

Abstract
Influenza vaccination is important for cancer survivors, a population with impaired immunity. This study was designed to assess influenza vaccination patterns among Korean cancer survivors. In this cross-sectional analysis, data were obtained from standardized questionnaires from 943 cancer survivors and 41,233 non-cancer survivors who participated in the Fourth and Fifth Korea National Health and Nutrition Examination Surveys (2007-2011). We identified the adjusted influenza vaccination rates and assessed factors associated with influenza vaccination using multivariate logistic regression. Cancer survivors tended to have a higher adjusted influenza vaccination rate than the general population. The rates for influenza vaccination in specific cancer types such as stomach, hepatic, colon, and lung cancers were significantly higher than non-cancer survivors. Among all cancer survivors, those with chronic diseases, elderly subjects, and rural dwellers were more likely to receive influenza vaccination; those with cervical cancer were less likely to receive influenza vaccination. Cancer survivors were more likely to receive influenza vaccinations than non-cancer survivors, but this was not true for particular groups, especially younger cancer survivors. Cancer survivors represent a sharply growing population; therefore, immunization against influenza among cancer survivors should be concerned as their significant preventative healthcare services.
Graphical Abstract
Keywords: Influenza Vaccines, Cancer Survivors, Korean
INTRODUCTION
Five-year relative cancer survival rates have been improving worldwide (1, 2). In Korea, the prevalence of cancer was 1,925.9 per 100,000 people in 2010; in other words, approximately 1 in 52 persons is a cancer patient (3). As the number of cancer survivors has increased, most cancer survivors require routine preventive healthcare services to maintain health and, furthermore, to improve their quality of life (4).
Influenza is an important cause of acute respiratory diseases (5). Cancer survivors are considered a high-risk group for influenza and post-influenza complications (6, 7). The higher risk for influenza in cancer survivors can be due to specific conditions such as neutropenia according to chemotherapy, impaired immunity associated with disease or treatement of disease, concomitant use of corticosteroids (8). Additionally, the rates of morbidity and mortality are high among cancer survivors compared to those among the general population (9, 10, 11). Current Centers for Disease Control and Prevention guidelines recommend annual influenza vaccinations for all immunocompromised individuals including cancer patients (12). However, despite recommendations for influenza vaccination, cancer survivors were less likely than controls to be vaccinated against influenza in some previous studies (13, 14). In particular, non-elderly adults with cancer had lower rates of influenza vaccination than their elderly counterparts in previous surveillance studies (15). It is important to clarify the rate of influenza vaccination among cancer survivors and identify the sociodemographic circumstances and behavioral factors that affect influenza vaccination rates, because these findings will help identify subgroups to be targeted by preventative interventions of cancer survivors (16).
Although some studies have examined influenza vaccination rates among Korean cancer survivors, population-level data were rarely used. Previous study of influenza vaccination in Korean cancer survivors examined levels of utilization H1N1 vaccination practices and factors related to the vaccination. The present results indicated low levels of utilization and significant predictors of vaccination such as age, educational level, time since cancer diagnosis, and comorbidities (17). This study compared influenza vaccination rates between Korean cancer survivors and non-cancer survivors using data from the Fourth and Fifth Korean National Health and Nutrition Examination Survey (2007-2009, KNHANES IV and 2010-2011, KNHANES V) and investigated the factors associated with vaccination uptake.
MATERIALS AND METHODS
Study population
We used the data of the KNHANES IV (2007-2009) and KNHANES V (2010-2011); these are nationwide surveys that represent the general Korean population and include comprehensive information on health status, health behavior, and sociodemographics. A stratified multistage probability sampling design was used. Face-to-face interviews were conducted at participants' homes by trained interviewers to gather health information. Each participant gave informed consent prior to inclusion in the studies.
The initial sample for the present study comprised 42,176 candidates who completed both the health interview and health examination surveys. Of these, 943 cancer survivors were selected as the study population, and 41,233 non-cancer survivors were selected as the controls. Cancer survivors in this study were defined as patients from the time of diagnosis through the remaining years of life according to the definition of National Coalition for Cancer Survivorship (NCCS).
Associated factors and definition of influenza vaccination
From the surveys, we collected information about various factors potentially associated with the influenza vaccination. The risk factors were divided into three groups: sociodemographic, behavioral, and clinical factors. The sociodemographic factors were current age (<65 yr or ≥65 yr), sex, education level (less than high school education, or high school education or more), marital status, household monthly income (<3,000,000 KRW [USD 2,682], or ≥3,000,000 KRW), area of residence (urban or rural), and health insurance types (medical assistance or none, government health insurance without private health insurance, government health insurance with private health insurance).
