

Abstract
Epidemiological, economic, and social forces have produced high levels of volatility in family and household structure for young people growing up in sub-Saharan Africa in recent decades. However, scholarship on the family to date has not examined the influence of this family instability on young people’s well-being. The current study employs unique life history calendar data from Western Kenya to investigate the relationship between instability in caregiving and early initiation of sexual activity. It draws on a body of work on parental union instability in the United States, and examines new dimensions of family change. Analyses reveal a positive association between transitions in primary caregiver and the likelihood of early sexual debut that is rapidly manifested following caregiver change and persists for a short period. The association is strongest at early ages, and there is a cumulative effect of multiple caregiver changes. The results highlight the importance of studying family stability in sub-Saharan Africa, as distinct from family structure, and for attention to dimensions such as age and recency.
Keywords: Family instability, Adolescence, Sexual behavior, Sub-Saharan Africa, Caregiving
Introduction
Young people transitioning to adulthood in contemporary sub-Saharan Africa have grown up amidst the AIDS epidemic, economic and political fluctuations, and rapid urbanization (National Research Council and Institute of Medicine 2005; United Nations 2007). The mortality, morbidity, and migration accompanying this combination of forces have in turn engendered disruption and volatility in family and household structures. Young people in the region today are exceedingly likely to have experienced changes in the presence of parents and other caregivers over the course of their early lives. Although these changes occur over time, research to date on the relationship between family situation and African youth well-being has been almost wholly cross-sectional.
Drawing on a life course perspective, this study takes as its starting point the dynamic nature of family structure (Shanahan 2000; Uhlenberg and Mueller 2003). I build on an existing body of work on family instability developed with regard to child and adolescent well-being in the United States. This scholarship suggests that changes in family situation (typically defined as changes in parental partnership status) in and of themselves produce stresses for young people and their parents, as well as needs for adjustment, that are distinct from family structure (Brown 2010; Cavanagh and Huston 2006; Fomby and Cherlin 2007; Wu 1996). I extend this framework to sub-Saharan Africa, and in particular to Kisumu, Kenya, the third largest city in Kenya and capital of Nyanza Province.
Using monthly life history calendar data that allow for an examination of caregiver stability and change for the first time in an African setting, I investigate the influence of family instability on early initiation of sexual activity. Early sexual debut has been associated with various poor socioeconomic and reproductive health outcomes in sub-Saharan Africa, including truncated schooling (Biddlecom et al. 2008), increased sexual risk behavior (Harrison et al. 2005), and elevated risk of HIV/AIDS (Gregson et al. 2005; Hallett et al. 2007; Pettifor et al. 2004).
The dimensions of family instability that I explore extend beyond those most often examined in the U.S. literature. Most empirical work has examined the number of family transitions, with the idea that each additional transition creates stress detrimental to child well-being. In addition to this, I also use detailed monthly data to investigate whether the effects of family instability are manifested immediately or with a lag, and how quickly they dissipate. Furthermore, I examine whether the relationship between having experienced family instability and sexual behavior is dependent on age, in line with the notion that experiences may affect individuals differently depending on timing in the life course (Elder 1994; Hogan and Astone 1986). Investigation of these latter dimensions of family instability can provide important information on when and how to best tailor interventions to assist youth with experiences of family volatility.
Background
Family Structure and Child Well-being in Sub-Saharan Africa
A considerable body of demographic and health research has examined the relationship between family structure in sub-Saharan Africa and child well-being. This scholarship has highlighted links between parental presence and youth sexual behavior (McGrath et al. 2009; Ngom et al. 2003; Rwenge 2000). It has also provided evidence that young people living with heads of household that are close nonparental kin (e.g., grandmothers) experience better outcomes with respect to schooling and sexual behavior than those living with more distantly related heads (Case et al. 2004; Nyamukapa and Gregson 2005; Rwenge 2000). Furthermore, several scholars have found positive associations between residing in female-headed households and children’s schooling, compared with residing in male-headed households (Lloyd and Blanc 1996; Townsend et al. 2002).
The research to date has, however, relied on snapshots of family situations at one point in time, most often the time of interview. This has presented two main challenges. First, the cross-sectional nature of the data has made it impossible to ensure that the measures of family structure precede the outcome. Second, it has also precluded examination of family structure over time and the influence of stability of caregiving. It is plausible that consistency over time is at least as important for young people’s well-being as a particular family structure.
A further limitation is that studies generally use parental coresidence and household headship measures as proxy measures for who cares for children. Although this likely reflects caregiving arrangements in many cases, it may be a less accurate representation of reality in extended-family households and compounds like those seen in many parts of sub-Saharan Africa. For example, a child with a grandparent household head may in actuality be cared for by a coresident parent or other relative. Likewise, although a father coresides, a young person may be most influenced by a coresident, or even a nearby resident, aunt, stepmother, or grandmother.
Orphanhood in Sub-Saharan Africa
A related line of research has examined the consequences of parental death for children in the region. Scholarship on this topic has exploded in the past two decades in light of the region’s high burden of AIDS mortality. Longitudinal studies have been more common in this body of work, and results have generally suggested a causal effect of orphanhood1 on poor schooling and physical health outcomes for maternal but not paternal orphans (Ainsworth et al. 2005; Beegle et al. 2010; Case and Ardington 2006; Evans and Miguel 2007). Cross-sectional analyses have also linked orphan status with early initiation of sexual activity, unprotected sex, and HIV serostatus (Birdthistle et al. 2008; Gregson et al. 2005; Nyamukapa et al. 2008; Operario et al. 2007; Palermo and Peterman 2009).
Empirical work on this topic usually compares the well-being of orphans to that of non-orphans under the implicit assumption that the latter are cared for by their living parents. However, recent studies have highlighted the problematic nature of this assumption in light of how frequently non-orphans in the region live apart from parents (Hosegood et al. 2007; Madhavan 2004; Monasch and Boerma 2004). Implications of this for the current study are twofold. First, because of factors like migration and fostering, a considerable fraction of non-orphans in the region experience family disruption, too. Second, a considerable proportion of orphans may not experience caregiver change, either because their primary caregiver was not parental before they became orphans or because they continue to be cared for by a surviving parent.
Family Instability and Child Well-Being
To investigate the relationship between volatility in caregiving and the timing of sexual initiation, I build on a large body of literature on family instability in the United States. This research is motivated by the high levels of union instability among adults with children in the United States in recent decades. In addition to examining the well-being of children in particular family types (e.g., two-biological-parent married, single-parent, stepfamily), it asks whether there is something about parental partnership instability in and of itself that diminishes child well-being (Brown 2010; Cavanagh and Huston 2006; Fomby and Cherlin 2007). Drawing on social stress theory (George 1993; Osborne and McLanahan 2007), the theoretical case generally rests on the idea that changes in a parent’s romantic history produce stresses to parents and children, which may accumulate with each partnership change. The term “family turbulence” has also been used to denote a similar concept (Teachman 2008; Wu 1996).
Prior research has employed varied conceptualizations of family instability (Brown 2010), although all reflect a focus on parental union transitions. Family instability is usually measured as the number of partnership transitions experienced by the child’s mother or the number of transitions experienced by the child in coresidence with parents and their partners. It is also sometimes measured as the amount of time that one is exposed to a particular family type (e.g., single-mother family) (Bulanda and Manning 2008; Cavanagh 2008; Magnuson and Berger 2009; Ryan et al. 2009). In addition, some analyses disaggregate family instability by type of parental union transition (e.g., cohabitation vs. marital) (Brown 2006; Hao and Xie 2002) or age at transition (Cavanagh and Huston 2008; Heard 2007; Ryan et al. 2009; Brauner-Otto and Axinn 2010).
Studies have linked family instability with a range of indicators of child and adolescent disadvantage. With respect to adolescents in the United States, these include lack of school engagement (Brown 2006; Heard 2007; Sun and Li 2002); early sexual debut (Albrecht and Teachman 2003; Brauner-Otto and Axinn 2010; Capaldi et al. 1996; Fomby et al. 2010; Wu and Thomson 2001); substance use (Cavanagh 2008); and early relationship formation and fertility (Cavanagh et al. 2008; Fomby et al. 2010; Hofferth and Goldscheider 2010; Ryan et al. 2009; Wu 1996).
