

Abstract
BACKGROUND:
Cardiopulmonary resuscitation (CPR) is a life-saving technique which is used after cardiopulmonary arrest. Chance of survival after arrest will increase if it is coupled with sufficient knowledge. Final year undergraduate health science students and interns manage many trauma and critically ill patients in our hospital. Even though all students took CPR training in undergraduate course, we sometimes saw difficulties in the resuscitation of patients after cardiopulmonary arrest by undergraduate health professionals. This study was to assess the level of knowledge of undergraduate health science students and medical interns about cardiopulmonary resuscitation.
METHODS:
Hospital based cross-sectional study was conducted from February 1 to March 30, 2013. All undergraduate health professionals were included. The mean score of knowledge was compared for sex, original residence and department of the participants by using Student's t test and ANOVA with Scheffe's test. P values <0.05 were considered statistically significant.
RESULTS:
Four hundred sixty-one out of 506 students were included in this study with a response rate of 91.1%. The overall mean knowledge score of final year undergraduate health science students and interns was 11.1 (SD=0.2). The mean knowledge scores of nurses, interns, health officer, midwifery, anesthesia and psychiatry nursing students were 9.84 (SD=2.5), 13.34 (SD=2.8), 9.81 (SD=3.0), 8.77 (SD=2.6), 13.31 (SD=2.7) and 8.43 (SD=2.4) respectively.
CONCLUSIONS:
The knowledge level of undergraduate health professionals about cardiopulmonary resuscitation was insufficient. Training about CPR for undergraduate health professionals should be emphasized.
KEYWORDS: Cardiopulmonary resuscitation, Knowledge, Undergraduate, Health professionals
INTRODUCTION
Cardiopulmonary arrest is a major public health problem[1,2] and many patients sustained cardiac arrest in two years.[3] It is more common in low socio-economic areas.[4–5] Cardiopulmonary arrest is one of the most common unfortunate incidents that may occur in and out of the health facilities.[6–10]
Cardiopulmonary resuscitation (CPR) is a life-saving technique[11] and consists of chest compression and rescue breathing.[12] The quality of cardiopulmonary resuscitation depends on the sufficiency of the knowledge of health professionals and facilities.[13–16] Increasing survival of patients from cardiopulmonary arrest requires improvement in resuscitation education.[17–24]
Studies conducted in Iran and New Zealand showed that the knowledge of interns and newly qualified doctors were substandard.[25–27]
A study conducted in India showed that the knowledge of nursing students and interns about basic life support (BLS) was very poor.[28] A study done in Nigeria found that the knowledge level of anesthesia trainees about CPR was poor.[29]
Although, all health professionals took CPR training in undergraduate course and involved in the management of many trauma and critically ill patients in our hospital, we sometimes saw difficulties in the resuscitation of patients after cardiopulmonary arrest. Hence, this study was undertaken to assess the knowledge level of undergraduate health professionals.
METHODS
Study design, area and period
This hospital based cross-sectional study was conducted from February 1 to March 30, 2013.
Study participants
All final year undergraduate health science students and interns who were at the time of data collection were included. Students who were sick and environmental-occupational health and safety, pharmacy, medical laboratory, optometry and physiotherapy students who had no exposure to cardiopulmonary resuscitation activities were excluded.
Study tools
We developed a structured questionnaire which addressed socio-demographics, field of study of students, theoretical and practical knowledge of participants about BLS and advanced cardiovascular life support (ACLS) based on 2010 UK Resuscitation Council Guidelines. The questionnaire was validated and pilot tested in other hospitals, and changes were made before the study. Twenty-seven knowledge questions were used and each correct answer was given a score of one point. The knowledge level of the students was classified as sufficient for students who answered correctly at least 22 out of 27 questions (total score of >80%) and insufficient for students who correctly answered for less than 22 out of 27 questions (total score <80%) according to 2005 AHA accreditation criteria.
Ethical approval
Ethical clearance was obtained from the Institutional Ethical Review Board. Written informed consent was obtained from study subjects and confidentiality was ensured using anonymous questionnaire.
