

Abstract
BACKGROUND:
With the development of internal fixation materials, simple operation with internal fixation has become a tendency. Ni-Ti shape memory alloy embracing fixator has such advantages as slight injury, easy operation, security, reliable fixation, and better histocompatibility. The present study was to explore curative effect and postoperative results of Ti-Ni shape memory alloy embracing fixator in patients with multiple fractured ribs and flail chest.
METHODS:
The curative effect and long-term follow-up results were observed after internal fixation with a shape memory alloy embracing fixator in patients with multiple fractured ribs and flail chest from January 2006 to December 2009.
RESULTS:
All patients were cured with an average hospital stay of 10.31±3.14 days. Post-operative pain was less severe than preoperative pain (P=0.02). The rate of postoperative complications such as atelectasis, pulmonary infection, etc was 17.65%. There were fewer long-term complications and less influence on daily work and life.
CONCLUSIONS:
It is practical to perform an operation for fracture of multiple ribs using a Ti-Ni shape memory alloy embracing fixator. The fixator, which is less traumatic, simple, safe, and reliable, has a good-histocompatibility and fewer postoperative complications.
KEY WORDS: Multiple fractured ribs, Flail chest, Internal fixation, Postoperative evaluation
INTRODUCTION
Rib fracture is the most common disease in chest trauma, which accounts for 55%.[1] Flail chest caused by rib fractures in different places is one of the six death causes in the early stage of chest trauma,[2] and the mortality of flail chest with lung amalgamation reaches up to 42%.[3,4] With the development of internal fixation materials, simple operation for internal fixation has become a tendency.[5,6] Ni-Ti shape memory alloy embracing fixator has such advantages as slight trauma, easy operation, security, reliable fixation, and better histocompatibility. From January 2006 to December 2009 we treated 17 patients with multiple fractured ribs or flail chest at our hospital.
METHODS
Patients
In this series, 12 patients were male and 5 female; their average age was 42±15.4 years (range, 21 to 65 years). Rib fracture (range, 3 to 11) was found in 5 patients and flail chest in 6 patients. The causes of injury were traffic accidents in 13 patients, falls from heights in 2, crush accidents in 2, associated chest injuries in 11 (lung amalgamation in 6, hemopneumothorax and (or) pneumatothorax in 10). All patients were diagnosed by X-ray or CT thin slice scan.
Treatment
All patients received operative treatment at the thoracic surgery department of our hospital within 24 hours. For internal fixation an oblique or straight sub-axillary incision in 8 to 12 cm length was made correspondingly according to rib fracture positions and numbers. Muscles were separated on the basis of chest muscle direction in multipoints, while exposing fragments of rib fractured bone, uncovering the periosteum 2 to 3 cm from the two ends for anatomical reduction. Subsequently the corresponding size of Ti-Ni shape memory alloy embracing fixator was selected and put into steriled ice water. After the amplectant arms were opened slowly, the fixator was quickly put into the fragments of rib fractured bone.
After operation, antibiotics were commonly used in the preoperative period to strengthen the lung management and prevent from complications. A thoracic catheter was removed according to chest X-ray and thoracic drainage.
Observational indexes
Subjective sensation of pain
Visual Analogue Scales[7] (VASs) (0: without pain, 10: the most severe pain) were recorded on the preoperative day, 1st day, and 7th day, and the 1st, 3rd, 6th, and 12th months after operation.
Long-term follow-up
Telephone was used in follow-up but some patients were followed up by clinical service or outpatient visit after operation. The time of follow-up was 3 to 12 months after operation. The items of follow-up included life quality indexes such as mental status ,VAS, chest discomfort, sleep quality, working and living conditions.
Statistical analysis
Income measures were dealt with statistics SPSS13.0 software package. Enumeration count data were expressed by n, and measurement data were expressed by means of standard deviation and analyzed with analysis of variance or Student’s t test.
RESULTS
In this series, all of the 17 patients were cured by placement of a drainage tube for an average of 4.3±1.4 days. Their median length of hospital stay was 10. 31±3.14 days. Postoperative pulmonary infection and atelectasis occurred in 3 and 2 patients respectively with an incidence of 17.65%. The condition of rib contraposition and resetting was so good that it held the chest integral without thoracocyllosis, obstacle of the chest, shoulder and upper limbs (Figure 1). Their postoperative VASs were 7.4±1.7 at the first day and 5.6±1.8 at the first week. Compared with preoperative VASs (7.7±2.1), the postoperative ones were significantly different (P=0.03) (Table 1).
