 | 0.030 | ||||
| No | 364 | 66.8 | 239 | 58.4 | ||
| Yes | 154 | 28.3 | 145 | 35.5 | ||
| Former drinker | 27 | 5.0 | 25 | 6.1 | ||
| Exercise | 6.60 | 0.010 | ||||
| No | 190 | 34.9 | 176 | 43.0 | ||
| Yes | 355 | 65.1 | 233 | 57.0 | ||
| BMI | 3.87 | 0.145 | ||||
| Normal | 256 | 47.0 | 166 | 40.6 | ||
| Overweight | 275 | 50.5 | 231 | 56.5 | ||
| Obesity | 14 | 2.6 | 12 | 2.9 | ||
| Abdominal obesity | 12.23 | <0.001 | ||||
| No | 358 | 65.7 | 223 | 54.5 | ||
| Yes | 187 | 34.3 | 186 | 45.5 | ||
| Hypertension | 14.30 | <0.001 | ||||
| No | 379 | 69.5 | 236 | 57.7 | ||
| Yes | 166 | 30.5 | 173 | 42.3 | ||
| CYP2A6 genotype | 3.76 | 0.153 | ||||
| Slower metabolizers | 229 | 42.0 | 147 | 35.9 | ||
| Intermediate metabolizers | 73 | 13.4 | 64 | 15.6 | ||
| Normal metabolizers | 243 | 44.6 | 198 | 48.74 | ||
Abbreviation: BMI, body mass index.
The interaction between smoking quantity and CYP2A6 genotypes on hypertension
Table 2 and Figure 1 present the interaction of smoking quantity with CYP2A6 genotypes on hypertension. After adjusting for age, education, alcohol consumption, physical exercise, family history of hypertension, BMI and WHR, the smokers who consumed more than 15 cigarettes per day had a significantly higher risk of hypertension than the smokers who consumed 1-15 cigarettes per day (OR=1.59, 95% confidence interval (CI) = 1.21-2.10). In addition, normal CYP2A6 metabolizers had a significantly higher risk of hypertension than slower metabolizers (OR=1.75, 95% CI=1.30-2.36). The interaction analysis showed a significant interaction effect between smoking more than 15 cigarettes per day and normal CYP2A6 metabolizer genotype on hypertension (OR Normal metabolizers × smoking > 15 cigarettes per day = 2.04, 95% CI = 1.11 - 3.75) (Table 2). In the six groups of current smokers stratified by smoking quantity and CYP2A6 genotypes, adjusted ORs for hypertension increased from those with slower CYP2A6 metabolizer genotype, intermediate metabolizer genotype and normal metabolizer in both smoker groups, while the smokers who consumed more than 15 cigarettes per day with normal CYP2A6 metabolizer genotype had the highest risk of hypertension (OR = 2.74, 95% CI=1.82-4.12) compared with the smokers who consumed 1-15 cigarettes per day with slower CYP2A6 metabolizer genotype (Figure 2).
Table 2. Interaction between smoking quantity and CYP2A6 genotypes on hypertension in 954 Chinese male current smokers.
| Hypertension | Model 1 Adjusted OR (95% CI)b |
Model 2 Adjusted OR (95% CI)b |
Model 3 Adjusted OR (95% CI)b |
||
|---|---|---|---|---|---|
|
| |||||
| Controls N (%) | Cases N (%) | ||||
| Hypertensiona | |||||
| Daily cigarettes consumption | |||||
| 1-15 cigarettes per day | 381 (62.0) | 164 (48.4) | 1 | 1 | |
| >15 cigarettes per day | 234 (38.0) | 175 (51.6) | 1.59* (1.21-2.10) | 1.07 (0.0.68-1.71) | |
| CYP2A6 genotype | |||||
| Slower metabolizers | 264 (42.9) | 112 (33.0) | 1 | 1 | |
| Intermediate metabolizers | 93 (15.1) | 44 (13.0) | 1.10 (0.71-1.70) | 1.06 (0.59-1.90) | |
| Normal metabolizers | 258 (42.0) | 183 (54.0) | 1.75* (1.30-2.36) | 1.25 (0.84-1.88) | |
| Interaction effect | |||||
| Intermediate metabolizers × (> 15 cigarettes per day) | 1.16 (0.49-2.75) | ||||
| Normal metabolizers × (> 15 cigarettes per day) | 2.04* (1.11-3.75) | ||||
Abbreviations: CI, confidence interval; OR, odds ratio.
