

Abstract
BACKGROUND:
Basic life support (BLS), a key component of the chain of survival decreases the arrest – cardiopulmonary resuscitation interval and increases the rate of hospital discharge. The study aimed to explore the knowledge of and attitude towards basic life support (BLS) among medical/paramedical professionals.
METHODS:
An observational study was conducted by assessing response to self prepared questionnaire consisting of the demographic information of the medical/paramedical staff, their personnel experience/attitude and knowledge of BLS based on the 2005 BLS Guidelines of European Resuscitation Council.
RESULTS:
After excluding incomplete questionnaires, the data from 121 responders (27 clinical faculty members, 21 dental and basic sciences faculty members, 29 house officers and 44 nurses and health assistants) were analyzed. Only 9 (7.4%) of the 121 responders answered ≥11, 53 (43%) answered 7-10, and 58 (48%) answered <7 of 15 questions correctly. The clinical faculty members, house officers and nurses/HA had a mean score of 7.4±3.15, 7.37±2.02 and 6.63±2.16 respectively, while dental/basic sciences faculty members attained a least mean score of 4.52 ±2.13 (P<0.001). Those who had received cardiopulmonary resuscitation (CPR) training within 5 years obtained a highest mean score of 8.62±2.49, whereas those who had the training more than 5 years back or no training obtained a mean score of 5.54±2.38 and 6.1±2.29 respectively (P=0.001). Those who were involved in resuscitation frequently had a higher median score of 8 in comparison to those who were seldom involved or not involved at all (P<0.001).
CONCLUSIONS:
The average health personnel in our hospital lack adequate knowledge in CPR/BLS. Training and experience can enhance knowledge of CPR of these personnel. Thus standard of CPR/BLS training and assessment are recommended at our hospital.
KEY WORDS: Basic life support (BLS), Cardiopulmonary resuscitation (CPR), Training, Knowledge, Attitude
INTRODUCTION
Survival after cardiopulmonary arrest is usually low and depends on early intervention, quality of cardiopulmonary resuscitation (CPR) and time to defibrillation.[1-4] Basic life support (BLS), a key component of the chain of survival decreases the arrest – CPR interval and increases the rate of hospital discharge.[3]
Individuals in the community at least the health care professionals should know how to perform BLS as they encounter such situation very often.[5] Health care professionals are expected to be competent to resuscitate from their first posting. In the United States, BLS training has been recommended for all health care professionals since 1966[6] especially for those who are involved in resuscitation.[7] Demand for courses of BLS is ever-increasing worldwide. However, in developing countries like Nepal, there is still no standard, and resuscitation training is not routine. Up to the present, few reports have addressed the current level of awareness and knowledge in this area among the health care professionals in Nepal.[8,9]
In recent years, several publications have highlighted the deficiencies in CPR quality, both out-of-hospital and in-hospital, which have partly been addressed in the newest BLS guidelines.[10,11] As a preliminary step, this study aimed to explore the level of knowledge and attitude towards BLS among medical/paramedical staffs in Kist Medical College Hospital, thereby to guide future planning of BLS program in this hospital. After this study, we hope that all aspects of BLS training for medical personnel will be improved and standardized.
METHODS
Study subjects
The medical/paramedical staffs who were on duty in different departments of the hospital in 2 weeks sample collection period. Those who were on leave, unwilling to participate in and incomplete questionnaires were excluded from the study.
Study tools
A questionnaire was prepared by the authors encompassing 3 main domains:
-
1.
Demography and professional qualification of the participants;
-
2.
Experience in and attitude of the participants to BLS/CPR (6 open-ended and MCQs);
-
3.
Theoretical and practical knowledge of the participants related to BLS (set of self-prepared 15 MCQs with 5 options based on 2005 European Resuscitation Council BLS Guidelines.
The validity of the questionnaire was determined by piloting in other hospitals before it was finalized for the study. After appropriate changes made in the questionnaire after the piloting, ethical approval was obtained.