The behavioral risk factors included smoking status (nonsmoker or past smoker, current smoker), alcohol consumption (nondrinker or non-risky drinker, risky drinker), physical activity (inactive, inadequately active, active), and self-perceived health status. Risky drinking was defined as alcohol consumption exceeding 3 standard drinks per day (18). Physical activity was classified as follows: inactive group (no physical activity), active group (moderate physical activity for at least 30 min per day on 5 days per week or vigorous physical activity for at least 20 min per day 3 days per week) and inadequately active group (exercised regularly but at levels that were less than sufficient) (19). Self-perceived health status was classified into two levels according to responses to the question "How do you assess your own health status?" One level included the responses: "very good," "good", and "fair" and the other level included the responses "poor", and "very poor"
The clinical factors included, comorbidities, all cancer types (gastric, hepatic, colon cancer, breast, cervical, lung, thyroid and other cancers), and time since cancer diagnosis (≤5 yr, 5-10 yr, and >10 yr). The comorbidities were hypertension, diabetes, chronic renal disease, coronary artery disease, and lung diseases such as asthma, tuberculosis, and chronic obstructive pulmonary disease. Vaccination against influenza was assessed using a self-reported answer to the following question: "Did you receive seasonal influenza (flu) vaccination during the last year?" Cancer survivors were identified using to the following question : "Have you had any cancers until now?"
Statistical analysis
We used a weighted population sample to reflect the sampling method and response rate. We calculated the estimated proportions and standard errors for baseline characteristics related to influenza vaccination. The statistical significance of differences between groups according to cancer status was assessed using logistic regression. We calculated the adjusted rate of influenza vaccination in non-cancer survivors versus cancer survivors, in younger individuals (<65 yr old), and in elderly individuals (≥65 yr old). We also examined the adjusted rate of influenza vaccination in cancer survivors according to cancer types comparing to non-cancer survivors. In addition, we calculated adjusted odds ratios (aORs) using multivariate logistic regression for all cancer controls, in the younger population (<65 yr old), and in the elderly population (≥65 yr old). We spilt into <65 yr and ≥65 yr of age variables, because the elderly cancer patients aged 65 yr or more are very high risk groups for influenza and related deaths among well-defined risk groups (20, 21). The level of significance was set at P<0.05. All estimates in the analysis were properly weighted to represent the general Korean population using a complex, multistage, probability sampling design. All statistical analyses were performed using STATA 10.0 (StataCorp., College Station, TX, USA). Because the survey data that we analyzed are publicly available, this study did not require the ethical approval of our Institutional Review Board.
RESULTS
General patient characteristics
