

Abstract
Objective: To evaluate the clinical significance of transrectal real-time elastography (TRTE) in diagnosis of prostate cancer (PCA). Methods: 195 patients with an elevated PSA level were enrolled in the study. A novel 5-grading score of prostate outer gland was applied by TRTE imaging. Receiver-operating characteristic curve (ROC) analyses were performed to assess the diagnostic performance of TRTE score. Results: TRTE scores in patients with PCA and benign condition were 3.20 ± 1.11 (range: 1-5) and 2.24 ± 1.01 (range: 1-4), respectively (P < 0.001). The best cutoff value of TRTE score was 3, and the sensitivity, specificity, accuracy in the diagnosis were 68.6% (35/51), 69.4% (100/144) and 69.2% (135/195), respectively. The accuracy of TRTE in volume ≤ 30 ml group was significantly higher than that in the volume ≥ 50 ml group and the 30-50 ml group (76.9% vs. 65.0% and 76.9% vs. 71.4%, both P < 0.001). Accuracy of TRTE score was higher for those with PSA ranged 4-10 ng/ml than those with PSA > 10 ng/ml (85.3% vs. 66.7%, P = 0.002). Conclusion: TRTE score, a novel semi-quantitative assessment of patients’ prostate stiffness, can be served as a useful screening method for patients suspicious of PCA, especially those only having an elevated PSA level.
Keywords: Prostate cancer, transrectal real-time elastography
Introduction
Prostate cancer (PCA) is one of the most common cancers in men in western countries and stands the second position in male malignant tumors worldwide [1]. With improvement in PSA screening and the prolonged life expectancy, incidence and prevalence of PCA has increased steadily in the last decade [2,3]. Nowadays, methods for diagnosis of PCA include prostate-specific antigen (PSA) serum level, digital rectal examination (DRE) and diagnostic imaging techniques such as ultrasound and MRI. However, 85% of PCA is multifocal and progresses along the capsule of prostate and it may not appear as a well-defined nodule like other malignant tumors [4,5], so it is difficult to detect the lesions accurately using the conventional imaging technology [6]. In this respect, it is necessary to find a new imaging modality for screening PCA.
Transrectal real-time elastography (TRTE) imaging technology assesses the differences in tissue strain produced by freehand compression, with the harder tissue presenting the smaller strain. TRTE can reflect the distribution of the strain by ultrasonic imaging in order to differentiate benign and malignant tissue [7,8]. As a novel biomechanics technique, TRTE makes up the deficiency of the conventional ultrasonic imaging mode, with better diagnostic value for PCA. However, it remains unclear whether TRTE can be used as routine clinical application [9].
Systematic biopsy guided by ultrasound is still the gold standard for diagnosis of PCA [3]. Elevated PSA level and/or abnormal DRE were widely accepted as biopsy indications [10,11]. However, the specificity of elevated PSA level is low, since benign conditions including benign prostatic hyperplasia, prostatitis and other non-cancerous lesions also can lead to an elevated PSA [12-16]. Therefore, elevated PSA level as a biopsy indication will lead to much unnecessary biopsies. In this case, we aimed to evaluate the diagnostic value of the new 5-grading score in the diagnosis of PCA with real-time elastography for patients with an elevated PSA, and to provide evidence for the decision-tree in selecting patients for biopsy.
Patients and methods
Patients
From August 2012 to October 2013, 352 consecutive patients with PSA ≥ 4 ng/ml underwent prostate biopsy in the university hospital. Diagnoses were confirmed by pathological examination after biopsy and the pathological diagnoses were made by one experienced pathologist. The flowchart for the patient selection was presented in Figure 1. The inclusion criteria for the patients were as follows: (1) Age ≤ 80 and no peripheral nodules visualized on grey-scale ultrasound; (2) No surgery performed on prostate tissue before; (3) Patients were willing to undergo TRTE. In total, 195 patients were enrolled in the present study and 3 patients were excluded because of unreliable imaging (TRTE images were not bilateral symmetrical or did not include prostate tissue completely). The patient age ranged from 48 to 80 yrs and the mean age was 66.8 ± 7.2 yrs. The PSA ranged from 4 ng/ml to 98.4 ng/ml (median, 9.9 ng/ml) and the volume of prostate ranged from 11 ml to 113 ml (median, 45 ml). The study was approved by the Ethical Committee of the university hospital and written informed consent was obtained from each patient.
Figure 1.
