

Abstract
Background
Pro re nata (PRN) prescription is a frequently used prescription method in hospitals. This study was conducted to investigate actual condition of PRN prescription and whether administration error occurred because of perception difference between doctors and nurses.
Methods
From May to July 2012, a survey was conducted among 746 doctors and nurses (88 doctors and 658 nurses) working at 5 hospitals located in Seoul, Gyeong-gi, and Gangwon Province. Doctors generating PRN prescription responded to actual conditions of PRN prescription and both doctors and nurses reported whether administration error occurred due to perception difference.
Results
Average number of PRN prescription of surgical residents was 4.6 ± 5.4, which was larger than that of medical residents (1.7 ± 1.0). Surgical residents more frequently recorded maximum number of daily intake (P = 0.034) and, although not statistically significant, more often wrote exact single dosage (P = 0.053) and maximum dosage per day (P = 0.333) than medical residents. Doctors expected nurses to notify them before the administration of medication; however, nurses were more likely to conduct PRN administration by their own decision without informing doctors. In addition, some doctors and nurses experienced administration errors because of it.
Conclusion
Standard prescription methods need to be established since there is a perception difference in PRN prescription between doctors and nurses and this could be related to administration errors.
Keywords: Drug Prescription, Perception, Medication Errors
INTRODUCTION
The PRN prescription stands for 'pro re nata,' which means that the administration of medication is not scheduled. Instead, the prescription is taken as needed. In previous studies, the administration of psychiatric medications in response to changes in patient symptoms and pain management in postoperative patients has shown to benefit from PRN prescriptions.1,2,3,4,5,6,7) Consequently, hospitals commonly resort to a PRN prescription for admitted patients. However, the PRN prescription can become a serious medical problem if differences in the perception of the PRN prescription between doctors and nurses lead to unnecessary prescriptions, or the lack of necessary prescriptions.
To prevent medication errors in cases of PRN prescriptions, the exact single dosage of the medication prescribed, the maximum daily intake, and the maximum dosage per day must be clearly articulated. Additionally, an appropriate level of communication must occur between the PRN-prescribing doctors and the administering nurses, to implement the correct regimen of medication for the patient. However, the segmentation and specialization of the respective occupations becomes an impediment to appropriate levels of communication,8) and because of the differences in the perception of medical problems between doctors and nurses,9) efforts should be made to narrow the discrepancy between these differences.
The present study investigated the perception of PRN prescription, its actual practice within hospitals, and experiences of medication errors by residents and ward nurses who assist with the administration of PRN prescription in five hospitals. Through the above investigation, the study tried to acquire basic data regarding methods for effective PRN prescription and prevention of medication errors.
METHODS
1. Study Participants
From May 2012 to July 2012, a survey was conducted in five hospitals in Seoul, Gyeong-gi, and Gangwon Province (Kangnam, Kangdong, Chuncheon, Hangang, and Hallym University Sacred Heart Hospital) targeting doctors and nurses working at the hospitals. The doctor subgroup of the study participants consisted of first-year residents who prescribed medications directly to patients as a primary care physician. Residents with specialties such as radiology and pathology who did not directly prescribe medications to patients were excluded from the study. The nurse subgroup of the study participants consisted of ward nurses who directly receive and administer the prescriptions of residents. Survey responses that were deemed incomplete or inappropriate were excluded from the study to bring the total number of study participants to 746 people (88 doctors and 658 nurses).
2. Survey
The survey sought to investigate the perception and the actual practice of administering PRN prescriptions within the hospital. In terms of the characteristics of the study participants, age, gender, affiliated hospital, affiliated department, and years of experience were investigated. To examine the actual administration of the PRN prescription, doctors who reported to have directly prescribed medications to patients were asked to respond whether they articulated or recorded information such as maximum dosage per day, maximum number of daily intake, exact single dosage, and which conditions necessitate medication when providing PRN prescription to patients. The doctors were asked to answer the above questions using the following responses: "always," "mostly," "on average," "mostly not," and "never." When performing statistical analysis, "always" and "mostly" were grouped into a single "mostly" category, and "mostly not" and "never" were grouped into a single "mostly not" category, to avail three categories, "mostly," "on average," and "mostly not" for statistical analysis. To identify a difference in perception with respect to PRN prescription, the participants were asked to provide a maximum of two responses to the following statements: "medications that are commonly involved in PRN prescription and reasons for the PRN prescription of such medications" and "reasons that PRN prescriptions in general are necessary."
The surveys for nurses were distributed to individual wards and collected, whereas the surveys for residents were distributed on the last day of group educational program for first-year residents.
