

Abstract
BACKGROUND:
Acute kidney injury (AKI) is associated with a high mortality. This study was undertaken to detect the factors associated with the prognosis of AKI.
METHODS:
We retrospectively reviewed 98 patients with AKI treated from March 2008 to August 2009 at this hospital. In these patients, 60 were male and 38 female. Their age ranged from 19 to 89 years (mean 52.4±16.1 years). The excluded patients were those who died within 24 hours after admission to ICU or those who had a history of chronic kidney disease or incomplete data. After 60 days of treatment, the patients were divided into a survival group and a death group. Clinical data including gender, age, history of chronic diseases, the worst laboratory values within 24 hours after diagnosis (values of routine blood tests, blood gas analysis, liver and renal function, levels of serum cystatin C, and blood electrolytes) were analyzed. Acute physiology, chronic health evaluation (APACHE) II scores and 60-day mortality were calculated. Univariate analysis was performed to find variables relevant to prognosis, odds ratio (OR) and 95% confidence interval (CI). Multiple-factor analysis with logistic regression analysis was made to analyze the correlation between risk factors and mortality.
RESULTS:
The 60-day mortality was 34.7% (34/98). The APACHE II score of the death group was higher than that of the survival group (17.4±4.3 vs. 14.2±4.8, P<0.05). The mortality of the patients with a high level of cystatin C>1.3 mg/L was higher than that of the patients with a low level of cystatin C (<1.3 mg/L) (50% vs. 20%, P<0.05). The univariate analysis indicated that organ failures≥2, oliguria, APACHE II>15 scores, cystatin C>1.3 mg/L, cystatin C>1.3 mg/L+APACHE II>15 scores were the risk factors of AKI. Logistic regression analysis, however, showed that organ failures≥2, oliguria, cystatin C>1.3 mg/L +APACHE II>15 scores were the independent risk factors of AKI.
CONCLUSION:
Cystatin C>1.3 mg/L+APACHE II>15 scores is useful in predicting adverse clinical outcomes in patients with AKI.
KEY WORDS: Intensive care unit, Acute kidney injury, Serum cystatin C, APACHE II, Oliguria, Retrospective studies, Prognosis
INTRODUCTION
In research into the cause of high mortality in critically ill patients in intensive care unit, the kidney has been recognized one of the most vulnerable organs, and the incidence of acute renal failure (ARF) and its mortality are very high.[1,2] Researchers have suggested acute kidney injury (AKI) instead of ARF be more emphasized in improving prognosis and reducing mortality. [3] Unfortunately, the indicators for precisely predicting the severity of AKI patients are lacking.
Based on the clinical data of the 98 AKI patients, we investigated the risk factors for patient death.
METHODS
Patients
Enrolled in this study were the 98 patients with AKI who had been admitted to the Second Affiliated Hospital of Xi’an Jiaotong University and Xiangya Hospital of Central-South University from March 2008 to August 2009. They met the criteria set by the acute kidney injury network (AKIN) in Amsterdam in September 2009.[3] Twenty-two patients who died within 24 hours after admission to the ICU or who had incomplete data or a history of chronic renal disease were excluded.
Methods
The clinical data including gender, age, history of chronic diseases, and the worst laboratory values within 24 hours of diagnosis (routine blood tests, blood gas analysis, and tests of liver and renal function, levels of serum cystatin C, and blood electrolytes) were analyzed. Acute physiology, chronic health evaluation (APACHE)II scores and 60-day mortality were calculated. Immediately after admission to ICU, the outcome (death or survival) of the patients was followed up for 60 days. Some severe patients were also included in this study for they were followed up less than 60 days but longer than 24 hours.
Assignment of variables
Death or not (0:no, 1:yes),age (0:≥60 years old, 1 :>60 years old), gender (0: female,1:male), APACHE II score (0:≤15, 1:>15), Cys C (0:<1.02 mg/l, 1:≥1.02 mg/l), pH (0:≥7.35, 1:<7.35), urine (0:≥0.5 ml/kg per hour, 1:<0.5 ml/kg per hour for 6 hours, 2:<0.5 ml/kg per hour for 12 hours, 3:<0.3 ml/kg per hour for 24 hours), the number of dysfunction organs (0:<2, 1:≥2), mechanical ventilation (0:no, 1:yes), CRRT (0:no, 1:yes), APACHE II>15+Cys C>1.3 mg/L (0:no, 1:yes).
Statistical analysis
All data were expressed as mean±SD. Pearson’s product-moment correlation coefficient test was used for the comparison of quantitative data. Single factor analysis was performed to screen the factors associated with the prognosis, and then logistic regression analysis was made to detect the independent risk factors for patient death. P<0.05 was considered statistically significant.