Extending the family instability perspective to sub-Saharan Africa requires taking into account that the high levels of family volatility experienced by young people in recent decades derive from a variety of factors that are largely different from those studied in the United States. The AIDS epidemic has rendered parental death a key source of family change. For example, in Nyanza Province, HIV prevalence was estimated at 15 % in 2007 (NASCOP 2009), and more than one in four children aged 0–14 (28 %) were considered orphans in 2003 (CBS, MOH, and ORC Macro 2004). Additional HIV/AIDS–related family change can be produced when children’s care-givers are too ill to care for them or when ill migrants return home for care (Ansell and van Blerk 2004; Clark et al. 2007). There is also evidence from Malawi that men and women may be turning to divorce as an HIV risk-avoidance strategy (Reniers 2008). Family transitions in the region are also commonly produced by labor migration, union formation and disruption, and fostering of children to nonparental caregivers for reasons such as sending a child to school or providing help to kin in need of assistance (Hosegood et al. 2007; Madhavan 2004). The current analysis captures the multiple sources of family instability that coexist in this setting by employing broad measures of family change rather than focusing on a particular source, such as mortality or partnership change.2
Application of the family instability perspective to the study setting also requires consideration of volatility in nonparental caregiving. The focus on parental changes in the measurement of family instability to date makes it difficult to disentangle the extent to which observed associations are produced by changes in parent-child relationships specifically or by changes in caregiving more broadly. The current study investigates the influence of caregiver instability, whether parental or nonparental.
Dimensions of Family Instability
I expect that each additional family transition increases the likelihood of initiation of sexual activity, in line with social stress theory and previous U.S. research (Albrecht and Teachman 2003; Brauner-Otto and Axinn 2010; Brown 2010; Wu and Thomson 2001). With regard to recency, research has found that the initial effects of exiting a partnership on mothers’ mental and physical health are relatively short-lived (Meadows et al. 2008). I anticipate that for young people, the greatest stresses of caregiver change are also manifested in a short window of time, diminishing as the situation normalizes. This is consistent with scholarship that has deemed the one- to two-year period following divorce the “crisis period” (Chase-Lansdale and Hetherington 1990; Morrison and Cherlin 1995). Nonetheless, there could plausibly be a lagged effect because of a “honeymoon” period following a shift in caregiving or the time that it could take for young people to build the social networks required to enact sexual activity if caregiver change has been accompanied by a move to a new location.
Finally, I anticipate that the effects of caregiver instability manifest themselves more strongly during early adolescence than during later adolescence. The former represents a time when sexual activity is less common and perhaps more likely to constitute acting-out behavior, and when young people also find themselves in the midst of major emotional and physical developmental changes associated with puberty.
Pathways Linking Family Instability and Sexual Debut
There are a variety of potential pathways linking caregiver instability and sexual debut. Young people may experience diminished emotional support or supervision from new caregivers for at least a short adjustment period. The U.S. literature suggests that after a family transition, children may experience increased ambiguity in expectations about behavior, disruption in their sense of security, and difficulties in acclimating to “blended” families, and they may begin to rely on peer groups for support or intimacy previously provided by caregivers (Albrecht and Teachman 2003; Brauner-Otto and Axinn 2010; Capaldi et al. 1996; Wu 1996; Wu and Thomson 2001).
Residential change is another pathway through which the relationship between family instability and sexual debut might operate. Moves have been linked with early sexual debut (Luke et al. 2012; Sambisa and Stokes 2006) and high-risk sexual behavior (Brockerhoff and Biddlecom 1999) in sub-Saharan Africa. Changes in residence may bring changes in community and family support networks, peer networks, and exposure to new ideas and social norms (Brockerhoff and Biddlecom 1999; South et al. 2005; Stack 1994). Nonetheless, several empirical analyses in the United States have not found that residential change explains observed family instability effects (Cavanagh et al. 2008; Osborne and McLanahan 2007).
Experience of family change also may be associated with a higher likelihood of having a distantly related caregiver, which may be linked to the outcome. Similarly, those who experience family change may be more likely to be orphans. Moreover, although both orphans and non-orphans experience caregiver instability, it could also be that orphans experience the stresses of caregiver change more intensely because of the particularly high levels of psychosocial distress associated with parental mortality (Atwine et al. 2005; Nyamukapa et al. 2008).
It is also possible that any observed link between caregiver change and the likelihood of sexual debut is actually attributable to stresses predating the shift in caregiving. This is akin to research in the United States that has found that at least some of the negative effects of divorce on children may be accounted for by predisruption factors (Cherlin et al. 1991; Morrison and Cherlin 1995; Sun and Li 2002). In the current study, this might be particularly relevant to caregiver change resulting from union disruption or mortality. Indeed, results from recent research in Kenya indicate a sharp decline in children’s school participation prior to maternal death (Evans and Miguel 2007).
The Kisumu life history data contain time-varying information to control for residential change, primary caregiver type, orphan status, and the likelihood of sexual debut in the months prior to caregiver change. I also test for gender differences in the effect of family instability on the timing of sexual initiation. Gender differences have not been extensively examined in the U.S. literature on this topic, and results have been inconsistent. One study found that family instability was more consequential for boys than for girls with respect to adolescent romantic relationship formation (Cavanagh et al. 2008). Another found no significant gender difference in the relationship between family instability and early marriage and cohabitation (Ryan et al. 2009). In sub-Saharan Africa, previous research has noted distinct norms of sexual behavior for men and women and, in particular, a double standard that gives men license to be sexually adventurous while restricting female sexuality (Orubuloye et al. 1997; Varga 2003). Because early sexual activity is considered a more deviant behavior for young women, one might expect family instability to be more consequential for girls with regard to the outcome. Conversely, the greater license for early sexual activity accorded to young men might make them more likely to exhibit this behavior in response to stresses of family change.
I also control for other variables that have been linked with the timing of sexual debut in sub-Saharan Africa. Being in school (Jukes et al. 2008; Lloyd 2007; McGrath et al. 2009) and possession of economic resources (Dinkelman et al. 2007; Dodoo et al. 2007; Hallman 2005) have been associated in previous studies with delayed initiation of sexual activity. Urban residence has been linked to early sexual debut (Dodoo et al. 2007).
Data, Measures, and Methods
Data
Investigation of the relationship between family instability and early sexual debut requires detailed family histories as well as detailed measures of the timing of sexual activity. The current analysis draws on unique data from the Urban Life Among Youth in Kisumu Study, conducted by researchers from Brown University, McGill University, and the African Population and Health Research Center (APHRC). Interviews were conducted with 608 18- to 24-year-olds in 2007.
Life history data were collected through the use of an instrument called the Relationship History Calendar (RHC). Demographers have used life history calendars to gather histories on contraception, fertility, migration, schooling, and employment from populations in developed and developing countries (e.g., Axinn and Pearce 2006; Curtis and Blanc 1997; Freedman et al. 1988; Goldman et al. 1989; White et al. 2008). The RHC records 10 years of retrospective monthly information on romantic and sexual relationships.3 It also collects histories on schooling, work, migration, and caregiving arrangements.
Like other life history calendars, the RHC is intended to facilitate respondent recall by measuring the timing and sequencing of events in several life course domains simultaneously. Participants can gauge the timing of one event based on the timing of other salient events in their histories, such as national tragedies, family milestones, or school holidays. The structure of the RHC also allows for clarification and cross-checking across domains.
The RHC is also intended to reduce social desirability bias, which is often an issue when gathering data on sensitive sexual behaviors. The flexible and conversational interview procedure used with the RHC draws on qualitative techniques, which have been found to reduce this type of bias (Plummer et al. 2004; Poulin 2010). Furthermore, relationships are discussed in the sequence that is the most comfortable for the individual respondent, and sexual behavior is embedded in the context of romantic relationships and in conjunction with more mundane histories of schooling, work, and migration. Finally, the ability for trained interviewers to cross-check across multiple life domains in real time using the calendar makes sustaining consistently socially desirable responses very difficult. Comparison with a standard survey instrument like the Demographic and Health Surveys finds that the RHC improves reporting of sensitive sexual behaviors (Luke et al. 2011). In particular, young females, who have been found to underreport their sexual activity in survey interviews (Mensch et al. 2001; Nnko et al. 2004), were found to report earlier ages of sexual debut in the RHC than on the standard instrument, with no significant differences in age at sexual initiation for young males.