Dependent variable: hypertension (0 = no, 1 = yes).
Binary logistic regression model adjusted for age, education level, physical exercise, alcohol consumption, family history of hypertension, BMI and WHR.
P<0.05
Figure 2.
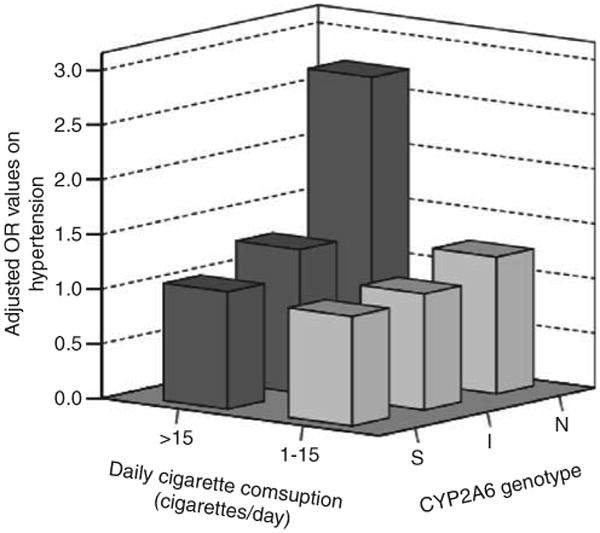
Effect size (adjusted ORs) of smoking quality and CYP2A6 genotypes on hypertension stratified by both levels of daily cigarette consumption and CYP2A6 genotypes in 954 Chinese male current smokers. The group with smokers who consumed 1 - 15 cigarettes per day and CYP2A6 slow metabolizer genotype was the reference group (OR=1). The adjusted variables were age, education level, physical exercise, alcohol consumption, family history of hypertension, BMI and WHR. N, CYP2A6 normal metabolizer genotype; I, CYP2A6 intermediate metabolizer genotype; S, CYP2A6 slower metabolizer genotype.
Discussion
In the present cross-sectional study in a community-based sample of Guangzhou and Zhuhai in Southern China, we found among current Chinese smokers that there was a significantly higher prevalence of hypertension in the smokers who consumed more than 15 cigarettes per day than the smokers who consumed 1-15 cigarettes per day. Interestingly, we further observed that smoking quantity and CYP2A6 genotypes might interact on risk for hypertension, such that the smokers who consumed more than 15 cigarettes per day with a normal CYP2A6 metabolizer genotype had significantly increased risk for hypertension compared with the smokers who consumed 1-15 cigarettes per day with a slower CYP2A6 metabolizer genotype.
Association between cigarette smoking and hypertension
The effect of cigarette smoking on hypertension remained consistent in recently published studies. Four prospective studies 3 in men consistently showed that heavy smoking (consuming more than 20 cigarettes per day) significantly increased the risk of incident hypertension with adjustment for age, BMI, physical exercise, alcohol intake and other confounders,5,6,8,41 and a prospective study in women found that smoking more than or equal to 15 cigarettes per day had a similar effect on increasing the risk for hypertension.7 Moreover, a population-based cross-sectional study in 12417 men indicated that current smoking was positively and significantly associated with systolic hypertension after adjusting for age, alcohol intake and BMI,42 and another cross-sectional study in a population-based sample of Vietnamese men found that men with smoking durations of over 30 years, or with lifetime smoking of over 20 pack-years, had a significantly higher rate of hypertension than those who had never smoked after controlling for age and BMI.43 Similar results were also obtained in the present study where we found that current smokers who consumed more than 15 cigarettes per day had a significantly higher risk for hypertension than the smokers who consumed 1-15 cigarettes per day after adjusting for age, education level, alcohol consumption, physical exercise, family history of hypertension, BMI and WHR. Together these studies confirm that cigarette smoking is an important risk factor for hypertension.
