

Abstract
Background:
Age is an essential factor in establishing the identity of a person. Teeth are one of the most durable and resilient part of skeleton. Gustafson (1950) suggested the use of six retrogressive dental changes that are seen with increasing age.
Aim:
The aim of the study was to evaluate the results and to check the reliability of modified Gustafson's method for determining the age of an individual.
Materials and Methods:
Total 70 patients in the age group of 20-65 years, undergoing extraction were included in this present work. The ground sections of extracted teeth were prepared and examined under the microscope. Modified Gustafson's criteria were used for the estimation of age. Degree of attrition, root translucency, secondary dentin deposition, cementum apposition, and root resorption were measured. A linear regression formula was obtained using different statistical equations in a sample of 70 patients.
Results:
The mean age difference of total 70 cases studied was ±2.64 years. Difference of actual and calculated age was significant and was observed at 5% level of significance, that is, t-cal > t-tab (t-cal = 7.72). P < 0.05, indicates that the results were statistically significant.
Conclusion:
The present study concludes that Gustafson's method is a reliable method for age estimation with some proposed modifications.
Keywords: Age determination, modified Gustafson's criteria, physiological changes of teeth
Introduction
Estimation of age at death and determination of sex of the victim or remains are important factors in the identification of an individual in forensic odontology. Teeth are among the most reliable tools in the process of identification of age. Teeth are one of the most durable parts of our body, which can withstand more assaults than any other part of the body. This is particularly useful in the identification of bodies in mass disasters and natural calamities.[1]
Teeth had been used in the identification of individuals throughout history. It is more significant in the present day world to identify missing, dead, murdered, or killed persons in accidents. The identification of the corpses, mutilated bodies, is of importance from social, emotional, and medicolegal aspects.
The stages of development can be considered as one of the most dependable indicators in estimation of age of the person. Developmental stages of dentition and craniofacial skeleton are well established, and any disturbance during this period produces changes in these tissues and serve as lifelong permanent record. Even after complete development of dentition and craniofacial skeleton, certain physical and biological changes takes place which aid in the age estimation.
Dental age estimation can be divided in to two periods in life. The first period is when the teeth are developing in jaws up to 20 years. Later, when all teeth are fully formed, regressive age-related changes might be used as a scientific method. Age can be estimated in children and in adolescents by means of development and eruption of deciduous and permanent teeth up to 14 years. After the age of 14 years, the third molar is the only remaining tooth which is still developing; and consequently, dental age estimation methods have to rely on the development of this tooth until the age of 20. After this period, age determination is mainly done by visual examination, radiographic methods,[2,3] and structural changes in teeth and by means of biochemical methods.[4]
Scientific methods must rely upon regressive age changes such as attritions, loss of periodontal attachment, and secondary dentin formations. Such parameters are partly influenced by function and also by pathologic process and are thus for less accurate compared to the developmental stages of the teeth.[1]
The first scientific technique for age estimation in adults was presented by Gustafson {1950}. It was based on longitudinal sections of teeth cut through the central area. The technique consisted in attributing scores from 0-3 for the presence and amount of age-related changes such as attrition, periodontal ligament retractions, secondary dentin formations, root translucency, and root resorption. The scores were added and a regression analysis with age was performed.[5]
The main aim of this study was to apply modified Gustafson's method and to evaluate the reliability of this method for age estimation.
Materials and Methods
The present work was undertaken in the Department of Oral and Maxillofacial Pathology, D.J. College of Dental Sciences and Research, Modinagar (UP).
The sample group comprised of extracted teeth from individuals in the age group of 20-65 years. The teeth were obtained after preextraction examination of the patient by the researcher in the Department. However, some teeth extracted from individuals of selected age group in private dental clinics in the absence of the researcher were also included in the study. In such cases, the preextraction evaluation of the patient was not feasible, and hence was not done. Teeth with caries excluded from the study. The actual age of the patient in each case was recorded [Table 1].