In addition to the calendar instrument, respondents were also administered introductory and follow-up questionnaires. These questionnaires gathered basic sociodemographic data and information about partnerships not reported on in the calendar; they also included a series of questions on maternal and paternal survival, including the timing of any parental death.
Enumeration areas (EAs) delimited by Kenya’s Central Bureau of Statistics were the study’s primary sampling units. Of Kisumu’s urban EAs, 45 were randomly selected. Five female and five male local interviewers were hired, with all but one in the age range of the respondents. In each selected EA, the interviewers visited every other household and listed all current residents in the household aged 18 to 24. If more than one eligible respondent was present, one young adult was selected for interview using a random draw procedure. The study’s overall response rate was 94.9 %. (For additional details on the study design, see Luke et al. (2011).) The author participated in the design of the study instruments and the fieldwork. Ethical clearance was granted by the Kenya Medical Research Institute, the Kenyan Ministry of Science and Technology, and Brown and McGill Universities.
Measures
Sexual Debut
The main outcome variable is a dichotomous indicator of whether sexual activity was initiated in a given month. It is based on a question in the RHC asking about the frequency of sexual intercourse.
Family Instability
Family instability is operationalized through measurement of changes in primary caregiver. To determine the best phrasing for the concept of primary caregiver in the major local languages of Luo and Kiswahili, I consulted with several local informants about who young people’s caregivers are, what their role entails, and how their roles might change in function and meaning throughout young people’s lives. Although it is likely that most caregivers reside in the same household, I was careful to make clear that this need not be the case.4 The terms used in the final study instrument roughly translate into a combination of “the one who is responsible for” and “the one who provides for” a young person. The 20 response categories in the RHC included distinctions by relation, kinship tie (maternal or paternal), and gender.
In the current study, for each month, I measure the cumulative number of months since the beginning of the calendar in which the response category for primary caregiver (of the 20) was different from that of the month prior. I also measure whether the last caregiver change was experienced 1–6 months ago, 7–12 months ago, or 13 or more months ago, with no change to date omitted. Finally, as an indicator of the stressful period before caregiver transition, I measure whether caregiver change will occur in the next 6 months.
Primary Caregiver Type, Orphan Status, and Residential Change
I summarize the 20 response categories of primary caregiver in the RHC with a five-category time-varying indicator of primary caregiver type. The five categories distinguish between parents,5 grandparents, aunts/uncles, siblings, and others.6 The “other” category includes responses of stepmother, no one/independent, spouse, boyfriend/girlfriend, and employer.
Orphan status is measured with a time-varying categorical indicator that distinguishes between non-orphans, maternal orphans, paternal orphans, and double orphans. Respondents become orphans of a given type in the month they enter that status.
I operationalize residential change with a time-varying indicator of major residential moves. This measure captures all moves from a rural to an urban area, and vice versa, as well as rural-rural or urban-urban moves that cross district (within Nyanza) or province (elsewhere in Kenya) boundaries.7 I assume that major moves like these are the most likely to affect young people’s sexual behavior, for example, through changes in support networks, peer group composition, and/or exposure to different sexual norms. In each specification, I match the indicators of residential change to the caregiver instability indicators being used (last move 1–6 months ago, 7–12 months ago, or 13+ months ago; and cumulative number of moves).
Sociodemographic Controls
I measure respondent age in each month as a continuous variable centered on age 8.8 I also include a time-invariant continuous indicator of age at time of interview to account for potential increased recall bias, as well as increased likelihood of experiencing sexual debut before the beginning of the calendar, for those older at the time of interview. I measure urban/rural residence, school status, and gender dichotomously. Finally, I measure household economic status at time of interview using an index constructed from 14 items relating to household assets and infrastructure. I generated standardized weight scores for the analytic sample, which were summed to produce index scores and then ranked and divided into quartiles.9
Methods
I employ discrete-time logit models to estimate the probability of sexual debut occurring in a given person-month. Event history methods are particularly useful for examining outcomes such as sexual debut because they allow for precise ordering around the outcome of interest (ensuring in this case that family transitions precede sexual onset) and for inclusion of time-varying covariates. They also explicitly incorporate right-censored cases.
Respondents are considered “at risk” of sexual debut from the beginning of the RHC through the month prior to initiating sexual activity, marrying, or turning 18, whichever comes first, and are censored afterward. I cap the exposure period at age 18 for two reasons. First, the interest in this article is early sexual debut. Using three criteria (physical maturation of the body; cognitive capacity for making safe, informed, and voluntary decisions; and legal frameworks and international standards), Dixon-Mueller (2008) concluded in a recent paper focused on developing countries that age 14 and younger is essentially “too young” to transition into sexual behavior; ages 15–17 may or may not be too young, depending on circumstances; and by age 18 and older, youth are generally “old enough” to make safe and voluntary transitions.
Second, as youth reach the early years of adulthood, caregiver changes are increasingly likely to be self-initiated (for example, by leaving one’s home of origin). The implications of youth-initiated family instability likely differ from that engendered by caregiver transitions.
I censor respondents at marriage to ensure examination of the predictors of early sexual debut rather than those of early marriage. Censoring at marriage did little to the sample size for the current analysis because only five individuals (0.9 % of the sample) were married before age 18 and did not initiate sexual activity prior to the month they married.
The regression models take the following form:
where h(ti ∣ x) is the conditional probability of debuting sexually at time ti for a given covariate vector X = (x1, …, xk). In the first set of regressions, I examine associations between the number and recency of caregiver changes and the likelihood of sexual debut, independent of sociodemographic controls. I also test for interactive effects between the measures of caregiver change and the time-varying measure of respondent age. In the second set of regressions, I include indicators of orphan status, residential change, caregiver type, and whether caregiver change will occur in the next six months. I also examine interactions between respondent sex and caregiver instability. Across all regressions, the caregiver change variables are lagged by one month to guard against reverse causality in the month of caregiver disruption. I employ robust standard errors to adjust for clustering of person-months within individuals. I use Stata 10.0 for all analyses.
The final analytic sample includes 533 young women and men, who contribute 31,515 person-months. Thirty-four individuals who initiated sexual activity before the beginning of the calendar are removed from the analysis because of the lack of information on caregiver transitions before their sexual debut. I describe checks for bias resulting from this left-censoring in the results section. The other individuals excluded from the sample were missing data on the outcome or covariates of interest.10
Results
Descriptive Statistics
Sexual Debut
Descriptive statistics indicate that a nontrivial proportion of youth experience early sexual debut in Kisumu. Table 1 shows that 21 % of the youth in the sample debuted sexually at age 14 or earlier, and 63 % debuted at age 17 or earlier. For those who initiated sexual activity prior to interview, the mean ages at sexual initiation were 16.4 for young women and 15.9 for young men. Figure 1 displays survival curves for sexual debut by sex. They indicate that the interval between ages 13 and 18 has the steepest declines in survival in this population, with minimal differences between the sexes. A log-rank test for equality of survival functions (not shown) confirms that the curves of male and female respondents are not statistically significantly different.
Table 1.
