

Abstract
Delleman syndrome is an unusual entity, characterized by ocular cysts or microphthalmia, focal dermal anomalies and cerebral malformations. In the following article, we carry out a review of the disease and we present the case of a patient with microphthalmos and palpebral coloboma. As we could not put orbital expanders at an early stage, we performed reconstructive surgery.
Keywords: Oculocerebrocutaneous syndrome, orbit, plastic surgery
The oculocerebrocutaneous syndrome is an unusual entity, given by a spontaneous mutation which affects the eye, brain and skin.
It was described by Delleman in the year 1981 and since then, nearly 40 cases have been reported.
In the following article we present a case, reviewing the main features of the disease.
Case Report
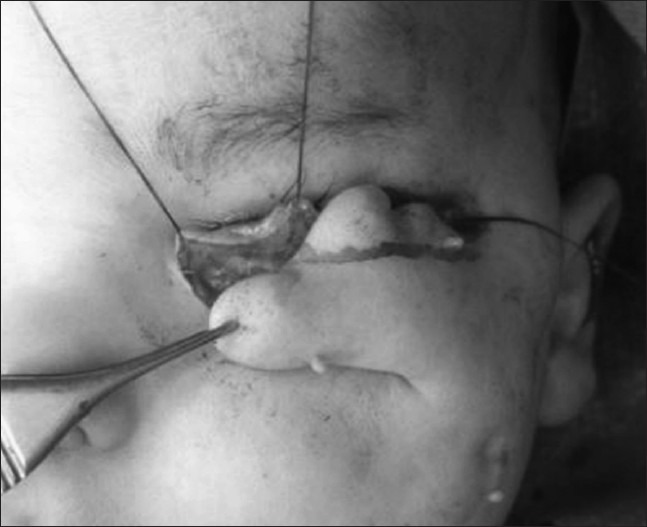
A male newborn patient was evaluated for genetic syndrome. He presented microphthalmos in the right eye and coloboma in the lower lid [Fig. 1]. The left eye had no anomalies.
Figure 1.

Newborn with Delleman Syndrome
He had a lesion in the scalp compatible with bilateral aplasia cutis, and, in the periocular region there were multiple mobile cutaneous appendages, as well as pits on the cheek and appendages on nostrils. In the lumbar region, he had a small lesion of aplasia cutis surrounded by hair growth.
MRI showed an encephalic trunk of dysmorphic aspect, with slight hypoplasia of the central vermis [Fig. 2].
Figure 2.

MRI showed an encephalic trunk of dysmorphic aspect
We performed an echocardiogram, which showed no structural cardiopathy and an abdominal renal ultrasound, with no anomalies. Genitalia, hands and feet were normal. He did not have convulsions.
He was the second child of a non-consanguineous couple. Both parents were 32, Argentinean, teachers, and healthy. The sister was 1 year and 9 months old, and she had unilateral microtia. There were no miscarriages, or any other data of importance in the genealogy. The pregnancy was controlled, with no complications and teratogenic exposure. Newborn in term (39 weeks), vaginal delivery with adequate weight for the gestational age (3200 g). Karyotype 46 normal XY.
Given the poor palpebral support, we could not put orbital expanders.
We waited for 4 months, when the hemoglobin had improved and he acquired the necessary conditions to undergo surgery, and we performed reconstructive surgery of the eyelid. We used a cutaneous appendage as a flap, to give shape to the lower lid [Figs. 3 and 4]. In this way, we created an adequate cavity to put orbital expanders [Fig. 5].
Figure 3.

Eyelid reconstruction
Figure 4.
Forming the flap
Figure 5.

