

Abstract
Introduction:
Recurrent aphthous stomatitis (RAS) is an unfortunately most common disease occurring in oral cavity. Although the lesion is usually self-limited, its painful presentation, high frequency of occurrence, and multifactorial etiology leads to significant morbidity. So, an efficient therapeutic strategy is needed to provide relief to the patients.
Aim:
To assess and compare the efficacy of Curcumin with Triamcinolone acetonide in the gel form in treatment of minor RAS.
Materials and Methods:
As a randomized clinical trial, 60 patients of either sex with clinically diagnosed RAS were randomly divided into 2 groups-Curcumin gel group (Group I) and Triamcinolone Acetonide gel group (Group II). Patients in either group were asked to apply the gel three times a day on each ulcer. Assessment of efficacy of gel was done on the basis of time required for regression in pain, size, and number of the ulcers.
Results:
The results showed significant difference in size, pain, number, and duration of ulcers in Group I and Group II within a period of 7 days. However, no significant difference was noted in both the groups in the treatment of RAS. To evaluate the efficacy, Mann-Whitney U test was used and statistical analysis was done using Statistical Package for the Social Sciences (SPSS) 19 software.
Conclusion:
Curcumin has strong antioxidant, with anti-inflammatory, immunomodulatory and analgesic properties, which according to the results obtained from the present study, can be used as an effective alternative to steroids in treatment of RAS.
Keywords: Curcumin, recurrent aphthous stomatitis, triamcinolone acetonide
INTRODUCTION
Recurrent aphthous stomatitis (RAS), commonly known as aphthous ulcer, is an unfortunately most common disease occurring in oral cavity. It is characterized by the development of painful, recurring solitary, or multiple ulcers in the oral cavity and upper throat. The ulcers are usually multiple, small, round, or ovoid, with circumscribed margins, having yellow or gray floors and are surrounded by erythematous haloes.[1]
RAS is classified into 3 types:
Minor RAS is also known as Miculiz's aphthae. Ulcers are usually less than 1 cm in size. Ulcers heal within 10-14 days without scarring.
Major RAS is also known as periadenitis mucosa necrotica recurrens or Sutton's disease. Ulcers exceed 1 cm in diameter. The ulcers persist for up to 6 weeks and heal with scarring.
Herpetiform ulceration is characterized by recurrent crops of multiple ulcers; may be up to 100 in number. These are small in size, measure 2-3 mm in diameter. Lesions may coalesce to form large irregular ulcers. These ulcers last for about 10-14 days.[1]
RAS is a multifactorial disease which can occur due to bacterial infections like infection with Streptococcus sanguis, immunologic abnormalities, nutritional deficiencies like iron, vitamin B12, folic acid deficiency, and certain precipitating factors like trauma, endocrine conditions, psychic, and allergic factors. Although the lesion is usually self-limited, its painful presentation, high frequency of occurrence, and multifactorial etiology leads to decreased quality of life and significant morbidity. So an efficient therapeutic strategy is needed to provide relief to the patients.[2,3,4]
Current treatment modalities include use of topical steroids like Triamcinolone acetonide gel, which is a fluoride synthetic corticosteroid. As corticosteroids are known to get absorbed systemically even on topical application, they can lead to certain adverse reactions. So nowadays, herbal medicines are gaining more attention due to their decreased side effects.[4,5,6]
Curcumin is a main pigment of principle spice in India, turmeric. It is bright yellow in color and is known from centuries for its strong antioxidant, antiseptic, antibacterial, anti-inflammatory, immunomodulatory, and analgesic properties. The anti-inflammatory properties of curcumin may be attributed to its ability to inhibit both biosynthesis of inflammatory prostaglandins which further blocks cyclooxygenase and lipooxygenase activity, thereby inhibiting prostaglandin leukotriene release and neutrophil function during inflammatory states.[7,8,9,10]
So, the aim of this study was to assess and compare the efficacy of Curcumin with Triamcinolone acetonide in the gel form in treatment of RAS.
MATERIALS AND METHODS
The study was a randomized, double blind, clinical trial and was carried out over a period of 6 months, from March 2013 to August 2013. After obtaining the written informed consent, 60 patients of either sex with clinically diagnosed minor RAS were selected from among the out patients visiting the Department of Oral Medicine and Radiology.
Patients willing to participate in the study and with clinically diagnosed minor RAS noticed within 2 days of development of ulcer were included in the study.
Patients between 13-66 years of age were included in the trial, if they presented with 1-5 minor recurrent aphthous ulcers of less than 48 hours duration. Patients were excluded from the study if the ulcers were present at inaccessible areas, if they had major RAS, traumatic ulcer, denture stomatitis or if they were suffering from any systemic illness. In order to minimize the effect of confounding variables in the psycho-physiological component of the study, the patients with any major illness in the past, or on any other topical or systemic medications were excluded from the study. Patients allergic to any constituents of gel used in the study, pregnant or lactating women were also excluded from the study. The trial was approved by the research and ethical committee at KLE's VKIDS, Belgaum, Karnataka.
Method of collection of data
Detailed case history, extraoral, and intraoral examination was performed on the patients, and 60 patients with clinically diagnosed minor RAS were selected for the study based on inclusion and exclusion criteria.
These 60 patients were randomly divided into two groups using computerized lottery method:
Group I 30 patients (Curcumin gel group)
Group II 30 patients (Triamcinolone Acetonide gel group)
The allocation sequence of the study and the examination of the patients were done by only one investigator in the department.
On day 0, patient was examined for number and size of ulcers and the pain score was noted [Figure 1]. Ulcer size was measured along its longest diameter using a sterile vernier caliper and the pain score was noted from 0-10, using the Visual Analogue Scale (VAS).
Figure 1.