Descriptive statistics of individual characteristics for young women and men in analytic sample (percentages unless otherwise noted)
| Characteristic | Total | Female | Male | Sig. |
|---|---|---|---|---|
| Caregiver Instability Between Beginning of Calendar and Age 18 | ||||
| Experienced any change in primary caregiver | 45.40 | 44.62 | 46.15 | |
| 3+ changes in primary caregiver | 9.94 | 10.77 | 9.16 | |
| Mean number of changes in primary caregiver | 0.93 (1.52) | 0.92 (1.46) | 0.94 (1.58) | |
| Sexual Behavior | ||||
| First sex at age 14 or younger | 21.01 | 18.46 | 23.44 | |
| First sex at age 17 or younger | 62.85 | 60.00 | 65.57 | |
| Mean age at first sex (for those who initiated sexual activity prior to the interview date) | 16.14 (2.40) | 16.38 (2.30) | 15.93 (2.48) | * |
| Ever Reported as Primary Caregiver Between Beginning of Calendar and Age 18 | ||||
| Parent | 90.99 | 91.15 | 90.84 | |
| Grandparent | 10.32 | 11.92 | 8.79 | |
| Aunt/uncle | 18.76 | 16.15 | 21.25 | |
| Sibling | 15.57 | 18.08 | 13.19 | |
| Other | 7.69 | 5.77 | 8.06 | |
| Orphaned by Age 18 | ||||
| Paternal orphan | 21.58 | 21.92 | 21.25 | |
| Maternal orphan | 5.44 | 5.77 | 5.13 | |
| Double orphan | 12.20 | 11.15 | 13.19 | |
| Major Residential Move Between Beginning of Calendar and Age 18 | ||||
| Experienced any major change in residence | 55.16 | 57.31 | 53.11 | |
| Age at Time of Interview | ||||
| Mean age | 20.55 (1.84) | 20.49 (1.84) | 20.60 (1.84) | |
| Gender | ||||
| Female | 48.78 | |||
| Schooling Status at Age 15 | ||||
| In formal school | 86.82 | 84.34 | 89.14 | |
| Urban/Rural Residence at Age 15 | ||||
| Urban | 66.60 | 63.31 | 69.66 | |
| Economic Status at Time of Interview | ||||
| Lowest | 24.95 | 21.15 | 28.57 | * |
| Lower middle | 24.95 | 24.23 | 25.64 | |
| Upper middle | 25.33 | 25.77 | 24.91 | |
| Highest | 24.77 | 28.85 | 20.88 | * |
| Number of Individuals | 533 | 260 | 273 | |
Note: Standard deviations are given in parentheses below means.
p < .05 for differences between young women and men.
Fig. 1.
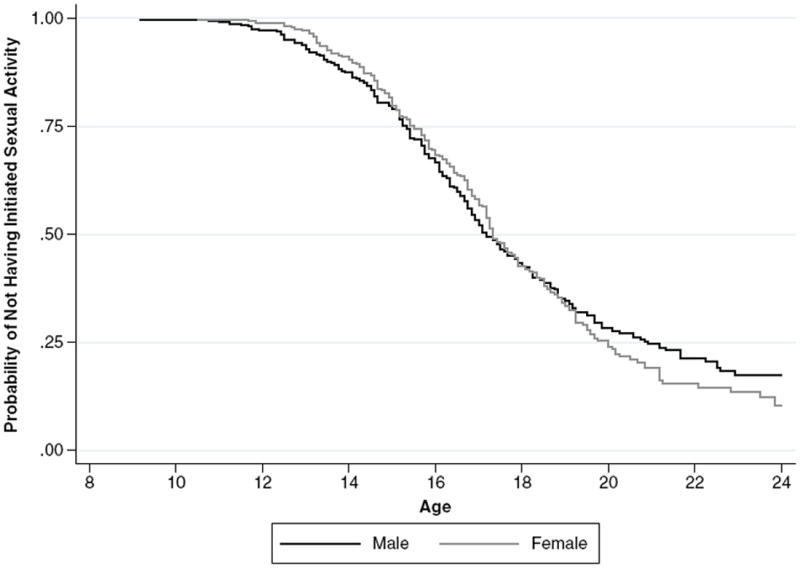
Survival curves for young women and men
Independent Variables
Table 1 suggests that caregiver change is a common experience in this population. Forty-five percent of youth experienced at least one transition in primary caregiver between the start of the calendar and age 18, and 10 % experienced three or more. The descriptive statistics also indicate that substantial proportions of young people spent at least some time under the care of someone other than a parent. Almost one-fifth (19 %) reported having an aunt or uncle as their primary caregiver during at least one month of the calendar; 16 % named a sibling; 10 %, a grandparent; and 8 %, another type of caregiver.
Reflecting the high prevalence of HIV/AIDS in Nyanza Province, 39 % of respondents were orphaned by the age of 18. In addition, more than one-half of young women and men experienced at least one major residential move between the beginning of the calendar and age 18. Overall, there were very few statistically significant differences between young women and men with regard to the independent variables in the analysis.
Caregiver Change and Sexual Debut
Table 2 presents results from discrete-time logit models predicting the likelihood of sexual debut. The first two models measure family instability as the cumulative number of changes in primary caregiver. Models 3 and 4 examine recency of last caregiver change. Models 1 and 3 assume that the effects of caregiver change are the same regardless of age, and Models 2 and 4 include interaction terms between the caregiver change variables and age.
Table 2.
Discrete-time logit models predicting sexual debut
| Model 1
|
Model 2
|
Model 3
|
Model 4
|
|||||
|---|---|---|---|---|---|---|---|---|
| β | RSE | β | RSE | β | RSE | β | RSE | |
| Cumulative Number of Changes in Primary Caregivera | −0.018 | (0.087) | 0.709*** | (0.126) | ||||
| Recency of Last Change in Primary Caregivera (none) | ||||||||
| 1–6 months ago | 0.501* | (0.226) | 3.764*** | (0.626) | ||||
| 7–12 months ago | 0.036 | (0.292) | 0.517 | (1.293) | ||||
| 13+ months ago | −0.109 | (0.184) | 1.529† | (0.888) | ||||
| Age | 0.369*** | (0.034) | 0.409*** | (0.034) | 0.367*** | (0.033) | 0.433*** | (0.037) |
| Cumulative Number of Changes in Primary Caregivera × Age | −0.096*** | (0.022) | ||||||
| Recency of Last Change in Primary Caregivera (none) × Age | ||||||||
| 1–6 months ago × age | −0.443*** | (0.088) | ||||||
| 7–12 months ago × age | −0.068 | (0.160) | ||||||
| 13+ months ago × age | −0.209† | (0.109) | ||||||
| Age at Time of Interview | 0.024 | (0.037) | 0.021 | (0.037) | 0.024 | (0.037) | 0.025 | (0.037) |
| Female | −0.121 | (0.118) | −0.111 | (0.118) | −0.121 | (0.119) | −0.124 | (0.119) |
| In Formal Schoola | −0.751*** | (0.180) | −0.810*** | (0.177) | −0.700*** | (0.174) | −0.733*** | (0.173) |
| Urban Residencea | 0.254* | (0.128) | 0.288* | (0.128) | 0.246† | (0.127) | 0.277* | (0.127) |
| Economic Status at Time of Interview (low) | ||||||||
| Lower middle | −0.287† | (0.160) | −0.301† | (0.160) | −0.310† | (0.161) | −0.282† | (0.160) |
| Upper middle | −0.413* | (0.173) | −0.402* | (0.172) | −0.442* | (0.174) | −0.409* | (0.174) |
| High | −0.725*** | (0.191) | −0.729*** | (0.191) | −0.731*** | (0.190) | −0.705*** | (0.190) |
| Intercept | −6.646*** | (0.728) | −6.842*** | (0.728) | −6.725*** | (0.725) | −7.202*** | (0.737) |
| N (person-months) | 31,467 | 31,467 | 31,515 | 31,515 | ||||
| Log-Likelihood | −1,701.45 | −1,694.09 | −1,698.89 | −1,687.95 | ||||
Notes: RSE = robust standard errors. Comparison categories are in parentheses. Age is centered on 8, referencing the first age represented in the life history calendar.
Variable lagged by one month.
p < .10;
p < .05;
p < .001
The results from Models 1 and 2 indicate no statistically significant association between the cumulative number of caregiver changes and the likelihood of sexual debut, independent of sociodemographic controls, on average across the exposure period. However, there is a strong and positive relationship apparent at the beginning of the interval that diminishes greatly with age.11
The results from Models 3 and 4 suggest that the relationship between caregiver instability and initiation of sexual behavior is strongest shortly following a caregiver change. Converting the coefficient in Model 3 to an odds ratio, the odds of initiating sexual activity in any given month were 1.6 times greater for young people who had experienced a transition in primary caregiver in the past six months than for those who had not experienced a change. The lack of significant differences between having experienced a last change in caregiver 7–12 months or 13+ months ago, compared with none, suggests minimal lingering effects of caregiver change for youth who do not initiate sexual activity in the first six months after caregiver transition. The results from Model 4 indicate that, as with the cumulative number of changes in primary caregiver, the magnitude of the association between recent caregiver change and the likelihood of sexual debut is very strong at the earliest ages in the calendar and diminishes greatly with age.12 In this last specification, the main effect for last change in caregiver 13+ months ago is marginally significant, as is the interaction with age.