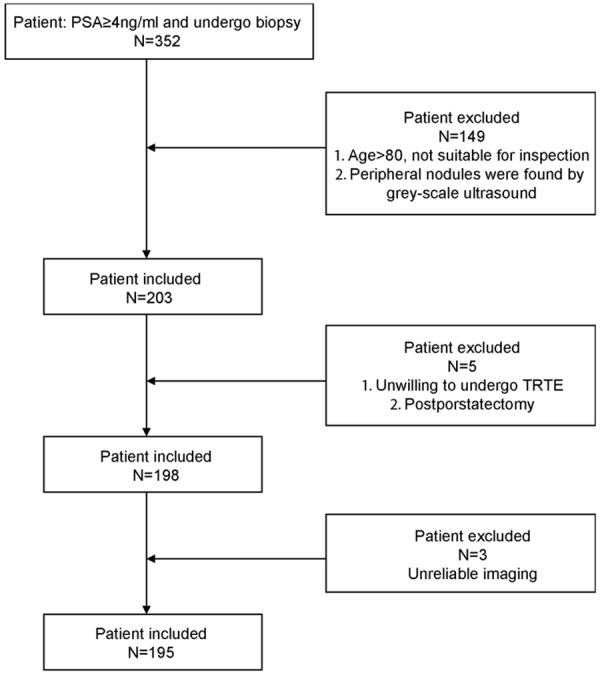
Flowchart of the selection of the patients for TRTE score.
Elasticity imaging
TRTE were performed with LOGIQ E9 machine (GE Healthcare, Milwaukee, Wl, USA). A transrectal endocavity probe (IC5-9-D) with a center frequency of 7 MHz (range, 5-9 MHz) was equipped for all the B-mode US and TRTE examinations. All the patients were examined by an experienced operator who had the experiences in prostate examination by transrectal ultrasound at least 5 years and experiences in TRTE examination at least 6 months.
All patients lied in left lateral position with bend knees hip flexion. Latex was set close to the probe besmeared a moderate amount of coupling agent and the probe was inserted to the rectum slowly. The prostate capsule, symmetry, internal echo and boundary were observed firstly by conventional ultrasound. Then the blood flow sign was observed with color Doppler and power Doppler ultrasound, the prostate volume was measured and recorded simultaneously. Then TRTE mode was started. Each section was checked from the apex to the bottom. TRTE images were obtained in the transverse plane at up to 10 frames per second with focus at the depth of 1.5 cm from the surface of probe. The region of interest of TRTE was set as approximately 1 cm to the edge of biggest transverse. The investigator manually induced slight compression and decompression of the prostate tissue using the probe. Under the guidance of quality bar in the process of compression and decompression, the pressure and direction of manual vibration were adjusted until stable, repeatable images (bilateral prostatic capsule was clear, smooth and symmetrical with the pressure indicator bar displayed as over 4) were obtained. The images were stored in the instrument system in the workstation for further analysis. Each patient was examined about 7 to 10 minutes.
Image analysis and TRTE score
All the images were interpreted by a senior doctor and a junior doctor and both of them didn’t know each other’s scores and pathological results. The repeated TRTE score for the same TRTE images were performed by the senior doctor. The first TRTE score of the senior doctor was recorded as final result. The two results of the senior doctor for TRTE score were used to assess intraobserver reproducibility. The first TRTE score of the senior doctor and the TRTE score of junior doctor were used to assess interobserver reproducibility.
The interpretation standard of TRTE was as following: score 1: there was no blue area or star-like blue in outer glands; score 2: the mosaic or a little symmetrical blue area in bilateral outer glands were seen and the blue area is less than 5 mm in diameter; score 3: a little symmetrical blue area in bilateral outer glands, the diameter of blue area ≥ 5 mm; score 4: asymmetric blue area in bilateral outer glands, the diameter of blue area ≥ 5 mm; score 5: asymmetric blue area in bilateral outer glands, the blue area of more than 50%, the blue area ≥ 50% of single outer gland area (Figure 2).
Figure 2.