3. Statistical Analysis
The data acquired through the surveys were analyzed using IBM SPSS ver. 20.0 (IBM Co., Armonk, NY, USA). The significance level of the data was set to P < 0.05. The residents and nurses were categorized into medical group and surgical group, based on the affiliated department for residents and the primary wards for nurses, respectively. To examine the difference between the medical and surgical group, a chi-square test and Fisher's exact test were performed. In addition, the perception difference in PRN prescription between doctors and nurses was examined by performing a chi-square test and Fisher's exact test.
RESULTS
1. Characteristics of the Study Participants
Among the 746 ultimately selected study participants, 88 were residents and 658 were nurses. Based on the affiliated department of the residents and the primary ward of the nurses, the participants were divided into medical group (internal medicine, neurology, etc.) and surgical group (general surgery, orthopedics, etc.), and compared. Among the 88 residents, 48 were male and 40 were female. In addition, 47 were affiliated with the medical group, whereas 41 were involved with the surgical group (Table 1). The average age of the residents was 28.9 ± 2.2. Among the 658 nurses, 10 were male and 648 were female. Additionally, 305 belonged to the medical group and 353 belonged to the surgical group. The average age of the nurses was 29.6 ± 5.9.
Table 1.
General characteristics of the study population (n = 746)
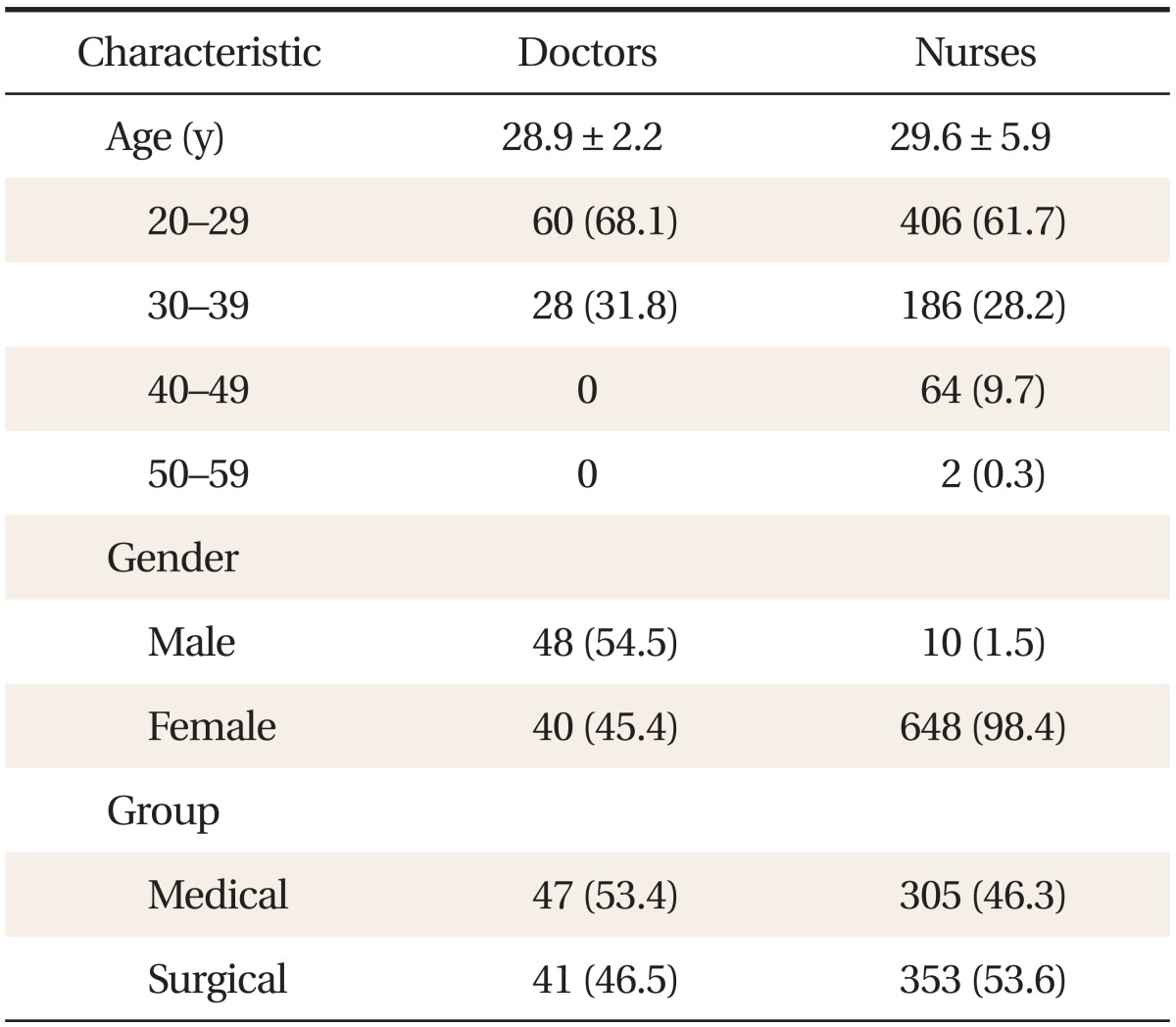
Values are presented as mean ± SD or number (%).