Figures 2 and 3 illustrate how the relationship between caregiver instability and the outcome varies with age. They present predicted probabilities of sexual debut in an average month at ages 13 and 16, based on Models 2 and 4 from Table 2. These ages represent early and mid-adolescence, and span the first two categories (ages <14 and 15–17) from Dixon-Mueller’s schema of readiness for sexual activity (2008). Overall, the low probabilities of sexual debut in any given month reflect the narrow time interval.
Fig. 2.
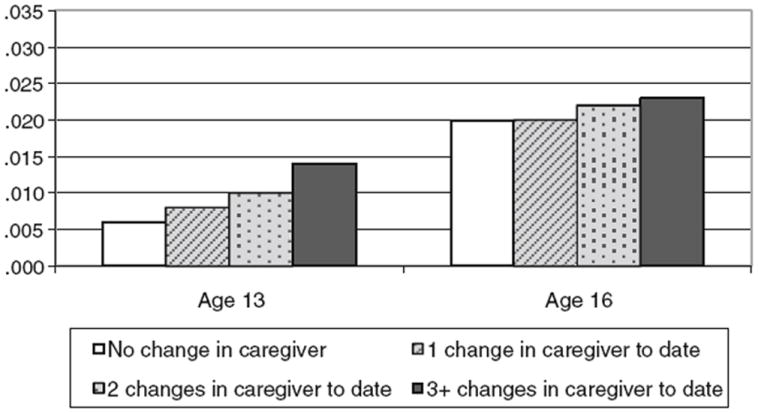
Predicted probability of sexual debut in an average month at ages 13 and 16, by cumulative number of changes in caregiver
Fig. 3.
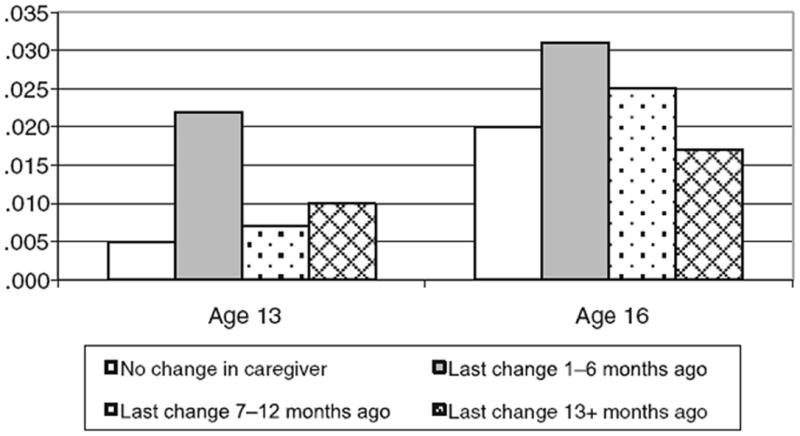
Predicted probability of sexual debut in an average month at ages 13 and 16, by recency of caregiver change
Figure 2 indicates that at age 13, the probability of initiating sexual activity more than doubles when moving from zero to three or more caregiver changes. By age 16, however, there is virtually no difference in the probability of sexual debut by the number of caregiver changes experienced. Figure 3 shows that at both ages 13 and 16, young people that experienced caregiver change in the previous six months have the highest probability of sexual debut. However, the difference between them and those who experienced no caregiver change or more distal caregiver change is much smaller by age 16.
Finally, the findings for the sociodemographic controls are virtually identical across all four models in Table 2 and are in line with expectations. Economic status and school enrollment are negatively associated, and age and urban residence positively associated, with the likelihood of sexual debut. Neither respondent sex nor age at time of interview is significantly associated with the outcome.
Additional Analyses
Additional Controls and Interactions
Table 3 subjects Models 2 and 4 from Table 2 to additional controls and interactions. Overall, the results for caregiver instability observed in Table 2 persist. Models 1 and 2 in Table 3 test for differences between young women and men in the relationship between caregiver instability and the timing of sexual debut. The coefficients for the interactions between caregiver change and gender are never statistically significant.13 Inclusion of the interaction terms also does not significantly improve fit over the models in Table 2.
Table 3.
Discrete-time logit models predicting sexual debut: Models 2 and 4 from Table 2 with additional controls and interactions
| Model 1
|
Model 2
|
Model 3
|
Model 4
|
Model 5
|
||||||
|---|---|---|---|---|---|---|---|---|---|---|
| β | RSE | β | RSE | β | RSE | β | RSE | β | RSE | |
| Cumulative Number of Changes in Primary Caregivera | 0.707*** | (0.137) | 0.733*** | (0.133) | ||||||
| Recency of Last Change in Primary Caregivera (none) | ||||||||||
| 1–6 months ago | 4.018*** | (0.672) | 3.984*** | (0.639) | 3.725*** | (0.653) | ||||
| 7–12 months ago | 0.599 | (0.685) | 0.823 | (1.241) | 0.450 | (1.339) | ||||
| 13+ months ago | 1.400 | (0.130) | 1.562† | (0.885) | 1.513† | (0.905) | ||||
| Age | 0.409*** | (0.034) | 0.433*** | (0.037) | 0.412*** | (0.035) | 0.443*** | (0.037) | 0.435*** | (0.037) |
| Cumulative Number of Changesa × Age | −0.096*** | (0.026) | −0.097*** | (0.023) | ||||||
| Recency of Last Change in Primary Caregivera (none) × Age | ||||||||||
| 6 months ago × Age | −0.443*** | (0.090) | −0.450*** | (0.087) | −0.439*** | (0.091) | ||||
| 7–12 months ago × Age | −0.069 | (0.161) | −0.058 | (0.157) | −0.063 | (0.166) | ||||
| 13+ months ago × Age | −0.204† | (0.109) | −0.196† | (0.108) | −0.209† | (0.111) | ||||
| Female | −0.108 | (0.133) | −0.081 | (0.139) | −0.153 | (0.123) | −0.156 | (0.121) | −0.119 | (0.119) |
| Cumulative Number of changes in Caregivera × Female | −0.007 | (0.144) | ||||||||
| Recency of Last Change in Primary Caregivera (none) × Female | ||||||||||
| 1–6 months ago × Female | −0.558 | (0.403) | ||||||||
| 7–12 months ago × Female | −0.156 | (0.584) | ||||||||
| 13+ months ago × Female | 0.152 | (0.340) | ||||||||
| Primary Caregiver Type in Given Montha (parent) | ||||||||||
| Grandparent | −0.097 | (0.263) | −0.139 | (0.266) | ||||||
| Aunt/uncle | −0.114 | (0.246) | −0.133 | (0.241) | ||||||
| Sibling | 0.413† | (0.244) | 0.351 | (0.240) | ||||||
| Other | −0.409 | (0.525) | −0.570 | (0.513) | ||||||
| Orphan Status (non-orphan) | ||||||||||
| Maternal orphan | 0.451 | (0.294) | 0.409 | (0.292) | ||||||
| Paternal orphan | 0.009 | (0.151) | −0.061 | (0.152) | ||||||
| Double orphan | −0.125 | (0.295) | −0.210 | (0.287) | ||||||
| Cumulative Number of Major Residential Movesa | −0.023 | (0.030) | ||||||||
| Recency of Last Major Residential Movea (none) | ||||||||||
| 6 months ago | −0.270 | (0.241) | ||||||||
| 7–12 months ago | −0.550 | (0.362) | ||||||||
| 13+ months ago | −0.177 | (0.234) | ||||||||
| Caregiver Change Will Occur Within Next 6 Months | 0.473 | (0.805) | ||||||||
| Caregiver Change Will Occur Within Next 6 Months × Age | −0.024 | (0.106) | ||||||||
| Intercept | −6.838*** | (0.730) | −7.214*** | (0.738) | −6.792*** | (0.736) | −7.007*** | (0.746) | −7.309*** | (0.739) |
| N (person-months) | 31,467 | 31,515 | 31,402 | 31,515 | 31,514 | |||||
| Log-Likelihood | −1,694.09 | −1,686.63 | −1,684.87 | −1,681.80 | −1,683.77 | |||||
Notes: RSE = robust standard errors. In addition to the indicators shown, all regressions control for age at time of interview, school status, urban/rural residence, and economic status at time of interview. Comparison categories are in parentheses. Age is centered on 8, referencing the first age represented in the life history calendar.