Ethical approval
The study was approved by the hospital ethical review committee and written informed consent was obtained before a respondent completed the questionnaire. The questionnaire didn’t contain the name of the participants, thus the confidentiality of the participants was maintained.
Data collection
The authors went to the respective departments and distributed the questionnaire to the subjects and collected the questionnaires after adequate time.
Data analysis
The collected data were calculated with Microsoft Excel and then statistical analysis was made by statistical package for social science (SPSS) 17 version. Descriptive and frequency analysis was made for counts, percentage and means or medians as appropriate to provide the overall picture of the responses. Mean score was compared for duration of clinical experience, professional qualification and previous training obtained by the participants by using ANOVA with Bonferroni’s test. The Kruskal Wallis test was used to compare the median score in reference to the previous involvement of participants in resuscitation. P values <0.05 were considered statistically significant.
RESULTS
Among 150 questionnaires which were distributed to the participants, 127 returned with a response rate of 84%. Among the 127 questionnaires, 6 incomplete ones were excluded from the study.
Of 121 responders, 27 were clinical faculty members, 21 faculty members of dental and basic sciences, 29 house officers, and 44 nurses and health assistants. The age of the participants (n=116) ranged from 18 to 61 years (mean of 30±8 years). Among all the participants, 68 (56%) were male and 53 (44%) were female. A larger proportion of females comprised nurses/HA group (36 of 44) and dental / basic sciences faculty members (13 of 21).
The duration of clinical experience was divided into <1 year, 1-5 years, 5-10 years and >10 years which comprised of 20 (16.5%), 55 (45.5%), 18 (14.8%) and 15 (12.2%) participants respectively. When the participants were inquired about any resuscitation training after graduation, 83 (69%) of them had had no training at all, and 27 (22%) had received some training within the last 5 years. Twenty-eight (23%) of the participants had not been involved in patient resuscitation after graduation, but 45(37%) have been involved rarely and 48 (40%) frequently.
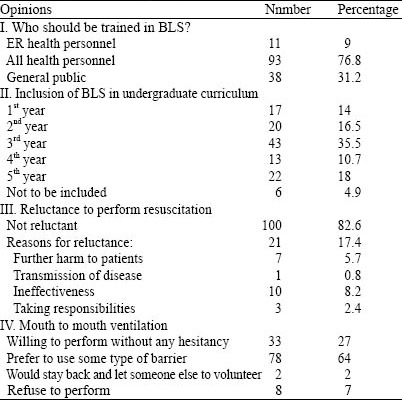
The attitude of the participants towards BLS is summarized in Table 1. Most (95 %) of the participants thought that BLS should be included in the undergraduate curriculum, 82.6%(100) of the participants were not reluctant to perform CPR, 64% (78) preferred to use some type of barrier for mouth to mouth ventilation, and 7% (8) refused to perform it.
Table 1.
Opinions of the participants
The number and percentage of knowledge score of the participants are listed in Table 2. The percentage of correct answer varied from 19% to 96.7%. The mean score for the participants was 6.6 with a median score of 7 (ranged 1 to 14 for15 questions). Nine (7.4%) of 121 participants had a score of ≥11, 53 (43%) 7-10, and 58 (48%) <7.
Table 2.
BLS knowledge of the participants
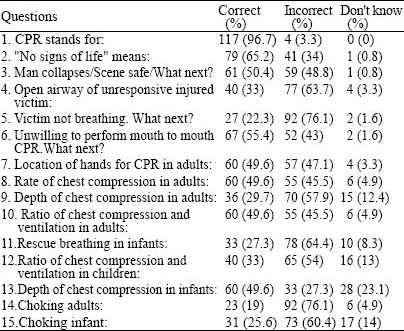
Almost all of the responders (96.7%) knew the abbreviation of CPR. Most of them (65%) could recognize “no signs of life”. The two questions that just about half of the responders could answer were: “What is the next step of BLS when you encounter an unresponsive victim?” and “What is the best option of resuscitation if you are not willing to perform mouth to mouth ventilation?”(50.4%, 55.4% respectively). When asked about the recommended maneuver for opening the airway of the injured victim, only 40% of them answered jaw thrust with immobilization of the cervical spine, whereas 57% pointed out head tilt-chin lift maneuver which should be avoided in suspected victims with C-spine injury.