Pre-treatment aphthous ulcer
Patients were asked to apply the gel three times a day on each ulcer after meals and not to consume food or water for half an hour after application of the gel. All patients were provided with same measuring applicator and were instructed about the quantity and method of gel application on the first appointment itself. Patients were examined on day 0, 3, 5, and 7 [Figure 2] to check for regression number and/or size of ulcer and any discomfort due to the gel. Pain score was noted daily by the patient.
Figure 2.

Post-treatment aphthous ulcer
Clinical estimation of ulcer
The response of treatment was assessed by quantitative measurement of diameter of ulcer using vernier caliper, at each follow-up visits by a single observer. The patients were instructed to note the pain score every morning on his/her record card as per the VAS.
Assessment of efficacy of gel was done on the basis of time required for regression in pain, size and number of the ulcer.
Details of Curcumin gel:
Curenext oral gel (Abbott Pharmaceuticals).
Per gram of gel contained 10 mg of curcuma longa extract.
Details of Triamcinolone Acetonide gel:
Kenacort oral paste (Abbott Pharmaceuticals).
The gel contains 0.1% triamcinolone acetonide.
Data was presented as mean ± standard deviation (SD) for quantitative variables with normal distribution and significance of difference was accepted at P < 0.05. Background and demographic data were summarized with descriptive statistics. To evaluate the efficacy, Mann-Whitney U test was used and statistical analysis was done using Statistical Package for the Social Sciences (SPSS) 19 software.
RESULTS
Total of 60 patients [Table 1] participated in the study and all patients completed the study protocol. No patient suffered from any allergic reaction to the gels used in the study for treatment of minor RAS. No significant difference was identified between patients randomly assigned to the group I or group II with regard to basic demographic data including age and gender; size and number of ulcers; and pain score on day 0.
Table 1.
Demographic statistics of study samples for both sexes

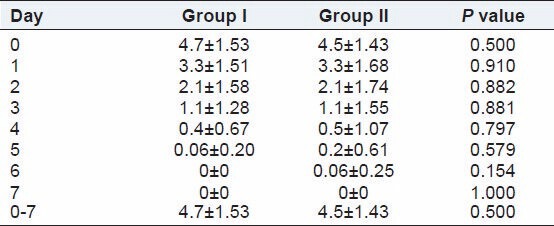
The reduction in pain was statistically significant in both the groups from day 0-day 7, respectively; but on comparison between group I and group II, no statistical significance was noted in the pain score. [Table 2]
Table 2.
Mean ± standard deviation of pain score in group I and group II, with their statistical significance expressed as P value
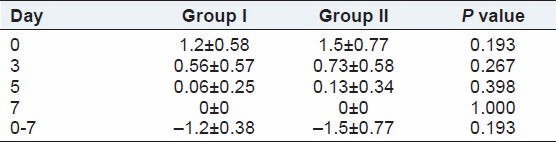
The reduction in size and number of ulcers were statistically significant in both the groups from day 0-day 7 (noted on day 0, 3, 5, 7), respectively; but on comparison between group I and group II, no statistical significance was noted in the size and number of ulcers. [Tables 3 and 4]
Table 3.
Mean ± standard deviation of size of ulcer in group I and group II, with their statistical significance expressed as P value
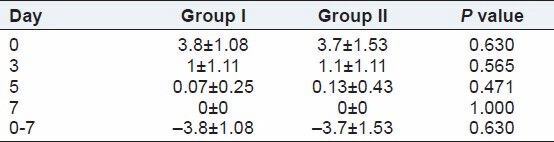
Table 4.
Mean ± standard deviation of number of ulcers in group I and group II, with their statistical significance expressed as P value
There was statistical significance in duration of ulcer in both the groups from day 0-day 7, respectively; but on comparison between group I and group II, no statistical significance was noted in the duration of ulcers. [Table 5]
Table 5.
Mean ± standard deviation of duration of ulcers in group I and group II, with their statistical significance expressed as P value