Variable lagged by one month.
p<.10;
p<.001
Models 3 and 4 in Table 3 indicate that the associations observed in Table 2 are not simply a function of primary caregiver type, orphan status, or residential mobility. Indeed, none of these independent variables have independent significant associations with sexual debut,14 nor does their inclusion improve model fit beyond the models in Table 2. Separate tests indicate that orphan status is not associated with the likelihood of sexual debut even before adjustment for caregiver instability (not shown). Furthermore, interactions tested between orphan status and recent caregiver change suggest that the effect of recent caregiver change does not depend on orphan status (not shown).15
Model 5 shows that individuals who will experience caregiver change in the next six months are not significantly more likely to initiate sexual activity than individuals who will not. That the relationship between caregiver change in the past six months and the likelihood of sexual debut persists in this model provides support for the interpretation that the results observed in Table 2 derive from caregiver change itself, and not from factors preceding it.
Left-Censoring
Finally, I explored the extent to which left-censoring might be biasing the results of the regressions. As noted earlier, 34 individuals (6 % of the sample) were removed from the analysis because their sexual debut occurred before the start of the RHC, and hence before measurement of caregiver change. I chose not to begin the exposure period at age 15, although it would have prevented this left-censoring, because it would have inaccurately represented the start of the risk of sexual debut for this population, given that one-fifth of the sample initiated sexual activity before this age.
I controlled for age at time of interview in all of the regressions under an assumption that this was the main difference between the left-censored individuals and those who initiated sexual activity early but were retained in the analysis. In addition, I conducted several sensitivity tests to check for biasing of the regression results.16 First, I compared observable time-constant characteristics (completed schooling, economic status at time of interview, and gender) between those with early sexual debut (age <14) before the start of the calendar and those with early sexual debut captured in the calendar. There were no statistically significant differences between these groups across the three variables. I then limited the analytic sample to only those respondents who were age 22 or younger at the time of interview, and began the exposure period at age 12 to create a scenario under which no individuals were left-censored. The results of the regression analyses were substantively identical to those seen in Tables 2 and 3, although the sample size decreased substantially. The predicted probabilities for ages 13 and 16 were also virtually indistinguishable from those in Figs. 2 and 3. Overall, these tests suggest that bias introduced to the regression results by removal of the 34 individuals was minimal.
Discussion
Epidemiological, economic, and social forces have engendered increasingly high levels of volatility in family and household structure for young people growing up in sub-Saharan Africa in recent decades. However, scholarship on the family has not been able to examine the influence of this family instability in and of itself on young people’s outcomes. In the current study, I drew on unique life history calendar data from Western Kenya with monthly measures of primary caregiver over a 10-year period to investigate the relationship between instability in caregiving and early initiation of sexual activity. The identification of predictors of young people’s sexual behavior is particularly urgent in the region, given high rates of HIV/AIDS and a disproportionate incidence of new cases among youth (UNAIDS 2008). I built on a growing body of work on the relationship between parental partnership instability and youth well-being in the United States and examined new dimensions of family change.
Descriptive statistics confirmed that young people in this setting experience substantial levels of caregiver instability. Almost one-half of the sample experienced at least one change in primary caregiver from the beginning of the calendar through age 18, and 1 in 10 experienced three or more changes.
Use of event history methods allowed for inclusion of time-varying covariates and ensured correct sequencing of the key independent and control variables with respect to the onset of sexual activity. The results indicated that caregiver instability is an important predictor of the timing of sexual debut, independent of variables such as schooling and urbanicity that have been associated in previous scholarship with the sexual behavior of adolescents. The relationship persisted after adjusting for indicators of primary caregiver type, orphan status, and residential change, suggesting that these are not the pathways through which the relationship operates. That there were no detectable differences between young women and men, or orphans and non-orphans, in the association between caregiver instability and sexual behavior suggests the import of caregiver stability for all children in this setting.
Investigation of specific dimensions of caregiver instability provided evidence that in this population, the effects of caregiver change accumulate with each transition, as has often been found in the U.S. literature on family instability. The number of caregiver changes experienced was strongly associated with the likelihood of sexual debut in late childhood and early adolescence, with this association diminishing in magnitude with age. That the relationship between change in primary caregiver and sexual initiation was highly age-dependent is consistent with the idea that the effects of caregiver instability are manifested most strongly in early adolescence, when sexual activity is less common and young people are in the midst of great emotional and physical changes.
The results also indicated that the relationship between change in primary caregiver and the likelihood of sexual initiation manifests itself largely during a short window of time after caregiver change. This is consistent with the hypothesis that the stresses of caregiver change are experienced most intensely in an adjustment period, and suggests an important window for intervention. In future work, data collection on affective aspects of young people’s relationships with their caregivers over time, as well as levels of monitoring and supervision, would likely further inform our understanding of the specific mechanisms linking family change with sexual behavior outcomes during this period.
The strengths of the current study included the availability of monthly longitudinal measures, the examination of various dimensions of family instability, and direct measurement of caregiving as opposed to use of proxy measures, such as household headship or parental coresidence. Nevertheless, there are several limitations. First, the information on primary caregiver extended back 10 years prior to the time of interview, rather than to birth. Future studies will need to consider carefully respondent burden and recall bias related to the collection of retrospective information, as well as the trade-off between compiling full lifetime histories and gathering information on narrow time intervals, such as the monthly interval in the current analysis. The latter enabled fine measurement of the influence of recency of caregiver change during a time in the life course when sexual activity is often initiated.
Second, because the calendar did not track comprehensive coresidence rosters, I could not control for the presence of other kin or non-kin relations in an individual’s life. It is possible that a change in primary caregiver may be more or less difficult depending on the presence or absence of other adults. Future research should attempt to measure both caregiving and coresidence with particular relations over time.
Third, although I was able to adjust in my models for a host of characteristics important to consider in the study setting, it is possible that unobserved factors affect both caregiver change and sexual debut. For example, attributes of parents and other caregivers, such as psychological well-being, could affect both these adults’ ability to maintain a stable caregiving environment and the well-being more generally of the children in their care (Fomby and Cherlin 2007). These issues are common to research on family instability. Unfortunately, data on caregiver or proxy attributes are not commonly collected in studies in sub-Saharan Africa. Nonetheless, as a check on the robustness of the results to unobserved heterogeneity, I also specified random intercept models assuming normally distributed random effects. The substantive results of the study held. New research in the region should aim to include information on caregiver characteristics, including caregiver antecedent behaviors and attributes, because investigation along these lines could further inform our understanding of processes at play.
The study results have important implications for programs and policies in the region. First, they indicate a potential need to sensitize those who in their work interact frequently with youth (such as teachers and clinicians) about the particular vulnerabilities that young people can face upon caregiver change. They also suggest a place for programs targeting adults taking on the care of new children with strategies for facilitating the adjustment period. More generally, the results suggest a need to prioritize the preservation of stability in young people’s caregiving arrangements in sub-Saharan Africa. This is somewhat akin to calls in the United States for keeping children in stable family situations as opposed to encouraging parental marriage across the board (Heard 2007; Lichter 2001; Osborne and McLanahan 2007). Finally, the findings are relevant to an ongoing discussion over which types of children (e.g., orphans, all poor children, children in female-headed households, or those under the care of distant relations) to target with policies and aid in sub-Saharan Africa in light of the HIV/ AIDS epidemic and ongoing social and economic instability (e.g., Ainsworth and Filmer 2002; Atwani Akwara et al. 2010; Case et al. 2004; Evans and Miguel 2007). The results presented here indicate that young people who have experienced instability in caregiving are a particularly disadvantaged group, regardless of orphan status or specific caregiving arrangement.