The interaction between smoking quantity and CYP2A6 genotypes on hypertension
The CYP2A6 enzyme not only activates some tobacco-specific nitrosamines into ultimate carcinogens but also alters smoking behaviors because of its participation in nicotine metabolic inactivation.44. Previous studies have reported that CYP2A6 genetic variation is related to smoking behaviors45,46 and the relationship between smoking quantity and risk of multiple cancers.44,47 Here, an interaction between smoking more than 15 cigarettes per day and CYP2A6 genotype on hypertension was observed, after adjustment for confounding factors. Compared with the smokers who consumed 1-15 cigarettes per day with slower CYP2A6 metabolizer genotypes, the smokers who consumed more than 15 cigarettes per day with normal CYP2A6 metabolizer genotypes had the highest risk of hypertension.
A potential explanation for the observed relationship between CYP2A6 genotypes, smoking and hypertension is as follows. Compared with light smokers, heavy smokers may be exposed to more harmful substances from cigarettes than light smokers. Moreover, smokers with normal CYP2A6 metabolism may smoke with increased mean puff volume and total puff volume compared with reduced CYP2A6 metabolizers, which could increase their overall exposure to harmful cigarette smoke constituents.23 As noted above, some harmful substances from cigarette smoke may cause oxidative stress,10 vasopressor effects,11 endothelial dys-function,12 vascular injury,14 increased arterial stiffness15 and markers of inflammation,13 all of which may be linked with the development of hypertension in smokers.16,17 Therefore, the combined effect of heavy smoking and normal CYP2A6 genotypes on smoking topography may increase inhaled cigarette toxicant exposure, thereby contributing to the risk of developing hypertension. In addition, we also analyzed the actual systole and diastolic blood pressure (mm Hg) in individuals with different CYP2A6 genotypes, and found higher systolic and diastolic blood pressure in normal CYP2A6 metabolizers than that in other CYP2A6 genotype metabolizers, although without statistical significance (see Appendix Table).
Appendix. The associations of CYP2A6 genotypes with systolic and diastolic blood pressure in 954 Chinese male current smokers.
| CYP2A6 genotypes | n (%) | Systolic blood pressure (mm Hg) | Diastolic blood pressure (mm Hg) | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
|
|
||||||||||||
| Mean±s.d. | F | P | Mean±s.e.a | F | P | Mean±s.d. | F | P | Mean±s.e.a | F | P | ||
| Slower metabolizers | 376 (39.4%) | 124.0 ± 18.6 | 1.81 | 0.165 | 124.0 ± 0.9 | 2.47 | 0.085 | 80.8 ± 11.0 | 0.47 | 0.623 | 80.7 ± 0.5 | 0.86 | 0.422 |
| Intermediate metabolizers | 137 (14.4%) | 125.5 ± 20.5 | 125.2 ± 1.6 | 80.7 ± 10.3 | 80.8 ± 0.9 | ||||||||
| Normal metabolizers | 441 (46.2%) | 126.6 ± 18.3 | 126.8 ± 0.9 | 81.5 ± 10.9 | 81.6 ± 0.5 | ||||||||
General linear model adjusted for age, education level, physical exercise, alcohol consumption, family history of hypertension, BMI and WHR.
Limitations
Several limitations may influence the interpretation of results. First, this was a cross-sectional study design. Therefore, the data do not permit making conclusions about a causal relationship. Second, the data was retrospectively collected with a self-administrated questionnaire that may lead to recall bias. Third, antihypertensive medication was not assessed, which might impact the measurement of blood pressure and the relationship between smoking, genotype and hypertension. Fourth, sample selection bias might result in less healthy individuals being over-represented among those who did not take part in the study. Moreover, females were not included in the final analyses because of very few female smokers, limiting generalizability. However, we do not expect that such selection biases substantially affected our findings. Another potential limitation is that although higher frequency variants with functional impact were assessed, not all CYP2A6 genetic variants were assayed in this study, which might lead to misclassification of CYP2A6 genotypes. Furthermore, because of the relative size of the final study sample, statistical power was insufficient to analyze the effect of smoking quantity (continuous measure, or more detail categories, such as 1 - 5, 5-10 cigarettes per day) on hypertension. Finally, participants' dietary and drug histories were not investigated that might affect the activity of CYP2A6(ref. 18) and further distort the relationship of CYP2A6 genotypes with hypertension. For instance, grapefruit juice can inhibit CYP2A6-mediated coumarin metabolism,48 but phenobarbital and rifampin can induce CYP2A6 activity.49
In summary, this study revealed that smoking quantity was positively associated with hypertension and CYP2A6 genotypes might moderate this relationship in Chinese male current smokers. These findings expand on our understanding of the effect, and possible mechanisms involved, in the relationship between cigarettes smoking and hypertension.