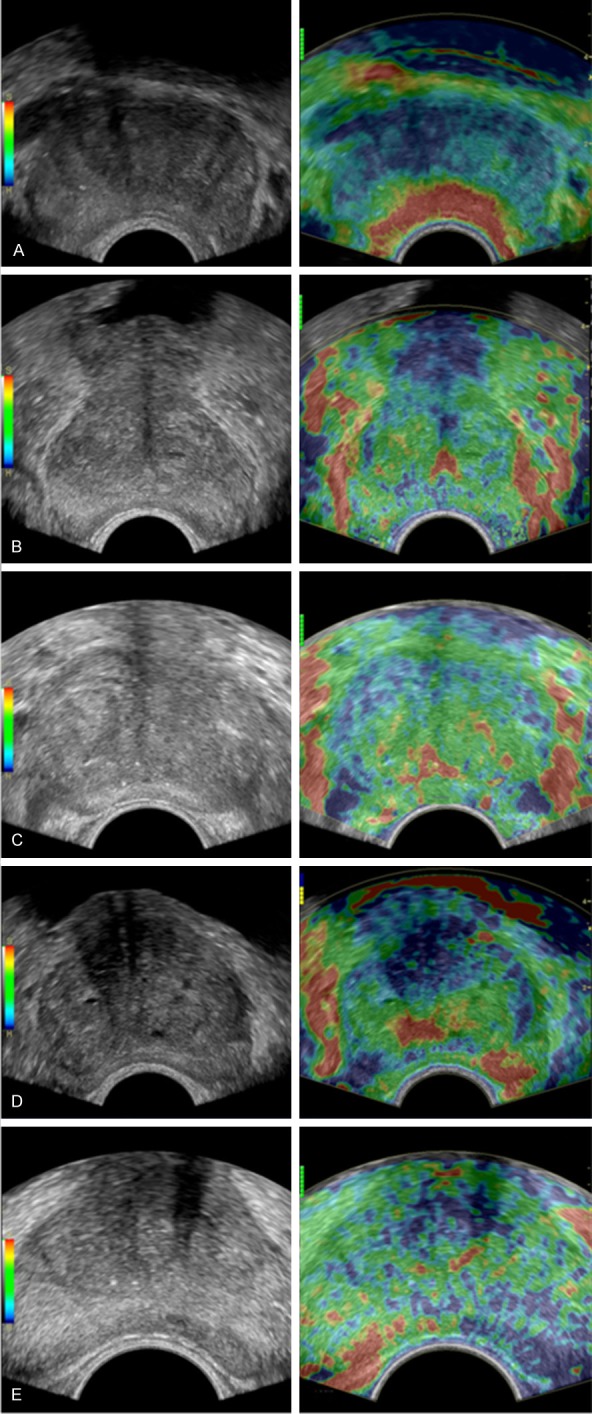
Transrectal real-time elastography (TRTE) imaging (left). Score 1: A: There was no blue area or star-like blue in outer glands; Score 2: B: The mosaic or a little symmetrical blue area in bilateral outer glands, the blue area is less than 5 mm in diameter; Score 3: C: A little symmetrical blue area in bilateral outer glands, the diameter of blue area ≥ 5 mm; Score 4: D: Asymmetric blue area in bilateral outer glands, the diameter of blue area ≥ 5 mm; Score 5: E: Asymmetric blue area in bilateral outer glands, the blue area of more than 50%, the blue area ≥ 50% of single outer gland area.
Prostate biopsy
All patients underwent transperineal ultrasound-guided prostate biopsy. For patients with the volume of prostate ≤ 30 ml, 8-core biopsy was performed (one core in apex, middle and bottom of bilateral outer glands and bilateral inner glands); For patients with the volume of prostate ranged from 30 ml to 50 ml, 10-core biopsy was performed (conventional 8-core and one core in apex bilateral outer glands); For patients with the volume of prostate ≥ 50 ml, 12-core biopsy was performed (conventional 8-core, one core in apex and middle of bilateral outer glands).
Statistical analysis
Differences in quantitative data were compared with independent t-test. The intra- and inter-observer reproducibility was assessed using the correlation coefficient analysis. Receiver-operating characteristic curve (ROC) analyses were performed to assess the diagnostic performance of TRTE score in differentiating benign from PCA and the best cutoff value was investigated. The chi-square test were used to assess the accuracy between the two groups within each PSA level (4-10 ng/ml and > 10 ng/ml). The One-way ANOVA and LSD-t were used to assess the accuracy between the three groups within each prostate volume category (≤ 30 ml, 30-50 mm, and ≥ 50 ml). The statistical analyses were carried out using SPSS17.0 software package (SPSS Inc, Chicago, IL). P < 0.05 was considered to be statistically significant.
Results
In total, 51 of 195 patients (26.2%) were diagnosed as PCA. Histologically and the Gleason score ranged from 4 to 9. The basic characteristics of the patients and final pathologic diagnoses were presented in Table 1.
Table 1.
Characteristics of the patients
| N (%) | Range | Mean ± SD | t | P | ||
|---|---|---|---|---|---|---|
| Age (y) | Benigna | 144 (73.8) | 48-79 | 66.13 ± 7.03 | 2.253 | 0.025 |
| PCA | 51 (26.2) | 50-80 | 68.76 ± 7.56 | |||
| Volume (ml) | Benign | 144 (73.8) | 11-113 | 47.99 ± 21.46 | -3.998 | 0.000 |
| PCA | 51(26.2) | 13-80 | 36.67 ± 15.68 | |||
| Serum PSA levels (ng/ml) | ||||||
| 4-10 | Benign | 87 (44.6) | 4-10 | 6.79 ± 1.75 | 0.263 | 0.793 |
| PCA | 15 (7.7) | 4.6-10 | 6.91 ± 1.72 | |||
| > 10 | Benign | 57 (29.2) | 10.19-74.9 | 21.16 ± 14.06 | 3.436 | 0.001 |
| PCA | 36 (18.5) | 11.1-98.4 | 36.72 ± 24.76 | |||
| Gleason score | ||||||
| 4 | 2 (3.9) | |||||
| 5 | 5 (9.8) | |||||
| 6 | 13 (25.5) | |||||
| 7 | 20 (39.2) | |||||
| 8 | 6 (11.8) | |||||
| 9 | 5 (9.8) | |||||
Benign indicates benign conditions, including benign prostatic hyperplasia and chronic prostatitis.