Acknowledgments
I gratefully acknowledge support from an NICHD training grant (T32-HD007338) to the Population Studies and Training Center at Brown University and an American Fellowship from the American Association of University Women (AAUW). I thank Nancy Luke, Susan Short, David Lindstrom, Elizabeth Frankenberg, Margot Jackson, Michael White, anonymous referees, and the Demography editors for invaluable comments and suggestions at various stages of this product. The data used in this analysis come from the Urban Life among Youth in Kisumu Project, directed by Nancy Luke, Shelley Clark, and Eliya Zulu. The research was funded by a grant from the Eunice Kennedy Shriver National Institute for Child Health and Human Development (#R21-HD 053587) and supported by the African Population and Health Research Center.
Footnotes
Consistent with standard practice in the international literature, orphans are defined in this article as children who have lost one or both parents (UNAIDS, UNICEF, and USAID 2004).
I also do not attempt to investigate whether particular sources of family change are more highly associated with the outcome than others. Rather, I aim to broaden the scope of family instability considered and measured.
Coming as they do from a cross-sectional study, the RHC data represent only those alive and residing in Kisumu in the year 2007, and not of all those in Kisumu at the start of the calendar in 1997.
For example, it is not uncommon for young people in rural Kenya to live in extended-family compounds that comprise multiple closely clustered residences. It is possible that a primary caregiver lives nearby, although not in the same household.
“Parent” is used rather than “mother” or “father” because some respondents did not think they could choose between their mother and father, prompting interviewers to place a response of “both parents” under “other” in the questionnaire. Separate analyses separated out responses of “mother,” “father,” and “both parents,” but there were no differences in the substantive results of the study.
In separate analyses, I used indicators that distinguished between maternal and paternal relatives. Based on these categories, the results for caregiver type were identical to those shown in Table 3.
I tested several additional model specifications that isolated rural/urban moves in particular. The results for residential change were the same as those presented in Table 3.
Age is started at 8 rather than the mean to allow for easier interpretation of the results by referencing the first age represented in the calendar. Various polynomials were tested, but none improved model fit compared with the linear treatment of age.
Because household economic status was elicited only for the time of survey, it might not reflect the status preceding sexual debut. Measures of wealth based on accumulated assets and housing characteristics, however, generally change less readily over time than employment and income (Mberu 2006). In addition, under an assumption that an effect between sexual debut and later economic status would most likely occur through pregnancy, I conducted an ordered logit analysis with household economic status as the outcome, sexual debut as the independent variable, and ever pregnant as the mediating variable. When the pregnancy variable was added, there was virtually no attenuation of the association between sexual debut and economic status for males and females, suggesting that reverse causality is unlikely. Like most research on family instability, I cannot address with this time-invariant measure whether change in economic status is a mechanism for any observed association between caregiver change and the outcome. However, changes in economic status have not been found in empirical work in the United States to explain observed family instability effects (Osborne and McLanahan 2007; Wu 1996).
Twenty-two individuals did not provide information on their timing of sexual debut, 12 were missing the timing of parental death, five were missing their date of birth, and two were missing data on economic status. Where possible, checks indicate that individuals missing data did not have significantly different ages of sexual debut than those with no missing data.
Quadratic and cubic terms for the number of caregiver changes were not statistically significantly related to the outcome, nor did their inclusion improve model fit.
A model including both the cumulative and recency variables was tested but did not significantly improve model fit over Models 2 and 4. In addition, there was no evidence of interactive effects between the two sets of variables.
The interactions with female in Model 2 were also not jointly significant. Running separate regressions for young women and men for the models in Tables 2 and 3 also suggested minimal gender differences in the relationship between caregiver instability and the outcome. The most substantial difference was that, for young men, although the association with sexual debut was of greatest magnitude and significance in the first 1–6 months after caregiver change, there was also a significant association 7–12 months after change that did not exist for women.
None of the variance inflation factors (VIFs) for these variables exceed approximately 2, suggesting that the observed results do not simply reflect multicollinearity.
For these two tests, I used two different specifications of the orphan status indicator. The first used the indicator presented in Table 3. The second used indicators of whether maternal or paternal death had occurred in the past six months. Results were the same regardless of the measure used.
I also examined to what extent the descriptive results in Table 1 were affected by the removal of left-censored individuals. With the 34 individuals included, the results for the independent variables did not differ from those shown in Table 1, although the significance level increased for the difference between young women and men in mean age at sexual debut and in the proportion debuting at age 14 or younger. This latter finding might be anticipated, given that young men are disproportionately represented in those left-censored because they have greater representation in the left tails of the distribution for sexual debut.
References
- Ainsworth M, Beegle K, Koda G. The impact of adult mortality and parental deaths on primary schooling in North-Western Tanzania. Journal of Development Studies. 2005;41:412–439. [Google Scholar]
- Ainsworth M, Filmer D. Inequalities in children’s schooling: AIDS, orphanhood, poverty, and gender. World Development. 2002;34:1099–1128. [Google Scholar]
- Albrecht C, Teachman JD. Childhood living arrangements and the risk of premarital intercourse. Journal of Family Issues. 2003;24:867–894. [Google Scholar]
- Ansell N, van Blerk L. Children’s migration as a household/family strategy: Coping with AIDS in Lesotho and Malawi. Journal of Southern African Studies. 2004;30:673–690. [Google Scholar]
- Atwani Akwara P, Noubary B, Lim Ah Ken P, Johnson K, Yates R, Winfrey W, Luo C. Who is the vulnerable child? Using survey data to identify children at risk in the era of HIV and AIDS. AIDS Care. 2010;22:1066–1085. doi: 10.1080/09540121.2010.498878. [DOI] [PubMed] [Google Scholar]
- Atwine B, Cantor-Graae E, Bajunirwe F. Psychological distress among AIDS orphans in rural Uganda. Social Science & Medicine. 2005;61:555–564. doi: 10.1016/j.socscimed.2004.12.018. [DOI] [PubMed] [Google Scholar]
- Axinn WG, Pearce LD. Mixed method data collection strategies. New York: Cambridge University Press; 2006. [Google Scholar]
- Beegle K, De Weerdt J, Dercon S. Orphanhood and human capital destruction: Is there persistence into adulthood? Demography. 2010;47:163–180. doi: 10.1353/dem.0.0094. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Biddlecom A, Gregory R, Lloyd CB, Mensch BS. Associations between premarital sex and leaving school in four sub-Saharan African countries. Studies in Family Planning. 2008;39:337–350. doi: 10.1111/j.1728-4465.2008.00179.x. [DOI] [PubMed] [Google Scholar]
- Birdthistle IJ, Floyd S, Machingur A, Mudziwapasi N, Gregson S, Glynn JR. From affected to infected? Orphanhood and HIV risk among female adolescents in urban Zimbabwe. AIDS. 2008;22:759–766. doi: 10.1097/QAD.0b013e3282f4cac7. [DOI] [PubMed] [Google Scholar]
- Brauner-Otto SR, Axinn WG. Parental family experiences, the timing of first sex, and contraception. Social Science Research. 2010;39:875–893. doi: 10.1016/j.ssresearch.2010.06.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brockerhoff M, Biddlecom AE. Migration, sexual behavior, and the risk of HIV in Kenya. International Migration Review. 1999;33:833–856. [Google Scholar]
- Brown SL. Family structure transitions and adolescent well-being. Demography. 2006;43:447–461. doi: 10.1353/dem.2006.0021. [DOI] [PubMed] [Google Scholar]