What was known about this topic
Smoking is a risk factor of hypertension.
Smoking and CYP2A6 genotype interacts to affect the risk for smoking-related cancers.
Whether CYP2A6 genotypes moderate the association between smoking and hypertension is unknown.
What this study adds
Smoking more than 15 cigarettes per day significantly increased the risk of hypertension compared with smoking 1-15 cigarettes per day.
Smoking more than 15 cigarettes per day interacted with normal CYP2A6 metabolizer genotype to increase the risk of hypertension compared with the smokers who consumed 1-15 cigarettes per day also with slower CYP2A6 metabolizer genotype.
Acknowledgments
This study was funded by the Guangzhou Health Bureau (2005-Zda-001) and National Institute on Drug Abuse/National Institutes of Health grants (K08-014276 and R21-027331). RFT acknowledges the support of CRC, CIHR and CAMH.
Footnotes
Conflict of Interest: Dr RF Tyndale holds shares in Nicogen, a company focused on the development of novel smoking cessation treatments. No support was provided by Nicogen for this study and the manuscript was not reviewed by other members of the company. Dr RF Tyndale has also consulted for Novartis on tobacco cessation. All other authors declare no conflicts of interests.
References
- 1.Helios P, Rodicio JL. European Society of Hypertension Scientific Newsletters: Update on Hypertension Management, high blood pressure, smoking and cardiovascular risk. J Hypertens. 2005;23:219–229. doi: 10.1097/00004872-200501000-00037. [DOI] [PubMed] [Google Scholar]
- 2.Skurnik Y, Shoenfeld Y. Health effects of cigarette smoking. Clin Dermatol. 1998;16:545–556. doi: 10.1016/s0738-081x(98)00037-6. [DOI] [PubMed] [Google Scholar]
- 3.Winniford MD. Smoking and cardiovascular function. J Hypertens Suppl. 1990;8:S17–S23. [PubMed] [Google Scholar]
- 4.Tuomilehto J, Elo J, Nissinen A. Smoking among patients with malignant hypertension. Br Med J (Clin Res Ed) 1982;284:1086. doi: 10.1136/bmj.284.6322.1086. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Dochi M, Sakata K, Oishi M, Tanaka K, Kobayashi E, Suwazono Y. Smoking as an independent risk factor for hypertension: a 14-year longitudinal study in male Japanese workers. Tohoku J Exp Med. 2009;217:37–43. doi: 10.1620/tjem.217.37. [DOI] [PubMed] [Google Scholar]
- 6.Niskanen L, Laaksonen DE, Nyyssonen K, Punnonen K, Valkonen VP, Fuentes R, et al. Inflammation, abdominal obesity, and smoking as predictors of hypertension. Hypertension. 2004;44:859–865. doi: 10.1161/01.HYP.0000146691.51307.84. [DOI] [PubMed] [Google Scholar]
- 7.Bowman TS, Gaziano JM, Buring JE, Sesso HD. A prospective study of cigarette smoking and risk of incident hypertension in women. J Am Coll Cardiol. 2007;50:2085–2092. doi: 10.1016/j.jacc.2007.08.017. [DOI] [PubMed] [Google Scholar]
- 8.Halperin RO, Gaziano JM, Sesso HD. Smoking and the risk of incident hypertension in middle-aged and older men. Am J Hypertens. 2008;21:148–152. doi: 10.1038/ajh.2007.36. [DOI] [PubMed] [Google Scholar]