7.9% (3/38) patients with a score of 1 and 16.7% (13/78) patients with a score of 2 were PCA. 63.3% (19/30) patients with a score of 3 and 56.8% (25/44) patients with a score of 4 were benign. None of the 5 patients in this group with a score of 5 were benign. The TRTE scores of PCA and benign conditions were 3.20 ± 1.11 (range: 1-5) and 2.24 ± 1.01 (range: 1-4) respectively. The mean TRTE score of PCA was significantly higher than that of benign conditions (P < 0.001).
ROC curve analyses showed that the area under the curve (AUC for the TRTE was 0.729 (95% CI: 0.648, 0.810). The best cutoff value of TRTE score was 3. The sensitivity, specificity, accuracy in diagnosis of PCA were 68.6% (35/51), 69.4% (100/144) and 69.2% (135/195), respectively. When dividing the patients into three groups according to their prostate volume, for the volume ≤ 30 ml, AUC was 0.679 (95% CI: 0.512, 0.846); for the volume ranged 30-50 ml, 0.709 (95% CI: 0.590, 0.827); for the volume ≥ 50 ml, 0.849 (95% CI: 0.720, 0.979). The accuracy of TRTE in volume ≤ 30 ml group was significantly higher than that in the volume ≥ 50 ml group and the 30-50 ml group (76.9% vs. 65.0% and 76.9% vs.71.4%, both P < 0.001). There was no significantly difference between the volume ≥ 50 ml group and the 30-50 ml group in the accuracy of TRTE (P = 0.175). When dividing the patients into two groups by PSA level, for the 4 ng/ml ≤ PSA ≤ 10 ng/ml group, AUC was 0.825 (95% CI: 0.709, 0.942); for the PSA > 10 ng/ml, 0.681 (95% CI: 0.571, 0.791). The accuracy of TRTE score was higher for PSA ranged 4-10 ng/ml than PSA > 10 ng/ml (85.3% vs. 66.7%, P = 0.002). The corresponding sensitivity, specificity, and accuracy were presented in Table 2.
Table 2.
Diagnostic performance of TRTE score in the diagnosis of PCA
| Accuracy %b | Sensitivity % | Specificity % | AUC | 95% CI | ||
|---|---|---|---|---|---|---|
| Volume (ml) | ≤ 30 | 76.9 (40/52) | 62.5 (15/24) | 89.3 (25/28) | 0.679 | 0.512, 0.846 |
| 30-50 | 65.0 (52/80) | 73.1 (19/26) | 61.1 (33/54) | 0.709 | 0.590, 0.827 | |
| ≥ 50 | 71.4 (54/63) | 71.4 (5/7) | 71.4 (40/56) | 0.849 | 0.720, 0.979 | |
| PSA (ng/ml) | 4-10 | 85.3 (87/102) | 96.3 (26/27) | 81.3 (75/87) | 0.825 | 0.709, 0.942 |
| > 10 | 66.7 (62/93) | 69.4 (25/36) | 64.9 (37/57) | 0.681 | 0.571, 0.791 |
One-way ANOVA result in F = 15.354, P = 0.000; further analysis with LSD-t test revealed that the accuracy of volume ≤ 30 group was significantly higher than that of the volume ≥ 50 ml group and the 30-50 ml group (all P < 0.001. There was no significantly difference between the volume ≥ 50 ml group and the 30-50 ml group (P = 0.175).
The accuracy of TRTE score was more higher for PSA ranged 4-10 ng/ml than PSA > 10 ng/ml (85.3% vs. 66.7%, P = 0.002).
The distribution of TRTE score for PCA according to Gleason score was shown in Figure 3. The mean TRTR score was 3.40 ± 1.05 for Gleason < 7 and 3.06 ± 1.15 for Gleason ≥ 7. There were no significant difference between the mean scores for Gleason < 7 and those for Gleason ≥ 7 (P = 0.298).
Figure 3.