Table 1 shows the baseline characteristics of the study population by cancer status. There were significant differences between the non-cancer controls and cancer survivors for all characteristics except physical activity and health insurance types. The most common cancer type among all patients was gastric cancer (16.7%). The most prevalent cancer types in men were gastric cancer (28.5%), colon cancer (17.4%), and liver cancer (7.7%), whereas those in women were cervical cancer (21.9%), breast cancer (19.7%), and thyroid cancer (11.4%). This distribution is a little different from the data of the Korea Central Cancer Registry. According to national statistics, the most prevalent cancer among all individuals in Korea is thyroid cancer. The most common cancers among male patients are gastric and colon cancers, whereas the most prevalent cancers among female patients are thyroid and breast cancers (3). Moreover, 48.4% of cancer survivors were diagnosed as having the disease less than 5 yr ago. In total, 64.0% of the cancer survivors were less than 65 yr old and 64.6% were female.
Table 1.
Characteristics of non-cancer controls (n=41,233) versus cancer survivors (n=943)
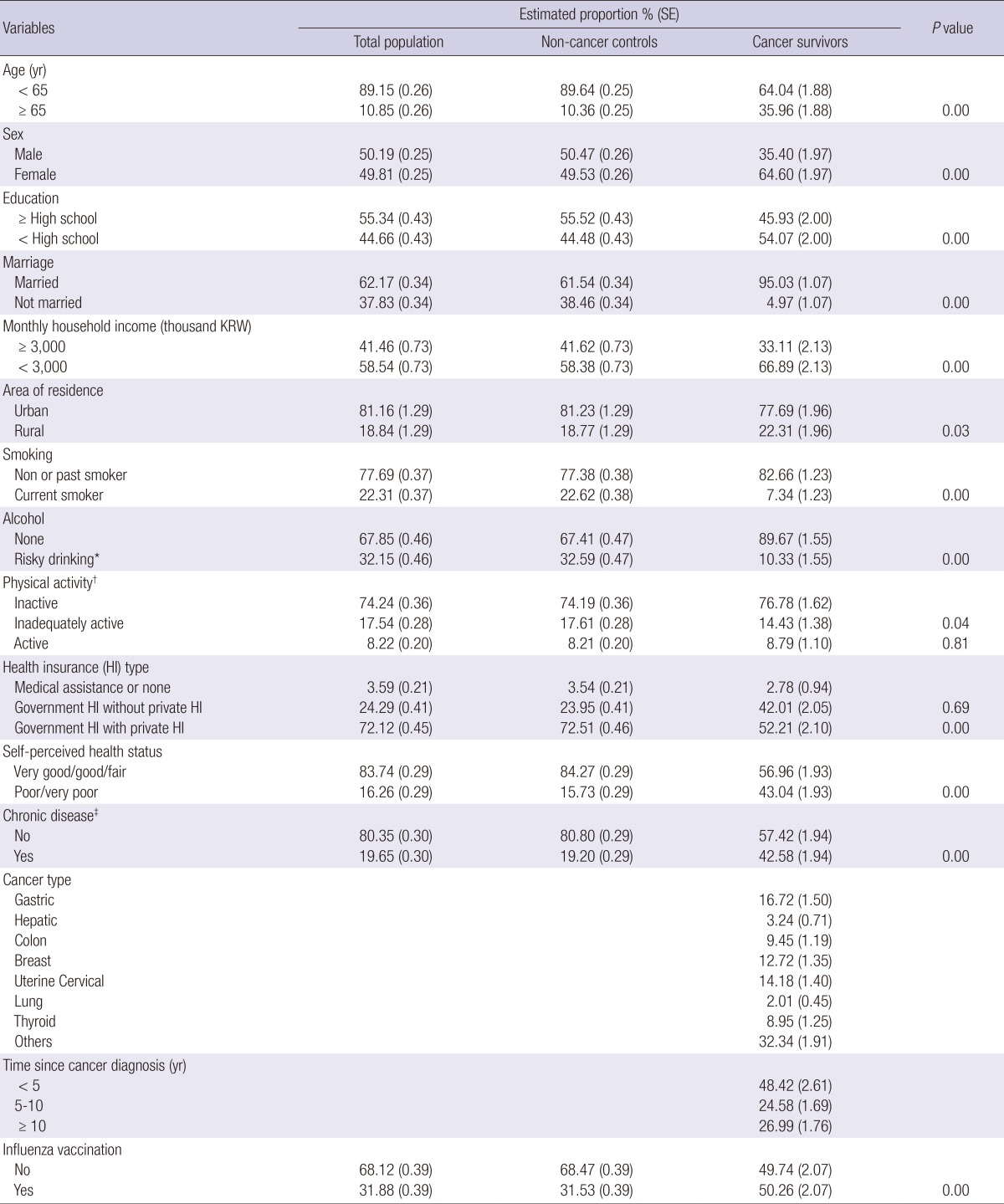
*Risk drinking is defined as consuming more than 3 standard drinks per day on occasion; †Physical activity was classified as inactive'group (no physical activity), active group (moderate physical activity for at least 30 min per day on 5 days per week or vigorous physical activity for at least 20 min per day on 3 days per and inadequately active group; ‡Chronic diseases were hypertension, diabetes, chronic renal disease, coronary artery disease, and lung disease such as asthma, tuberculosis, chronic obstructive pulmonary disease. KRW, Korean Won.
Adjusted influenza vaccination rates in non-cancer survivors versus cancer survivors, in younger individuals, and in elderly individuals
After adjustment for sociodemographic factors (age, sex, educational level, marriage status, monthly income, and residential area), the influenza vaccination rates for non-cancer survivors and cancer survivors were 35.5% and 42.5%, respectively (P<0.05); those for younger non-cancer survivors and cancer survivors were 27.8% and 36.0%, respectively, (P<0.05); and those for elderly non-cancer survivors and cancer survivors were 76.1% and 76.7%, respectively (P<0.05) (Fig. 1).
Fig. 1.

Adjusted rate for influenza vaccination in non-cancer survivors versus cancer survivors, adjusted for patient characteristics (age, sex, educational level, marriage status, monthly income, and residential area). *P value <0.05.
Adjusted rate of influenza vaccination in cancer survivors according to cancer types comparing to non-cancer survivors
After adjustment for sociodemographic factors (age, sex, educational level, marriage status, monthly income, and residential area), the rate for influenza vaccination was 35.5% in stomach cancer patients, 37.4% in hepatic cancer patients, 39.3% in colon cancer patients, 41.3% in breast cancer patients, 43.3% in cervical cancer patients, 45.3% in lung cancer patients, and 47.4% in thyroid cancer patient, respectively. The rates for influenza vaccination in stomach, hepatic, colon, and lung cancer patients were significantly higher than non-cancer survivors' (Fig. 2).
Fig. 2.

Adjusted rate of influenza vaccination in cancer survivors according to cancer types comparing to non-cancer survivors, adjusted for patient characteristics (age, sex, educational level, marriage status, monthly income, and residential area). *P value <0.05.
