

Abstract
Objective: To study the accuracy of fine needle aspiration biopsy (FNAB) processed by smear cytology and cell block (CB) techniques for the diagnosis of lacrimal gland tumors (LGTs). Study Design: In a prospective study, we enrolled 48 consecutive patients with LGTs. Immediately after excision of LGTs, the tissues were underwent FNAB with 23-gauge needles. The FNAB samples were processed to produce cytologic smears and CB from which slides were cut for immunohistochemical staining. The remainders were submitted for routine histopathologic processing. The diagnostic value of FNAB was assessed by comparing the FNAB diagnoses to those made by routine histopathology. Results: Cytopathologic evaluations based on smear cytology and CB with sections stained immunohistochemically can distinguish non-epithelial lesions from epithelial ones in all cases. The diagnostic sensitivities, specificities, and accuracies for distinguishing benign from malignant lesions were: cytologic smears--76%, 68%, and 71%, respectively; CB with immunohistochemical staining--88%, 87%, and 88%, respectively. The accuracy of the tissue diagnosis compared to routine histopathology was less for cytologic smears (58%) than for CB with immunohistochemistry (81%; P < 0.05). Conclusions: FNAB of LGT processed using a CB technique capable of producing immunohistochemically stained slides results in a greater percentage of accurate tissue diagnoses than do cytologic smears, when compared to routine histopathology.
Keywords: Lacrimal gland lesions, fine needle aspiration, cell blocks, immnohistichemistry, cytopathology
Introduction
Lacrimal gland tumors (LGTs) consist of a diverse group of diseases that account for 9% of all orbital tumors. Three main types of lesions occur: inflammatory lesions, lymphoid disorders and epithelial tumors [1]. The preoperative diagnosis is mainly based on the clinical symptoms and imaging data, but these findings are often insufficient to establish a reliable diagnosis due to the fact that many LGTs can show similar characteristics on imaging and may be misdiagnosed as other tumors [2-4]. Besides, the treatment for different lesions is quite different. For example, most inflammatory lesions and lymphoid disorders are usually treated medically with or without radiation therapy, while epithelial tumors are primarily treated surgically with only adjunctive radiotherapy and/or chemotherapy [5-7]. Therefore, it is desirable and of great importance to build a reliable preoperative diagnosis technique.
Incisional biopsy, a common technique, has been wildly used in the diagnosis of orbital tumors other than LGTs [8-11]. The technique in LGTs has been doubted because it may increase the risk of tumor recurrence or malignant transformation [12-14]. Moreover, this technique also troubled many orbital surgeons due to undesirable cosmetic problems [4]. Fine needle aspiration biopsy (FNAB), a minimally invasive method for obtaining pathologic material to arrive at a tissue diagnosis, has attracted much attention. And this method as a safe, cost-effective, rapid, and accurate diagnostic method, had been widely used in the diagnosis of breast tumors, thyroid tumors and orbital tumors [15-20].
Typically, the material is used to prepare cytologic smears which, when stained conventionally, are interpreted to arrive at the diagnosis based on morphology and tinctorial characteristics. Centrifugation of the FNAB material to form a cell block (CB) permits sectioning for routine pathologic staining and for immunohistochemistry which is valuable in identifying distinctive immunoreactive profiles of various cell types, adding greatly to diagnostic accuracy. Heretofore, studies of FNAB processed by cytologic smear and CB techniques for the diagnosis of LGT are rare. So we designed and performed a prospective study in 48 patients to evaluate FNAB in the diagnosis of LGT.
Materials and methods
Patients
This is a single-center prospective study performed at Eye & ENT Hospital of Fudan University. The inclusion criteria to be met were as follows: (1) age greater than 18 years and able to provide informed consent, (2) LGT diagnosed by the computerized tomography or magnetic resonance imaging (3) need for surgery or biopsy to diagnose or treat the LGT. The patients with typical dacryoadenitis (pseudotumor) were excluded.