As to questions on chest compression in adults, nearly half of the participants could identify that the right location of the hands for chest compression is the center of the chest between two nipples, the compression rate is 100/min, and the chest compression to ventilation ratio is 30:2. However, only 30% of the participants knew that the recommended depth of chest compression in an adult is 1.5-2 inches. About 73% of the responders failed to select mouth to mouth and nose technique as the rescue breathing for infants, 67% were unable to identify the chest compression to ventilation ratio in infants and children, nevertheless 50% of them knew that the depth of chest compression in an infant is one third of the chest. Likewise, wrong answers to the questions concerning adult and pediatric choking were found (81%, 74% respectively).
The scores were compared according to the different characteristics of the participants (Tables 3 and 4), showing no association between the knowledge scores of the participants and the duration of their clinical work (P=0.91). The mean knowledge score was significantly different in staffs of different categories (clinical vs. dental/basic faculty members, P<0.001; dental/basic faculty members vs. house officers, P<0.001; dental/basic faculty members vs. nurses/HA, P=0.007). The mean knowledge score was significantly higher in those who had received CPR training within 5 years than in those who had training more than 5 years ago and those had no training at all (no training vs. training<5 years, P<0.001; training<5 years vs. training>5 years P=0.001). Those participants who were involved in resuscitation frequently had a significantly higher median score than those who were seldom involved or not involved at all (P=<0.001).
Table 3.
Comparison of the scores in relation to the different characteristics of the participants
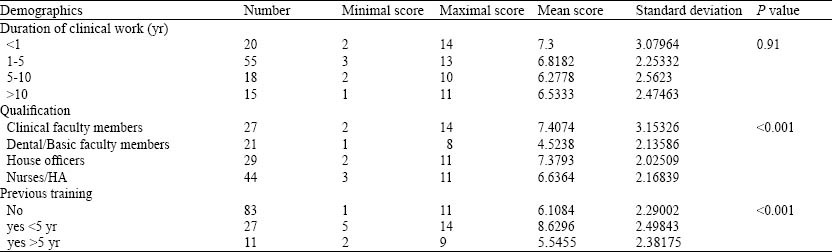
Table 4.
Comparison of resuscitation experience and scores

DISCUSSION
Health professionals should have sound CPR/ BLS knowledge and skills, but there is a major problem with retention of skills and outdated information.[12,13] This study was to explore the present knowledge of medical/paramedical staffs of our hospital about BLS/CPR so as to make a plan for BLS training.
This study revealed that the participants had inadequate knowledge on BLS. Although 52% of the participants answered ≥7 of the 15 questions, only 7.4% (n=9) of them could answer 75% of the questions correctly. Other studies also demonstrated inadequate CPR knowledge in health care professionals.[14-17] In this study, only one question was correctly answered by 96.7% of the participants, whereas 11 questions were correctly answered by <50% of them. Another key area this study has identified is the positive attitude of the participants towards BLS and their readiness to perform it despite the paucity in their knowledge. Of the participants, 82.6% were not reluctant to perform CPR when needed, and 21 (17.4%) were reluctant to perform resuscitation. The most commonly cited anxiety for the performance of resuscitation was fear of being ineffective (8.2 %) which was followed by fear of further harm to the victim (5.7%).
The clinical faculty members, house officers and nurses/HA had the similar mean score of 7.4±3.15, 7.37±2.02 and 6.6±2.16 respectively, whereas dental/basic faculty members had the least mean score of 4.52±2.13. Clinical faculty members were expected to have a higher score as demonstrated in other studies.[14] CPR might not be part of some postgraduate curricula which could have lowered the overall knowledge of clinical faculty members.