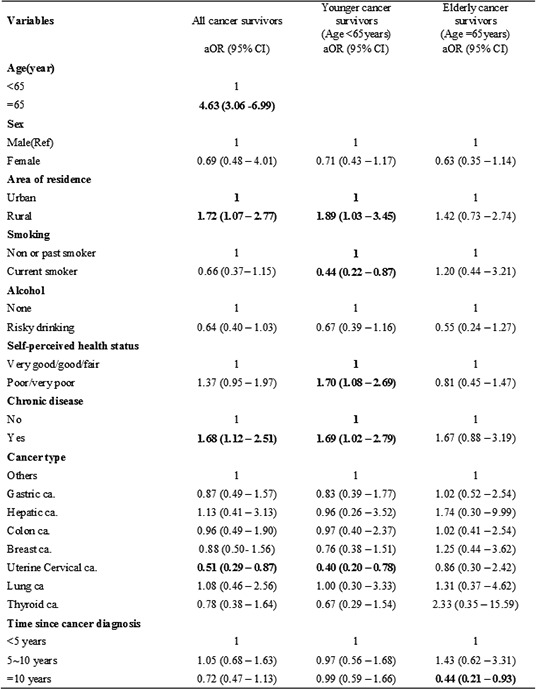
Factors associated with influenza vaccination rates among cancer survivors
In multivariate logistic regression analysis, adjusted for all sociodemographic, behavioral, and clinical factors, the rate of influenza vaccination among all cancer survivors was related to age, area of residence, the presence of a chronic disease, and cancer type. Among cancer survivors, those with chronic diseases (aOR, 1.68; 95% confidence interval [CI], 1.12-2.51), elderly subjects (aOR, 4.63; 95% CI, 3.06-6.99), and rural dwellers (aOR, 1.72; 95% CI, 1.07-2.77) were more likely to receive influenza vaccination, whereas patients with cervical cancer were less likely to receive influenza vaccination (aOR, 0.51; 95% CI, 0.29-0.87). Among younger cancer survivors, current smokers (aOR, 0.44; 95% CI, 0.22-0.87) were less likely to be vaccinated, whereas those with a poor self-perceived health status (aOR, 1.70; 95% CI, 1.08-2.69), rural dwellers (aOR, 1.89; 95% CI, 1.03-3.45), and those with chronic diseases (aOR, 1.69; 95% CI, 1.02-2.79) were more likely to be vaccinated. Among elderly cancer survivors, a period of more than 10 yr since cancer diagnosis was associated with a lower rate of influenza vaccination (aOR, 0.44; 95% CI, 0.21-0.93) (Table 2).
Table 2.
Factors associated with influenza vaccination rates using using multivariate logistic regression analysis adjusted for all variables
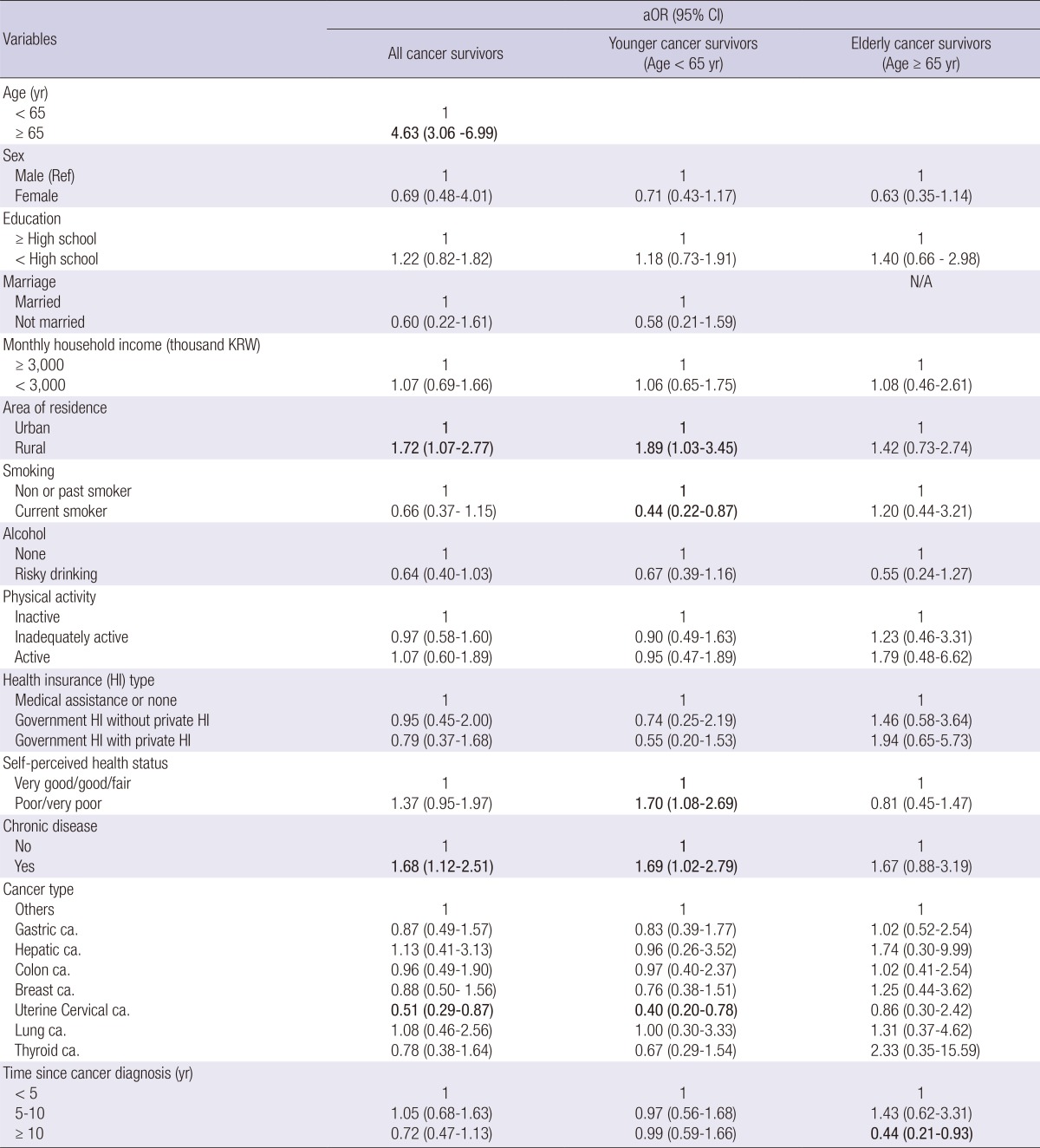
Statistically significant results were written in bold. KRW, Korean Won.