- 9.Narkiewicz K, van de Borne PJ, Hausberg M, Cooley RL, Winniford MD, Davison DE, et al. Cigarette smoking increases sympathetic outflow in humans. Circulation. 1998;98:528–534. doi: 10.1161/01.cir.98.6.528. [DOI] [PubMed] [Google Scholar]
- 10.Burke A, Fitzgerald GA. Oxidative stress and smoking-induced vascular injury. Prog Cardiovasc Dis. 2003;46:79–90. doi: 10.1016/s0033-0620(03)00076-8. [DOI] [PubMed] [Google Scholar]
- 11.Barutcu I, Esen AM, Degirmenci B, Acar M, Kaya D, Turkmen M, et al. Acute cigarette smoking-induced hemodynamic alterations in the common carotid artery-a transcranial Doppler study. Circ J. 2004;68:1127–1131. doi: 10.1253/circj.68.1127. [DOI] [PubMed] [Google Scholar]
- 12.Li H, Srinivasan SR, Chen W, Xu JH, Li S, Berenson GS. Vascular abnormalities in asymptomatic, healthy young adult smokers without other major cardiovascular risk factors: the Bogalusa Heart Study. Am J Hypertens. 2005;18:319–324. doi: 10.1016/j.amjhyper.2004.10.005. [DOI] [PubMed] [Google Scholar]
- 13.Bazzano LA, He J, Muntner P, Vupputuri S, Whelton PK. Relationship between cigarette smoking and novel risk factors for cardiovascular disease in the United States. Ann Intern Med. 2003;138:891–897. doi: 10.7326/0003-4819-138-11-200306030-00010. [DOI] [PubMed] [Google Scholar]
- 14.Sharrett AR, Ding J, Criqui MH, Saad MF, Liu K, Polak JF, et al. Smoking, diabetes, and blood cholesterol differ in their associations with subclinical atherosclerosis: the Multiethnic Study of Atherosclerosis (MESA) Atherosclerosis. 2006;186:441–447. doi: 10.1016/j.atherosclerosis.2005.08.010. [DOI] [PubMed] [Google Scholar]
- 15.Narkiewicz K, Kjeldsen SE, Hedner T. Is smoking a causative factor of hypertension? Blood Press. 2005;14:69–71. doi: 10.1080/08037050510034202. [DOI] [PubMed] [Google Scholar]
- 16.Sesso HD, Buring JE, Rifai N, Blake GJ, Gaziano JM, Ridker PM. C-reactive protein and the risk of developing hypertension. JAMA. 2003;290:2945–2951. doi: 10.1001/jama.290.22.2945. [DOI] [PubMed] [Google Scholar]
- 17.Oparil S, Zaman MA, Calhoun DA. Pathogenesis of hypertension. Ann Intern Med. 2003;139:761–776. doi: 10.7326/0003-4819-139-9-200311040-00011. [DOI] [PubMed] [Google Scholar]
- 18.Hukkanen J, Jacob P, 3rd, Benowitz NL. Metabolism and disposition kinetics of nicotine. Pharmacol Rev. 2005;57:79–115. doi: 10.1124/pr.57.1.3. [DOI] [PubMed] [Google Scholar]
- 19.Carter BL, Long TY, Cinciripini PM. A meta-analytic review of the CYP2A6 genotype and smoking behavior. Nicotine Tob Res. 2004;6:221–227. doi: 10.1080/14622200410001676387. [DOI] [PubMed] [Google Scholar]
- 20.Schoedel KA, Hoffmann EB, Rao Y, Sellers EM, Tyndale RF. Ethnic variation in CYP2A6 and association of genetically slow nicotine metabolism and smoking in adult Caucasians. Pharmacogenetics. 2004;14:615–626. doi: 10.1097/00008571-200409000-00006. [DOI] [PubMed] [Google Scholar]
- 21.Gu DF, Hinks LJ, Morton NE, Day IN. The use of long PCR to confirm three common alleles at the CYP2A6 locus and the relationship between genotype and smoking habit. Ann Hum Genet. 2000;64:383–390. doi: 10.1046/j.1469-1809.2000.6450383.x. [DOI] [PubMed] [Google Scholar]