RESULTS
Clinical data
In the 98 patients, 34 (34.7%) died, and 64 (62.6%) survived. Mean APACHE II score was (15.4±4.6), and the level of cystatin C was (1.8±1.5) mg/L. In AKI patients with APACHE II score>15, those with cystatin C level>1.3 mg/L, and those with APACHE II score>15 plus cystatin C level>1.3 mg/L, the mortality was 48% (24/50), 50% (24/48), and 57.1% (16/28), respectively.
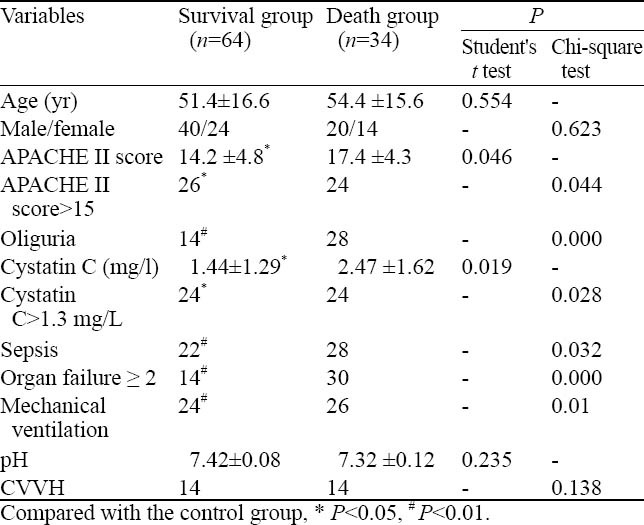
Sixty days after diagnosis, the 98 patients were divided into a survival group and a death group. There were significant differences in other variables except age, gender, pH between the two groups (Table 1).
Table 1.
Comparison of clinical data between the survival group and death group (n=98)
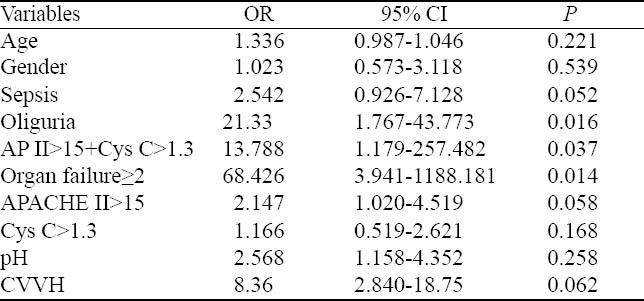
Univariate logistic regression analysis
Twelve factors were analyzed using univariate logistic regression analysis, and the results showed three significant factors (Table 2). APACHE II score>15+cystatin C>1.3 mg/L, organ failure ≥ 2, and oliguria were found to be associated with AKI (P<0.05).
Table 2.
Univariate logistic regression analysis of risk factors for AKI patients
Multivariate logistic regression analysis
We considered death and survival as the dependent variables (7=1.0) and logistic conditional regression analysis was performed. APACHE II score>15+cystatin C>1.3 mg/L and organ failure ≥ 2 were considered the independent factors (P<0.05) (Table 3).
Table 3.
Independent lethal risk factors for AKI patients

DISCUSSION
In recent years, new methods have been used in the diagnosis and treatment of patients with AKI. The reported mortality of AKI varied from 14.6% to 83%.[4-6] The causes for the mortality may be due to different criteria of exclusion and inclusion, the severity of renal damage, as well as the severity of AKI. In this study the hospital mortality was 34.7%, which was consistent with a mortality of 38.75% reported by Liu et al.[7]
Research has been concentrated on the indicators for prognosis of AKI. Clinical trials revealed that age, APACHE II score, mechanical ventilation, increased oxygen free radicals and oxidative stress are the high-risk factors for kidney injury.[8-10] Herget-Rosenthal et al[11] found that urinary cystatin C may reflect the severity of toxicity in non-oliguric ischemic tubular necrosis, and that it is associated with the high mortality rate. Shi et al[12] found that the elevated levels of serum cystatin C were associated with the mortality during the Wenchuan earthquake in Sichuan province, China. In the 376 patients admitted to the Cardiac Surgery ICU, Didier et al[13] found that serum cystatin C was an independent risk factor for hospital mortality.
Logistic regression analysis in the present study showed that organ failure ≥2, oliguria, and cystatin C>1.3 mg/ L+APACHE II>15 were associated with the mortality of AKI patients. This study also demonstrated that the level of cystatin C was higher in the death group than in the survival group and the level of serum cystatin C was associated with the mortality. This finding was consistent with the results reported elsewhere.[14,15] Yet whether the increased level of cystatin C was an independent risk factor for death, researchers have their different opinions. Ahlstrom et al[15] found that APACHE II was an independent risk factor for death, whereas cystatin C was not. In our study, APACHE II score>15+cystatin C>1.3 mg/L and organ failure ≥ 2 were the independent factors (P<0.05). The severity of patients with AKI at the time of admission to ICU, the distribution and severity of dysfunction organs, and treatment may affect the prediction of the mortality.
