

Abstract
BACKGROUND:
This study aimed to determine the necessity of pregnancy test in women of reproductive age admitted to emergency department (ED) in routine practice.
METHODS:
We retrospectively reviewed the records of patients who presented to the ED between January 1, 2006 and December 31, 2010 and received a pregnancy test.
RESULTS:
The median age of 1 586 patients enrolled into the study was 27 years. Of these patients, 19.55% had a positive result of pregnancy test. The most common complaint at admission was abdominal pain in 60.15% of the patients, and pregnancy test was prescribed. 15.83% of the patients with abdominal pain had a positive result of pregnancy test. Of the patients, 30.64% had nausea-vomiting at admission, and 11.52% had a positive result of pregnancy test. When other complaints were considered, the most commonly observed complaints were non-specific symptoms such as dizziness, malaise and respiratory problems. Of the patients, 70.93% were not remembering the date of last menstruation, and 9.51% showed a positive result of pregnancy test. Urinary tract infection (UTI) was commonly diagnosed with an incidence of 17.65%, which was followed by non-specific abdominal pain (NSAP) (16.77%) and gastrointestinal disorders such as gastritis and peptic ulcer (6.87%). Of the patients, 88.40% were discharged from ED, and 11.60% were hospitalized.
CONCLUSION:
Pregnancy test should be given to women of reproductive age as a routine practice in ED in developing countries like Turkey.
KEY WORDS: Female, Emergency Medical Services, Pregnancy, Reproduction
INTRODUCTION
Women of reproductive age often attend the emergency department (ED) for pregnancy conditions such as abdominal pain, vaginal bleeding, syncope or shock.[1] To know the pregnancy status of a woman presented to the ED is an important component of diagnosis and treatment.[2] During the pregnancy, many drugs are contraindicated and diagnostic imaging should be avoided as much as possible.[1] As the exclusion of pregnancy based on menstrual history alone is not reliable, it is necessary to take a pregnancy test, a precise, non-invasive and cost-effective method in the ED.[1,3] Reports[2–5] present conflicting results about patient history in detecting pregnancy in the ED. This study aimed to examine the need of pregnancy test for women of reproductive age presented to our ED.
METHODS
This study was conducted in the ED of Faculty of Medicine, Uludag University, which has an annual visit rate of approximately 75 000. By searching the hospital database, we retrospectively reviewed the records of the patients who had a pregnancy test between January 1, 2006 and December 31, 2010. Patients below the age of 18 years were excluded from the study because they were admitted to the pediatric ED of our hospital.
Pregnancy test included the measurement of serum ß-HCG, which was quantitatively analyzed. Based on the clinical files of the patients, age, complaints at admission, clinical findings, laboratory findings and final diagnosis were recorded.
Categorical variables were expressed by counts and percentages. The groups were compared using the Chi-square test for the variables. The value α=0.05 was taken as a significant level. Statistical analyses were made with SPSS version 16.0 (SPSS Inc., Chicago, IL).
RESULTS
This study included 1 586 women of reproductive age (18–50 years) who presented to the ED and had a pregnancy test for 5 years. Their median age was 27 years, IQR was 11, and 62.2% of them were at age of 18–29 years (Figure 1).
Figure 1.
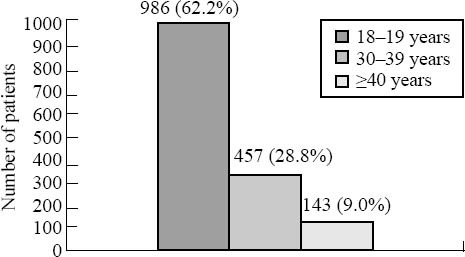
Distribution of the patients in age groups.
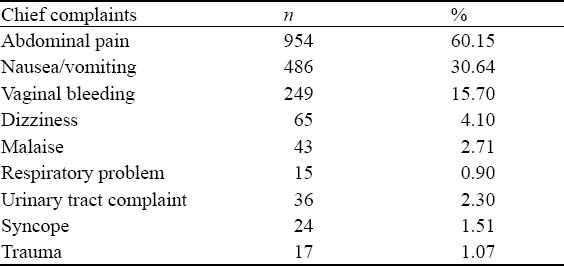
Of the patients, 19.55% (n=310) had a positive result of pregnancy test. In the patients who were subjected to a pregnancy test, the most common complaint at admission was abdominal pain (60.15%, n=954) (Table 1). Pregnancy test was positive in 15.83% (n=151) and negative in 84.17% (n=803) of the patients with abdominal pain. But it was positive in 25.16% (n=159) and negative in 74.84% (n=473) of the patients without abdominal pain. A significant difference was seen between the patients with abdominal pain and those without (P<0.001). Abdominal pain was commonly localized in the bilateral lower quadrants (15.26%) or in the right lower quadrant (11.66%). Of the patients, 30.64% (n=486) had nausea-vomiting at admission, and 11.52% (n=56) had a positive result of pregnancy test. It was positive in 23.09% (n=254) of the patients without nausea-vomiting. A significant difference was observed between the patients with nausea-vomiting and those without (P<0.001). When other complaints were considered, the most commonly observed complaints were non-specific symptoms like dizziness, malaise and respiratory problems. Of the patients, 70.93% didn’t remember the date of last menstruation, and 9.51% had a positive result of pregnancy test. Ninety-six patients reported menstrual irregularity and 16.67% of them had a positive result of pregnancy test. A positive result of pregnancy test was found in 71.43% of patients with a history of ectopic pregnancy (n=21). Among the patients, 32% (n=507) had a consultation with the doctors of the department of obstetrics and gynecology (61.93%, n=314).