2. The Actual Practice of PRN Prescription by Doctors
Whereas the average number of patients managed by a medical resident was 10.8 ± 6.7, the average number of patients managed by a surgical resident was greater, at 19.4 ± 13.3. A medical resident prescribed an average of 1.7 ± 1.0 PRN prescriptions per patient to 53.6% of the patients under the resident's care. However, the surgical resident prescribed an average of 4.6 ± 5.4 PRN prescriptions per patient to 63.4% of their patients (P = 0.001).
With respect to the medical residents, 38.3% responded that they prescribe PRN medication to all of the patients under their care, 57.4% responded that they prescribe PRN medication on an as-needed basis, and 4.2% responded that they do not prescribe PRN medications. However, 43.9% of the surgical residents responded that they prescribe PRN medication to all the patients, and 56.1% responded that they prescribe it on an as-needed basis. There were no surgical residents who did not prescribe PRN medication. There was no statistical difference between the two groups (Table 2).
Table 2.
Actual condition of PRN prescription by doctors
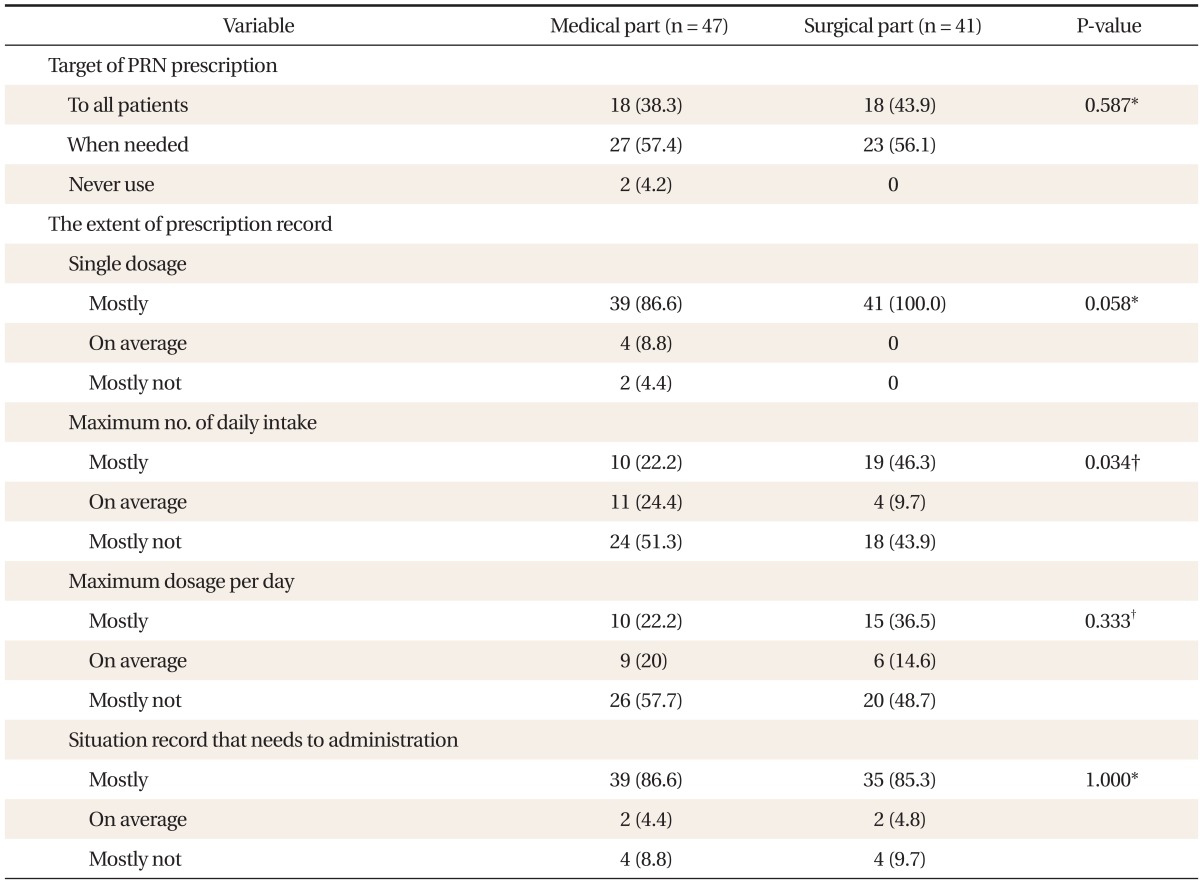
Values are presented as number (%).