Study design
Between December 2009 and May 2012, 48 patients with LGT were studied. FNAB of excised tissue was performed after removal from the patient during the immediate post-operative period. The removed tissue underwent standard FNAB by a pathologist using a 23-gauge needle attached to a 10 ml plastic syringe (Becton Dickinson S.A. Spain). Each tissue specimen was biopsied through the same perforation by four passes of the needle through the tissue with negative pressure was maintained on the syringe in order to obtain enough pathologic material for processing. The tissue adsorbed in the needle was pushed out on to glass slides for the preparation of cytologic smears. And for preparation of CB, the tissue was dispersed into 10% formalin in a 1.5 ml of conical polypropylene centrifuge tubes. For a compare, the excised specimens were submitted for routine histopathological examination.
Cytologic smears were immediately fixed by 95% ethanol, and three glass slides were prepared for Papanicolaou stain, Hematoxylin-eosin (H&E) stain and Wright’s stain, respectively. Two pathologists made cytological diagnosis while simultaneously viewing the slides through the light microscope. Each diagnosis included information indicating the final diagnosis and comments as to whether the LGT was epithelial or non-epithelial and benign or malignant.
CB sections were made by a routine agar-paraffin embedding technique. First, two CB sections were prepared from each CB for H&E staining upon which a diagnosis was rendered. Second, for epithelial LGT, CK, P53, Ki-67, S-100, and CEA immunostains were performed on CB sections; for non-epithelial lesions, immunostains for CD20, CD3, CD45RO, Ki-67, κ Light Chain, and λ Light Chain were made on CB sections. The sources, types, codes, and dilutions of these antibodies are shown in Table 1. The H&E and immunohistochemically stained sections were then evaluated by the same two pathologists simultaneously viewing them at the light microscope to render the final diagnosis with comments made on the epithelial or non-epithelial and benign or malignant nature of the LGT.
Table 1.
Sources, type, clone, and dilutions of primary antibodies used for immunostaining
| Antibody | Source | Type | Clone/Code | Dilution |
|---|---|---|---|---|
| CK | DAKO, DK | Mouse IgG1 | AE1/AE3 | 1:200 |
| S-100 | DAKO, DK | Rabbit anti- | Z0311 | 1:400 |
| P53 | DAKO, DK | Mouse IgG2b | DO-7 | 1:100 |
| Ki-67 | DAKO, DK | Mouse IgG1 | MIB-1 | 1:100 |
| CEA | DAKO, DK | Mouse IgG1 | II-7 | 1:100 |
| CD20 | DAKO, DK | Mouse IgG2a | L26 | 1:200 |
| CD3 | DAKO, DK | Mouse IgG1 | F7.2.38 | 1:200 |
| CD45RO | DAKO, DK | Mouse IgG2a | UCHL1 | 1:200 |
| κ Light Chain | DAKO, DK | Rabbit anti- | A0192 | 1:100 |
| λ Light Chain | DAKO, DK | Rabbit anti- | A0193 | 1:100 |
Statistical analysis
The accuracies of the cytologic smear and CB techniques were compared with the diagnosis rendered by routine histopathology of the excised specimen. Statistical analyses were performed by the χ2 test or Fish test or Fisher’s exact test where appropriate. Differences were considered significant when P < 0.05.
Results
A total of 48 LGT of 48 patients were analyzed. Histopathology of 31 LGT revealed epithelial lesions: 19 PAs, 6 adenoid cystic carcinomas (ACCs), 4 carcinomas ex-pleomorphic adenoma, and 2 primary adenocarcinomas. Histopathology of 17 LGT revealed non-epithelial tumors: 6 inflammatory lesions, 6 lymphoid hyperplasias, 4 lymphomas and 1 fibrosarcoma.