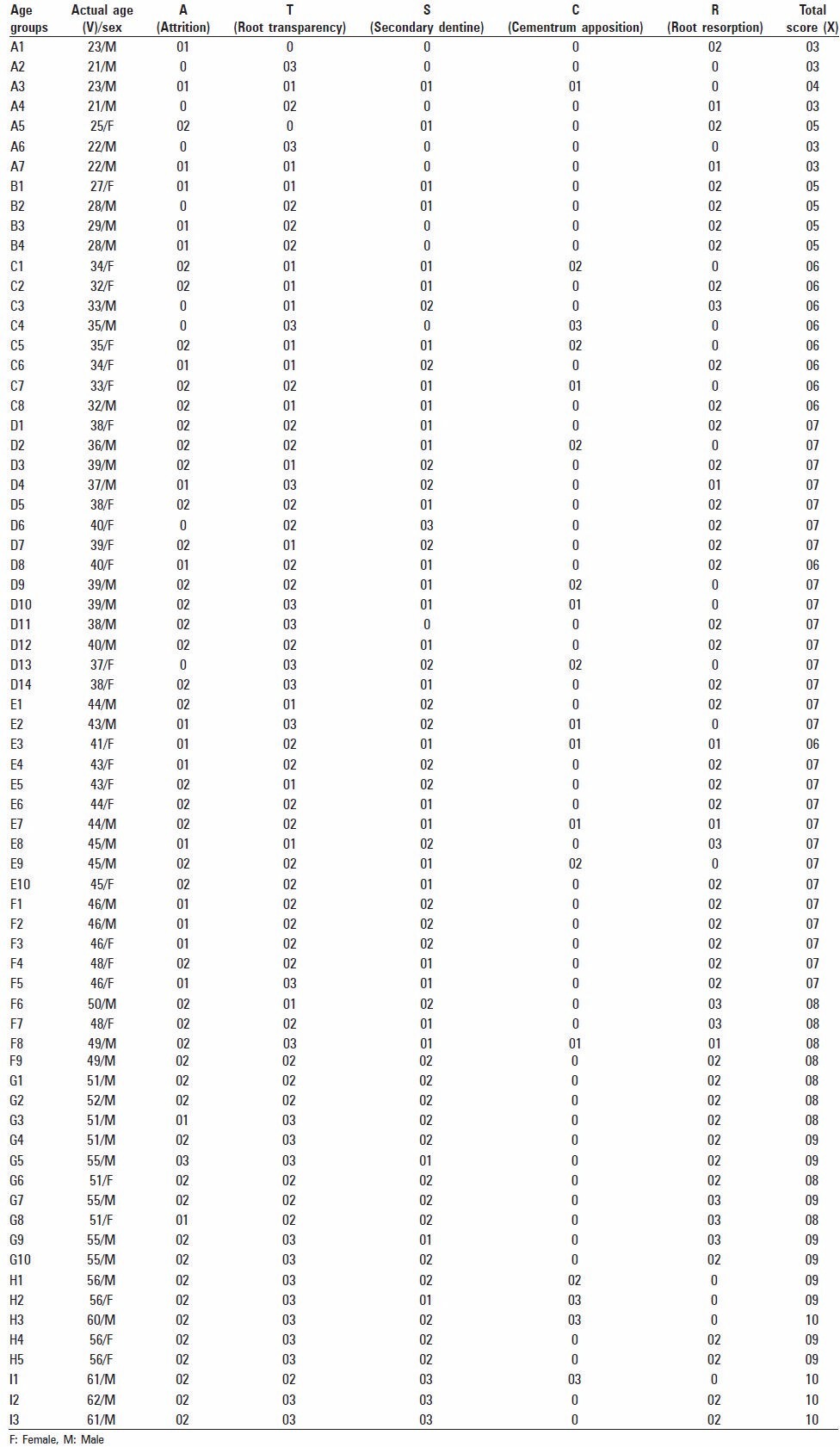
Table 1.
Age range of the cases studied
The following parameters were evaluated:
Degree of attrition
Degree of root transparency
Degree of secondary dentin deposition
Cementum apposition
Root resorption
The extracted teeth were preserved in separate vials containing 10% neutral buffered formalin solution. The degree of attrition was recorded by visual inspection and modified while reading the section microscopically.
The extracted teeth were prepared for examination by first grinding with lathe and then hand grinding using two Arkansas stone, one rough, and the other fine. Grinding was done first on the rough stone by making approximately equal grinding movements on either side so as to reach the center of the tooth.
At the thickness of 1 mm, the section was held over printed material such that the printing could be read through the section and the grading of root transparency was noted.
The grinding was carefully continued on the fine Arkansas stone up to 0.25 mm thickness. Finally, the cleaned and dried ground sections were mounted on glass slide with the code number marked on it. Then the extent of secondary dentine deposition, cementum apposition, and root resorption were recorded under low power microscope (×4).