DISCUSSION
To the best of our knowledge, this is the first study to investigate the patterns of influenza vaccination among Korean cancer survivors using representative population. The rate of influenza vaccination among Korean cancer survivors was 50.3% higher than that of the entire Korean population, which was reported as 31.5%. However, the rate of influenza vaccination in younger cancer survivors was 35.4% lower than elderly cancer survivors. Generally, cancer survivors actively utilize preventive healthcare services such as vaccination (22); and high influenza vaccination rates were previously reported for cancer survivors compared to the rates of the general population (23). Although differences in vaccination rates according to cancer type were noted, generally, cancer survivors have high influenza vaccination rate up to 65% (15, 23, 24, 25, 26). However, there is evidence that fewer than 50% of patients are vaccinated in previous studies (27, 28).
Various factors can affect the uptake of influenza vaccination, and in this study, age, area of residence, comorbidities, smoking status, perceived health status, and years since the cancer diagnosis were associated with the influenza vaccination rate among cancer survivors.
Elderly patients exhibited significantly higher influenza vaccination rates after a cancer diagnosis than the younger population; and this finding was consistent with previously reported data (29, 30). This finding may be attributable to the focus on infants and the elderly regarding influenza vaccination recommendations. Furthermore, free influenza vaccinations are offered to people older than 65 yr in some countries including Korea, and thus, the elderly population has greater accessibility to influenza vaccination than the younger population (31). In other words, vaccination insurance coverage for younger cancer survivors is less common than that for elderly cancer survivors (9). Future clinical trials will be needed to increase the rate of influenza vaccination in subpopulations such as younger cancer survivors, because it has been demonstrated that influenza vaccination was related to subsequent reductions in hospitalization related to influenza and high cost-effectiveness for younger cancer survivors as well as elderly cancer survivors (9).
In this study, rural dwellers were more likely to be vaccinated against influenza than urban dwellers. There is little research about influenza vaccination rates in relation to area of residence. However, rural dwellers have less social support and access to medical services when they become ill, and thus, they have a greater need for influenza vaccination as a preventive healthcare service. In particular, more health centers in rural areas than in urban areas actively participate in influenza vaccination programs in Korea.
The comorbidity had statistically significant associations with influenza vaccination rates among cancer survivors, consistent with previous research (30, 32). Cancer survivors with chronic diseases are more likely to receive influenza vaccination than are cancer survivors without chronic diseases because influenza vaccination is recommended for people with this comorbidity. Additionally, cancer survivors with comorbidities have more opportunities to be recommended by their physicians to be vaccinated due to their frequent clinic visits. This trend was noted in previous research in that cancer survivors who frequently visited their healthcare providers were more likely to receive influenza vaccination (32).
In the younger cancer survivor population, current smokers were less likely to receive influenza vaccination. In general, smokers are significantly less likely to use preventive medical services than nonsmokers (33, 34). Our findings were consistent with those of previous studies on the effects of sociodemographic inequalities and health status on influenza vaccination rates (35). Working-age patients with cancer, especially current smokers, are considered a target group to increase the rate of influenza vaccination because they may have a number of barriers to vaccination such as a stressful living situation or a lack of social support concerning vaccination.
Younger cancer survivors with a poor self-assessed health status had a higher vaccine uptake rate than cancer survivors with a good self-assessed health status. This result was consistent with a previous study of the general population (35). Thus, a poor self-assessed health status may be a motivating factor to receive influenza vaccinations. In elderly cancer survivors, a longer time since the cancer diagnosis (more than 10 yr) was associated with a lower influenza vaccination rate. This result was not consistent with previous studies that reported an increase in influenza vaccination rates over time (29, 32). However, other preventive health services were used significantly more commonly within the first 5 yr after cancer diagnosis than at later times (36). According to these results, the time since cancer diagnosis does not affect preventive behaviors, but various socioeconomic and clinical variables should be considered associated factors. In particular, a long duration since cancer diagnosis may lower the desire for preventive healthcare to less than that of the general population.