Diagnostic values of cytologic smear and CB techniques
The accuracies of the cytologic smear and CB techniques with immunohistochemistry in distinguishing benign from malignant lesions when compared to routine histopathology are shown in Table 2. For cytologic smears, the sensitivity was 76%, but the specificity and accuracy were only 68% and 71%, respectively. In contrast, the sensitivity, specificity and accuracy of the CB with immunohistochemistry technique were 88%, 87%, and 88%, respectively, and much higher than that of cytologic smears, indicating that this technique is better in distinguishing benign lesions from malignant lesions.
Table 2.
Diagnostic efficacies of smear cytology and CB method with immunostaining to distinguish benign lesions from malignant lesions
| Final diagnosis | Smear cytology | CB method with immunostaining | |||
|
| |||||
| malignant | benign | malignant | benign | ||
|
| |||||
| Malignant | 13 | 4 | 15 | 2 | |
| Benign | 10 | 21 | 4 | 27 | |
|
| |||||
| Smear cytology | CB method with immunostaining | P value | |||
|
| |||||
| Sensitivity | 76.47% (13/17) | 88% (15/17) | 0.65 | ||
| Specificity | 67.74% (21/31) | 87% (27/31) | 0.13 | ||
| PPV | 56.52% (13/23) | 79% (15/19) | 0.19 | ||
| NPV | 84.00% (21/25) | 93% (27/29) | 0.40 | ||
| Accuracy | 70.83% (34/48) | 88% (42/48) | 0.08 | ||
CB, cell block; PPV, positive predictive value; NPV, negative predictive value.
Then, the diagnostic efficacies from FNAB processed by the two techniques were compared to the pathologic ones rendered by routine histopathology (Table 3). The accuracy of CB with immunohistochemistry was 81% and significantly higher than that (58%) of cytologic smears (p < 0.05).
Table 3.
Diagnostic efficacies of smear cytology and CB method with immunostaining for final diagnosis
| Final diagnosis | cases | Smear cytology (diagnostic accuracy) | CB method with immunostaining (diagnostic accuracy) | P value |
|---|---|---|---|---|
| Epithelial lesions | 31 | 71% (22/31) | 81% (25/31) | 0.55 |
| PA | 19 | 93% (18/19) | 93% (18/19) | 1.00 |
| Carcinoma ex-pleomophic adenoma | 4 | 25% (1/4) | 50% (2/4) | - |
| ACC | 6 | 33% (2/6) | 67% (4/6) | 0.57 |
| Primary adenocarcinoma | 2 | 50% (1/2) | 50% (1/2) | - |
| Non-epithelial lesions | 17 | 35% (6/17) | 82% (14/17) | 0.01 |
| Lymphoma | 4 | 100% (4/4) | 100% (4/4) | - |
| Inflammatory lesions | 6 | 17% (1/6) | 83% (5/6) | 0.08 |
| Lymphoid hyperplasia diseases | 6 | 0% (0/6) | 67% (4/6) | 0.06 |
| Fibrosarcoma | 1 | 100% (1/1) | 100% (1/1) | - |
| SOLs of the lacrimal gland | 48 | 58% (28/48) | 81% (39/48) | 0.03 |
CB, cell block; PA, pleomorphic adenoma; ACC, adenoid cystic carcinoma; SOLs, Space-occupying lesions.
Cytopathological findings
The most common epithelial LGT was PA and the most common malignant epithelial LGT was ACC [1]. PAs show typical cytopathologic characteristics with uniform, cytologically bland epithelial cells arranged in cohesive clusters, individually or in tubular arrangements in extracellular myxoid stroma containing variable degrees of cellularity (Figure 1) [21]. In contrast, the malignant epithelial tumors exhibite basaloid cells arranged in cohesive clusters or individually, with dark round to oval nuclei with considerable variability in size and shape, in a scant extracellular myxoid stroma with high degrees of cellularity (Figure 2) [22,23].
Figure 1.