DISCUSSION
The multifactorial etiology of RAS and lack of effective treatment modality makes it a challenge for the dentist to relieve the patient from the morbidity associated with RAS. As the treatment of RAS aims at providing symptomatic relief for the patient, the goals of treatment include reduction in healing time of ulcer, decrease pain, size, and number of ulcers.[4,5,6] Current treatment modalities include use of systemic and topical steroids, cauterization, antibiotics, mouth rinses containing active enzymes, laser treatments, and combination therapy.[9]
As curcumin is known for its strong antioxidant, antiseptic, antibacterial, anti-inflammatory, immunomodulatory, and analgesic properties, a study was carried out to evaluate the therapeutic effect of viscous curcumin solution at 10% and 50%, on the healing of ulcer in patients with RAS showed a good percentage of complete healing of ulcer in patients with RAS.[11,12]
In 2012, an randomized placebo controlled trial was done using 2% curcumin gel in treatment of minor RAS, which showed that it is a well-tolerated effective antibacterial, anti-tumor agent with potent anti-inflammatory and analgesic properties.[13]
This study showed that there was significant difference between the pain score, size, number, and duration of ulcers from day 0-day 7 in both the groups, respectively. Statistical significance was not noted between all the parameters when both the groups were compared with each other. The results of this study, as consistent with other studies provide positive evidence that curcumin gel can be used as an effective and safer alternative to steroids in treatment of minor RAS.
CONCLUSION
The topical application of curcumin and triamcinolone acetonide gel showed similar efficiency in the treatment of minor RAS. The results obtained from the present study provide strong evidence that curcumin gel can be used as an effective and safer alternative to steroids in treatment of RAS.
ACKNOWLEDGEMENT
We acknowledge the guidance provided by all the staff of KLE VK Institute of Dental Sciences and the colleagues for their valuable input.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Preeti L, Magesh K, Rajkumar K, Karthik R. Recurrent aphthous stomatitis. J Oral Maxillofac Pathol. 2011;15:252–6. doi: 10.4103/0973-029X.86669. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Greenberg MS, Glick M, Ship JA. Burket's Oral Medicine. Vol. 11. Hamilton: BC Decker Inc; 2008. pp. 57–60. [Google Scholar]
- 3.Porter SR, Hegarty A, Kaliakatsou F, Hodgson TA, Scully C. Recurrent aphthous stomatitis. Clin Dermatol. 2000;18:569–78. doi: 10.1016/s0738-081x(00)00147-4. [DOI] [PubMed] [Google Scholar]
- 4.Ship JA. Recurrent aphthous stomatitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996;81:141–7. doi: 10.1016/s1079-2104(96)80403-3. [DOI] [PubMed] [Google Scholar]
- 5.Akintoye SO, Greenberg MS. Recurrent aphthous stomatitis. Dent Clin North Am. 2005;49:31–47. doi: 10.1016/j.cden.2004.08.001. [DOI] [PubMed] [Google Scholar]
- 6.Shashy RG, Ridley MB. Aphthous ulcers: A difficult clinical entity. Am J Otolaryngol. 2000;21:389–93. doi: 10.1053/ajot.2000.18872. [DOI] [PubMed] [Google Scholar]
- 7.Akram M, Shahab-Uddin, Ahmed A, Khan U, Hannan A, Mohiuddin E, et al. Curcuma longa and curcumin: A review article. Rom J Biol Plant Biol. 2010;55:65–70. [Google Scholar]
- 8.Chainani-Wu N. Safety and anti-inflammatory activity of curcumin: A component of turmeric (Curcuma Longa) J Altern Complement Med. 2003;9:161–8. doi: 10.1089/107555303321223035. [DOI] [PubMed] [Google Scholar]
- 9.Thorne R. Curcuma longa (Turmuric) Altern Med Rev. 2001;6:62–8. [PubMed] [Google Scholar]
- 10.Janson MD. Curcumine. Healthy Living. 2000;2:1–3. [Google Scholar]
- 11.Itsuki K, Tetsuya F, Teruo N, Toshihiko I, Keinosuke N. Therapeutic effect of curcumin chewable on aphthous ulcer and traumatic ulcer. Clin All-Round. 2006;55:204–8. [Google Scholar]
- 12.Al-Saffar MT. The therapeutic effect of viscous solution of curcumine in the treatment of recurrent aphthous stomatitis (RAS) Al-Rafidain Dent J. 2006;6:48–52. [Google Scholar]
- 13.Manifar S, Obwaller A, Gharehgozloo A, Boorboor Shirazi Kordi HR, Akhondzadeh S. Curcumin gel in treatment of minor aphthous ulcer: A randomized, placebo-controlled trial. J Med Plants. 2012;11:41. [Google Scholar]