This study revealed significant variation in influenza vaccination rates across cancer types compared to non-cancer survivors. Gastric, hepatic, colon, and lung cancer patients had significant higher rates for influenza vaccination more than non-cancer survivors'. There was little study to show the differences of rate for influenza vaccination according to cancer types. Previous study to evaluate factors associated with receiving vaccination in cancer survivors did not show the significant cancer types as factor to affect rate for vaccination (17). In multivariate analysis, only cervical cancer was associated with a lower vaccination rate. It is difficult to understand the various characteristics of influenza vaccination uptake according to cancer type. Perhaps these differences could be explained by other sociodemographic and clinical factors such as immunity and treatment. Patients with cervical cancer were reported to have a lower socioeconomic status in a previous study (37), and this factor can affect the use of preventive services.
Although we determined the influenza vaccination rates and related factors for cancer survivors, this study has several limitations that should be considered. First, because much information was collected from self-reported questionnaires, reporting bias cannot be excluded. Second, we unfortunately could not evaluate the treatments used by cancer survivors or cancer staging data, which may have influenced our results. Therefore, this study could not clarify why influenza vaccination rates differed between cancer survivors and non-cancer survivors. Generally, immunity can vary among cancer survivors according to treatment methods, and thus, the immunity of patients can affect both their motivation to be vaccinated and the severity of influenza (38). Third, we did not examine or adjust for variation over time as seasonal influenza strains may differ in severity between years. For example, in a year with a more virulent strain (ex. H1N1 in 2009) more individuals may receive the influenza vaccine than in years with less threatening influenza. Finally, this study did not consider the direct accessibility to healthcare services, which could be a significant factor in preventive behaviors such as the receipt of influenza vaccination (39). Cancer survivors can be encouraged to receive influenza vaccination during consultations with their healthcare providers.
Despite these limitations, this study revealed the status of influenza vaccination and identified factors related to vaccination uptake among cancer survivors. Although the influenza vaccination rate was higher among cancer survivors than among non-cancer survivors, lower vaccination rates were observed for particular groups such as younger cancer survivors, urban dwellers, and cancer survivors without comorbid conditions. Cancer survivors are now living longer and represent a sharply growing population; therefore, immunization against influenza among cancer survivors is a critical component of their preventative healthcare services. Additional research to particular target groups with lower influenza vaccination rates is necessary to protect cancer survivors from the significant mortality related to diseases that can be prevented by vaccination (40).
ACKNOWLEDGMENT
This study was based on Korea National Health & Nutritional Examination Survey, Ministry of Health and Welfare, Republic of Korea. We gratefully acknowledge the numerous investigators involved in the collection and management of data.
Footnotes
We have no conflicts of interest to disclose.
References
- 1.Jung KW, Park S, Kong HJ, Won YJ, Lee JY, Park EC, Lee JS. Cancer statistics in Korea: incidence, mortality, survival, and prevalence in 2008. Cancer Res Treat. 2011;43:1–11. doi: 10.4143/crt.2011.43.1.1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin. 2012;62:10–29. doi: 10.3322/caac.20138. [DOI] [PubMed] [Google Scholar]
- 3.National Cancer Information Center. Cancer incidence. [accessed on 1 November 2012]. Available at http://www.cancer.go.kr/ncic/cics_f/01/011/index.html.
- 4.Cooksley CD, Avritscher EB, Bekele BN, Rolston KV, Geraci JM, Elting LS. Epidemiology and outcomes of serious influenza-related infections in the cancer population. Cancer. 2005;104:618–628. doi: 10.1002/cncr.21203. [DOI] [PubMed] [Google Scholar]
- 5.Prevention and control of influenza: recommendations of the Advisory Committee on Immunization Practices (ACIP): Centers for Disease Control and Prevention. MMWR Recomm Rep. 1996;45:1–24. [PubMed] [Google Scholar]