The thickness of Cementum was measured by using Motic 2.0 Image Analysis Software. Cementum thickness of 150-200 μ was recorded as normal.
The various parameters were recorded using Gustafson's criteria as shown below. The allotment of four points (0, 1, 2, and 3) to all the parameters evaluated according to degree of change as per Gustafson's method.[6]
Attrition
A0 – No attrition
A1 – Attrition limited to enamel level
A2 – Attrition limited to dentin level [Figure 1]
Figure 1.
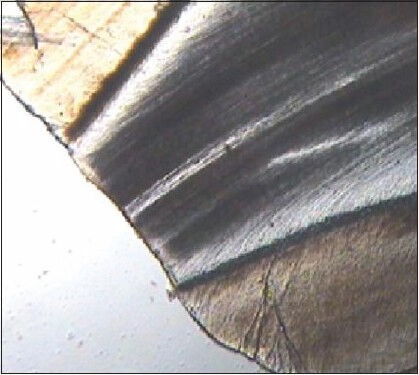
A2-Attrition extending to dentin
A3 – Attrition up to pulp cavity.
Periodontal disease
P0 – No obvious periodontal disease
P1 – Beginning of periodontal disease but no bone loss
P2 – Bone loss more than one-third of the root
P3 – Bone loss more than two-third of the root.
Secondary dentin
S0 – No secondary dentin formation
S1 – Secondary dentin up to upper part of pulp cavity [Figure 2]
Figure 2.

S1- Secondary Dentine upto upper part of pulp cavity
S2 – Secondary dentin up to two-third of the pulp cavity
S3 – Secondary dentin of entire pulp cavity.
Root transparency
T0 – No transparency
T1 – Beginning of transparency
T2 – Transparency more than one-third of the apical root
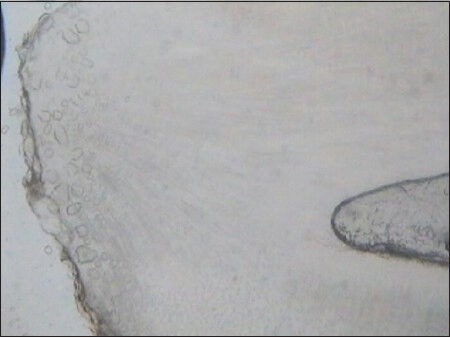
T3 – Transparency more than two-third of the apical root [Figure 3].
Figure 3.
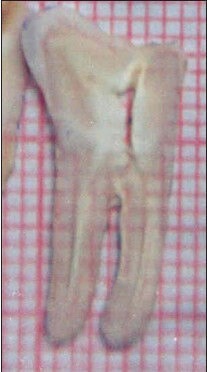
T3-Transparency more than two-third of the apical root
Cementum apposition
C0 – Normal cementum
C1 – Thickness of cementum but normal [Figure 4]
Figure 4.
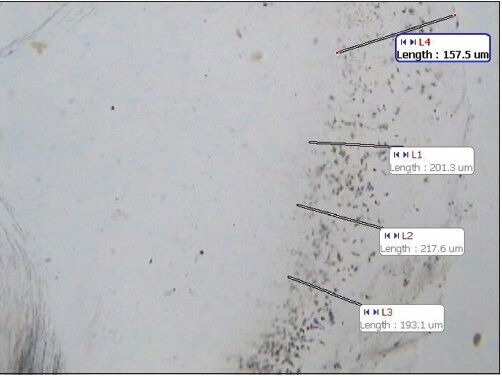
C1-Thickness of cementum, but more than normal
C2 – Abnormal thickness of cementum near the apex of the root
C3 – Generalized abnormal thickness of cementum throughout the apex of the root.
Root resorption
R0 – No resorption
R1 – Spotted resorption
R2 – Resorption limited to cementum
R3 – Extensive resorption of cementum and dentin both [Figure 5].
Figure 5.
R3-Extensive resorption of the cementum and dentin both
The parameter involving periodontal status was not considered for the study because the radiographic evaluation of major sample size could not be carried out.
After collecting the data and calculating the total score, estimated age was calculated by using the linear regression formula.[7]
A graph was plotted with actual age on one side and total scores on other side and regression formula was obtained using different statistical equations.
