

Abstract
Proximal femur osteochondromas are relatively rare, particularly in the femoral neck. The choice of treatment poses difficulties to the surgeon. We report an unusual case of a patient with 2 osteochondromas in the femoral neck causing femoroacetabular impingement. Appropriate identification and precise resection of the lesions are important steps of the surgical procedure. We present our arthroscopic surgical technique to access the lesions and perform their resection. To our knowledge, this is the first report of hip arthroscopic resection of 2 osteochondromas with considerable dimensions causing femoroacetabular impingement.
Osteochondroma is a hamartoma derived from an aberrant subperiosteal germ of the physeal cartilage, which grows and matures according to normal endochondral ossification. Generally, it originates from the metaphysis of the long bones, predominantly the distal femur, proximal humerus, and proximal tibia.1,2 It is the most frequent benign bone tumor and usually presents as a solitary lesion (90%) or as a clinical form of hereditary multiple exostoses.1
Femoral neck osteochondromas are intra-articular and relatively uncommon but have been reported in the literature.2,3 In this location they may lead to mechanical restriction of hip motion, which may explain the damage to the labrum and adjacent cartilage.2,3 Resection of the tumor poses difficulties in choosing the treatment modality with regard to the risk of compromising femoral head perfusion.2-4 We report a case of a patient with 2 osteochondromas in the femoral neck causing a labral tear who underwent arthroscopic surgery (Video 1).
Surgical Technique
Preoperative Planning
In our experience, preoperative planning for the treatment of femoroacetabular impingement (FAI) is an essential part of the procedure (Table 1). Its importance is simply explained by avoiding either under-resection, leading to residual impingement, or over-resection, which may lead to a point of fragility in the femur or a dysplastic acetabulum. In unusual cases preoperative planning assumes greater importance.
Table 1.
Tips and Pearls
| Preoperative planning is of major importance for every case. |
| Use the supine position because it allows arthroscopy to be performed more easily without traction. |
Use the following portals:
|
| One has the ability to switch between portals. |
| Perform capsular thinning, which improves the mobility of the instruments. |
| Perform sequential examination. |
| Use flexion and rotation to increase visibility and access. |
| During burr resection, alternate with radiofrequency because of bleeding bone. |
In our patient we used a true anteroposterior pelvic radiograph and 45° Dunn view of the left hip to identify both osteochondromas (the larger osteochondroma was in the anterolateral femoral neck and the smaller osteochondroma was more anterior) (Figs 1A and 1B); afterward, we determined the depth of bony resection required. Magnetic resonance imaging (magnetic resonance arthrogram) was obtained for differential diagnostic and evaluation of associated injuries (Fig 2). Computed tomography scan is also important in preoperative planning to better define the localization and extension of the tumor (Fig 1C). Magnetic resonance imaging showed an anterolateral labral tear (Fig 2). Evaluation of the articular cartilage showed minimal thinning on the acetabular side near the labral lesion, without any cartilage defect (Fig 2). The alpha angle was 104° on the anteroposterior view (Fig 1B) and 99° on the 45° Dunn view.
Fig 1.
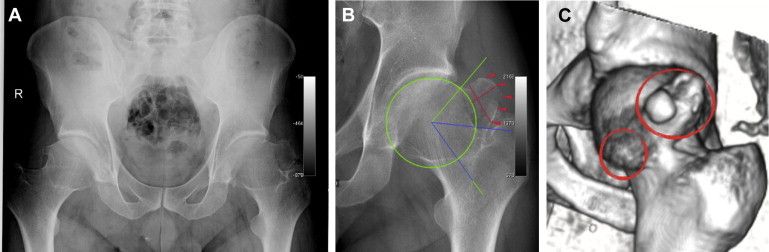
(A) Preoperative anteroposterior radiograph, (B) resection planning radiograph, and (C) computed tomography scan with 3-dimensional reconstruction showing 2 osteochondromas.
Fig 2.
