

Abstract
BACKGROUND:
Acute pancreatitis is a serious complication during pregnancy, however the incidence of hyperlipidemia induced by pancreatitis is lower.
METHODS:
We treated a pregnant woman with hypertriglyceridemia-associated acute gestational pancreatitis who simultaneously developed hypoxemic acute respiratory failure (ARF).
RESULTS:
The woman was successfully treated through noninvasive positive pressure ventilation (NPPV), emergent caesarean delivery, drainage of chylous ascites, and peritoneal lavage.
CONCLUSION:
The signs and symptoms of ARF were greatly improved in this patient after NPPV and conventional therapies. Early NPPV may be related to good prognosis of the disease.
KEY WORDS: Hyperlipidemia, Pancreatitis, Pregnancy
INTRODUCTION
Pancreatitis in pregnancy remains a rare event, and is often associated with gallstone disease. Hyperlipidemic gestational pancreatitis usually occurs in women with a preexisting abnormality of lipid metabolism.[1] We treated a pregnant woman with acute pancreatitis who had been previously healthy with no history of cholelithiasis, alcohol, inherited diseases, diabetes, nongestational hyperlipidemia or drug abuse. We also reviewed the literature about hyperlipidemic pancreatitis.
CASE REPORT
A pregnant woman with acute pancreatitis caused by hyperlipidemia, aged 31 years, G2P0, was admitted to our emergency department. On admission, she complained of severe abdominal pain complicated by nausea and vomiting for one day in her 27-week gestation. She was previously healthy with no history of cholelithiasis, alcohol, inherited diseases, diabetes, nongestational hyperlipidemia or drug abuse. Her body mass index was 22 kg/m2 before pregnancy. On admission, her body temperature was 36.8 °C, blood pressure 120/70 mmHg, heart rate 120 bpm, and respiration 20 bpm. Physical examination showed harsh breath sounds and subxiphoid tenderness without Grey Turner’s or Cullen’s sign. Laboratory examination revealed amylase was 178 U/L, white blood cell count 7.9×109/L, hemoglobin 126 g/L, neutrophil 70%, HCT 0.39, platelets 106×109/L, CRP 148 mg/L, calcium 1.87 mmol/L, and blood glucose 7.2 mmol/L. At the same time, arterial blood gas was pH 7.43, PCO2 41 mmHg, PO2 78 mmHg, SaO2 96%, and HCO3 27 mmol/L. Renal function was normal and blood sample was milky. Triglyceride was 29.05 mmol/L and cholesterol was 18.05 mmol/L. The diagnosis of acute pancreatitis was confirmed by computed tomography (Figure 1).
Figure 1.
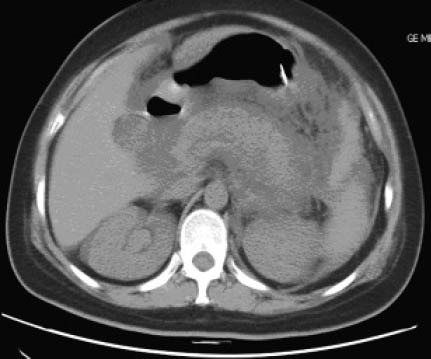
CT showing an extensively swollen pancreas, disappearance of the space among peripancreatic adipose tissues and thickening of the anterior fascia of the kidney on the left side.
Abdominal pain was not relieved after the treatment of abrosia, intravenous nutritional support, hydration, lipid lowering agent, and gemfibrozil. The next day, the patient presented dyspnea with tachypnea 45 bmp, noninvasive finger blood oxygen saturation 86%, and heart rate 130 bmp. D-dimer assay was normal. Chest X-ray showed diffuse infiltration of the lung. Arterial blood gas analysis disclosed severe hypoxemia with a PaO2/FiO2 ratio of 190. A diagnosis of acute respiratory failure was made and APACHE II score was 5. The patient was transferred to ICU. After NPPV, SaO2 increased to above 90%, respiration decreased to 28 bmp, and heart rate reduced to 102 bmp. Lipid panel evidently decreased on the fifth day after hospitalization. However, fetal heart rate showed decelerations later. An emergent cesarean delivery was performed under spinal anesthesia, and a male infant weighing 1 180 g was delivered successfully. The first and fifth minute Apgar scores were 5 and 6 respectively. The infant was then transferred to NICU. Unfortunately, the infant died of severe immaturity after one week. Intraoperative findings included collection of 750 mL milky peritoneal fluid. Marked swelling and saponification of the greater omentum and gastrointestinal wall were noted. Peritoneal lavage with normal saline and abdominal duct drainage were performed. The operation was successful. Subsequently, dyspnea was resolved. Two weeks after operation, serum triglyceride and cholesterols almost returned to normal. Two months later, abdominal ultrasound showed a pancreatic pseudocyst. One-year follow-up showed that plasma lipid levels were within the normal ranges and no recurrence of acute pancreatitis was noted.
DISCUSSION
Hyperlipidemia is a rare cause of pancreatitis.[2,3] Severe hyperlipidemia is uncommon in pregnancy. Patients usually have pre-existing genetic defects or diseases that can compromise lipid metabolism. However, only a few cases of non-genetic, non-familial, pregnancy-induced hypertriglyceridemia have been reported.[4] The pathogenesis of acute hyperlipidemic pancreatitis in pregnancy is under research.