Yc = a + bx
Where, Y = estimated age
X = sum of total points recorded
a and b = coefficients calculated by statistical analysis
Results
The sample group comprised of extracted teeth from the individuals of age group 20-65 years. The selected teeth were prepared for examination by hand grinding using two Arkansas stones, one was rough, and other was fine. The cleaned and dried ground sections were mounted on glass slide and examined under the low power field of a light microscope.
The four-point allotment system of the Gustafson's criteria was used to record the degree of secondary changes in the teeth and total score of each case were obtained [Table 2].
Table 2.
Actual age and points allotted to Gustafson's criteria and total score (X)
The points allotted to the 70 cases were plotted graphically against the corresponding known ages of the cases. The scatter diagram prepared from the data showed a definite increase in the values of the points with increasing age. Then using the different statistically equations, the following findings were calculated; and from the relationship between the sum values of secondary changes and the known ages, the regression line was drawn as shown in Graphs 1 and 2.
Graph 1.
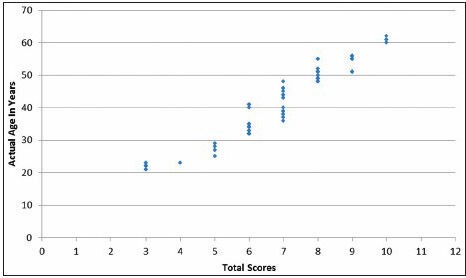
Scatter diagram between actual age and total score
Graph 2.
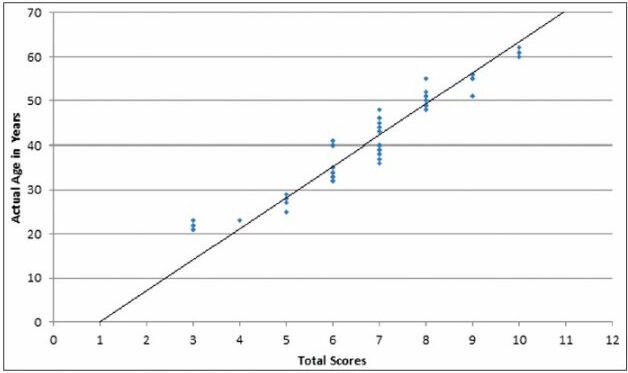
Scatter diagram with regression line between actual age and total score
The regression equation Yc = a + bx was calculated from following equations:
(i) EY = Na + bEx
(ii) EXY = aEx + bE× 2
Where X = average sum values of the degree of secondary changes of each case, Y = actual age in years, N = total number of cases studied, Yc = calculated age; and thus the regression equation became Yc = 0.27 + 6.07x
The other results were also obtained:
Regression coefficient (b) was 6.07 and coefficient of correlation was calculated from the equation:
Standard deviation from the regression line (Syx) was ±2.86 years, which was calculated from the equation:
The average point values, calculated ages, and difference between actual age and calculated age in each case were calculated [Table 3]:
Table 3.
Actual age (Y), total score (X), calculated age (Yc) and age difference between actual and calculated age
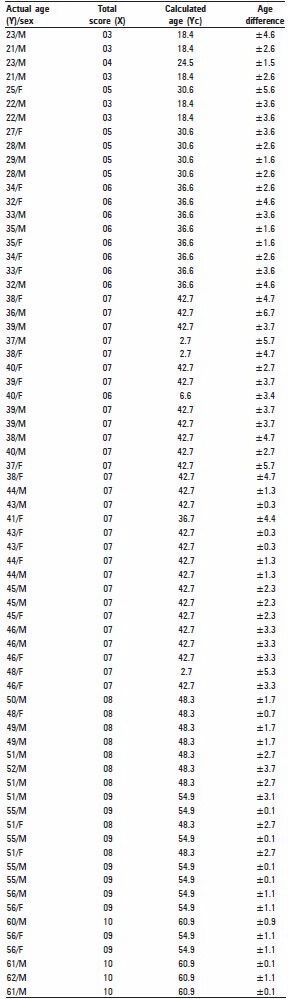
The mean age difference of total 70 cases studied was ± 2.64 years.
By using “paired t-test of significance” to test the significant difference in the mean difference of actual and calculated age was significant and was observed at 5% level of significance, that is, t-cal > t-tab (t-cal = 7.72). P < 0.05, indicates that the results were statistically significant.
The age difference between actual and calculated age of each case was observed as shown in Graph 3.
Graph 3.