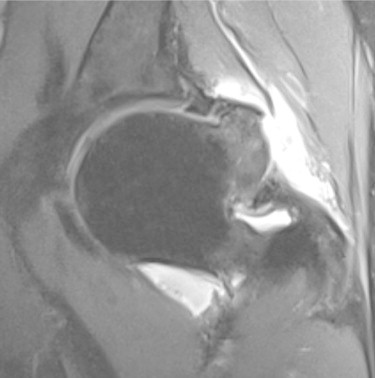
Magnetic resonance arthrogram showing anterolateral labral tear and minimal cartilage lesion.
Arthroscopic Procedure
Preoperative planning showed a large osteochondroma in the anterolateral femoral neck that interfered with our usual first anterolateral portal. For that reason, we started in the peripheral compartment without traction using the proximal anterolateral portal as the viewing portal5 (70° arthroscope) and a mid-anterior portal as the working portal (Table 1). To establish the first portal, it is important to find the soft spot located at the union of the proximal one-third and the middle one-third of a line drawn from the anterior superior iliac spine to the tip of the great trochanter.6 Under fluoroscopy, the arthroscopic needle (Disposable Hip Pac; Smith & Nephew, Andover, MA) is directed perpendicular to the femoral neck axis to the anterolateral head-neck transition.
The second portal is established with slight hip flexion to expand the anterior capsule. After that, to increase the mobility of the instruments and improve inspection, capsular thinning, particularly of the zona orbicularis, is performed from medial to lateral using first a shaver (4.5-mm-long Incisor Plus Elite; Smith & Nephew) and then a radiofrequency wand (Saphyre II Ablation Probe with suction, 90°; Smith & Nephew). A sequential examination is performed in the peripheral compartment. During the procedure, the viewing portal is alternated for enhanced exposure.
Our first concern is to expose the “tip of the iceberg” of the larger osteochondroma, and because of its size, some degree of capsulectomy is inevitable (Fig 3). During this step, it is fundamental to delineate both lesions with the help of radiofrequency. After good visualization is obtained, samples are taken for pathologic analysis. Routinely, the medial synovial fold is used as a landmark for the medial resection limitation and as a model for re-creation of the anatomic femoral contour. Femoral bone resection is initiated, beginning at the anterior lesion, with a burr (5.5-mm-long Abrader; Smith & Nephew) (Fig 3). Because of the bleeding bone, it is necessary to alternate the burr with radiofrequency. During the procedure and after some anterolateral osteochondroma resection, the anterolateral portal is established as a second working portal with the goal of obtaining better access to the lateral and posterolateral head and neck area to complete the resection (Fig 4). At this time, internal rotation of the hip and the use of a switching stick to push the lateral capsule can be very helpful to increase the observation field. Slight traction is useful in the resection of the proximal part of the larger osteochondroma, diminishing the risk of damage to the labrum because of its proximity.
Fig 3.
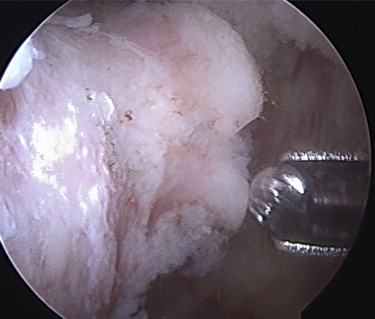
Arthroscopic view showing osteochondroma identification and resection.
Fig 4.
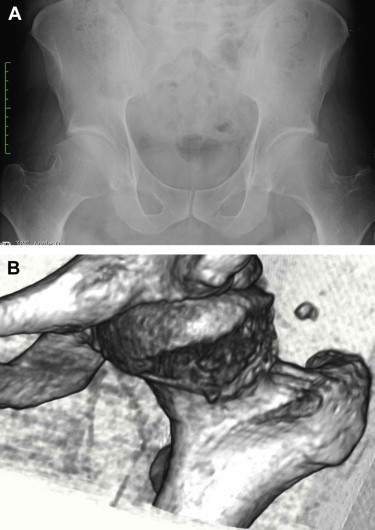
(A) Postoperative radiograph and (B) computed tomography scan showing complete resection of tumors.
For inspection of the central compartment, the portals are changed after traction is applied. With the help of an arthroscopic needle and by use of the same skin incision, the anterolateral portal is repositioned near the labrum with the assistance of a small capsulotomy and under arthroscopic visualization. In the same fashion, the mid-anterior portal is improved. Subsequently, the anterolateral portal is used as the viewing portal and the mid-anterior portal as the working portal. The labrum and articular cartilage are then evaluated for tissue quality. In our case an irreparable labral tear in the anterosuperior aspect of the acetabulum, reflecting the area of major impingement, was discovered. This poor-quality labrum was debrided until stabilization was achieved.
