

Abstract
BACKGROUND:
Caffeinated energy drinks are widely used worldwide. They are associated with a variety of adverse effects and are of concern to health authorities, yet there is still scarce information about their adverse effects and inadequate awareness among medical personnel.
METHODS:
Case description and discussion of a patient presenting to the emergency room after overdose of energy drinks in combination with 3,4-methylenedioxymethamphetamine (MDMA).
RESULTS:
Despite best medical efforts, the patient died of fatal cardiac arrhythmias. There is a paucity of information about adverse effects of energy drinks.
CONCLUSION:
Although energy drinks are widely used, there is a lack of awareness in the population and medical staff about their hazards.
KEY WORDS: Energy drink, Caffeine, MDMA
INTRODUCTION
Use of caffeinated energy drinks is a growing health concern worldwide.[1,2] There are growing concerns of adverse effects including addiction, neuropsychiatric, cardiac and metabolic adverse effects. We report a young male patient suffering from fatal myocardial infarction due to overdose of energy drink combined with ecstasy. To our knowledge, this is the first report of fatal myocardial infarction that may be related to energy drinks.
Case presentation
A 24-year-old Caucasian man presented to the Emergency Department with a one-hour history of crushing chest pain, nausea, and vomiting. He was brought from a night club, where he works as a doorman. He reported consuming about 20 cans of energy drink (XL) over the previous night, but denied taking any drugs or drinking any alcohol. His medical history included overweight (BMI of about 40), and a mild hypertension for which he denied taking medications. There was no family history of ischemic heart disease.
On arrival, he was anxious, sweating, and tachycardic (110 beats/minute), with blood pressure 90/60 mmHg. Heart sounds were normal on auscultation, and respiratory examination revealed slight basal rales, with no jugular vein distension.
Electrocardiogram (ECG) on admission (Figure 1) showed widespread ST segment elevation confirming acute myocardial infarction. He was given aspirin, oxygen, and morphine, and was preceded to primary percutaneous intervention (PCI). While waiting for the Cath-Lab team, the patient developed a wide complex tachycardia (Figure 2), which was resistant for administration of DC shocks and a bolus of amiodarone. His level of consciousness deteriorated, and he was then intubated. His cardiac rhythm further deteriorated to ventricular fibrillation (Figure 3). Resuscitation according to ACLS protocols was carried out, while a cardiologist inserting a pacemaker. Time for pacemaker placement was 15 minutes. In spite of all the resuscitative efforts, the medical team in place had to announce the patient’s death after more than half and an hour resuscitation, and after a bedside echocardiogram failed to demonstrate any spontaneous cardiac activity.
Figure 1.
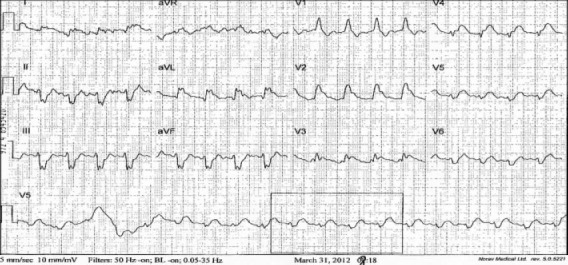
Electrocardiogram (ECG) on admission.
Figure 2.
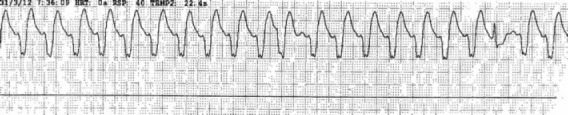
ECG showing a wide complex tachycardia.
Figure 3.
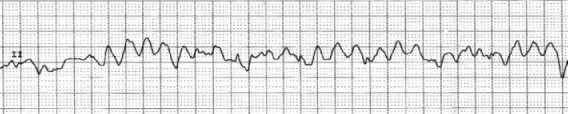
ECG showing ventricular fibrillation.