- 6.Kim HS, Kim JH, Shin SY, Kang YA, Lee HG, Kim JS, Lee JK, Cho B. Fatal cases of 2009 pandemic influenza A (H1N1) in Korea. J Korean Med Sci. 2011;26:22–27. doi: 10.3346/jkms.2011.26.1.22. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Baek JH, Seo YB, Choi WS, Kee SY, Jeong HW, Lee HY, Eun BW, Choo EJ, Lee J, Kim SR, et al. Guideline on the prevention and control of seasonal influenza in healthcare setting. Korean J Intern Med. 2014;29:265–280. doi: 10.3904/kjim.2014.29.2.265. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wingard JR. Influenza: preparedness for an inevitable "Emergency" for oncology and BMT units. J Natl Compr Canc Netw. 2008;6:215–222. doi: 10.6004/jnccn.2008.0018. [DOI] [PubMed] [Google Scholar]
- 9.Avritscher EB, Cooksley CD, Geraci JM, Bekele BN, Cantor SB, Rolston KV, Elting LS. Cost-effectiveness of influenza vaccination in working-age cancer patients. Cancer. 2007;109:2357–2364. doi: 10.1002/cncr.22670. [DOI] [PubMed] [Google Scholar]
- 10.Kunisaki KM, Janoff EN. Influenza in immunosuppressed populations: a review of infection frequency, morbidity, mortality, and vaccine responses. Lancet Infect Dis. 2009;9:493–504. doi: 10.1016/S1473-3099(09)70175-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Rodrigues RS, Marchiori E, Bozza FA, Pitrowsky MT, Velasco E, Soares M, Salluh JI. Chest computed tomography findings in severe influenza pneumonia occurring in neutropenic cancer patients. Clinics (Sao Paulo) 2012;67:313–318. doi: 10.6061/clinics/2012(04)03. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Fiore AE, Shay DK, Broder K, Iskander JK, Uyeki TM, Mootrey G, Bresee JS, Cox NJ Centers for Disease Control and Prevention. Prevention and control of seasonal influenza with vaccines: recommendations of the Advisory Committee on Immunization Practices (ACIP), 2009. MMWR Recomm Rep. 2009;58:1–52. [PubMed] [Google Scholar]
- 13.Snyder CF, Frick KD, Peairs KS, Kantsiper ME, Herbert RJ, Blackford AL, Wolff AC, Earle CC. Comparing care for breast cancer survivors to non-cancer controls: a five-year longitudinal study. J Gen Intern Med. 2009;24:469–474. doi: 10.1007/s11606-009-0903-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Nordøy T, Aaberge IS, Husebekk A, Samdal HH, Steinert S, Melby H, Kolstad A. Cancer patients undergoing chemotherapy show adequate serological response to vaccinations against influenza virus and Streptococcus pneumoniae. Med Oncol. 2002;19:71–78. doi: 10.1385/MO:19:2:71. [DOI] [PubMed] [Google Scholar]
- 15.Ring A, Marx G, Steer C, Prendiville J, Ellis P. Poor uptake of influenza vaccinations in patients receiving cytotoxic chemotherapy. Int J Clin Pract. 2003;57:542–543. [PubMed] [Google Scholar]
- 16.Shih YC, Pan IW. Influenza vaccination among individuals with cancer and their family members. Am J Prev Med. 2010;38:61–69. doi: 10.1016/j.amepre.2009.09.032. [DOI] [PubMed] [Google Scholar]
- 17.Shin DW, Kim Y, Park JH, Cho J, Jho HJ, Yang HK, Kim HS, Kim SY. Practices and predictors of 2009 H1N1 vaccination in cancer patients: a nationwide survey in Korea. Influenza Other Respir Viruses. 2012;6:e120–e128. doi: 10.1111/j.1750-2659.2012.00378.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ganry O, Baudoin C, Fardellone P. Effect of alcohol intake on bone mineral density in elderly women: the EPIDOS Study: Epidémiologie de l'Ostéoporose. Am J Epidemiol. 2000;151:773–780. doi: 10.1093/oxfordjournals.aje.a010277. [DOI] [PubMed] [Google Scholar]
- 19.Han MA, Kim KS, Park J, Kang MG, Ryu SY. Association between levels of physical activity and poor self-rated health in Korean adults: the Third Korea National Health and Nutrition Examination Survey (KNHANES), 2005. Public Health. 2009;123:665–669. doi: 10.1016/j.puhe.2009.08.005. [DOI] [PubMed] [Google Scholar]
- 20.Nagata JM, Hernández-Ramos I, Kurup AS, Albrecht D, Vivas-Torrealba C, Franco-Paredes C. Social determinants of health and seasonal influenza vaccination in adults ≥65 years: a systematic review of qualitative and quantitative data. BMC Public Health. 2013;13:388. doi: 10.1186/1471-2458-13-388. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Armstrong K, Berlin M, Schwartz JS, Propert K, Ubel PA. Barriers to influenza immunization in a low-income urban population. Am J Prev Med. 2001;20:21–25. doi: 10.1016/s0749-3797(00)00263-4. [DOI] [PubMed] [Google Scholar]
- 22.Fairley TL, Hawk H, Pierre S. Health behaviors and quality of life of cancer survivors in Massachusetts, 2006: data use for comprehensive cancer control. Prev Chronic Dis. 2010;7:A09. [PMC free article] [PubMed] [Google Scholar]