Data collection procedures
We distributed the questionnaires to students after morning sessions and classes from the respective departments. Self administered questionnaires were used to collect data from the students.
Statistical analysis
Data were analyzed using SPSS version 20.0 software for Windows. The mean score of knowledge was compared for sex, original residence and department of the students by using Student's t test and ANOVA with Scheffe's test. P values <0.05 were considered statistically significant.
RESULTS
Socio-demographic characteristics of respondents
A total of 506 final year undergraduate students in those departments were included in the study. Of these students, 21 were excluded due to incomplete filling of questionnaires, 20 students refused to participate in the study, and 4 students were excluded because of sickness during data collection.
Four hundred sixty-one (91.1%) out of the 506 students responded. Males accounted for 66.4% of the respondents. The minimum, maximum and mean age of the students were 19, 39 and 23 years respectively. The original residences of 244 (52.9%) students were from the urban areas.
This study comprised medical interns (135; 29.3%), nurses (123; 26.7%), as well as health officer (88; 17.4%), midwifery (77; 16.7%), anesthesia (32; 6.9%) and psychiatry nursing students (14; 3.0%) respectively.
Knowledge level of graduate health science students and medical interns about cardiopulmonary resuscitation
The minimum and maximum knowledge scores of the students was 3 and 21 (interquartile range =5). The mean knowledge score was 11.1 (SD=0.2) and the overall knowledge level of undergraduate health science students and interns about cardiopulmonary resuscitation was poor (< 80%).
Of twenty-seven knowledge questions, your first response when you get adult patient unresponsive somewhere in the health facility (11; 8.9%) and your immediate measure after you confirm the patient is unresponsive after shaking (19; 15.5%), duration of time to check for sign of life in arrested patients (19; 15.5%) and depth of chest compression in adult patients during CPR (19; 15.5%) were correctly answered by a small number of nursing students respectively.
On the other hand, best site to check pulse for adult and older children during cardiac arrest and depth of chest compression in neonates during CPR were correctly answered by 76 (61.7%) and 86 (69.9%) of undergraduate nursing students respectively. The percentage of correct response to 20 (74.1%) questions was below 50%.
Of 27 knowledge questions, definition of BLS (132; 97.8%), best site to check pulse for adult and older children during cardiac arrest (116; 85.9%) and your first response when you get unresponsive child somewhere in the health facility (116; 85.9%) were correctly answered by the majority of interns. Whereas shockable rhythm and dose of adrenaline for children were answered by (103; 76.3%) and (96; 71.1%) interns respectively. On the other hand, your first response when you get adult patient unresponsive somewhere in the health facility (13; 9.6%), rescue breathing techniques for infants (25; 18.5%), definition of AED (25; 18.5%) were correctly answered by a very small number of interns. The percentage of correct response for fourteen questions was <50%.
The definition of BLS was correctly answered by the majority (69; 86.5%) of health officer students. Your first response when you get adult patient unresponsive somewhere in the health facility, technique of rescue breathing for infants, depth of chest compression in adults during CPR, rate of chest compression in adults and older children during CPR, definition of AED and your first response when your friend gets choking while eating food, were answered by 4 (5%), 12 (15%), 12 (15%), 13 (16.3%), 5 (6.3%), and 3 (3.7%) health officer students respectively. The percentage of correct response for 20 questions was <50%.
More than 50% of reponses was given to only three knowledge questions. The definition of BLS, depth of chest compression for neonates during CPR and shockable rhythm were answered by (43; 55.8%), (43; 55.8%) and (39; 50.6%) midwifery students respectively. Duration of time to check for sign of life in arrested patients (5; 6.5%), your first response when you get adult patient unresponsive somewhere in the health facility (9; 11.7%), depth of chest compression in adults during CPR (6; 7.8%), depth of chest compression in children during CPR (14; 18.2%), ratio of CPR with single rescuer (6; 7.8%), your first response when your friend gets choking while eating food (6; 7.8%) were answered by a very small number of midwifery students.