PRN: pro re nata.
*By Fisher's exact test. †By chi-square test.
When making a PRN prescription, 100% of the surgical residents reported recording a single recommended dose of medication, and 86.6% of the medical residents reported recording it. Despite the fact that surgical residents have an ostensibly better record of information provision, there was no statistical significance (P = 0.058). With respect to the maximum daily intake, 46.3% of the surgical residents reported that they "mostly" record the information, whereas only 22.2% of the medical residents reported that they "mostly" record it. In other words, surgical residents articulate the maximum number of daily intake significantly better than the medical residents (P = 0.034). With respect to maximum dosage per day, 36.5% of the surgical residents reported "mostly" recording the data, whereas only 22.2% of the medical residents reported "mostly" recording the data (P = 0.333). A similar proportion of doctors reported recording the conditions for the intake of medication: 86.6% for medical residents, and 85.3% for surgical residents (Table 2).
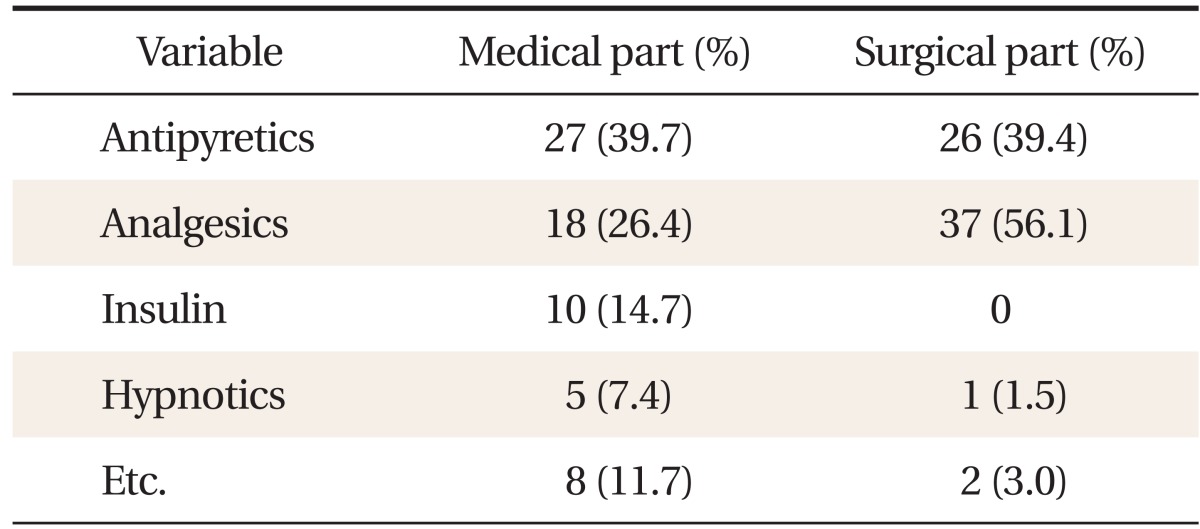
The types of medications prescribed as PRN were also shown to differ between medical and surgical group. In the medical group, the types of PRN medications reported were antipyretics (39.7%), analgesics (26.4%), insulin (14.7%), hypnotics (7.4%), and others (11.7%). In the surgical group, they were typically limited to analgesics (56.1%) and antipyretics (39.4%) (Table 3).
Table 3.
Type of medicines prescribed as pro re nata
With respect to the reasons that residents order PRN prescriptions, medical residents most commonly responded with, "To quickly respond to patient symptoms" (61.7%). The second most common reason was "To decrease the hassle of writing a prescription order for every situation" (42.6%). With respect to the surgical residents, 70.7% of the residents have reasoned that they order PRN prescriptions "To decrease the hassle of writing a prescription order for every situation," followed by "To quickly respond to patient symptoms" (51.2%).