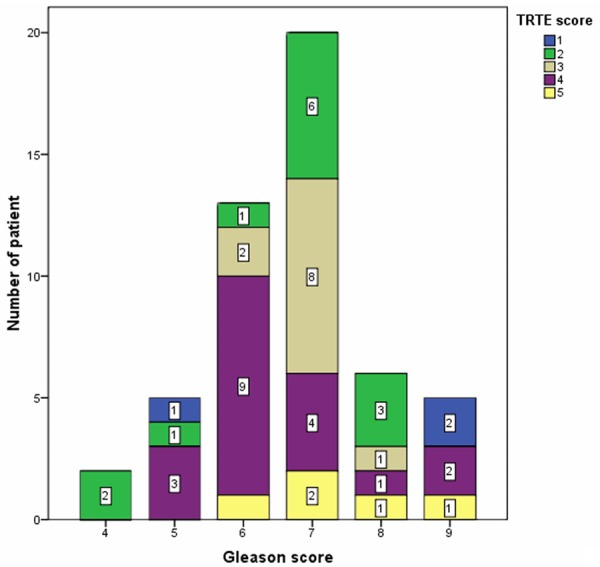
Distribution of TRTE score for PCA according to Gleason score.
The correlation coefficients were 0.948 (P = 0.000) for intraobserver measurement and 0.725 for interobserver measurement (P < 0.001).
Discussion
Ultrasound is the most common imaging method for direct visualization of the prostate due to the advantages of real-time imaging, free of radiation, and low cost. However, transrectal ultrasound is not highly sensitive or specific in the diagnosis of PCA [17]. Meanwhile, color Doppler and power Doppler imaging do not substantially improve the diagnostic accuracy [18]. Pathological result obtained by transrectal ultrasonography guided biopsy remains the mainstay in confirming PCA [3]. It was reported that about one million biopsies per year were performed in the United States [19]. However, it was not useful to increase the detection rates of PCA by modifying biopsy protocols that focus on obtaining increased biopsy sample number [20-24], which may be attributable to the limitation of placing biopsy needles into the desired region as per biopsy protocol [17]. The ideal imaging technology should be affordable and minimally invasive; however, if prostate biopsy is used as a routine procedure, it is likely to bring more complications and cost. In this respect, more effort is needed to improve the prostate imaging. Elastography has been used clinically to examine a variety of organs, including the breast, thyroid and prostate [21,25,26], since it was first introduced by Ophir et al [27]. TRTE is currently mainly used for differentiating benign from malignant prostatic lesions [28] and guiding prostate biopsy [6,20,29,30] as a new ultrasonic technique and the diagnostic performance is ideal with potential in improving the diagnosis of PCA.
For the patients with abnormal DRE or abnormal nodules on conventional ultrasound, the cases can be diagnosed by transrectal ultrasonography guided biopsy targeting to the suspicious area, which is the most direct and efficient way. However, for the patients with elevated PSA levels only, it remains unclear whether all biopsies are necessary. This question has great clinical implication since use of TRTE could reduce the rate and the cost of biopsies for those only having an elevated PSA level.
Cell density is greater in neoplastic tissue than in normal tissue, which causes a change in tissue elasticity [31]. TRTE allows an assessment of tissue elasticity with color coding, in which the scale ranged from red (soft) to blue (hard). Kamoi et al [28] initially reported that the grading system of TRTE was valuable in the diagnosis of PCA, as was successfully applied to breast lesions and thyroid nodules [28,32]. In the clinical application of TRTE-guided biopsy, the hard areas with a diameter ≥ 5 mm in elasticity imaging were considered as malignant [33,34]. Many prostate cancers detected at biopsy were not visible at TRUS [28] and many cases were isoechoic. Therefore, the TRTE score based on the symmetry and elastic distribution of prostate outer gland was proposed for the patients only having an elevated PSA level.
In this study, the mean TRTE score of PCA was significantly higher than that of benign conditions. The sensitivity, specificity, and accuracy in diagnosis of PCA were 68.6%, 69.4% and 69.2%, respectively. On the other hand, the sensitivity, specificity and accuracy of the grading system of TRTE focus on prostate lesions were 68%, 81% and 76% in the study of Kamoi K [28]. It showed a relatively balanced sensitivity, specificity and accuracy. Until present, there have been no studies on the relationship between the TRTE score and the prostate or prostate lesion size. In this study, the diagnostic value of TRTE score was associated with the prostate volume with relatively high value for those volume ≤ 30 ml. The diagnostic value of TRTE score was also associated with the PSA level, with relatively high value for those with 4 ng/ml ≤ PSA ≤ 10 ng/ml. It is controversial to perform biopsy for patients only having PSA ranged 4-10 ng/ml, thus this finding can help clinicians with the pressing need. Therefore, it may be useful to introduce TRTE score into routine clinical practice.
At present, Gleason score is one of the most used histological grading systems for prostate cancer and the prognosis of prostate cancer is closely related to the Gleason score. The progression and fatality rate of Gleason 6 were much lower than Gleason ≥ 7 [35,36]. Some studies [3,20,28,30,37] reported that the TRTE detection rate of prostate cancer with a higher Gleason score was higher than that of lower Gleason score, whereas Tsutsumi et al [33] found that TRTE detection rate was higher for low-staged tumors. In the present study, there were no significant differences between the mean scores for Gleason < 7 and those for Gleason ≥ 7.