- 22.Lerman C, Jepson C, Wileyto EP, Patterson F, Schnoll R, Mroziewicz M, et al. Genetic variation in nicotine metabolism predicts the efficacy of extended-duration transdermal nicotine therapy. Clin Pharmacol Ther. 2010;87:553–557. doi: 10.1038/clpt.2010.3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Strasser AA, Malaiyandi V, Hoffmann E, Tyndale RF, Lerman C. An association of CYP2A6 genotype and smoking topography. Nicotine Tob Res. 2007;9:511–518. doi: 10.1080/14622200701239605. [DOI] [PubMed] [Google Scholar]
- 24.Nakajima M, Yokoi T. Interindividual variability in nicotine metabolism: C-oxidation and glucuronidation. Drug Metab Pharmacokinet. 2005;20:227–235. doi: 10.2133/dmpk.20.227. [DOI] [PubMed] [Google Scholar]
- 25.Mwenifumbo JC, Tyndale RF. Genetic variability in CYP2A6 and the pharmacokinetics of nicotine. Pharmacogenomics. 2007;8:1385–1402. doi: 10.2217/14622416.8.10.1385. [DOI] [PubMed] [Google Scholar]
- 26.Fujieda M, Yamazaki H, Saito T, Kiyotani K, Gyamfi MA, Sakurai M, et al. Evaluation of CYP2A6 genetic polymorphisms as determinants of smoking behavior and tobacco-related lung cancer risk in male Japanese smokers. Carcinogenesis. 2004;25:2451–2458. doi: 10.1093/carcin/bgh258. [DOI] [PubMed] [Google Scholar]
- 27.Derby KS, Cuthrell K, Caberto C, Carmella SG, Franke AA, Hecht SS, et al. Nicotine metabolism in three ethnic/racial groups with different risks of lung cancer. Cancer Epidemiol Biomarkers Prev. 2008;17:3526–3535. doi: 10.1158/1055-9965.EPI-08-0424. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Tiwawech D, Srivatanakul P, Karalak A, Ishida T. Cytochrome P450 2A6 polymorphism in nasopharyngeal carcinoma. Cancer Lett. 2006;241:135–141. doi: 10.1016/j.canlet.2005.10.026. [DOI] [PubMed] [Google Scholar]
- 29.Kadlubar S, Anderson JP, Sweeney C, Gross MD, Lang NP, Kadlubar FF, et al. Phenotypic CYP2A6 variation and the risk of pancreatic cancer. JOP. 2009;10:263–270. [PMC free article] [PubMed] [Google Scholar]
- 30.Song DK, Xing DL, Zhang LR, Li ZX, Liu J, Qiao BP. Association of NAT2, GSTM1, GSTT1, CYP2A6, and CYP2A13 gene polymorphisms with susceptibility and clinicopathologic characteristics of bladder cancer in Central China. Cancer Detect Prev. 2009;32:416–423. doi: 10.1016/j.cdp.2009.02.003. [DOI] [PubMed] [Google Scholar]
- 31.Ruwali M, Pant MC, Shah PP, Mishra BN, Parmar D. Polymorphism in cytochrome P450 2A6 and glutathione S-transferase P1 modifies head and neck cancer risk and treatment outcome. Mutat Res. 2009;669:36–41. doi: 10.1016/j.mrfmmm.2009.04.007. [DOI] [PubMed] [Google Scholar]
- 32.Wang H, Qiu Q, Tan LL, Liu T, Deng XQ, Chen YM, et al. Prevalence and determinants of diabetes and impaired fasting glucose among urban community-dwelling adults in Guangzhou, China. Diabetes Metab. 2009;35:378–384. doi: 10.1016/j.diabet.2009.03.006. [DOI] [PubMed] [Google Scholar]
- 33.Centers for Disease Control. National Health Interview Survey: Early release of selected estimates based on data from January to September 200. [Accessed 1 April 2011]; www.cdc.gov.