Six knowledge questions were answered by the majority of anesthesia students. Definition of BLS (31; 96.8%), your immediate measure after you confirm the patient is unresponsive after shaking (21; 81.3%), shockable rhythm (29; 90.6%), energy for children and infants (29; 90.6%), dose of adrenaline for adults during CPR (27; 84.3%) and dose of adrenaline for children during CPR (30; 93.7%) were answered by the majority of anesthesia students. The definition of AED (4; 12.5%) was answered by a very small number of anesthesia students.
The percentage of response of anesthesia students was below 50% for questions all can be used during mouth-to-mouth breath with CPR except 12 students (37.5%), technique of rescue breathing for 8 infants (25%), depth of chest compression for 10 children during CPR (31.3%), ratio of CPR with single rescuer for 8 (25%), when will you give adrenaline and amiodarone during CPR 10 (31.3%), and your first response when your friend gets choking while eating food 10 (31.3%).
The percentage of the responses of psychiatric nursing students was >50% for knowledge questions: the right location for chest compression for children and infants (8; 57.1%), depth of chest compression in neonates during CPR (9; 64.3%), shockable rhythm (7; 50%) and when will you give adrenaline and amiodarone during CPR (8; 57.1%). No student got the correct answer for your first response when your friend gets choking while eating food. Very few psychiatric students got correct answer for questions about your first response when you get adult patient unresponsive somewhere in the health facility (1; 7.1%), techniques of rescue breathing for infants (2; 14.3%), depth of chest compression in children during CPR (1; 7.1%), depth of chest compression in adults during CPR (2; 14.3%), ratio of CPR with single rescuer (1; 7.1%), definition of AED (1; 7.1%), and duration of one cycle of CPR (2; 14.3%).
Comparisons of the knowledge scores in relation to the different characteristics of the participants
There was no significant difference in the knowledge scores in terms of age and their original residence of the participants. From the ANOVA test, the mean knowledge score was significantly different in students of different categories (nurses vs. interns, P<0.001; nurses vs. anesthesia, P<0.001; intern vs. health officer, P=0.001; intern vs. midwifery, P<0.001; intern vs. anesthesia, P<0.001; intern vs. psychiatry nursing, P=0.001).
The mean knowledge score of anesthesia students was significantly different from the mean knowledge score of students of each category (nursing, intern, health officer, midwifery and psychiatry nursing) with P<0.001. The overall difference in the attitude score within different categories was significant (P <0.001) (Tables 1 and 2).
Table 1.
Post hoc test of ANOVA (Scheffe), and multiple comparisons of knowledge scores of students from different departments (n=461)
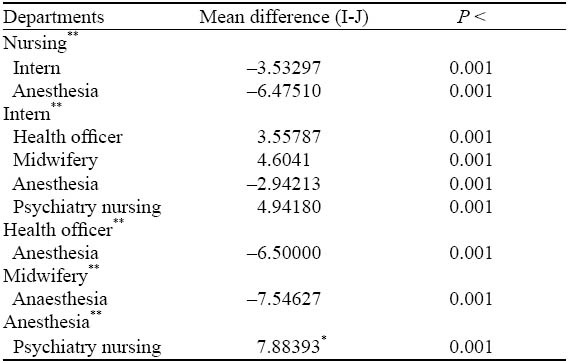
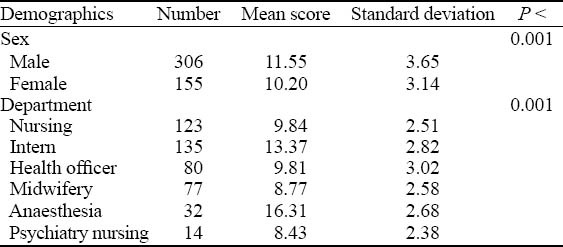
Table 2.
Comparisons of the knowledge scores in relation to the different characteristics of the participants, ANOVA test (n=461)
DISCUSSION
This study showed that the overall knowledge level of final year undergraduate health science students and medical interns was poor. The overall mean knowledge score was 11.1 (SD=0.2). The mean knowledge scores of nurses, interns, as well as health officer, midwifery, anesthesia and psychiatry nursing students were 9.84 (SD=2.5), 13.34 (SD=2.8), 9.81 (SD=3.0), 8.77 (SD=2.6), 13.31 (SD=2.7) and 8.43 (SD=2.4) respectively.