Because of the rare and dramatic presentation, atypical in young men, a urine sample was sent for toxic screening, and it returned out to be positive for urine specimen showing the presence of 3, 4-methylenedioxymethamphetamine (MDMA). The patient’s family refused the execution of post mortem investigation.
DISCUSSION
The recreational use of commercial energy drinks is a growing habit in most of the world, and there are reports about their adverse effects.[1–4] These drinks contain, among other ingredients, large amounts of caffeine. Though these drinks contain many other ingredients in addition to caffeine, there is little evidence they bare any hazards.[5] Caffeine in high doses is well related to various adverse effects, and though it has a wide therapeutic index, there are many reports of serious toxicities, even death.[6] One study[7] found that one hour after consumption of a caffeine drink containing caffeine (80 mg), taurine (1000 mg), and glucouronolactone (600 mg), there are objective cardiovascular changes characterized by an increase in blood pressure and an increase in platelet aggregation.[7] Physiologic studies[8–9] indicate a reduction of myocardial reserve by caffeine, providing a biological plausibility for the sudden deaths reported in the literature. There are several series in the literature describing the direct link between heavy caffeine intake, mostly in coffee, and myocardial infarctions.[10–11]
Earliest symptoms of acute caffeine poisoning are usually anorexia, tremor, and restlessness, followed by nausea, vomiting, tachycardia, and agitation. With serious intoxication, delirium, seizures, supraventricular and ventricular tachyarrhythmias, hypokalemia, and hyperglycemia may occur. Hypotension is caused by excessive beta-2-mediated vasodilatation and is characterized by a low diastolic pressure and a wide pulse pressure. The lethal oral caffeine dose is considered to be 10 grams. One can of the commercial energy drinks contains 40–200 milligrams of caffeine (about equal to one cup of coffee). The recommended daily caffeine dose for an adult is a maximum of 400 mg.[12] Relying on this figure, the patient in our case drank in a few hours 5 times more than the safe daily dose.
MDMA (3, 4-methylenedioxymethamphetami ne), the other drug of abuse ingested by the patient, is a synthetic phenyl ethylamine derivative structurally related to both amphetamines and mescaline. It is commonly known by the street name “ecstasy”. MDMA is best known for its psychedelic properties and unique effects on mood and intimacy. The increase in popularity of MDMA has been accompanied by an increase in reports of serious complications and death related to its use. [13–16] There are reports on morbidity and mortality due to cardiac effects of MDMA by coronary thrombosis and arrhythmia.[15–18]
In conclusion, though the cardiac hazards of caffeine and MDMA are known, there are no descriptions of their combined effects so far. Moreover, there are no descriptions in the literature of cardiac mortality due to ingestion of energy drinks, though their use (or abuse) is a growing problem worldwide. This may be due to lack of awareness to this problem.
Footnotes
Funding: None.
Ethical approval: This study was approved by the Ethical Committee of Rambam Medical Center, Haifa, Israel.
Conflicts of interest: There is no conflict of interest in this study.