Figure 1.
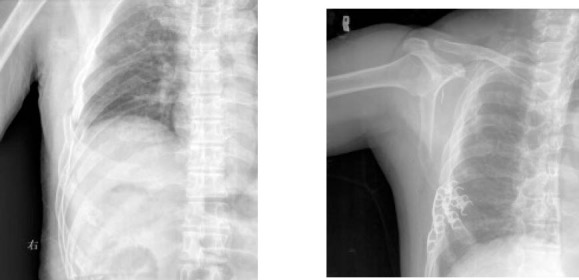
Perioperative X-ray of internal fixation with a Ti-Ni shape memory alloy embracing fixator
Table 1.
Comparison of VASs
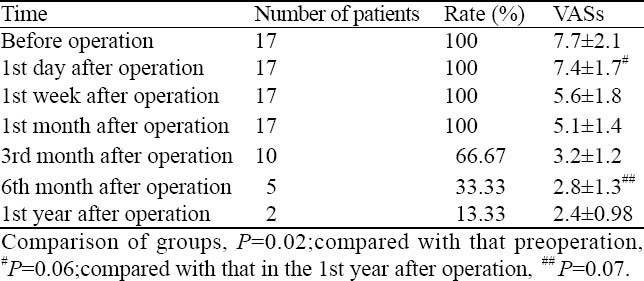
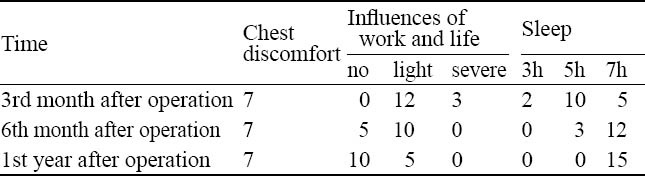
All but two patients were followed up, and ten experienced chest pain of different degree at night after operation in three months. Five patients experienced mild pain after operation within 6 months and 2 patients had mild pain after operation in the twelfth month. VASs showed a downward tendency, but there was no significant difference between them nor difference between the sixth month and the twelfth month (P=0.07). Seven patients presented with sensation of foreign body in the chest. With the relief of pain, their sleep quality gradually improved; all patients could sleep 7 hours in the twelfth month, and had effect on their routine work (Table 2).
Table 2.
Results of long-term follow-up
DISCUSSION
Multiple rib fractures and flail chest constitute one of the severe chest traumas. Conservative treatment easily leads to thoracic deformity, long-term severe pain, respiratory complications, and delayed pneumothorax. But there is much controversial whether it is necessary to take an active fixation or not. Balci et al[6,8] found that internal fixation was superior to non-internal fixation in ICU stay, mechanical ventilation, pulmonary infection, sepsis, airway injury, mortality, hospitalization and other indicators of patients. From our practice we think internal fixation should be taken actively since it is beneficial to early recovery of the patient. Indications of this fixation include: (1) exploratory thoracotomy; (2) flail chest; (3) obvious thoracic abnormalities; and (4) severe pain or strong surgical demanding. The first three are direct indications for surgery, which is similar to the report by Nirula et al.[9] In our 17 patients, 6 had flail chest, 6 had multiple rib fractures without significant flail chest but thoracic deformity, and 5 had other causes of chest surgery simultaneously. In the patient with root fracture ≤ 3 without obvious dislocation, displacement, no significant pain or thoracic deformity, surgery should not be performed for internal fixation.
Preoperative X-ray is important for surgical incision. According to the position and number of rib fractures appropriate oblique or vertical incision can be made. In our series, one patient was placed seven Ni-Ti memory alloy devices for internal fixation of 3-5 ribs, which are under the shoulder where blade block is difficult to expose. Claws of an embracing fixator should be distracted to the maximum before placing, while adjusting the major axis angle according to the curvature of the ribs, which is good for device insertion. Ni-Ti shape memory alloy devices are not removed usually.[10] Three patients in our series required surgery for removal of foreign body. A small incision was made, and after soaking in disinfected ice water immersion for 1-2 minutes, the cock clamp arm would be surrounded by one side. The operation is simple and short, and the appropriate operative time is one year after internal fixation.