- 23.Kwong JC, Rosella LC, Johansen H. Trends in influenza vaccination in Canada, 1996/1997 to 2005. Health Rep. 2007;18:9–19. [PubMed] [Google Scholar]
- 24.Baldwin LM, Dobie SA, Cai Y, Saver BG, Green PK, Wang CY. Receipt of general medical care by colorectal cancer patients: a longitudinal study. J Am Board Fam Med. 2011;24:57–68. doi: 10.3122/jabfm.2011.01.100080. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Underwood JM, Townsend JS, Stewart SL, Buchannan N, Ekwueme DU, Hawkins NA, Li J, Peaker B, Pollack LA, Richards TB, et al. Surveillance of demographic characteristics and health behaviors among adult cancer survivors: Behavioral Risk Factor Surveillance System, United States, 2009. MMWR Surveill Summ. 2012;61:1–23. [PubMed] [Google Scholar]
- 26.Chin-Yee BH, Monkman K, Hussain Z, Minuk LA. Attitudes toward vaccination for pandemic H1N1 and seasonal influenza in patients with hematologic malignancies. J Support Oncol. 2011;9:156–160. doi: 10.1016/j.suponc.2011.03.006. [DOI] [PubMed] [Google Scholar]
- 27.Loulergue P, Mir O, Alexandre J, Ropert S, Goldwasser F, Launay O. Low influenza vaccination rate among patients receiving chemotherapy for cancer. Ann Oncol. 2008;19:1658. doi: 10.1093/annonc/mdn531. [DOI] [PubMed] [Google Scholar]
- 28.Sommer AL, Wachel BK, Smith JA. Evaluation of vaccine dosing in patients with solid tumors receiving myelosuppressive chemotherapy. J Oncol Pharm Pract. 2006;12:143–154. doi: 10.1177/1078155206070868. [DOI] [PubMed] [Google Scholar]
- 29.Snyder CF, Frick KD, Herbert RJ, Blackford AL, Neville BA, Carducci MA, Earle CC. Preventive care in prostate cancer patients: following diagnosis and for five-year survivors. J Cancer Surviv. 2011;5:283–291. doi: 10.1007/s11764-011-0181-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Snyder CF, Earle CC, Herbert RJ, Neville BA, Blackford AL, Frick KD. Trends in follow-up and preventive care for colorectal cancer survivors. J Gen Intern Med. 2008;23:254–259. doi: 10.1007/s11606-007-0497-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Australian Government Department of Health. [accessed on 1 September 2013]. Avaliable at http://www.health.gov.au/internet/immunise/publishing.nsf/Content/immunise-influenza.
- 32.Snyder CF, Earle CC, Herbert RJ, Neville BA, Blackford AL, Frick KD. Preventive care for colorectal cancer survivors: a 5-year longitudinal study. J Clin Oncol. 2008;26:1073–1079. doi: 10.1200/JCO.2007.11.9859. [DOI] [PubMed] [Google Scholar]
- 33.Takayama M, Wetmore CM, Mokdad AH. Characteristics associated with the uptake of influenza vaccination among adults in the United States. Prev Med. 2012;54:358–362. doi: 10.1016/j.ypmed.2012.03.008. [DOI] [PubMed] [Google Scholar]
- 34.Vander Weg MW, Howren MB, Cai X. Use of routine clinical preventive services among daily smokers, non-daily smokers, former smokers, and never-smokers. Nicotine Tob Res. 2012;14:123–130. doi: 10.1093/ntr/ntr141. [DOI] [PubMed] [Google Scholar]
- 35.La Torre G, Iarocci G, Cadeddu C, Boccia A. Influence of sociodemographic inequalities and chronic conditions on influenza vaccination coverage in Italy: results from a survey in the general population. Public Health. 2010;124:690–697. doi: 10.1016/j.puhe.2010.06.006. [DOI] [PubMed] [Google Scholar]
- 36.Suh B, Shin DW, Kim SY, Park JH, Chang WY, Lim SP, Yim CY, Cho BL, Park EC, Park JH. Mode of primary cancer detection as an indicator of screening practice for second primary cancer in cancer survivors: a nationwide survey in Korea. BMC Cancer. 2012;12:557. doi: 10.1186/1471-2407-12-557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Van der Aa MA, Siesling S, Louwman MW, Visser O, Pukkala E, Coebergh JW. Geographical relationships between sociodemographic factors and incidence of cervical cancer in the Netherlands 1989-2003. Eur J Cancer Prev. 2008;17:453–459. doi: 10.1097/CEJ.0b013e3282f75ed0. [DOI] [PubMed] [Google Scholar]
- 38.Souza TM, Salluh JI, Bozza FA, Mesquita M, Soares M, Motta FC, Pitrowsky MT, de Lourdes, Mishin VP, Gubareva LV, et al. H1N1pdm influenza infection in hospitalized cancer patients: clinical evolution and viral analysis. PLoS One. 2010;5:e14158. doi: 10.1371/journal.pone.0014158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Kwong EW, Lam IO, Chan TM. What factors affect influenza vaccine uptake among community-dwelling older Chinese people in Hong Kong general outpatient clinics? J Clin Nurs. 2009;18:960–971. doi: 10.1111/j.1365-2702.2008.02548.x. [DOI] [PubMed] [Google Scholar]
- 40.Arrowood JR, Hayney MS. Immunization recommendations for adults with cancer. Ann Pharmacother. 2002;36:1219–1229. doi: 10.1345/aph.1A277. [DOI] [PubMed] [Google Scholar]