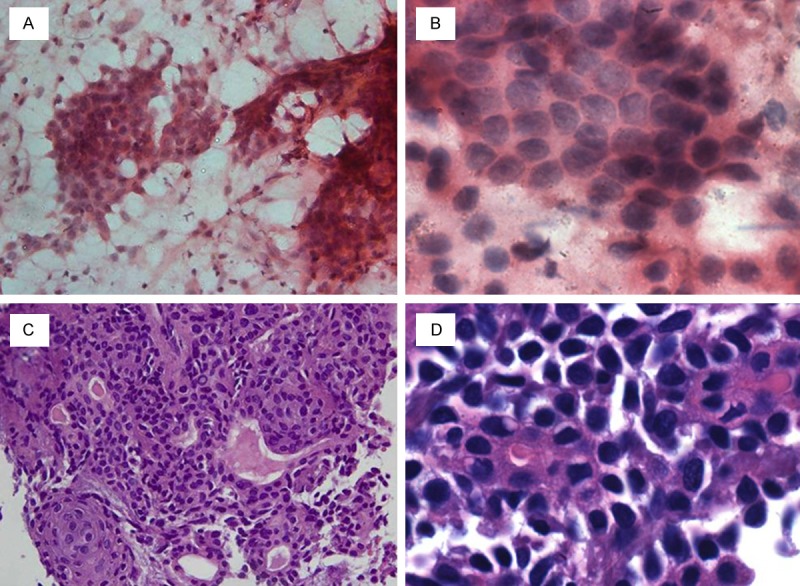
Smears (A, B) and cell block sections (C, D) of pleomorphic adenoma stained with hematoxylin-eosin. (Original magnification: A and C, × 400; B and D, × 1000).
Figure 2.

Smears (A, B) and cell block sections (C, D) of adenoid cystic carcinoma stained with hematoxylin-eosin. (Original magnification: A and C, × 400; B and D, × 1000).
The non-epithelial LGT includes inflammatory and lymphoid lesions. The inflammatory lesions show mixed lymphoid population (Figure 3A, 3B). In lymphoid hyperplasia leisons, there are numerous lymphocytes with tingible body macrophages and phagocytosis (Figure 3C, 3D). While, the lymphoma lesions showed numerous monomorphic lymphocytes (Figure 3E, 3F).
Figure 3.

Papanicolaou stained smear (A) and hematoxylin-eosin stained CB section (D) of inflammatory lesions; Wrigh’s stained smear (B) and hematoxylin-eosin stained CB section (E) of lymphoid hyperplasia diseases; hematoxylin-eosin stained smear (C) and CB section (F) of lymphoma. (All images, original magnification: × 1000).
Discussion
The safety of FNAB for the diagnosis of LGT has been questioned due to the potential risk of tumor recurrence caused by disruption of the LGT pseudocapsule which leads tumor seeding along the needle track [13,14]. However, there have been no reports of recurrence due to the use of FNAB [24] or evidence of tumor seeding upon serially sectioning the needle track [25,26]. In addition, Lai et al [27] in a systematic review of the literature concerning recurrence of LGT after incomplete excision or biopsy found that inadequate excision rather than FNAB led to greater risk of recurrence.
We found that PAs can be distinguished from malignant epithelial tumors by their typical cytopathologic characteristics. However, only through the malignant cellular characteristics, it is difficult to distinguish carcinomas ex-pleomorphic adenoma from ACC or primary adenocarcinomas. The tumor histopathologic features such as the cytomorphological features and histological growth patterns: the cribriform, solid and tubular forms in ACC were hardly observed in FNAB tissue. Besides the diagnosis accuracy was influenced by the limited number of cases and diagnosis experiences. In our study, 3 carcinomas ex-pleomorphic adenoma, 4 ACC, and 1 adenocarcinoma were demonstrated discrepancies based on FNAB compared to routine histopathologic assessment.