There were some limitations in the present study. Firstly, the major limitation of TRTE is that the procedure is manually compressing the prostate and it is operator-dependant, which may affect the repeatability [38]. Pelzer et al [39] reported that transition zone cancers were very rare in a PSA screening population, and additionally, TRTE can produce hard artifacts (blue) with increasing depth of penetration [33]. Therefore, the inner gland findings were not included in the TRTE score. Another limitation was that biopsy specimen cannot diagnose all the PCAs because of sampling error. Lastly, volunteers with normal PSA are not included in the study.
In conclusion, TRTE score, a novel semi-quantitative assessment of patients’ prostate, can be served as a useful screening method for those patients suspicious of PCA, especially those only having an elevated PSA level.
Acknowledgements
This work was supported by Research Project of Science and Technology Committee of Shanghai Municipality (124119a3201).
Disclosure of conflict of interest
None.
References
- 1.Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin. 2011;61:69–90. doi: 10.3322/caac.20107. [DOI] [PubMed] [Google Scholar]
- 2.Hsing AW, Tsao L, Devesa SS. International trends and patterns of prostate cancer incidence and mortality. Int J Cancer. 2000;85:60–67. doi: 10.1002/(sici)1097-0215(20000101)85:1<60::aid-ijc11>3.0.co;2-b. [DOI] [PubMed] [Google Scholar]
- 3.Sparchez Z. Real-time ultrasound prostate elastography. An increasing role in prostate cancer detection? Med Ultrason. 2011;13:3–4. [PubMed] [Google Scholar]
- 4.Byar DP, Mostofi FK. Carcinoma of the prostate: prognostic evaluation of certain pathologic features in 208 radical prostatectomies. Examined by the step-section technique. Cancer. 1972;30:5–13. doi: 10.1002/1097-0142(197207)30:1<5::aid-cncr2820300103>3.0.co;2-s. [DOI] [PubMed] [Google Scholar]
- 5.McNeal JE, Redwine EA, Freiha FS, Stamey TA. Zonal distribution of prostatic adenocarcinoma. Correlation with histologic pattern and direction of spread. Am J Surg Pathol. 1988;12:897–906. doi: 10.1097/00000478-198812000-00001. [DOI] [PubMed] [Google Scholar]
- 6.Kapoor A, Kapoor A, Mahajan G, Sidhu BS. Real-time elastography in the detection of prostate cancer in patients with raised PSA level. Ultrasound Med Biol. 2011;37:1374–1381. doi: 10.1016/j.ultrasmedbio.2011.05.014. [DOI] [PubMed] [Google Scholar]
- 7.Dinter DJ, Weidner AM, Wenz F, Pelzer AE, Michel MS, Schoenberg SO. Imaging diagnostics of the prostate. Urologe A. 2010;49:963–975. doi: 10.1007/s00120-010-2338-0. [DOI] [PubMed] [Google Scholar]
- 8.Rago T, Santini F, Scutari M, Pinchera A, Vitti P. Elastography: new developments in ultrasound for predicting malignancy in thyroid nodules. J Clin Endocrinol Metab. 2007;92:2917–2922. doi: 10.1210/jc.2007-0641. [DOI] [PubMed] [Google Scholar]
- 9.Aboumarzouk OM, Ogston S, Huang Z, Evans A, Melzer A, Stolzenberg JU, Nabi G. Diagnostic accuracy of transrectal elastosonography (TRES) imaging for the diagnosis of prostate cancer: a systematic review and meta-analysis. BJU Int. 2012;110:1414–1423. doi: 10.1111/j.1464-410X.2012.11106.x. discussion 1423. [DOI] [PubMed] [Google Scholar]
- 10.Tsivian M, Kimura M, Sun L, Mouraviev V, Mayes JM, Polascik TJ. Predicting unilateral prostate cancer on routine diagnostic biopsy: sextant vs extended. BJU Int. 2010;105:1089–1092. doi: 10.1111/j.1464-410X.2009.08904.x. [DOI] [PubMed] [Google Scholar]
- 11.Pepe P, Aragona F. Prostate biopsy: results and advantages of the transperineal approach--twenty-year experience of a single center. World J Urol. 2014;32:373–377. doi: 10.1007/s00345-013-1108-1. [DOI] [PubMed] [Google Scholar]