Table 1.
Female patients of 18–50 years old undergoing pregnancy test (n=1 586)
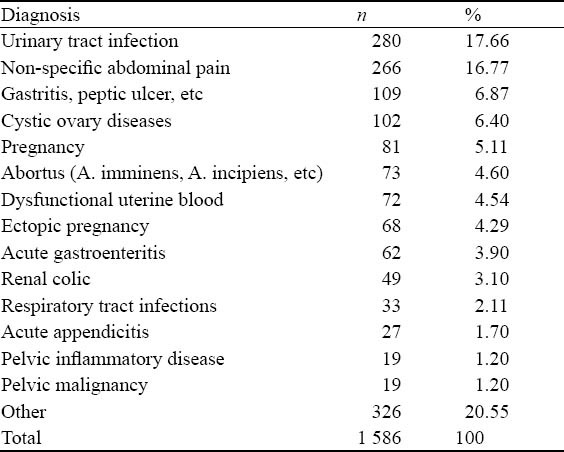
Urinary tract infection (UTI) was often diagnosed with an incidence of 17.66% (n=280), which was followed by non-specific abdominal pain (NSAP) (16.77%, n=266) and gastrointestinal complaints such as gastritis and peptic ulcer (6.87%) (Table 2). Of the patients, 5.11% (n=81) were diagnosed with normal pregnancy, whereas 4.29% (n=68) were diagnosed with ectopic pregnancy. Interestingly, 7.14% (n=20) of the patients were diagnosed with UTI and 4.51% (n=12) with NSAP; all had a positive result of pregnancy test. But 88.40% (n=1 402) of the patients were discharged from the ED, and 11.60% (n=184) were hospitalized. A majority of the patients (64.67%) were hospitalized in the department of obstetrics and gynecology, and ectopic pregnancy was the most common disease.
Table 2.
The most common diseases in the patients with a positive pregnancy test
DISCUSSION
Pregnancy test should become a routine practice to rule out pregnancy in women of reproductive age in the emergency department (ED). Except life-threatening conditions, pregnancy test can be done before radiological diagnostic analyses or medications are given in routine practice, but some reports[2–4] argued that patient history, patient self-assessment, and physician's estimates are adequate and that pregnancy test is not needed in routine practice.
In the present study, pregnancy test showed a high positivity of 19.55% in contrast to 12% reported by Minnerop et al[2] and to 2.3% by Strote et al.[5] In these aforementioned studies, the investigators argued that pregnancy test is not necessary in routine practice and that patient history would be adequate. Ramoska et al[3] reported that although patients precisely knew their menstrual regularity and had a low likelihood of pregnancy because of anamnesis, they found a pregnancy rate of 7% and that in ED pregnancy test was necessary instead of patient history. Compared to the study by Ramoska et al,[3] most of our patients (70.93%) did not know the date of their last menstruation. Therefore, we consider that pregnancy test should be done routinely for women admitted to ED.
In our study, the median age of the patients was 27 years and more than half of them were young patients at age of 18–29 years who may have a high pregnancy rate. The median age of the patients was similar to the reported in the literature.[2,5]
Abdominal pain, urinary complaints and nausea-vomiting were the most common complaints in the study performed by Strote and Chen,[5] whereas abdominal pain, vaginal bleeding and respiratory tract diseases were recognized as the most common complaints in the study performed by Minnerop et al.[2] In our study, however, the most common complaints were abdominal pain, nausea-vomiting and vaginal bleeding.
Pregnancy test is one of the diagnostic methods to rule out ectopic pregnancy in women of reproductive age with abdominal pain and vaginal bleeding who are admitted to the ED.[7] In our patients, the most commonly seen complaint at admission was abdominal pain (60.15%, n=954), and 15.83% of them had a positive result of pregnancy test. Vaginal bleeding was observed in 15.70% (n=249) of the patients, and 51.81% had a positive result of pregnancy test. Menon et al[8] reported a rate of 21.7% for ectopic pregnancy in patients ≥20 years old, but other studies showed the rate varied from 8% to 13%. Schuur et al[10] reported that in 4 different EDs which included only the patients with abdominal pain, the rate of pregnancy test request was 33% and the rate of ectopic pregnancy was 55.6%. In their patients, 89.4% of complained of abdominal pain. In our study, the lower rate of ectopic pregnancy (4.2% for ≥18 years-old patients) may be due to the exclusion of patients with abdominal pain or vaginal bleeding who were subjected to a pregnancy test. Stengel et al[11] found a rate of 6.3% for unknown pregnancy, whereas the rate was 13% in patients with abdominal and pelvic complaints and 2.5% in those with other complaints. In our study, the overall pregnancy rate was 19.50%, and it was 16% in the patients with abdominal pain and 11.60% in those with nausea-vomiting. The pregnancy rate and other complaints were taken into account because of non-specific symptoms such as dizziness, malaise and respiratory tract problems.