It has been reported that the usage of P53, Ki-67, S-100, and CEA in CB sections is helpful to distinguish epithelial tumors [28-30]. However, these usages have no obvious advantages in rendering a diagnosis based on the FNAB in our study. For epithelial tumors, the diagnostic accuracy of the CB technique with immunohistochemistry (81%) was higher than that of the cytologic smear technique (71%), but the difference was not statistically significant (P < 0.05). This may partly due to the limited cases and the selected markers (P53, Ki-67, S-100, and CEA) in our study, which may be insufficient to distinguish these tumors completely. We are still looking forward to discovering some potential markers in distinguishing the epithelial tumors.
The diagnosis of non-epithelial lesions often depends on structural changes, including the presence and type of lymphoid follicles which can assist in distinguishing inflammatory or reactive lymphoid infiltrates from malignant lymphoid tumors. The patterns of infiltration by malignant lymphocytes are another feature that assists in this differentiation. However, samples obtained by FNAB cannot offer such structural information. In our series, there was a high false positive rate for the diagnosis of lymphoma due to the fact that LGT in which lymphocytes infiltrated fragments of lacrimal gland epithelium in the FNAB samples were diagnosed as lymphoma. Thus, 4 inflammatory LGT and 5 LGT due to lymphoid hyperplasia were misdiagnosed as lymphoma, resulting in low diagnostic accuracy of 17% and 0% for these two types of benign LGT.
Immunohistochemistry is considered to be useful in distinguishing benign inflammatory LGT from malignant lymphoma [31]. Ki-67 nuclear immunopositivity, a measure of cellular proliferation, is useful in distinguishing inflammatory lesions which do not stain and lymphoid disorders which show positive staining [32]. In as much as lymphoma is a monoclonal disease and lymphoid hyperplasia disease is a polyclonal disease, patterns for CD20, CD3, and κ and λ light immunoglobulin chain immunohistochemical staining is often useful in rendering a pathologic diagnosis. In our study, 5 of 6 inflammatory LGT did not stain with Ki-67, and all 10 LGT due to lymphoid disorders stained for Ki-67. All 4 LGT due to lymphoma show a preponderance of CD20 immunopositivity with little or no CD3 positivity along with immunostaining positive for λ light immunoglobulin chain rather than κ light immunoglobulin chain. While, all 6 LGT attributed to lymphoid hyperplasia show a diffused immunopositivity CD20 and CD3 along with immnustaing positive for both κ and λ light immunoglobulin chain. The typical results of FNAB immunostaining in CB sections for non-specific inflammation (Figure 4), lymphoid hyperplasia (Figure 5), and lymphoma (Figure 6) of the LGT are shown in our study. Hence, for 17 LGT of non-epithelial lesions, the diagnostic accuracy of the CB technique with immunohistochemistry (82%) was higher than that of the cytologic smear technique (35%) (P < 0.05).
Figure 4.

Non-specific inflammation with positivity for CD3 (A), CD45RO (B), and CD20 (C), but lack of Ki-67 (D) immunopositivity. (Immunoperoxidase reaction, all images, original magnification: × 1000).
Figure 5.

Lymphoid hyperplasia with positivity for CD3 (A), CD20 (B), and Ki-67 (C). Immunopositivity for κ (D) and λ (E) light chains is seen. (Immunoperoxidase reaction, all images, original magnification: × 1000).
Figure 6.

Lymphoma with positivity for CD20 (A) and Ki-67 (C), but lack of immunostaining for CD3 (B). Light chain restriction with positivity for λ light chains (E) and lack of staining for κ light chains (D). (Immunoperoxidase reaction, all images, original magnification: × 1000).
In our study, we did not perform cytologic smears with immunostaining because there are several problems in attempting to perform this type of analysis. First, many samples have a limited amount of cellular material. When distributed by smearing over several slides, results in loss of diagnostic material that may render the FNAB non-diagnostic. Second, antibodies may be trapped by the three-dimensional cell groups, leading to nonspecific immunostaining. Third, cellular disruption during the process of mechanically smearing the sample may result in antigen leakage and either diffuse positivity or loss that is not localized to cells. Fourth, blood and necrotic material attached to cell surfaces in samples may cause a high background staining [33]. Therefore, cytologic smears were only used for Papanicolaou stain, H&E stain and Wright’s stain preparations.