3. The Necessity of PRN Prescription
Asked whether PRN prescription was necessary, 88.8% of the medical residents, 95.1% of surgical residents, 92.1% of medical nurses, and 94.0% of surgical nurses reported that it was. The most common reason for the necessity of PRN prescription was "To quickly respond to patient symptoms" (79.1%), followed by "To decrease the hassle of writing a prescription order for every situation" (28.2%), and "In cases of difficulties in contacting the residents" (25.5%).
4. Residents' Expectations of Nursing Behavior in Cases of PRN Prescription, and Actual Nursing Behavior
In cases of PRN prescription, 64.4% of the medical residents who had articulated the conditions in which PRN medications should be administered, expected nurses to consult the resident prior to the administration of the PRN medication. In reality, 56.0% of the nurses responded that they confer with the residents prior to the administration of the medication. Additionally, in cases where the resident did not record and articulate the conditions in which the medications should be administered, 100.0% of the residents expected the nurses to execute the PRN administration after first conferring with the residents. In reality, 93.7% of the nurses responded that they confer with the residents prior to the administration of the medication in such cases. In summation, there was no statistically significant difference between the residents' expectations of nursing behavior with respect to PRN medications, and the actual nursing behavior. However, in the surgical field, 56.0% of the surgical residents expected nurses to consult with them if the resident had articulated or recorded the conditions in which the medication should be administered. In reality, only 43.3% of the nurses administered the medication after consulting with the resident. When the resident had not articulated or recorded the conditions in which the PRN medication should be administered, 95.1% of the residents expected the nurses to consult with them prior to the administration of the medication. In reality, only 82.4% of the nurses reported consulting the residents prior to the administration of medication. As such, there was a statistically significant difference between the residents' expectations and the actual nursing behavior in the surgical field (Table 4).
Table 4.
Expected versus actual nurses' behavior to pro re nata administration
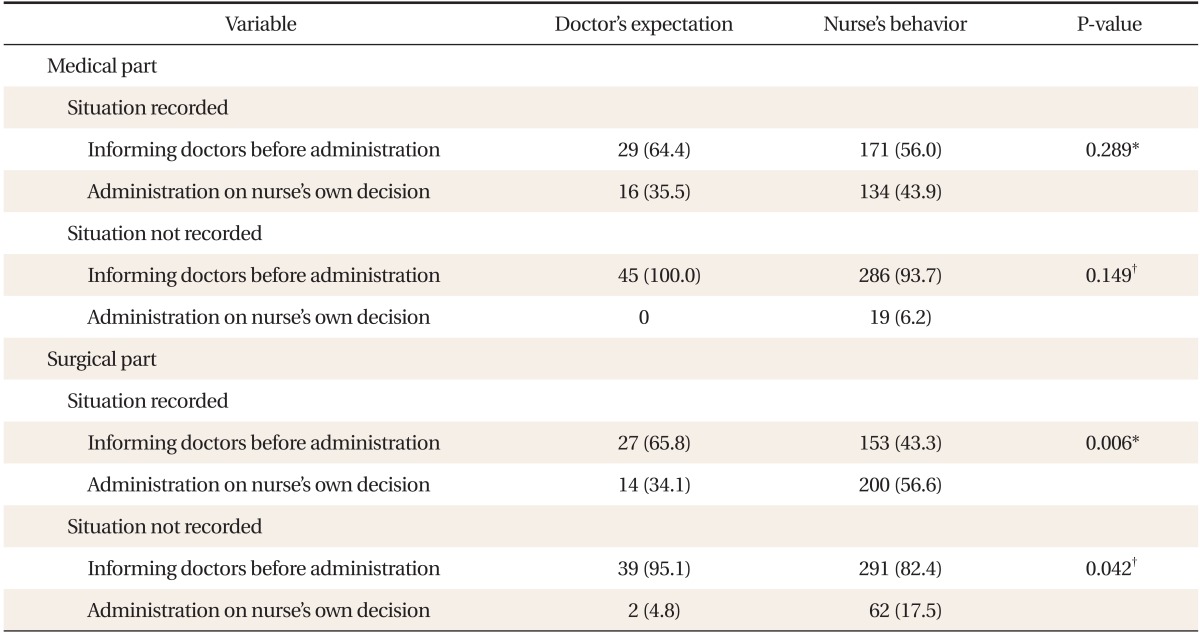
Values are presented as number (%).
*By chi-square test. †By Fisher's exact test.
5. Medication Error
When the study participants were asked whether they had experienced instances where a patient did not receive the necessary medication or received unnecessary medication because of a misalignment between the residents' expectation and the actual nursing behavior, 8 medical residents (17.0%) and 6 surgical residents (14.6%) reported affirmatively. With respect to the frequency of such experiences, medical residents reported an instance of medication error per 35 patients, whereas the surgical residents reported an instance per 11 patients (Table 5).