Limitations
Our study is limited by its single center experience and the retrospective nature. In addition, a higher estimated rate of pregnancy may due to the fact that more than half (62.2%) of the patients were at age of 18–29 years. Besides, the patients who had a pregnancy test were determined by searching the hospital database, but we did not know the results of the patients who didn’t have a pregnancy test in the study period. The major limitation in this study was the lack of data of the patients of reproductive age including those who did not have a pregnancy test.
In conclusion, it is impossible to rule out pregnancy by patient history, patient self assessment or physician's estimates, and pregnancy test should be done as a routine practice to exclude the pregnancy before radiological tests or medications have been prescribed. However, the results of this study should be further evaluated by prospective multicenter studies. As more than half of the patients in our study were young people, we suggest that preventive or educational measures should be taken.
Footnotes
Funding: None.
Ethical approval: The study was approved by the Medical Ethics Committee of Uludag University, Bursa, Turkey.
Conflicts of interest: The authors declare that there is no conflict of interest.
Contributors: Köksal Ö proposed the study, analyzed the data and wrote the first drafts. All authors contributed to the design and interpretation of the study and to further drafts.
REFERENCES
- 1.Lazarenko GC, Dobson C, Enokson R, Brant R. Accuracy and speed of urine pregnancy tests done in the emergency department: a prospective study. CJEM. 2001;3:292–295. doi: 10.1017/s1481803500005790. [DOI] [PubMed] [Google Scholar]
- 2.Minnerop MH, Garra G, Chohan JK, Troxell RM, Singer AJ. Patient history and physician suspicion accurately exclude pregnancy. Am J Emerg Med. 2011;29:212–215. doi: 10.1016/j.ajem.2009.10.017. [DOI] [PubMed] [Google Scholar]
- 3.Ramoska EA, Sacchetti AD, Nepp M. Reliability of patient history in determining the possibility of pregnancy. Ann Emerg Med. 1989;18:48–50. doi: 10.1016/s0196-0644(89)80310-5. [DOI] [PubMed] [Google Scholar]
- 4.Lippmann S, Bordador B, Shaltout T. Detection of unknown early pregnancy. A matter of safety. Postgrad Med. 1988;83:129–131. doi: 10.1080/00325481.1988.11700308. [DOI] [PubMed] [Google Scholar]
- 5.Strote J, Chen G. Patient self assessment of pregnancy status in the emergency department. Emerg Med J. 2006;23:554–557. doi: 10.1136/emj.2005.031146. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Bachman GA. Myth or fact: can women self-diagnose pregnancy? Med Soc NJ. 1984;81:857–858. [PubMed] [Google Scholar]
- 7.Kohn MA, Kerr K, Malkevich D, O’Neil N, Kerr MJ, Kaplan BC. Beta-human chronic gonadotropin levels and the likelihood of ectopic pregnancy in emergency department patients with abdominal pain or vaginal bleeding. Acad Emerg Med. 2003;10:119–126. doi: 10.1111/j.1553-2712.2003.tb00028.x. [DOI] [PubMed] [Google Scholar]
- 8.Menon S, Sammel MD, Vichnin M, Barnhart KT. Risk factors for ectopic pregnancy: a comparison between adults and adolescent women. J Pediatr Adolesc Gnynecol. 2007;20:181–185. doi: 10.1016/j.jpag.2007.01.007. [DOI] [PubMed] [Google Scholar]
- 9.Kaplan BC, Dart RG, Moskos M, Kuligowska E, Chun B, Adel Hamid M, et al. Ectopic pregnancy: prospective study with improved diagnostic accuracy. Ann Emerg Med. 1996;28:10–17. doi: 10.1016/s0196-0644(96)70131-2. [DOI] [PubMed] [Google Scholar]
- 10.Schuur JD, Tibbetts SA, Pines JM. Pregnancy testing in women of reproductive age in US emergency departments, 2002 to 2006: assessment of a national quality measure. Ann Emerg Med. 2010;55:449–457. doi: 10.1016/j.annemergmed.2009.08.017. [DOI] [PubMed] [Google Scholar]
- 11.Stengel CL, Seaberg DC, MacLeod BA. Pregnancy in the emergency department: risk factors and prevalence among all women. Ann Emerg Med. 1994;24:697–700. doi: 10.1016/s0196-0644(94)70280-2. [DOI] [PubMed] [Google Scholar]