The accuracy of FNAB, to some degree, depends on the experience of the cytopathologists [34]. As time goes on, the diagnosis accuracy of FNAB will be improved. In addition, lack of unique markers in distinguishing the epithelial tumors is another limitation of our study. Once some potential unique markers are found, the accuracy of FNAB will be improved dramatically.
In conclusion, we found that the diagnostic value of a CB technique with immunohistochemistry to be superior to cytologic smears for the diagnosis of LGT and compares favorably to the pathologic diagnosis rendered by routine histopathologic techniques.
Acknowledgements
The authors thank Dr. Victor M. Elner, University of Michigan, for his advice and correction on this work.
Disclosure of conflict of interest
None.
References
- 1.Shields JA, Shields CL, Scartozzi R. Survey of 1264 patients with orbital tumors and simulating lesions: The 2002 Montgomery Lecture, part 1. Ophthalmology. 2004;111:997–1008. doi: 10.1016/j.ophtha.2003.01.002. [DOI] [PubMed] [Google Scholar]
- 2.Prabhakaran VC, Cannon PS, McNab A, Davis G, O’Donnell B, Dolman PJ, Ghabrial R, Selva D. Lesions mimicking lacrimal gland pleomorphic adenoma. Br J Ophthalmol. 2010;94:1509–1512. doi: 10.1136/bjo.2008.156307. [DOI] [PubMed] [Google Scholar]
- 3.Jung WS, Ahn KJ, Park MR, Kim JY, Choi JJ, Kim BS, Hahn ST. The radiological spectrum of orbital pathologies that involve the lacrimal gland and the lacrimal fossa. Korean J Radiol. 2007;8:336–342. doi: 10.3348/kjr.2007.8.4.336. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.von Holstein SL, Coupland SE, Briscoe D, Le Tourneau C, Heegaard S. Epithelial tumours of the lacrimal gland: a clinical, histopathological, surgical and oncological survey. Acta Ophthalmol. 2013;91:195–206. doi: 10.1111/j.1755-3768.2012.02402.x. [DOI] [PubMed] [Google Scholar]
- 5.Wright JE, Rose GE, Garner A. Primary malignant neoplasms of the lacrimal gland. Br J Ophthalmol. 1992;76:401–407. doi: 10.1136/bjo.76.7.401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Font RL, Smith SL, Bryan RG. Malignant epithelial tumors of the lacrimal gland: a clinicopathologic study of 21 cases. Arch Ophthalmol. 1998;116:613–616. doi: 10.1001/archopht.116.5.613. [DOI] [PubMed] [Google Scholar]
- 7.Tse DT, Benedetto P, Dubovy S, Schiffman JC, Feuer WJ. Clinical analysis of the effect of intraarterial cytoreductive chemotherapy in the treatment of lacrimal gland adenoid cystic carcinoma. Am J Ophthalmol. 2006;141:44–53. doi: 10.1016/j.ajo.2005.08.068. [DOI] [PubMed] [Google Scholar]
- 8.von Holstein SL, Therkildsen MH, Prause JU, Stenman G, Siersma VD, Heegaard S. Lacrimal gland lesions in Denmark between 1974 and 2007. Acta Ophthalmol. 2013;91:349–354. doi: 10.1111/j.1755-3768.2012.02403.x. [DOI] [PubMed] [Google Scholar]
- 9.Stewart WB, Krohel GB, Wright JE. Lacrimal gland and fossa lesions: an approach to diagnosis and management. Ophthalmology. 1979;86:886–895. doi: 10.1016/s0161-6420(79)35467-7. [DOI] [PubMed] [Google Scholar]
- 10.Gunduz K, Shields JA, Eagle RC Jr, Shields CL, De Potter P, Klombers L. Malignant rhabdoid tumor of the orbit. Arch Ophthalmol. 1998;116:243–246. doi: 10.1001/archopht.116.2.243. [DOI] [PubMed] [Google Scholar]