CPR training significantly influenced the BLS knowledge of the participants. Those who had received some CPR training within 5 years obtained the highest mean score of 8.62±2.49, whereas those who had training >5 years back and without training obtained mean score of 5.54±2.38 and 6.1±2.29 respectively. This later important observation must be noted and is of great clinical significance. Other studies also concluded that that the knowledge of trained personnel was better than those of untrained ones.[18] Chaudhari A et al[19] demonstrated improvement of knowledge and skill of CPR following a BLS training. The skills of CPR are difficult to teach and once taught difficult to retain.[20,21] It is also a fact that after graduation, training of resuscitation skills is difficult due to busy schedules and lack of teachers and resources in developing countries like ours. Federico et al[13] concluded the significant decay of ALS skills 6 months post-ALS recorded among anesthesiologist in their study. Moreover, as the guidelines are updated and revised from time to time, the need of refreshers training cannot be ignored to correct the poor technique and to ensure changes are addressed. As stated by Cooper et al[5] there was significant improvement in knowledge and skills of the people who have taken BLS course 6 month ago after taking a short ILS course.Therefore above references and our findings also recommend periodical reinforcement by such refreshers trainings to attain adequate CPR skills and to maintain continued competency in the technique.
Those who were involved in resuscitation frequently secured significantly higher median score (8) in comparison to those who were seldom involved and not involved at all. Elif et al[15] and Mohamed et al[22] also observed that previous experience in real life resuscitation increased the incidence of correct answers.This demonstrates the impact of previous experience on the retention of knowledge.
In conclusion, this study has revealed a critical issue that the average health personnel in our centre lack adequate knowledge in CPR/BLS which should be addressed promptly. Since prior CPR training and clinical exposure influence the retention of knowledge there is need for all health care professionals to have some standard of CPR/BLS training and assessment. In conclusion, we recommend that CPR/BLS should be a core competency across all health care professional programs.
ACKNOWLEDGEMENTS
The authors gratefully acknowledge Mrs Amita Pradhan, Associate professor of community medicine department for the guidance in statistical analysis. We would also like to express our gratitude to the staff of the Kist Medical College Hospital for the contribution to the data collection and the study.
Footnotes
Funding: None.
Ethical approval: The study was approved by the hospital ethical review committee and written informed consent was obtained before a respondent completed the questionnaire.
Conflicts of interest: The authors declare that there is no conflict of interest.
Contributors: Shrestha R wrote the paper. All authors read, edited and approved the final version of the manuscript.
REFERENCES
- 1.Ritter G, Wolfe RA, Goldstein S, Landis JR, Vasu CM, Acheson A, et al. The effect of by-stander CPR on survival of out-of-hospital cardiac arrest victims. Am Heart J. 1985;110:932–937. doi: 10.1016/0002-8703(85)90187-5. [DOI] [PubMed] [Google Scholar]
- 2.Wenzel V, Lehmkuhl P, Kubilis PS, Idris AH, Pichlmayr I. Poor correlation of mouth-to-mouth ventilation skills after basic life support training and 6 months later. Resuscitation. 1997;35:129–134. doi: 10.1016/s0300-9572(97)00044-0. [DOI] [PubMed] [Google Scholar]
- 3.Wik L, Steen PA, Bircher NG. Quality of bystander cardiopulmonary resuscitation influences outcome after prehospital cardiac arrest. Resuscitation. 1994;28:195–203. doi: 10.1016/0300-9572(94)90064-7. [DOI] [PubMed] [Google Scholar]
- 4.Gwinnutt C, Columb M, Harris R. Outcome after cardiac arrest in adults in UK hospitals: effect of the 1997 guidelines. Resuscitation. 2000;47:125–135. doi: 10.1016/s0300-9572(00)00212-4. [DOI] [PubMed] [Google Scholar]