Discussion
Osteochondroma of the femoral neck is relatively uncommon and may cause impingement against the acetabular rim in a normally developed hip.2,3 It may also be associated with growth abnormalities of the hip, resulting in alterations of the length, width, and inclination of the femoral neck or acetabular dysplasia.2,3
The first case of arthroscopic resection of an osteochondroma was in the knee.4 Other reports have described open and arthroscopic resection of femoral neck osteochondromas.2,3 Siebenrock and Ganz2 reported 4 cases and performed open resection in all of them. Recently, Feeley and Kelly3 described 1 case with a solitary lesion; it had a smaller dimension, was not located in the head-neck transition, was associated with a labral tear, and was treated arthroscopically. Our case was more demanding because of the number of lesions and the size of the larger osteochondroma, imposing difficulties that could have led to open surgery in many centers. FAI was verified intraoperatively in our patient, and this led to a labral tear at the site of maximal impingement. In accordance with Siebenrock and Ganz, as well as Feeley and Kelly, we believe there was significant evidence that the labral tear was caused by the tumors.
Until this case, we frequently initiated arthroscopy in the central compartment, starting with the anterolateral portal once traction was applied. This case, in association with a literature revision,5,6 gave us the possibility to take into account the advantages of a peripheral-compartment approach to hip arthroscopy. As in other procedures and after some experience, we improved our technique as described by Dienst et al.,5,6 namely beginning with the proximal anterolateral portal as the viewing portal and subsequently establishing the anterior and anterolateral portals. When labral repair is necessary, the mid-anterior portal is normally used for anchor placement.
Although the size and location of an osteochondroma could lead to open surgery, hip arthroscopy is exceeding its limits day after day, showing several advantages over surgical hip dislocation in the management of FAI and intra-articular pathology.
Footnotes
The authors report the following potential conflict of interest or source of funding: P.D. receives support from Smith & Nephew, Biomet.
Supplementary Data
Left hip arthroscopy. The patient had 2 intra-articular osteochondromas with an anterolateral labral tear. Resection of the tumors and debridement of the labrum were performed.
References
- 1.Florez B., Mon Florez B., Monckeberg J., Castillo G., Beguiristain J. Solitary osteochondroma long-term follow-up. J Pediatr Orthop B. 2008;17:91–94. doi: 10.1097/bpb.0b013e3282f450c3. [DOI] [PubMed] [Google Scholar]
- 2.Siebenrock K.A., Ganz R. Osteochondroma of the femoral neck. Clin Orthop Relat Res. 2002;394:211–218. doi: 10.1097/00003086-200201000-00025. [DOI] [PubMed] [Google Scholar]
- 3.Feeley B., Kelly B. Arthroscopic management of an intraarticular osteochondroma of the hip. Orthop Rev (Pavia) 2009;1:e2. doi: 10.4081/or.2009.e2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Takahashi M., Nishihara A., Ohishi T., Shiga K., Yamamoto K., Nagano A. Arthroscopic resection of an intra-articular osteochondroma of the knee in the patient with multiple osteochondromatosis. Arthroscopy. 2004;20(suppl 2):28–31. doi: 10.1016/j.arthro.2004.04.012. [DOI] [PubMed] [Google Scholar]
- 5.Dienst M., Gödde S., Seil R. Hip arthroscopy without traction: In vivo anatomy of the peripheral hip joint cavity. Arthroscopy. 2001;17:924–931. doi: 10.1053/jars.2001.25342. [DOI] [PubMed] [Google Scholar]
- 6.Dienst M. Peripheral compartment approach to hip arthroscopy. In: Sekiya JK, Safran MR, Ranawat AS, Leuning M, eds. Techniques in hip arthroscopy and joint preservation surgery. Philadelphia: Elsevier Saunders, 2011;105-112.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Left hip arthroscopy. The patient had 2 intra-articular osteochondromas with an anterolateral labral tear. Resection of the tumors and debridement of the labrum were performed.