Table 5.
Experiences of administration error
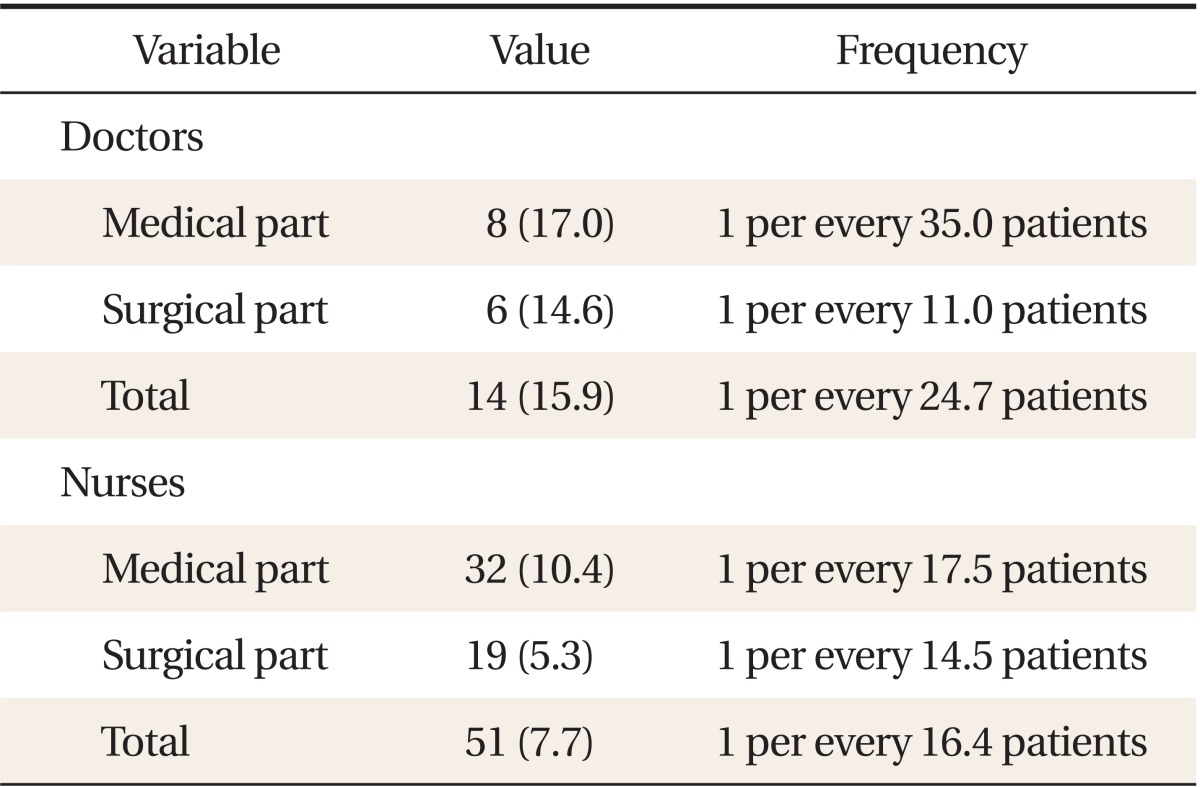
Values are presented as number (%).
With respect to the response of the nurses, 32 medical nurses (10.4%) reported having an experience of medication error, whereas 19 surgical nurses (5.3%) reported having such an experience. When asked about the frequency of the experience, the medical nurses and surgical nurses reported an instance per 17.5 patients, and an instance per 14.5 patients, respectively (Table 5).
DISCUSSION
The PRN prescription is a common treatment method for hospitalized patients. If appropriate, a PRN prescription can aid in the treatment of the patient's disease and ease the patient's symptoms.1,2,3,4,5,6,7) However, abuse or misuse of a PRN prescription can negatively influence the treatment of the patient. To prevent such risks, a sufficient level of communication must exist between the resident who directly prescribes medications to patients under her/his care, and the nurse who administers such prescriptions.