- 5.Cooper S, Johnston E, Priscott D. Immediate lifesupport training. Impact in a primary care setting? Resuscitation. 2007;72:92–99. doi: 10.1016/j.resuscitation.2006.06.004. [DOI] [PubMed] [Google Scholar]
- 6.Cardiopulmonary resuscitation: statement by the Ad Hoc Committee on Cardiopulmonary Resuscitation of the Division of Medical Sciences, National Academy of Sciences, National Research Council. Cardiopulmonary Resuscitation. JAMA. 1966;198:372–379. [Google Scholar]
- 7.Royal college of anesthetist; 1999. Guidelines for the provision of anaesthetic services. Anesthetic practice in respect of resuscitation. [Google Scholar]
- 8.Parajuli S, Selvaraj V. Knowledge of nurses towards cardiopulmonary resuscitation in a Tertiary care teaching hospital in Nepal. J Clin Diag Res. 2011;5:1585–1588. [Google Scholar]
- 9.Shrestha R. Comparative study on level of knowledge of nursing personnel working in critical/ general ward regarding cardiopulmonary resuscitation in BPKIHS, Dharan, Nepal [Google Scholar]
- 10.Document 2005 International Consensus on Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science with Treatment Recommendations (CoSTR) [PubMed] [Google Scholar]
- 11.Effestol T, Sunde K, Steen PA. Effects of interrupting precordial compressions on the calculated probability of defibrillation success during out-of-hospital cardiac arrest. Circulation. 2002;105:2270–2273. doi: 10.1161/01.cir.0000016362.42586.fe. [DOI] [PubMed] [Google Scholar]
- 12.Chamberlain D, Smith A, Woollard M, Colquhoun M, Handley AJ, Leaves S, et al. Trials of teaching methods on basic life support: comparison of simulated CPR performance after first training and at 6 months, with a note on the value of retraining. Resuscitation. 2002;53:179–187. doi: 10.1016/s0300-9572(02)00025-4. [DOI] [PubMed] [Google Scholar]
- 13.Federico S, Luciano S, Erga L. Retention of CPR performance in anaesthetists. Resuscitation. 2006;68:101–108. doi: 10.1016/j.resuscitation.2005.06.011. [DOI] [PubMed] [Google Scholar]
- 14.Osinaike BB, Aderinto DA, Oyebamiji EO, Dairo MD, Diya KS. Evaluation of knowledge of doctors in Nigerian tertiary hospital about CPR. Nigerian Medical Practitioner. 2007;52:16–18. [Google Scholar]
- 15.Elif AA, Zeynep K. Knowledge of basic life support: a pilot study of the Turkish population by Baskent university in Ankara. Resuscitation. 2003;58:187–192. doi: 10.1016/s0300-9572(03)00126-6. [DOI] [PubMed] [Google Scholar]
- 16.Chandrasekaran S, Kumar S, Bhat SA, Saravanakumar Shabbir PM, Chandrasekaran V. Awareness of basic life support among medical, dental, nursing students and doctors. Indian J Anaesth. 2010;54:121–126. doi: 10.4103/0019-5049.63650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Zaheer H, Haque Z. Awareness about BLS(CPR) among medical students:status and requirements. J Pak Med Assoc. 2009;59:57–59. [PubMed] [Google Scholar]
- 18.Abbas A, Bukhari SI, Ahmed F. Knowledge of first aid and basic life support amongst medical students:a comparison between trained and un-trained students. JPMA. 2011;61:613–616. [PubMed] [Google Scholar]
- 19.Chaudhary A, Parikh H, Dave V. Current scenario: Knowledge of basic Life support in medical college. National J Med Res. 2011;1:80–82. [Google Scholar]
- 20.Christenson J, Nafziger S, Compton S, Vijayaraghavan K, Slater B, Ledingham R, et al. The effect of time on CPR and automated external defibrilator skills in the Public Access Defibrillation Trial. Resuscitation. 2007;74:52–62. doi: 10.1016/j.resuscitation.2006.11.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Sternbach GL, Kiskaddon RT, Fossel M, Eliastam M. The retention of cardiopulmonary resuscitation skills. J Emerg Med. 1984;2:33–36. doi: 10.1016/0736-4679(84)90046-5. [DOI] [PubMed] [Google Scholar]
- 22.Mohamed A, Mohamed N. Cardiopulmonary resuscitation skills of medical professionals. Resuscitation. 1990;20:31–39. doi: 10.1016/0300-9572(90)90084-r. [DOI] [PubMed] [Google Scholar]