- 34.Primatesta P, Falaschetti E, Gupta S, Marmot MG, Poulter NR. Association between smoking and blood pressure: evidence from the health survey for England. Hypertension. 2001;37:187–193. doi: 10.1161/01.hyp.37.2.187. [DOI] [PubMed] [Google Scholar]
- 35.Wen W, Xiang YB, Zheng W, Xu WH, Yang G, Li H, et al. The association of alcohol, tea, and other modifiable lifestyle factors with myocardial infarction and stroke in Chinese men. CVD Prev Control. 2008;3:133–140. doi: 10.1016/j.cvdpc.2008.07.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Park MS, Chung SY, Chang Y, Kim K. Physical activity and physical fitness as predictors of all-cause mortality in Korean men. J Korean Med Sci. 2009;24:13–19. doi: 10.3346/jkms.2009.24.1.13. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.WHO/IASO/IOTF. Melbourne: Health Communications Australia. Vol. 18. 2000. The Asia-Pacific perspective: redefining obesity and its treatment. [Google Scholar]
- 38.Adamu GB, Onyemelukwe GC. Indices of obesity among type-2 diabetic Hausa-Fulani Nigerians. Int J Diabetes & Metabolism. 2005;13:28–29. [Google Scholar]
- 39.Liu T, David SP, Tyndale RF, Wang H, Zhou Q, Ding P, et al. Associations of CYP2A6 genotype with smoking behaviors in southern China. Addiction. 2011;106:985–994. doi: 10.1111/j.1360-0443.2010.03353.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Mancia G, De Backer G, Dominiczak A, Cifkova R, Fagard R, Germano G, et al. 2007 ESH-ESC Practice Guidelines for the Management of Arterial Hypertension: ESH-ESC Task Force on the Management of Arterial Hypertension. J Hypertens. 2007;25:1751–1762. doi: 10.1097/HJH.0b013e3282f0580f. [DOI] [PubMed] [Google Scholar]
- 41.Okubo Y, Suwazono Y, Kobayashi E, Nogawa K. An association between smoking habits and blood pressure in normotensive Japanese men: a 5-year follow-up study. Drug Alcohol Depend. 2004;73:167–174. doi: 10.1016/j.drugalcdep.2003.10.005. [DOI] [PubMed] [Google Scholar]
- 42.Halimi JM, Giraudeau B, Vol S, Caces E, Nivet H, Tichet J. The risk of hypertension in men: direct and indirect effects of chronic smoking. J Hypertens. 2002;20:187–193. doi: 10.1097/00004872-200202000-00007. [DOI] [PubMed] [Google Scholar]
- 43.Thuy AB, Blizzard L, Schmidt MD, Luc PH, Granger RH, Dwyer T. The association between smoking and hypertension in a population-based sample of Vietnamese men. J Hypertens. 2010;28:245–250. doi: 10.1097/HJH.0b013e32833310e0. [DOI] [PubMed] [Google Scholar]
- 44.Rossini A, de Almeida Simao T, Albano RM, Pinto LF. CYP2A6 polymorphisms and risk for tobacco-related cancers. Pharmacogenomics. 2008;9:1737–1752. doi: 10.2217/14622416.9.11.1737. [DOI] [PubMed] [Google Scholar]
- 45.Pianezza ML, Sellers EM, Tyndale RF. Nicotine metabolism defect reduces smoking. Nature. 1998;393:750. doi: 10.1038/31623. [DOI] [PubMed] [Google Scholar]
- 46.Tyndale RF, Sellers EM. Genetic variation in CYP2A6-mediated nicotine metabolism alters smoking behavior. Ther Drug Monit. 2002;24:163–171. doi: 10.1097/00007691-200202000-00026. [DOI] [PubMed] [Google Scholar]
- 47.Kamataki T, Fujieda M, Kiyotani K, Iwano S, Kunitoh H. Genetic polymorphism of CYP2A6 as one of the potential determinants of tobacco-related cancer risk. Biochem Biophys Res Commun. 2005;338:306–310. doi: 10.1016/j.bbrc.2005.08.268. [DOI] [PubMed] [Google Scholar]
- 48.Runkel M, Bourian M, Tegtmeier M, Legrum W. The character of inhibition of the metabolism of 1, 2-benzopyrone (coumarin) by grapefruit juice in human. Eur J Clin Pharmacol. 1997;53:265–269. doi: 10.1007/s002280050374. [DOI] [PubMed] [Google Scholar]
- 49.Madan A, Graham RA, Carroll KM, Mudra DR, Burton LA, Krueger LA, et al. Effects of prototypical microsomal enzyme inducers on cytochrome P450 expression in cultured human hepatocytes. Drug Metab Dispos. 2003;31:421–431. doi: 10.1124/dmd.31.4.421. [DOI] [PubMed] [Google Scholar]