The present study confirmed that the majority of residents and nurses believe that PRN prescription is necessary. Furthermore, the study investigated the actual practice of prescribing PRN medications, as well as the perception difference in PRN prescription between residents and nurses. Compared to medical residents, surgical residents have reported resorting to PRN prescriptions more frequently. They also reported prescribing a higher quantity of PRN mediations than medical residents. The reason for the above phenomenon may be that the number of patients under the care of surgical residents is greater than that of medical residents. As such, a higher rate of PRN prescriptions by surgical residents is considered to be a manner of increasing their efficiency in patient care. However, significantly more surgical residents reported clarifying the maximum number of daily intake; and, although the result was not statistically significant, more surgical residents also reported they prescribe the maximum dosage per day than medical residents. Such differences may be attributed to surgical residents and nurses having fewer experiences of medication errors.
The present study shows that the residents' expectation of the nurses' administration of PRN prescriptions is different from the nurses' actual practice. Whereas residents wanted nurses to confer with them before administering the PRN prescriptions, in practice nurses frequently did not confer with residents when they administered PRN prescriptions. Although the above survey outcome was not statistically significant in the medical group, for cases in which conditions for administering the medication are articulated by the residents, 64.4% of the residents wanted the nurses to administer the medication after conferring with them, but only 56.0% of nurses conformed to these expectations. Furthermore, if the resident did not articulate the conditions in which medications should be administered, 100% of the medical residents expected the nurses to confer with them prior to the administration of the PRN medication. Additionally, surgical residents expressed an expectation of nurses conferring with them prior to the administrating of PRN prescriptions, regardless of providing a record of conditions for administering the medication. However, nurses in the surgical field did not conform to the expectations of the residents, and administered PRN medication without prior consultation with the doctor. This difference in perception was shown to be statistically significant. This survey result shows that there was a perception difference in the practice of PRN prescription between the residents and the nurses. Nurses work on rotation in various wards for a designated period. Similarly, circumstances can compel residents to prescribe medications to patients in wards not assigned under their care. Both of these work environment circumstances increase the chance of incurring medication error when perception differences in PRN prescriptions exist. Consequently, the perceived differences between the doctors and nurses should be considered by the hospital organization, to provide a protocol and education modules for narrowing the discrepancy in perception. The administration of PRN prescriptions by nurses is based on their knowledge of the drug, as well as their interpretation of the prescription intention.10) Nurses have also reported that the most considerable barrier to pain management for admitted patients is insufficient contact with doctors, and difficulties in communicating with doctors.11) Additionally, it has been reported that many medication errors are caused by difficulties in communication between the patient and the medical professionals, as well as difficulties in communication among the medical professionals themselves.12) The present study corroborated the findings of the precedent studies, confirming that some medication errors are the result of differences between residents' expectation of nurses in terms of PRN prescription, and the nurses' actual practice of PRN administration. Such discrepancies in perceptions must be rectified in pursuant to the proper treatment of the patient. In the present study, it was also found that the residents and nurses in the medical field experienced greater frequencies of medication errors, compared to those in the surgical field. This result was contrary to expectations, as it was expected that medical professionals in the surgical field would have experienced a greater number of medication errors due to the greater frequency of PRN prescriptions. As previously mentioned, the experience of fewer medication errors can be attributed to the more meticulous provision of records regarding exact single dosage, maximum number of daily intake, and maximum dosage per day by the medical professionals of the surgical field, compared to those in the medical field. However, the above cause may also be overdetermined by the fact that the prescription of medications in the medical field requires greater expertise and specialization than that of the surgical field. This can be inferred by the medication regimen commonly used by the two fields in PRN prescriptions, wherein medical residents exhibited a relatively even distribution in their prescriptions of analgesics, antipyretics, insulin, hypnotics, and other medications, whereas surgical residents prescribed a limited range of PRN prescription medications, primarily consisting of analgesics and antipyretics. Because the proportion of actual administration of medication to the patient given the PRN prescription was not investigated, we cannot conclude that a greater frequency of PRN prescription necessarily leads to a greater frequency in the administration of the prescribed PRN medication. The absence of such investigation reflects a limitation in the present study, in that we could not compare the rate of the actual administration of the PRN prescribed medications among the subgroups of the study participants.
Even though a greater proportion of doctors and nurses in the medical field reported having an experience of medication error than those in the surgical field, the frequency of medication errors experienced by individual residents and nurses is higher in the surgical field than the medical field, such that a medical resident experienced one instance of medication error per 35 patients, whereas a surgical resident experienced one instance of medication error per 11 patients. Consequently, further studies must be conducted to examine how individuals are associated with medication errors, irrespective of their departmental affiliations.