- 12.Barentsz JO, Richenberg J, Clements R, Choyke P, Verma S, Villeirs G, Rouviere O, Logager V, Futterer JJ. ESUR prostate MR guidelines 2012. Eur Radiol. 2012;22:746–757. doi: 10.1007/s00330-011-2377-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Aigner F, Pallwein L, Schocke M, Lebovici A, Junker D, Schafer G, Mikuz G, Pedross F, Horninger W, Jaschke W, Halpern EJ, Frauscher F. Comparison of real-time sonoelastography with T2-weighted endorectal magnetic resonance imaging for prostate cancer detection. J Ultrasound Med. 2011;30:643–649. doi: 10.7863/jum.2011.30.5.643. [DOI] [PubMed] [Google Scholar]
- 14.Borley N, Feneley MR. Prostate cancer: diagnosis and staging. Asian J Androl. 2009;11:74–80. doi: 10.1038/aja.2008.19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Catalona WJ, Richie JP, Ahmann FR, Hudson MA, Scardino PT, Flanigan RC, deKernion JB, Ratliff TL, Kavoussi LR, Dalkin BL, et al. Comparison of digital rectal examination and serum prostate specific antigen in the early detection of prostate cancer: results of a multicenter clinical trial of 6,630 men. J Urol. 1994;151:1283–1290. doi: 10.1016/s0022-5347(17)35233-3. [DOI] [PubMed] [Google Scholar]
- 16.Gomez Veiga F, Ponce Reixa J, Barbagelata Lopez A, Fernandez Rosado E, Gonzalez Martin M. Current role of PSA and other markers in the diagnosis of prostate cancer. Arch Esp Urol. 2006;59:1069–1082. doi: 10.4321/s0004-06142006001000014. [DOI] [PubMed] [Google Scholar]
- 17.Heijmink SW, van Moerkerk H, Kiemeney LA, Witjes JA, Frauscher F, Barentsz JO. A comparison of the diagnostic performance of systematic versus ultrasound-guided biopsies of prostate cancer. Eur Radiol. 2006;16:927–938. doi: 10.1007/s00330-005-0035-y. [DOI] [PubMed] [Google Scholar]
- 18.Halpern EJ, Frauscher F, Strup SE, Nazarian LN, O’Kane P, Gomella LG. Prostate: high-frequency Doppler US imaging for cancer detection. Radiology. 2002;225:71–77. doi: 10.1148/radiol.2251011938. [DOI] [PubMed] [Google Scholar]
- 19.Loeb S, Carter HB, Berndt SI, Ricker W, Schaeffer EM. Complications after prostate biopsy: data from SEER-Medicare. J Urol. 2011;186:1830–1834. doi: 10.1016/j.juro.2011.06.057. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Aigner F, Pallwein L, Junker D, Schafer G, Mikuz G, Pedross F, Mitterberger MJ, Jaschke W, Halpern EJ, Frauscher F. Value of real-time elastography targeted biopsy for prostate cancer detection in men with prostate specific antigen 1.25 ng/ml or greater and 4.00 ng/ml or less. J Urol. 2010;184:913–917. doi: 10.1016/j.juro.2010.05.026. [DOI] [PubMed] [Google Scholar]
- 21.Cochlin DL, Ganatra RH, Griffiths DF. Elastography in the detection of prostatic cancer. Clin Radiol. 2002;57:1014–1020. doi: 10.1053/crad.2002.0989. [DOI] [PubMed] [Google Scholar]
- 22.Nelson ED, Slotoroff CB, Gomella LG, Halpern EJ. Targeted biopsy of the prostate: the impact of color Doppler imaging and elastography on prostate cancer detection and Gleason score. Urology. 2007;70:1136–1140. doi: 10.1016/j.urology.2007.07.067. [DOI] [PubMed] [Google Scholar]
- 23.Lane BR, Zippe CD, Abouassaly R, Schoenfield L, Magi-Galluzzi C, Jones JS. Saturation technique does not decrease cancer detection during followup after initial prostate biopsy. J Urol. 2008;179:1746–1750. doi: 10.1016/j.juro.2008.01.049. discussion 1750. [DOI] [PubMed] [Google Scholar]
- 24.Jones JS, Patel A, Schoenfield L, Rabets JC, Zippe CD, Magi-Galluzzi C. Saturation technique does not improve cancer detection as an initial prostate biopsy strategy. J Urol. 2006;175:485–488. doi: 10.1016/S0022-5347(05)00211-9. [DOI] [PubMed] [Google Scholar]
- 25.Garra BS, Cespedes EI, Ophir J, Spratt SR, Zuurbier RA, Magnant CM, Pennanen MF. Elastography of breast lesions: initial clinical results. Radiology. 1997;202:79–86. doi: 10.1148/radiology.202.1.8988195. [DOI] [PubMed] [Google Scholar]