Postoperative
Discussion
As Delleman described, the syndrome is characterized by the presence of an orbital cyst or microphthalmia, associated with palpebral colobomas, focal dermal malformations and cerebral anomalies.[1,2,3] Some more severe forms present hydrocephaly, anophthalmos, palatine fissure or cleft palate.
In the skin, you can find areas of focal aplasia or hypoplasia, even alopecia. The formation of cutaneous appendages in the periocular region is a characteristic.[4,5]
Neurological anomalies can be manifested by convulsions and psychomotor development disorders. These include polymicrogyria, ventricular system malformations, cerebral or cerebellum cysts and agenesia of the corpus callosum. Malformations of the midline and mesencephalon are pathognomonic.[4,5,6]
There is no determined etiology yet, but there is a hypothesis that suggests a sporadic mutation in the fifth or sixth week of development. It states that it is associated with a somatic mosaicism, which compromises the development of the ectodermal structures.[7] Other authors suggested that there would be a relation with the chromosome X, given the higher prevalence of this syndrome in men. Also, based on the appearance of malformations in structures of the midline and mesencephalon, it could be due to an early anomaly in the development, when the organizing center is establishing the limits between the mesencephalon and the brain.[6]
Delleman syndrome usually shares some characteristics with certain syndromes such as Goldenhar or Goltz. The first one, also known as oculo-auriculo-vertebral syndrome, is characterized by the presence of a dermoid cyst and auditory and vertebral anomalies. The second one is associated to microphthalmia, dermic hypoplasia, polysyndactyly and bad dentition.[5,8,9] These kind of syndromes can be differentiated by the pattern of cerebral malformations. The ones in the midline and mesencephalon are characteristic of Delleman syndrome.[6]
Our case presented a coloboma of the lower lid, which hindered the early placement of orbital expanders. The importance of putting expanders in an early stage is known for the correct orbito-facial growth. The normal size of an eye at birth is 70% of the adult, and by the time it is 3 months, it is 40%. However, the size of the face evolves quickly; by the time it is 3 months, which presents 40% of the adult size, by the age of 2 it is 70%, and at 5.5 years of age it is 90%. This development in an anophthalmic or microphthalmic cavity is torpid, which is why the early placement of expanders is important, as well as its timely replacement as the orbital cavity develops.[10,11]
Acknowledgment
Patricia Adduci for English translation and manuscript preparation.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
References
- 1.Delleman JW, Oorthuys JW. Orbital cyst in addition to congenital cerebral and focal dermal malformations: A new entity? Clin Genet. 1981;19:191–8. doi: 10.1111/j.1399-0004.1981.tb00695.x. [DOI] [PubMed] [Google Scholar]
- 2.Delleman JW, Oorthuys JW, Bleeker-Wagemakers EM, ter Haar BG, Ferguson JW. Orbital cyst in addition to congenital cerebral and focal dermal malformations: A new entity. Clin Genet. 1984;25:470–2. doi: 10.1111/j.1399-0004.1984.tb02019.x. [DOI] [PubMed] [Google Scholar]
- 3.Saatci AO, Arikan G, Saatci P, Saatci Y, Kavukcu S. Oculocerebrocutaneous syndrome. J Pediatr Ophthalmol Strabismus. 2008;45:181–3. doi: 10.3928/01913913-20080501-19. Arora V, Kim UR, Khazei HM Delleman Oorthuys syndrome: ‘Oculocerebrocutaneous syndrome’ Indian J Ophthalmol 2009;57:387-9. [DOI] [PubMed] [Google Scholar]
- 4.Patil SJ, Phadke SR. Delleman syndrome. Indian Pediatr. 2006;43:173–4. [PubMed] [Google Scholar]
- 5.Moog U, Jones MC, Bird LM, Dobyns WB. Oculocerebrocutaneous syndrome: The brain malformation defines a core phenotype. J Med Genet. 2005;42:913–21. doi: 10.1136/jmg.2005.031369. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Hoo JJ, Kapp-Simon K, Rollnick B, Chao M. Oculocerebrocutaneous (Delleman) syndrome: A pleiotropic disorder affecting ectodermal tissues with unilateral predominance. Am J Med Genet. 1991;40:290–3. doi: 10.1002/ajmg.1320400308. [DOI] [PubMed] [Google Scholar]
- 7.Sujit Kumar GS, Haran RP, Rajshekhar V. Delleman syndrome with Goldenhar overlap. J Pediatr Neurosci. 2009;4:53–5. doi: 10.4103/1817-1745.49115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Roszkowski M, Dabrowski D. Encephalo-cranio-cutaneous lipomatosis (ECCL) :Haberland syndrome. A case report with review of the literature. Neurol Neurochir Pol. 1997;31:607–13. [PubMed] [Google Scholar]
- 9.Chen D, Heher K. Management of the anophthalmic socket in pediatric patients. Curr Opin Ophthalmol. 2004;15:449–53. doi: 10.1097/01.icu.0000137855.45573.02. [DOI] [PubMed] [Google Scholar]
- 10.Ragge NK, Subak-Sharpe ID, Collin JR. A practical guide to the management of anophthalmia and microphthalmia. Eye (Lond) 2007;21:290–300. doi: 10.1038/sj.eye.6702858. [DOI] [PubMed] [Google Scholar]
- 11.Farkas LG, Posnick JC, Hreczko TM, Pron GE. Growth patterns in the orbital region: A morphometric study. Cleft Palate Craniofac J. 1992;29:315–8. doi: 10.1597/1545-1569_1992_029_0315_gpitor_2.3.co_2. [DOI] [PubMed] [Google Scholar]