Severe hyperlipidemia may trigger acute pancreatitis and lead to serious complications. In the present case, the patient developed hypoxemic ARF in early stage. Some studies have indicated that hypoxemia is closely related to the prognosis of acute pancreatitis. UK guidelines for the management of acute pancreatitis emphasize that SaO2 should be kept over 95%. NPPV could relax respiratory muscles, reduce oxygen consumption and atelectasis, increase lung volume, and alleviate hypoxemia. Accordingly, patients with respiratory failure caused by acute pancreatitis would benefit from NPPV.[5]
Severe hyperlipidemia may lead to acute pancreatitis in pregnancy. Early diagnosis and prompt intervention are proved to be live-saving. Treatment of acute hyperlipidemic pancreatitis should be non-operative in addition to appropriate timing, indications for surgery. And operative procedures should follow the principles of minimally invasive surgery.[6] Peritoneal lavage and post-operative abdominal duct drainage may be effective in the treatment of such patients. In our case, 750 mL of chylous ascites was drained from the abdominal cavity during caesarean delivery. Few studies[7] have reported pregnancy-associated hyperlipidemic pancreatitis complicated with chylous ascites.
Therapeutic plasma exchange has been used in the treatment of hyperlipidemic pancreatitis.[8] Double filtration plasmapheresis can be effectively and safely applied in patients with acute hyperlipidemic pancreatitis.[9] Early plasmapheresis or lipid apheresis can effectively reduce serum triglyceride, inhibit disease progression, and prevent the recurrence of hyperlipidemic pancreatitis, but it has risk of acute coronary events.[10,11] Batashki et al[12] reported that intubation with artificial pulmonary ventilation and high volume continuous veno-venous hemofiltration (HV CVVH) should be performed because of the development of polyorgan insufficiency and ARDS. In our case, signs and symptoms of ARF were greatly improved after NPPV and conventional therapies, thus creating the opportunity to perform caesarean delivery when fetal distress occurred. We think that early NPPV is closely related to good prognosis.
Footnotes
Funding: None.
Ethical approval: Not needed.
Conflicts of interest: None.
Contributors: Hang Y proposed the study, analyzed the data and wrote the first draft. All authors contributed to the design and interpretation of the study and to further drafts.
REFERENCES
- 1.Crisan LS, Steidl ET, Rivera-Alsina ME. Acute hyperlipidemic pancreatitis in pregnancy. Am J Obstet Gynecol. 2008;198:e57–59. doi: 10.1016/j.ajog.2008.01.003. [DOI] [PubMed] [Google Scholar]
- 2.Serpytis M, Karosas V, Tamosauskas R, Dementaviciene J, Strupas K, Sileikis A, et al. Hypertriglyceridemia-induced acute pancreatitis in pregnancy. JOP. 2012;13:677–680. doi: 10.6092/1590-8577/1148. [DOI] [PubMed] [Google Scholar]
- 3.Yadav D, Pitchumoni CS. Issues in hyperlipidemic pancreatitis. J Clin Gastroenterol. 2003;36:54–62. doi: 10.1097/00004836-200301000-00016. [DOI] [PubMed] [Google Scholar]
- 4.Eskandar O, Eckford S, Roberts TL. Severe, gestational, non-familial, non-genetic hypertriglyceridemia. J Obstet Gynaecol Res. 2007;33:186–189. doi: 10.1111/j.1447-0756.2007.00506.x. [DOI] [PubMed] [Google Scholar]
- 5.Song RR, Qiu YP, Chen YJ, Ji Y. Application of fiberoptic bronchscopy in patients with acute exacerbations of chronic obstructive pulmonary disease during sequential weaning of invasive-noninvasive mechanical ventilation. World J Emerg Med. 2012;3:29–34. doi: 10.5847/wjem.j.issn.1920-8642.2012.01.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Sun B, Xu DS, Jiang HC, Tai S, Cui YF, Xu J, et al. Study on combined therapy of hyperlipidemic severe acute pancreatitis. Zhonghua Wai Ke Za Zhi. 2007;45:733–735. [PubMed] [Google Scholar]
- 7.Chuang SC, Lee KT, Wang SN, Kuo KK, Chen JS. Hypertriglyceridemia-associated acute pancreatitis with chylous ascites in pregnancy. J Formos Med Assoc. 2006;105:583–587. doi: 10.1016/S0929-6646(09)60154-6. [DOI] [PubMed] [Google Scholar]
- 8.Al-Humoud H, Alhumoud E, Al-Hilali N. Therapeutic plasma exchange for acute hyperlipidemic pancreatitis: a case series. Ther Apher Dial. 2008;12:202–204. doi: 10.1111/j.1744-9987.2008.00572.x. [DOI] [PubMed] [Google Scholar]
- 9.Zhang G, Feng J, Xu QP, Huang HY. Double filtration plasmapheresis in treatment of hyperlipidemic acute pancreatitis. Zhejiang Da Xue Xue Bao Yi Xue Ban. 2008;37:93–96. doi: 10.3785/j.issn.1008-9292.2008.01.017. [DOI] [PubMed] [Google Scholar]
- 10.Kyriakidis AV, Raitsiou B, Sakagianni A, Harisopoulou V, Pyrgioti M, Panagopoulou A, et al. Management of acute severe hyperlipidemic pancreatitis. Digestion. 2006;73:259–264. doi: 10.1159/000095425. [DOI] [PubMed] [Google Scholar]
- 11.Kadikoylu G, Yavasoglu I, Bolaman Z. Plasma exchange in severe hypertriglyceridemia a clinical study. Transfus Apher Sci. 2006;34:253–257. doi: 10.1016/j.transci.2005.11.009. [DOI] [PubMed] [Google Scholar]
- 12.Batashki I, Milchev N, Uchikova E, Pekhlivanov B, Chifligarov K, Uchikov A. Hyperlipidemic pancreatitis during pregnancy-a case report. Akush Ginekol (Sofiia) 2006;45(Suppl 1):41–43. [PubMed] [Google Scholar]