The majority of medical professionals have collectively suggested that PRN prescription is necessary for seamless patient care. However, the lack of protocol in doctor and nursing training and hospital policy, with respect to a detailed education in PRN prescription, has resulted in the execution of PRN prescription primarily based on past experience. The effective administration of PRN prescriptions should be built on sufficiently shared general knowledge regarding the prescribed medication, exact understanding the patient condition,13) and an appropriate level of communication between doctors and nurses, as well as patient involvement.14) As such, a guideline that reflects the above convictions of unified perception and administration of PRN prescription should be established and implemented.
The present study has various limitations. First, as the study was based on a survey, the study results were dependent on the memories of the study participants. As such, participants may have failed to recall memories of medication error or falsely recalled fabricated memories of a medication error. Second, it was difficult to objectively compare and determine whether the participants were in fact behaving in alignment with their responses to the survey. Third, the present study could not confirm the degree to which PRN prescriptions were actually being administered in practice. Such limitations require revisions and supplementations through future studies.
Footnotes
No potential conflict of interest relevant to this article was reported.
References
- 1.Caisley H, Muller U. Adherence to medication in adults with attention deficit hyperactivity disorder and pro re nata dosing of psychostimulants: a systematic review. Eur Psychiatry. 2012;27:343–349. doi: 10.1016/j.eurpsy.2012.01.002. [DOI] [PubMed] [Google Scholar]
- 2.Stein-Parbury J, Reid K, Smith N, Mouhanna D, Lamont F. Use of pro re nata medications in acute inpatient care. Aust N Z J Psychiatry. 2008;42:283–292. doi: 10.1080/00048670701881553. [DOI] [PubMed] [Google Scholar]
- 3.Geffen J, Cameron A, Sorensen L, Stokes J, Roberts MS, Geffen L. Pro re nata medication for psychoses: the knowledge and beliefs of doctors and nurses. Aust N Z J Psychiatry. 2002;36:642–648. doi: 10.1046/j.1440-1614.2002.01068.x. [DOI] [PubMed] [Google Scholar]
- 4.Baker JA, Lovell K, Harris N. A best-evidence synthesis review of the administration of psychotropic pro re nata (PRN) medication in in-patient mental health settings. J Clin Nurs. 2008;17:1122–1131. doi: 10.1111/j.1365-2702.2007.02236.x. [DOI] [PubMed] [Google Scholar]
- 5.Smyth W, Toombes J, Usher K. Children's postoperative pro re nata (PRN) analgesia: nurses' administration practices. Contemp Nurse. 2011;37:160–172. doi: 10.5172/conu.2011.37.2.160. [DOI] [PubMed] [Google Scholar]
- 6.Lee JK, Kim JM, Chung JK, Cheun JK. Patient controlled analgesia for pain management after upper abdominal surgery. J Korean Pain Soc. 1992;5:229–233. [Google Scholar]
- 7.Moon YS, Lee HR, Yeom CH. The analysis of analgesic use in hospitalized terminal cancer patients. J Korean Acad Fam Med. 1996;17:827–833. [Google Scholar]
- 8.Kim YS, Park JH, Lim KY. Interpersonal conflicts and communication among medical residents, nurses and technologists. Korean J Hosp Manage. 2006;11:16–31. [Google Scholar]
- 9.Han SS. Doctor's and nurses' perception and experiences of DNR. J Korean Acad Nurs Adm. 2005;11:255–264. [Google Scholar]
- 10.Gordon DB, Pellino TA, Higgins GA, Pasero C, Murphy-Ende K. Nurses' opinions on appropriate administration of PRN range opioid analgesic orders for acute pain. Pain Manag Nurs. 2008;9:131–140. doi: 10.1016/j.pmn.2008.03.003. [DOI] [PubMed] [Google Scholar]
- 11.Titler MG, Herr K, Schilling ML, Marsh JL, Xie XJ, Ardery G, et al. Acute pain treatment for older adults hospitalized with hip fracture: current nursing practices and perceived barriers. Appl Nurs Res. 2003;16:211–227. doi: 10.1016/s0897-1897(03)00051-x. [DOI] [PubMed] [Google Scholar]
- 12.Benjamin DM. Reducing medication errors and increasing patient safety: case studies in clinical pharmacology. J Clin Pharmacol. 2003;43:768–783. [PubMed] [Google Scholar]
- 13.Szczesny S, Miller M. PRN medication use in inpatient psychiatry. J Psychosoc Nurs Ment Health Serv. 2003;41:16–21. doi: 10.3928/0279-3695-20030101-09. [DOI] [PubMed] [Google Scholar]
- 14.Cumbler E, Wald H, Kutner J. Lack of patient knowledge regarding hospital medications. J Hosp Med. 2010;5:83–86. doi: 10.1002/jhm.566. [DOI] [PubMed] [Google Scholar]