Contributors: Israelit SH proposed the study, and wrote the first draft. All authors read and approved the final version
REFERENCES
- 1.Reissig CJ, Strain EC, Griffiths RR. Caffeinated energy drinks – a growing problem. Drug Alcohol Depend. 2009;99:1–10. doi: 10.1016/j.drugalcdep.2008.08.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Higgins JP, Tuttle TD, Higgins CL. Energy beverages: content and safety. Mayo Clin Proc. 2010;85:1033–1041. doi: 10.4065/mcp.2010.0381. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Petit A, Levy F, Lejoyeux M, Reynaud M, Karila L. Energy drinks: an unknown risk. Rev Prat. 2012;62:673–678. [PubMed] [Google Scholar]
- 4.Wolk BJ, Ganetsky M, Babu KM. Toxicity of energy drinks. Curr Opin Pediatr. 2012;24:243–251. doi: 10.1097/MOP.0b013e3283506827. [DOI] [PubMed] [Google Scholar]
- 5.Clauson KA, Shields KM, McQueen CE, Persad N. Safety issues associated with commercially available energy drinks. J Am Pharm Assoc. 2008;48:e55–63. doi: 10.1331/JAPhA.2008.07055. [DOI] [PubMed] [Google Scholar]
- 6.Tintinalli JE, Stapczynski JS, Cline DM, Cydulka RK, Meckler GD. 7th Edition. McGraw Hill Companies; 2011. Tintinalli's Emergency Medicine. [Google Scholar]
- 7.Worthley MI, Prabhu A, De Sciscio P, Schultz C, Sanders P, Willouqhby SR. Detrimental Effects of Energy Drink Consumption on Platelet and Endothelial Function. Am J Med. 2010;123:184–187. doi: 10.1016/j.amjmed.2009.09.013. [DOI] [PubMed] [Google Scholar]
- 8.Böttcher M, Czernin J, Sun KT, Phelps ME, Schelbert HR. Effect of caffeine on myocardial blood flow at rest and during pharmacological vasodilation. J Nucl Med. 1995;36:2016–2021. [PubMed] [Google Scholar]
- 9.Namdar M, Koepfli P, Grathwohl R, Siegrist PT, Klainguti M, Schepis T, et al. Caffeine decreases exercise-induced myocardial flow reserve. J Am Coll Cardiol. 2006;47:405–410. doi: 10.1016/j.jacc.2005.08.064. [DOI] [PubMed] [Google Scholar]
- 10.Happonen P, Voutilainen S, Salonen JT. Coffee drinking is dose-dependently related to the risk of acute coronary. Events in middle-aged men. J Nutr. 2004;134:2381–2386. doi: 10.1093/jn/134.9.2381. [DOI] [PubMed] [Google Scholar]
- 11.Tavani A, Bertuzzi M, Negri E, Sorbara L, La Vecchia C. Alcohol, smoking, coffee and risk of non-fatal acute myocardial infarction in Italy. Eur J Epidemiol. 2001;17:1131–1137. doi: 10.1023/a:1021276932160. [DOI] [PubMed] [Google Scholar]
- 12.Macdonald N, Hamilton R, Malloy P, Moride Y, Shearer J. Report by the Expert Panel on Caffeinated Energy Drinks. 2010 Nov 10; [Google Scholar]
- 13.Pilgrim JL, Gerostamoulos D, Woodford N, Drummer OH. Serotonin toxicity involving MDMA (ecstasy) and moclobemide. Forensic Sci Int. 2012;215:184–188. doi: 10.1016/j.forsciint.2011.04.008. [DOI] [PubMed] [Google Scholar]
- 14.Schifano F. A bitter pill. Overview of ecstasy (MDMA, MDA) related fatalities. Psychopharmacology (Berl) 2004;173:242–248. doi: 10.1007/s00213-003-1730-5. [DOI] [PubMed] [Google Scholar]
- 15.Vuori E, Henry JA, Ojanperä I, Nieminen R, Savolainen T, Wahlsten P, Jäntti M. Death following ingestion of MDMA (ecstasy) and moclobemide. Addiction. 2003;98:365–368. doi: 10.1046/j.1360-0443.2003.00292.x. [DOI] [PubMed] [Google Scholar]
- 16.Sano R, Hasuike T, Nakano M, Kominato Y, Itoh H. A fatal case of myocardial damage due to misuse of the “designer drug” MDMA. Leg Med (Tokyo) 2009;11:294–297. doi: 10.1016/j.legalmed.2009.09.003. [DOI] [PubMed] [Google Scholar]
- 17.Lai TI, Hwang JJ, Fang CC, Chen WJ. Methylene 3, 4 Dioxymethamphetamine– Induced Acute Myocardial Infarction. Ann Emerg Med. 2003;42:759–762. doi: 10.1016/s0196-0644(03)00511-0. [DOI] [PubMed] [Google Scholar]
- 18.Bassi S, Rittoo D. Ecstacy and chest pain due to coronary artery spasm. Int J Cardiol. 2005;99:485–487. doi: 10.1016/j.ijcard.2003.11.057. [DOI] [PubMed] [Google Scholar]