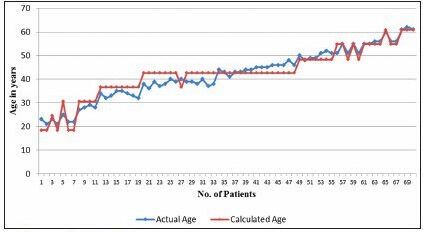
Comparison between actual and calculated age
In 44.3% of total cases studied, the error came within 1.1-3 years, in 32.80% of cases the error came within 3.1-5 years, in 15.70% of the cases the error came within 0-1 years, and in 7.20% of the cases the error came above 5 years as shown in Graph 4.
Graph 4.
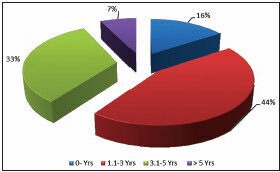
Distribution of cases as per age difference between actual and calculated age
Discussion
Age is one of the essential factors in establishing the identity of a person. Age estimation from teeth is a field in forensic odontology which is of great interest in the identification of a person. It has been shown that the state of the teeth has closer correlation with age than any other hard tissue of the body. Age can be estimated in children and in adolescent by means of development and eruption of deciduous and permanent teeth up to 14 years. After the age of 14 years, the third molar is the only remaining tooth which is still developing and consequently dental age estimation methods have to rely on the development of this tooth until 20 years of age. After this period, age determination is mainly done by visual examination, radiographic methods, and structural changes in teeth; and by means of biochemical methods.[1]
The Gustafson's method is the most popular age estimation method being used since 1950. He used six retrogressive changes in teeth, namely attrition, secondary dentin deposition, periodontal status, root transparency, cementum apposition, and root resorption.[3]
This technique was modified in many ways by several investigators to get optimum results.[8]
In our study, only five retrogressive changes were taken into consideration excluding periodontal status assessment. The extent of periodontal disease was not assessed. Since the study group comprised of those teeth that were already extracted at various private dental clinics, the radiographic evaluation of these samples could not be carried out. Hence, the parameter involving periodontal status was not considered for the study.
The sample group comprised of extracted teeth from individuals in the age group of 20-65 years. The extracted teeth were prepared for examination and the extent of secondary dentine deposition, cementum apposition, and root resorption were recorded under low power microscope and ranked them on an arbitrary scale, allotted 0-3 points according to the degree of secondary changes.
In our study, “paired t-test of significance” was used to test a significant difference in the mean difference between actual and calculated age. The mean age difference between actual and calculated age of total 70 cases studied was ±2.64 years.
It was observed significant at 5% level of significance, that is, t-cal (t-cal = 7.72) was greater than t-tab (t-tab = 2.101). P < 0.05, indicates that the results were statistically significant. In 44.30% of total cases studied, the average error came within 1.1-3 years; in 32.80% of the cases the error came within 3.1-5 years; in 15.70% of the cases the error came within 0-1 years, and in 7.20% of the cases the error came above 5 years.
The mean age difference between actual and calculated age was less as compared to the Gustafson's original work which was ±3.63 years. The mean age difference between actual and calculated age was significant, but the difference was less as compared to those reported by previous workers like Dalitz[9] in 1962; Miles[10] in 1963; Bang and Ramm's[8] in 1970; Johanson[11] in 1971; Pillai and Bhaskar,[12] in 1974; Singh and Mukharjee[7] in 1985; and Lucy et al.,[13] in 1996 except the work done by Kashyap and Rao[14] in 1990 and Singh and Gorea,[6] in 2004 [Table 4].
Table 4.
Comparison of mean age difference between actual and calculated age of our study with various other previous studies

The difference was more than the study done by Kashyap et al., (1990), where the average error was ±1.59 years which was attributed to using objective measurements and excluding the criteria like root resorption and periodontal assessment. All changes were scored as index values.[15]
In our study the difference between estimated and actual age could have been reduced by considering some more factors like the inclusion of more precise objective measurements of secondary changes in teeth rather than scored in an arbitrary manner and considering the similar parameters as suggested by Kashyap et al., in 1990.
The regression and correlation coefficients in this presented work and those of Gustafson' method was more or less in the same positive trend. The value of correlation coefficient (r) in this present work was 0.99, which was higher; and established the good correlation between actual age and total scores of each selected teeth. The regression coefficient in this presented work was 6.07, which brought about in the significant slope of the regression line. The standard deviation (SD) obtained in this work was ±2.86 years.