- 11.Shome D, Honavar SG, Gupta P, Vemuganti GK, Reddy PV. Metastasis to the eye and orbit from renal cell carcinoma--a report of three cases and review of literature. Surv Ophthalmol. 2007;52:213–223. doi: 10.1016/j.survophthal.2006.12.004. [DOI] [PubMed] [Google Scholar]
- 12.Auran J, Jakobiec FA, Krebs W. Benign mixed tumor of the palpebral lobe of the lacrimal gland. Clinical diagnosis and appropriate surgical management. Ophthalmology. 1988;95:90–99. doi: 10.1016/s0161-6420(88)33223-9. [DOI] [PubMed] [Google Scholar]
- 13.Wright JE, Stewart WB, Krohel GB. Clinical presentation and management of lacrimal gland tumours. Br J Ophthalmol. 1979;63:600–606. doi: 10.1136/bjo.63.9.600. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Currie ZI, Rose GE. Long-term risk of recurrence after intact excision of pleomorphic adenomas of the lacrimal gland. Arch Ophthalmol. 2007;125:1643–1646. doi: 10.1001/archopht.125.12.1643. [DOI] [PubMed] [Google Scholar]
- 15.Hanley KZ, Birdsong GG, Cohen C, Siddiqui MT. Immunohistochemical detection of estrogen receptor, progesterone receptor, and human epidermal growth factor receptor 2 expression in breast carcinomas: comparison on cell block, needle-core, and tissue block preparations. Cancer. 2009;117:279–288. doi: 10.1002/cncy.20034. [DOI] [PubMed] [Google Scholar]
- 16.Briffod M, Hacene K, Le Doussal V. Immunohistochemistry on cell blocks from fine-needle cytopunctures of primary breast carcinomas and lymph node metastases. Mod Pathol. 2000;13:841–850. doi: 10.1038/modpathol.3880149. [DOI] [PubMed] [Google Scholar]
- 17.Chandan VS, Faquin WC, Wilbur DC, Khurana KK. The role of immunolocalization of CD57 and GLUT-1 in cell blocks in fine-needle aspiration diagnosis of papillary thyroid carcinoma. Cancer. 2006;108:331–336. doi: 10.1002/cncr.22172. [DOI] [PubMed] [Google Scholar]
- 18.Bartolazzi A, Orlandi F, Saggiorato E, Volante M, Arecco F, Rossetto R, Palestini N, Ghigo E, Papotti M, Bussolati G, Martegani MP, Pantellini F, Carpi A, Giovagnoli MR, Monti S, Toscano V, Sciacchitano S, Pennelli GM, Mian C, Pelizzo MR, Rugge M, Troncone G, Palombini L, Chiappetta G, Botti G, Vecchione A, Bellocco R Italian Thyroid Cancer Study G. Galectin-3-expression analysis in the surgical selection of follicular thyroid nodules with indeterminate fine-needle aspiration cytology: a prospective multicentre study. Lancet Oncol. 2008;9:543–549. doi: 10.1016/S1470-2045(08)70132-3. [DOI] [PubMed] [Google Scholar]
- 19.Glasgow BJ, Layfield LJ. Fine-needle aspiration biopsy of orbital and periorbital masses. Diagn Cytopathol. 1991;7:132–141. doi: 10.1002/dc.2840070206. [DOI] [PubMed] [Google Scholar]
- 20.Tijl JW, Koornneef L. Fine needle aspiration biopsy in orbital tumours. Br J Ophthalmol. 1991;75:491–492. doi: 10.1136/bjo.75.8.491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sturgis CD, Silverman JF, Kennerdell JS, Raab SS. Fine-needle aspiration for the diagnosis of primary epithelial tumors of the lacrimal gland and ocular adnexa. Diagn Cytopathol. 2001;24:86–89. doi: 10.1002/1097-0339(200102)24:2<86::aid-dc1016>3.0.co;2-5. [DOI] [PubMed] [Google Scholar]