- 26.Lyshchik A, Higashi T, Asato R, Tanaka S, Ito J, Mai JJ, Pellot-Barakat C, Insana MF, Brill AB, Saga T, Hiraoka M, Togashi K. Thyroid gland tumor diagnosis at US elastography. Radiology. 2005;237:202–211. doi: 10.1148/radiol.2363041248. [DOI] [PubMed] [Google Scholar]
- 27.Ophir J, Cespedes I, Ponnekanti H, Yazdi Y, Li X. Elastography: a quantitative method for imaging the elasticity of biological tissues. Ultrason Imaging. 1991;13:111–134. doi: 10.1177/016173469101300201. [DOI] [PubMed] [Google Scholar]
- 28.Kamoi K, Okihara K, Ochiai A, Ukimura O, Mizutani Y, Kawauchi A, Miki T. The utility of transrectal real-time elastography in the diagnosis of prostate cancer. Ultrasound Med Biol. 2008;34:1025–1032. doi: 10.1016/j.ultrasmedbio.2007.12.002. [DOI] [PubMed] [Google Scholar]
- 29.Ferrari FS, Scorzelli A, Megliola A, Drudi FM, Trovarelli S, Ponchietti R. Real-time elastography in the diagnosis of prostate tumor. J Ultrasound. 2009;12:22–31. doi: 10.1016/j.jus.2009.01.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Tsutsumi M, Miyagawa T, Matsumura T, Endo T, Kandori S, Shimokama T, Ishikawa S. Real-time balloon inflation elastography for prostate cancer detection and initial evaluation of clinicopathologic analysis. AJR Am J Roentgenol. 2010;194:W471–476. doi: 10.2214/AJR.09.3301. [DOI] [PubMed] [Google Scholar]
- 31.Krouskop TA, Wheeler TM, Kallel F, Garra BS, Hall T. Elastic moduli of breast and prostate tissues under compression. Ultrason Imaging. 1998;20:260–274. doi: 10.1177/016173469802000403. [DOI] [PubMed] [Google Scholar]
- 32.Itoh A, Ueno E, Tohno E, Kamma H, Takahashi H, Shiina T, Yamakawa M, Matsumura T. Breast disease: clinical application of US elastography for diagnosis. Radiology. 2006;239:341–350. doi: 10.1148/radiol.2391041676. [DOI] [PubMed] [Google Scholar]
- 33.Pallwein L, Mitterberger M, Struve P, Pinggera G, Horninger W, Bartsch G, Aigner F, Lorenz A, Pedross F, Frauscher F. Real-time elastography for detecting prostate cancer: preliminary experience. BJU Int. 2007;100:42–46. doi: 10.1111/j.1464-410X.2007.06851.x. [DOI] [PubMed] [Google Scholar]
- 34.Konig K, Scheipers U, Pesavento A, Lorenz A, Ermert H, Senge T. Initial experiences with real-time elastography guided biopsies of the prostate. J Urol. 2005;174:115–117. doi: 10.1097/01.ju.0000162043.72294.4a. [DOI] [PubMed] [Google Scholar]
- 35.Mitterberger M, Pinggera GM, Horninger W, Bartsch G, Strasser H, Schafer G, Brunner A, Halpern EJ, Gradl J, Pallwein L, Frauscher F. Comparison of contrast enhanced color Doppler targeted biopsy to conventional systematic biopsy: impact on Gleason score. J Urol. 2007;178:464–468. doi: 10.1016/j.juro.2007.03.107. discussion 468. [DOI] [PubMed] [Google Scholar]
- 36.Stark JR, Perner S, Stampfer MJ, Sinnott JA, Finn S, Eisenstein AS, Ma J, Fiorentino M, Kurth T, Loda M, Giovannucci EL, Rubin MA, Mucci LA. Gleason score and lethal prostate cancer: does 3 + 4 = 4 + 3? J Clin Oncol. 2009;27:3459–3464. doi: 10.1200/JCO.2008.20.4669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Pallwein L, Aigner F, Faschingbauer R, Pallwein E, Pinggera G, Bartsch G, Schaefer G, Struve P, Frauscher F. Prostate cancer diagnosis: value of real-time elastography. Abdom Imaging. 2008;33:729–735. doi: 10.1007/s00261-007-9345-7. [DOI] [PubMed] [Google Scholar]
- 38.Miyagawa T, Tsutsumi M, Matsumura T, Kawazoe N, Ishikawa S, Shimokama T, Miyanaga N, Akaza H. Real-time elastography for the diagnosis of prostate cancer: evaluation of elastographic moving images. Jpn J Clin Oncol. 2009;39:394–398. doi: 10.1093/jjco/hyp026. [DOI] [PubMed] [Google Scholar]
- 39.Pelzer AE, Bektic J, Berger AP, Halpern EJ, Koppelstatter F, Klauser A, Rehder P, Horninger W, Bartsch G, Frauscher F. Are transition zone biopsies still necessary to improve prostate cancer detection? Results from the tyrol screening project. Eur Urol. 2005;48:916–921. doi: 10.1016/j.eururo.2005.07.012. discussion 921. [DOI] [PubMed] [Google Scholar]