Synthetic resin of internal fixation has absorbable characteristics, without second surgery for removal, but fixed insertion place is bone marrow cavity which may induce rib infection, insufficient thickness of cortical bone defects and poor fixity.[11] Ni-Ti memory alloy devices are more advantageous than other types of internal fixation materials. Patients in our series received surgery within 24 hours after injury. Stable and reliable anatomic reduction after fractures eliminated abnormal stimulation to fracture fragments and alleviated the pain effectively (P<0.05). At the same time, the operation shortened extubation time, helped the patient to spit sputum effectively, reduced the incidence rates of ARDS and pulmonary complications, and restored the integrity and stability of the thorax.[12] Ni-Ti shape memory alloy devices fixation has less long-term complications and thoracic deformity. Chest pain and sensation of foreign body are the main complaints of discomfort, and the pain can be alleviated obviously within 6 months after surgery (13.33%). But there is long-term chest discomfort (46.67%), this is why our 3 patients required the removal of internal fixation.
In short, Ni-Ti memory alloy devices fixation is good for the recovery of patients with multiple rib fractures and flail chest. It is an advanced and practical treatment method.
Footnotes
Funding: None.
Ethical approval: Not needed.
Conflicts of interest: The authors have no competing interests.
Contributors: Yang Y proposed and wrote the paper. All authors read and approved the final version.
REFERENCES
- 1.Oswanski MF, Jolly S, Lauer SK, Dressel R, Stombaugh HA. Perils of rib fractures. Am Surg. 2008;74:310–314. doi: 10.1177/000313480807400406. [DOI] [PubMed] [Google Scholar]
- 2.Yamamoto L, Schroeder C, Morley D, Beliveau C. Thoracic trauma: the deadly dozen. Crit Care Nurs Q. 2005;28:22–40. doi: 10.1097/00002727-200501000-00004. [DOI] [PubMed] [Google Scholar]
- 3.3Pettiford BL, Luketich JD, Landreneau RJ. The management of flail chest. Thorac Surg Clin. 2007;17:25–33. doi: 10.1016/j.thorsurg.2007.02.005. [DOI] [PubMed] [Google Scholar]
- 4.Bastos R, Calhoon JH, Baisden CE. Flail chestand pulmonary contusion. Semin Thorac Cardiovasc Surg. 2008;20:39–45. doi: 10.1053/j.semtcvs.2008.01.004. [DOI] [PubMed] [Google Scholar]
- 5.Richardson JD, Franklin GA, Heffley S, Seligson D. Operative fix-ation of chestwall fractures: an underused procedure. Am Surg. 2007;73:591–597. [PubMed] [Google Scholar]
- 6.Balci AE, Eren S, Cakir O, Eren MN. Open fixation in flailchest: review of 64 patients. Asian Cardiovasc Thorac Ann. 2004;12:11–15. doi: 10.1177/021849230401200104. [DOI] [PubMed] [Google Scholar]
- 7.Curtiss CP. Challenges in pain assessment in cognitively intact and cognitively impaired older adults with cancer. Oncol Nurs Forum. 2010;37:S7–16. doi: 10.1188/10.ONF.S1.7-16. [DOI] [PubMed] [Google Scholar]
- 8.Zhang S, Wang P, Li H, Peng A, Zhao C, Li Z. Treatment of fractures of proximal radius with Ni-Ti shape memory alloy embracing. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi. 2006;20:272–275. [PubMed] [Google Scholar]
- 9.Nirula R, Diaz JJ, Jr, Trunkey DD, Mayberry JC. Rib fracture repair:indications, technical issues, and future directions. World J Surg. 2009;33:14–22. doi: 10.1007/s00268-008-9770-y. [DOI] [PubMed] [Google Scholar]
- 10.Pal Singh A, Pal Singh A, Vaishya R. Open reduction and internal fixation combined with hinged elbow fixator in capitellum and trochlea fractures. Acta Orthop. 2010;81:518. doi: 10.3109/17453674.2010.504612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Li Q, Xia YY, Tang JC, Wang RY, Bei CY, Zeng Y. In vitro and in vivo biocompatibility investigation of diamond-like carbon coated nickel-titanium shape memory alloy. Artif Cells Blood Substit Immobil Biotechnol. 2010 Jul;:23. doi: 10.3109/10731199.2010.502880. [DOI] [PubMed] [Google Scholar]
- 12.Zhang S, Wang P, Li H, Peng A, Zhao C, Li Z. Treatment of fractures ofproximal radiuswith Ni-Ti shape memory alloy embracing. Zhongguo Xiu Fu Chong JianWaiKe Za Zhi. 2006;20:272–275. [PubMed] [Google Scholar]