In this study, the mean knowledge score of interns was poor (49.4%). This finding was in line with studies conducted in Iran[25,26] and New Zealand[27] respectively.This could be due to lack of exposure to enough number of real cardiopulmonary resuscitation cases, simulation based training, updating training and certification process before graduation.
The mean knowledge score of final year nursing students was poor (36.4%). This finding was consistent with a study done in India.[28] This might be due to failure to give graduate students appropriate training before graduation and simulation-based training. In addition to this, the absence of certification criteria on the knowledge of students about cardiopulmonary resuscitation before leaving university might significantly affect their knowledge.
The mean knowledge score of final year health officer students was poor (36.3%). This might be due to lack of insufficient training in undergraduate course and failure to get adequate number of real cardiopulmonary resuscitation cases. This could also be evidenced by less than 50% of their responses to twenty knowledge questions, only 9 (11.3%) students who attended CPR session in their curriculum, 30 (37.5%) said they had adequate knowledge, 17 (21.3%) attended 1–5 real CPR cases and 1 (1.3%) attended more than five real CPR cases respectively during their undergraduate course and clinical attachments.
The mean knowledge score of final year midwifery students was poor (32.5%). This finding was in line with a study conducted in Iran.[29] This might be due to their limited exposure to cardiopulmonary resuscitation cases and insufficient training about BLS and ACLS during the undergraduate course. This could also be evidenced by only 36 (46.7%) students who said they had adequate knowledge, 29 (37.7%) and 7 (9.1%) midwifery students said they attended CPR session in their curriculum and attended more than five real CPR cases.
The mean knowledge score of final year anesthesia students was poor (49.3%). The percentage of their responses to knowledge questions was >80% for six questions, >50% for fourteen questions, and <50 % for seven questions respectively. Only 25 (78.1%) students attended CPR sessions in their curriculum, 17 (53.1%) said they were adequately equipped with knowledge about cardiopulmonary resuscitation, 12 (37.5%) attended 1–5 real CPR cases and 7 (9.1%) attended greater than 5 real CPR cases during undergraduate course and clinical practice periods. This finding was in line with a study conducted in Nigeria.[30] This could be due to lack of simulation-based training, updating training and failure to get enough number of real CPR cases because of an increase in the number of students in the last four years.
The mean knowledge score of anesthesia students was significantly different and higher than the mean knowledge score of students of each category (nursing, intern, health officer, midwifery and psychiatry nursing) (P<0.001). This could be due to their frequent involvement in the management of critical patients.
The mean knowledge score of final year psychiatry nursing students was poor (31.2%). The percentage of their responses to knowledge questions was >50% for four questions, 0 (0%) for one question, and <50% for 22 questions. Only 5 (35.7%) students attended CPR sessions in their curriculum, 4 (28.6%) said they had adequate knowledge about cardiopulmonary resuscitation, 4 (28.6%) attended 1–5 real CPR cases and no students attended more than five real CPR cases during the undergraduate course and clinical attachment. This might be due to their limited exposure to critically ill patients, lack of updating and simulation-based training.
In conclusion, the overall knowledge level of final year undergraduate health science students and interns about cardiopulmonary was insufficient (41.1%). Training about BLS and ACLS for undergraduate health science students and medical interns should be emphasized.
Footnotes
Funding: We did not have any support for the study.
Ethical approval: This study was approved by the institutional ethical review board of University of Gondar.
Conflicts of interest: We have no conflicts of interest to the report.
Contributors: Gebreegziabher E conceived the study and developed the proposal. Berhe G and Bradley B revised the proposal, involved in data collection, data analysis, paper writing and manuscript preparation with Endale. All authors approved the final manuscript.