There is a distinct possibility of an error in recording the real age of the patients due to low literacy level and improper maintenance of birth registers and other records of the patients. This may be a contributory factor in the difference between actual age and calculated age in our study.
The modifications proposed in our study do not contradict the Gustafson's method; but complement it because of exclusion of one parameter, that is, periodontal status assessment which gave the better results than previous studies except the work done by Lopez et al., in 1993.[15]
Various pathological conditions and quality of oral hygiene influence adversely the different dental features which may affect the scoring of secondary changes in teeth. In Gustafson's method, no consideration was given to changes in teeth due to pathological conditions, whereas in our study some modifications in Gustafson's method like exclusion of one parameter, that is, periodontal status assessment and measuring cementum thickness more precisely by using Motic 2.0 Image Analysis computer software system was performed.
This suggests that the Gustafson's method is a reliable method with some modifications in methodology and considering other factors related to all parameters which can alter the scores. Other relevant factors should be considered and all the parameters should be precisely recorded to achieve the correct age of an individual.
Conclusion
The present study concludes that regressive alterations of teeth can be used for estimation of age which helps in identification of the corpses; mutilated bodies; and is of importance for social, emotional, and medicolegal aspects. We also conclude that Gustafson's method is a reliable method for age estimation with some proposed modification.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
References
- 1.Dayal PK. Text book of forensic odontology. 1st ed. Paras Medical Publishers Publication; 1998. pp. 1–4. [Google Scholar]
- 2.Kuilman L. Accuracy of two dental and one skeletal age estimation method on Swedish adolescents. Forensic Sci Int. 1995;75:225–36. doi: 10.1016/0379-0738(95)01792-5. [DOI] [PubMed] [Google Scholar]
- 3.Kvaal KI. Age estimation of adults from dental radiographs. Forensic Sci Int. 1995;74:175–85. doi: 10.1016/0379-0738(95)01760-g. [DOI] [PubMed] [Google Scholar]
- 4.Mornstad H, Pfeiffer H, Teivens A. Estimation of dental age using HPLC technique to determine the degree of aspartie acid racemization. J Forensic Sci. 1994;39:1425–31. [PubMed] [Google Scholar]
- 5.Gustafson G. Age determinations on teeth. J Am Dent Assoc. 1950;41:45–54. doi: 10.14219/jada.archive.1950.0132. [DOI] [PubMed] [Google Scholar]
- 6.Singh A, Gorea RK. Age estimation from the physiological changes of teeth. JIAFM. 2004;26 ISSN 0971-0973. [Google Scholar]
- 7.Singh AM, Mukharjee JB. Age determination from teeth of bangalee subjects by following Gustafson's method. JIAFS. 1985;24:1–4. [Google Scholar]
- 8.Bang G, Ramm E. Determination of age in humans from root dentine transparency. Acta Odontol Scand. 1970;28:3–35. doi: 10.3109/00016357009033130. [DOI] [PubMed] [Google Scholar]
- 9.Dalitz GD. Age determination of adult human remains by teeth examination. J Forensic Sci. 1963;21:11–21. [Google Scholar]
- 10.Miles AE. The dentine in the assessment of individual age in skeletal material. In: Brothwell DR, editor. Dental Anthropology Synopsis of the Society For the Society For the Study of Human Biology. Vol 6. Oxford, London, New York, Paris: Pergamon Press; 1963. pp. 191–209. [Google Scholar]
- 11.Johanson G. Age determination from human teeth. Odont Revy. 1971;22(Suppl 21):40–126. [Google Scholar]
- 12.Pillai PS, Bhaskar GR. Age estimation from teeth using Oustafson's method-a study in India. Forensic Sci. 1974;3:135–41. doi: 10.1016/0300-9432(74)90022-3. [DOI] [PubMed] [Google Scholar]
- 13.Lucy D, Aykroyd RG, Pollard AM, Solheim T. A Bayesian approach to adult human age estimation from dental observations by Johanson's age changes. J Forensic Sci. 1996;41:189–94. [PubMed] [Google Scholar]
- 14.Kashyap VK, Koteswara Rao NR. A modified Gustafson method of age estimation from teeth. Forensic Sci Int. 1990;47:237–47. doi: 10.1016/0379-0738(90)90293-8. [DOI] [PubMed] [Google Scholar]
- 15.Lopez Nicolas M, Morales A, Luna A. Morphometrie study in age calculation. J Forensic Odontostomatol. 1993;11:1–8. [PubMed] [Google Scholar]