- 22.Kapadia SB, Dusenbery D, Dekker A. Fine needle aspiration of pleomorphic adenoma and adenoid cystic carcinoma of salivary gland origin. Acta Cytol. 1997;41:487–492. doi: 10.1159/000332543. [DOI] [PubMed] [Google Scholar]
- 23.Klijanienko J, Vielh P. Fine-needle sampling of salivary gland lesions. III. Cytologic and histologic correlation of 75 cases of adenoid cystic carcinoma: review and experience at the Institut Curie with emphasis on cytologic pitfalls. Diagn Cytopathol. 1997;17:36–41. doi: 10.1002/(sici)1097-0339(199707)17:1<36::aid-dc7>3.0.co;2-n. [DOI] [PubMed] [Google Scholar]
- 24.Taxin A, Tartter PI, Zappetti D. Breast cancer diagnosis by fine needle aspiration and excisional biopsy. Recurrence and survival. Acta Cytol. 1997;41:302–306. doi: 10.1159/000332516. [DOI] [PubMed] [Google Scholar]
- 25.Qizilbash AH, Sianos J, Young JE, Archibald SD. Fine needle aspiration biopsy cytology of major salivary glands. Acta Cytol. 1985;29:503–512. [PubMed] [Google Scholar]
- 26.McGurk M, Hussain K. Role of fine needle aspiration cytology in the management of the discrete parotid lump. Ann R Coll Surg Engl. 1997;79:198–202. [PMC free article] [PubMed] [Google Scholar]
- 27.Lai T, Prabhakaran VC, Malhotra R, Selva D. Pleomorphic adenoma of the lacrimal gland: is there a role for biopsy? Eye (Lond) 2009;23:2–6. doi: 10.1038/eye.2008.16. [DOI] [PubMed] [Google Scholar]
- 28.Tosaka Y. Immunohistochemical study of pleomorphic adenoma of lacrimal gland. Jpn J Ophthalmol. 1991;35:367–376. [PubMed] [Google Scholar]
- 29.Strianese D, Baldi G, Staibano S, Baldi A, De Rosa G, Tranfa F, Bonavolonta G. Expression of apoptosis-related markers in malignant epithelial tumours of the lacrimal gland and their relation to clinical outcome. Br J Ophthalmol. 2007;91:1239–1243. doi: 10.1136/bjo.2007.118661. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Saghravanian N, Mohtasham N, Jafarzadeh H. Comparison of immunohistochemical markers between adenoid cystic carcinoma and polymorphous low-grade adenocarcinoma. J Oral Sci. 2009;51:509–514. doi: 10.2334/josnusd.51.509. [DOI] [PubMed] [Google Scholar]
- 31.Zukerberg LR, Ferry JA, Southern JF, Harris NL. Lymphoid infiltrates of the stomach. Evaluation of histologic criteria for the diagnosis of low-grade gastric lymphoma on endoscopic biopsy specimens. Am J Surg Pathol. 1990;14:1087–1099. [PubMed] [Google Scholar]
- 32.Bryant RJ, Banks PM, O’Malley DP. Ki67 staining pattern as a diagnostic tool in the evaluation of lymphoproliferative disorders. Histopathology. 2006;48:505–515. doi: 10.1111/j.1365-2559.2006.02378.x. [DOI] [PubMed] [Google Scholar]
- 33.Ronald AD, Hoda RS. Immunochemistry and molecular biology in cytological diagnosis. In: Koss LG, Melamed MR, editors. Koss’s diagnostic cytology and its histopathologic bases. 5th edition. Philadelphia: Lippincott Williams & Wilkins; 2005. pp. 1635–1680. [Google Scholar]
- 34.Speight PM, Barrett AW. Salivary gland tumours. Oral Dis. 2002;8:229–240. doi: 10.1034/j.1601-0825.2002.02870.x. [DOI] [PubMed] [Google Scholar]