REFERENCES
- 1.Chugh SS, Reinier K, Teodorescu C, Evanado A, Kher E, Samara AM, et al. Epidemiology of sudden cardiac death: clinical and research implications. Prog Cardiovasc Dis. 2008;51:213–228. doi: 10.1016/j.pcad.2008.06.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Lioyd-Jones D, Adams R, Carnethon M, Simone DG, Ferguson BT, Flegal K, et al. Heart disease and stroke statistics-update: A report from the American Heart Association statistics committee and stroke statistics subcommittee. Circulation. 2009;119:480–486. doi: 10.1161/CIRCULATIONAHA.108.191259. [DOI] [PubMed] [Google Scholar]
- 3.Peberdy MA, Kaye W, Ornato JP, Larkin LG, Nadkarni V, Mancini EM, et al. Cardiopulmonary resuscitation of adults in the hospital: A report of 14 720 cardiac arrests from the national registry of cardiopulmonary resuscitation. Resuscitation. 2003;58:297–308. doi: 10.1016/s0300-9572(03)00215-6. [DOI] [PubMed] [Google Scholar]
- 4.Feero S, Hedges JR, Stevens P. Demographics of cardiac arrest: association with residence in a low-income area. Acad Emerg Med. 1995;2:11–16. doi: 10.1111/j.1553-2712.1995.tb03071.x. [DOI] [PubMed] [Google Scholar]
- 5.SOO L, Natasha H, David G, John H. Geographical distribution of cardiac arrest in Nottinghamshire. Resuscitation. 2001;48:137–147. doi: 10.1016/s0300-9572(00)00248-3. [DOI] [PubMed] [Google Scholar]
- 6.Shultz JJ, Lurie KG. Variations in cardiopulmonary resuscitation techniques: past, present and future. Can J Cardiol. 1995;11:873–880. [PubMed] [Google Scholar]
- 7.Heller RF, Steele LR, Fisher DJ, Alexander MH, J Dobson JA. Success of cardiopulmonary resuscitation after heart attack in hospital and outside hospital. BMJ. 1995;311:1332–1336. doi: 10.1136/bmj.311.7016.1332. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Yap H, Li ST T, Tan KS, Cheung Y, Chui P, Lam K P, et al. Characteristics, management process, and outcome of patients suffering in-hospital cardiopulmonary arrests in a teaching hospital in Hong Kong. Hong Kong Med J. 2007;13:258–265. [PubMed] [Google Scholar]
- 9.Sodhi K, Singla MK, Shrivastava A. Impact of advanced cardiac life support training program on the outcome of cardiopulmonary resuscitation in a tertiary care hospital. Indian J Crit Care Med. 2011;15:209–212. doi: 10.4103/0972-5229.92070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Borimnejad L, Nasrabadi NA, Mohammadi H, Kheirati L. Improving the outcomes of CPR: A report of a reform in the organization of emergency response. The Internet Journal of Emergency Medicine. 2008;4:2. [Google Scholar]
- 11.2012. WWW.familydoctor.org : Cardiopulmonary resuscitation, downloaded on July 11 .
- 12.2012. WWW.WIKIPEDIA : Cardiopulmonary resuscitation, downloaded on July 11.