In conclusion, cystatin C>1.3 mg/L+APACHE II>15 can be used to predict clinical outcomes of patients with AKI.
Footnotes
Funding: None.
Ethical approval: Not needed.
Conflicts of interest: No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
Contributors: Shi HP wrote the first draft. All authors contributed to the design and interpretation of the study and to further drafts.
REFERENCES
- 1.Gallego N, Pérez-Caballero C, Gallego A, Estepa R, Liãno F, Ortuño J. Prognosis of patients with acute renal failure without cardiopathy. Arch Dis Child. 2001;84:258–260. doi: 10.1136/adc.84.3.258. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lins RL, Elseviers M, Daelemans R, Zachée P, Gheuens E, Lens S, et al. Prognostic value of a new scoring system forhospital mortality in acute renal failure. Clin Nephrol. 2000;53:10–17. [PubMed] [Google Scholar]
- 3.Wamoch DG. Towards definition and classification of acute kidney injury. J Am Soc Nephrol. 2005;16:3149–3150. doi: 10.1681/ASN.2005090934. [DOI] [PubMed] [Google Scholar]
- 4.Akcan-Arikan A, Zappitelli M, Loftis LL. Modified RIFLE criteria in critically ill children with acute kidney injury. Kidney Int. 2007;71:1028–1035. doi: 10.1038/sj.ki.5002231. [DOI] [PubMed] [Google Scholar]
- 5.D’Intini V, Ronco C, Bonello M, Bellomo R. Renal replacement therapy in acute renal failure. Best Pract Res Clin Anaesthesiol. 2004;18:145–157. doi: 10.1016/j.bpa.2003.09.004. [DOI] [PubMed] [Google Scholar]
- 6.Metcalfe W, Simpson M, Khan IH, Prescott GJ, Simpson K, Smith WC, et al. Acute renal faliure requiring renal replacement therapy: incidence and outcome. QJM. 2002;95:579–583. doi: 10.1093/qjmed/95.9.579. [DOI] [PubMed] [Google Scholar]
- 7.Liu HB, Cheng W, Wang HM. Analysis on prognostic with CRRT in different stages of acute kidney injury in patients with MODS. J Blood Purification. 2007;6:587–589. [Google Scholar]
- 8.Chen JX, Hu Y, Lin L. Acute renal failure and oxidative damage. Chin J Emerg Med. 2006;15:629–632. [Google Scholar]
- 9.Xie CX, Zhong XU. Clinical analysis in hospital-acquired acute renal failure. Chin J Integrated Trad Western Nephrol. 2007;8:290. [Google Scholar]
- 10.Peng YQ, Liang QL, Shi W. Clinical character istics and outcome evaluation of acute renal failure in critically ill patients in ICU. Chin J Pract Inter Med. 2007;27:1753–1755. [Google Scholar]
- 11.Herget-Rosenthal S, Pietruck F, Volbracht L, Philipp T. Kribben Serum cystatin C-a superior marker of rap idly reduced glomerular filtration after uninephrectomy in kidney donors compared to creatinine. Clin Nephrol. 2005;64:41–46. doi: 10.5414/cnp64041. [DOI] [PubMed] [Google Scholar]
- 12.Shi B, Yang TF. Crush syndrome caused by earthquake in acute renal injury. Chin J Emerg Med. 2009;18:640–644. [Google Scholar]
- 13.Lambermont B, D’Orio V. Cystatin C blood level as a risk factor for death after heart surgery. Eur Heart J. 2007;28:1848–1853. doi: 10.1093/eurheartj/ehm432. [DOI] [PubMed] [Google Scholar]
- 14.Lassus J, Harjola VP, Sund R, Siirilä-Waris K, Melin J, Peuhkurinen K, et al. Prognostic value of cystatin C in acute heart failure in relation to other markers of renal function and NT-proBNP. Eur Heart J. 2007;28:1841–1847. doi: 10.1093/eurheartj/ehl507. [DOI] [PubMed] [Google Scholar]
- 15.Balík M, Jabor A, Waldauf P, Kolár M, Pavlisová M, Brest’an D, et al. Cystatin C as a marker of residual renal function during continuous hemodiafiltration. Kidney Blood Press Res. 2005;28:14–19. doi: 10.1159/000080936. [DOI] [PubMed] [Google Scholar]