- 13.Leong BS, Chua GS. Quality of resuscitation in hospitals. Singapore Med J. 2011;52:616. [PubMed] [Google Scholar]
- 14.Luo XR, Zhang HL, Chen GJ, Ding WS, Huang L. Active compression-decompression cardiopulmonary resuscitation (CPR) versus standard CPR for cardiac arrest patients: a metaanalysis. World J Emerg Med. 2013;4:266–272. doi: 10.5847/wjem.j.issn.1920-8642.2013.04.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ian J, Vinay N. Cardiac arrest and cardiopulmonary resuscitation Outcome reports: update and simplification of the Utstein templates for resuscitation registries: A statement for healthcare professionals from a task force of the international liaison committee on resuscitation (American Heart Association, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Councils of Southern Africa) Circulation. 2004;110:3385–3397. doi: 10.1161/01.CIR.0000147236.85306.15. [DOI] [PubMed] [Google Scholar]
- 16.Jäntti H. Publications of the University of Eastern Finland dissertations in health sciences; 2010. Cardiopulmonary resuscitation quality and education. [Google Scholar]
- 17.Bhanji F, Mancini ME, Sinz E, Rodgers DL, McNeil MA, Hoadley TA, et al. Part 16: education, implementation, and teams: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation. 2010;122:S920–933. doi: 10.1161/CIRCULATIONAHA.110.971135. [DOI] [PubMed] [Google Scholar]
- 18.Sutton RM, Niles D, Nysaether J, Abella BS, Arbogast KB, Nishisaki A, et al. Quantitative analysis of CPR quality during in-hospital resuscitation of older children and adolescents. Pediatrics. 2009;124:494–499. doi: 10.1542/peds.2008-1930. [DOI] [PubMed] [Google Scholar]
- 19.Losert H, Sterz F, Kohler K, Sodeck G, Fleischhackl R, Eisenburger P, et al. Quality of cardiopulmonary resuscitation among highly trained staff in an emergency department setting. Arch Intern Med. 2006;166:2375–2380. doi: 10.1001/archinte.166.21.2375. [DOI] [PubMed] [Google Scholar]
- 20.Peters R, Boyde M. Improving survival after in-hospital cardiac arrest: the Australian experience. Am J Crit Care. 2007;16:240–246. [PubMed] [Google Scholar]
- 21.El-Menyar AA. The resuscitation outcome. Chest. 2005;128:2835–2846. doi: 10.1378/chest.128.4.2835. [DOI] [PubMed] [Google Scholar]
- 22.Topjian AA, Berg RA, Nadkarni VM. Pediatric cardiopulmonary resuscitation: advances in science, techniques, and outcomes. Pediatrics. 2008;122:1086–1098. doi: 10.1542/peds.2007-3313. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Moretti MA, Cesar LAM, Nusbacher A, Kern BK, Timerman S, Ramires FAJ. Advanced cardiac life support training improves long-term survival from in-hospital cardiac arrest. Resuscitation. 2007;72:458–465. doi: 10.1016/j.resuscitation.2006.06.039. [DOI] [PubMed] [Google Scholar]
- 24.Falcão LFR, Ferez D, Amaral JLG. Update on cardiopulmonary resuscitation guidelines of interest to anesthesiologists. Rev Bras Anestesiol. 2011;61:624–640. doi: 10.1016/S0034-7094(11)70074-5. [DOI] [PubMed] [Google Scholar]
- 25.Ravari H, Abrishami M, Ghezel-Sofla M, Shahroodi VM, Abrishami M. Knowledge of Iranian medical interns regarding cardio-pulmonary resuscitation. Trauma Mon. 2012;17:242–244. doi: 10.5812/traumamon.4230. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Isazadehfar Kh, Sadaghat M, Entezariasl M. Cardiopulmonary resuscitation training for medical students in anesthesiology rotation in Ardabil medical University (Iran) J Med Education. 2008;12:37–34. [Google Scholar]
- 27.Price CS, Bell SF, Janes SE, Ardagh M. Cardio-pulmonary resuscitation training, knowledge and attitudes of newly qualified doctors in New Zealand in 2003. Resuscitation. 2006;68:295–299. doi: 10.1016/j.resuscitation.2005.07.002. [DOI] [PubMed] [Google Scholar]
- 28.Chandrasekaran S, Kumar S, Bhat SA, Saravanakumar, Shabbir PM, Chandrasekaran V. Awareness of basic life support among medical, dental, nursing students and doctors. Indian J Anaesth. 2010;54:121–126. doi: 10.4103/0019-5049.63650. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Abdollahi AA, Yazdi Kh, Hosseini SA, Khoddam H. Effect of station training method on students’ cardiopulmonary resuscitation activity. Iran J Crit Care Nursing. 2010;3:105–108. [Google Scholar]
- 30.Ibironke D, Olanrewaju OO, Olutola JO. Training and confidence level of junior anaesthetists in CPR experience in a developing country. Indian J Anaesthesia. 2008;52:297–300. [Google Scholar]