- Brown SL. Marriage and child well-being: Research and policy perspectives. Journal of Marriage and Family. 2010;72:1059–1077. doi: 10.1111/j.1741-3737.2010.00750.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bulanda RE, Manning WD. Parental cohabitation experiences and adolescent behavioral outcomes. Population Research and Policy Review. 2008;27:593–618. [Google Scholar]
- Capaldi DM, Crosby L, Stoofanffler M. Predicting the timing of first sexual intercourse for at-risk adolescent males. Child Development. 1996;67:344–359. [PubMed] [Google Scholar]
- Case A, Ardington C. The impact of parental death on school outcomes: Longitudinal evidence from South Africa. Demography. 2006;43:401–420. doi: 10.1353/dem.2006.0022. [DOI] [PubMed] [Google Scholar]
- Case A, Paxson C, Ableidinger J. Orphans in Africa: Parental death, poverty, and school enrollment. Demography. 2004;41:483–508. doi: 10.1353/dem.2004.0019. [DOI] [PubMed] [Google Scholar]
- Cavanagh SE. Family structure history and adolescent adjustment. Journal of Family Issues. 2008;29:944–980. [Google Scholar]
- Cavanagh SE, Crissey SR, Raley RK. Family structure history and adolescent romance. Journal of Marriage and Family. 2008;70:698–714. [Google Scholar]
- Cavanagh SE, Huston AC. Family instability and children’s early problem behavior. Social Forces. 2006;85:551–581. [Google Scholar]
- Cavanagh SE, Huston AC. The timing of family instability and children’s social development. Journal of Marriage and Family. 2008;70:1258–1269. [Google Scholar]
- Central Bureau of Statistics (CBS) [Kenya], Ministry of Health (MOH) [Kenya], and ORC Macro. Kenya demographic and health survey 2003. CBS, MOH and ORC Macro; 2004. [Google Scholar]
- Chase-Lansdale PL, Hetherington EM. The impact of divorce on life-span development: Short and long-term effects. In: Baltes PB, Featherman DL, Lerner RM, editors. Life-span development and behavior. Vol. 10. Hillsdale, NJ: Lawrence Erlbaum; 1990. pp. 107–151. [Google Scholar]
- Cherlin AJ, Furstenberg FF, Chase-Lansdale PL, Kiernan KE, Robins PK, Morrison DR, Teitler JO. Longitudinal studies of effects of divorce on children in Great Britain and the United States. Science. 1991;252:1386–1389. doi: 10.1126/science.2047851. [DOI] [PubMed] [Google Scholar]
- Clark SC, Collinson MA, Kahn K, Drullinger K, Tollman SM. Returning home to die: Circular labour migration and mortality in South Africa. Scandinavian Journal of Public Health. 2007;35(Suppl. 69):35–44. doi: 10.1080/14034950701355619. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Curtis SL, Blanc A. Determinants of contraceptive failure, switching, and discontinuation: An analysis of DHS contraceptive histories. Calverton, MD: Macro International Inc; 1997. Demographic and Health Surveys Analytical Reports No. 6. [Google Scholar]
- Dinkelman T, Lam D, Leibbrandt M. Household and community income, economic shocks, and risky sexual behavior of young adults: Evidence from the Cape Area Panel Study 2002 and 2005. AIDS. 2007;21(Suppl. 7):S49–S56. doi: 10.1097/01.aids.0000300535.05226.a9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dixon-Mueller R. How young is “too young”? Comparative perspectives on adolescent sexual, marital, and reproductive transitions. Studies in Family Planning. 2008;39:247–262. doi: 10.1111/j.1728-4465.2008.00173.x. [DOI] [PubMed] [Google Scholar]
- Dodoo FN, Zulu EM, Ezeh AC. Urban-rural differences in the socioeconomic deprivation-sexual behavior link in Kenya. Social Science & Medicine. 2007;64:1019–1031. doi: 10.1016/j.socscimed.2006.10.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elder GH., Jr Time, human agency, and social change: Perspectives on the life course. Social Psychology Quarterly. 1994;57:4–15. [Google Scholar]
- Evans DK, Miguel E. Orphans and schooling in Africa: A longitudinal analysis. Demography. 2007;44:35–57. doi: 10.1353/dem.2007.0002. [DOI] [PubMed] [Google Scholar]
- Fomby P, Cherlin AJ. Family instability and child well-being. American Sociological Review. 2007;72:181–204. doi: 10.1177/000312240707200203. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fomby P, Mollborn S, Sennott CA. Race/ethnic differences in effects of family instability on adolescents’ risk behavior. Journal of Marriage and Family. 2010;72:234–253. doi: 10.1111/j.1741-3737.2010.00696.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Freedman D, Thornton A, Camburn D, Alwin D, Young-DeMarco L. The life history calendar: A technique for collecting retrospective data. Sociological Methodology. 1988;18:37–68. [PubMed] [Google Scholar]
- George L. Sociological perspectives on life transitions. Annual Review of Sociology. 1993;19:353–373. [Google Scholar]
- Goldman N, Moreno L, Westoff CF. Collection of survey data on contraception: An evaluation of an experiment in Peru. Studies in Family Planning. 1989;20:147–157. [PubMed] [Google Scholar]
- Gregson S, Nyamukapa CA, Garnett GP, Wambe M, Lewis JJC, Mason PR, Anderson RM. HIV infection and reproductive health in teenage women orphaned and made vulnerable by AIDS in Zimbabwe. AIDS Care. 2005;17:785–794. doi: 10.1080/09540120500258029. [DOI] [PubMed] [Google Scholar]
- Hallett TB, Gregson S, Lewis JJC, Lopman BA, Garnett GP. Behaviour change in generalised HIV epidemics: Impact of reducing cross-generational sex and delaying age at sexual debut. Sexually Transmitted Infections. 2007;83:i50–i54. doi: 10.1136/sti.2006.023606. [DOI] [PubMed] [Google Scholar]
- Hallman K. Gendered socioeconomic conditions and HIV risk behaviors among young people in South Africa. African Journal of AIDS Research. 2005;4:37–50. doi: 10.2989/16085900509490340. [DOI] [PubMed] [Google Scholar]
- Hao L, Xie G. The complexity and endogeneity of family structure in explaining children’s misbehavior. Social Science Research. 2002;31:1–28. [Google Scholar]
- Harrison A, Cleland J, Gouws E, Frohlich J. Early sexual debut among young men in rural South Africa: Heightened vulnerability to sexual risk? Sexually Transmitted Infections. 2005;81:259–261. doi: 10.1136/sti.2004.011486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Heard HE. Fathers, mothers, and family structure: Family trajectories, parent gender, and adolescent schooling. Journal of Marriage and Family. 2007;69:435–450. [Google Scholar]
- Hofferth SL, Goldscheider F. Family structure and the transition to early parenthood. Demography. 2010;47:415–437. doi: 10.1353/dem.0.0102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hogan DP, Astone NM. The transition to adulthood. Annual Review of Sociology. 1986;12:109–130. [Google Scholar]
- Hosegood V, Floyd S, Marston M, Hill C, McGrath N, Isingo R, Zaba B. The effects of high HIV prevalence on orphanhood and living arrangements of children in Malawi, Tanzania, and South Africa. Population Studies. 2007;61:327–336. doi: 10.1080/00324720701524292. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jukes M, Simmons S, Bundy D. Education and vulnerability: The role of schools in protecting young women and girls from HIV in Southern Africa. AIDS. 2008;22(Suppl. 4):S41–S56. doi: 10.1097/01.aids.0000341776.71253.04. [DOI] [PubMed] [Google Scholar]
- Lichter DJ. Marriage as public policy (Progressive Policy Institute (PPI) policy report, September) Washington, DC: PPI; 2001. [Google Scholar]
- Lloyd CB. The role of schools in promoting sexual and reproductive health among adolescents in developing countries. New York: Population Council; 2007. Poverty, Gender, and Youth Working Paper No. 6. [Google Scholar]
- Lloyd CB, Blanc AK. Children’s schooling in sub-Saharan Africa: The role of fathers, mothers, and others. Population and Development Review. 1996;22:265–298. [Google Scholar]
- Luke N, Clark S, Zulu EM. The relationship history calendar: Improving the scope and quality of data on youth sexual behavior. Demography. 2011;48:1151–1176. doi: 10.1007/s13524-011-0051-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Luke N, Xu H, Mberu BU, Goldberg RE. Migration experience and premarital sexual initiation in Urban Kenya: An event history analysis. Studies in Family Planning. 2012;43:115–126. doi: 10.1111/j.1728-4465.2012.00309.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Madhavan S. Fosterage patterns in the age of AIDS: Continuity and change. Social Science & Medicine. 2004;58:1443–1454. doi: 10.1016/S0277-9536(03)00341-1. [DOI] [PubMed] [Google Scholar]
- Magnuson K, Berger LM. Family structure states and transitions: Associations with children’s well-being during middle childhood. Journal of Marriage and Family. 2009;71:575–591. doi: 10.1111/j.1741-3737.2009.00620.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mberu BU. Internal migration and household living conditions in Ethiopia. Demographic Research. 2006;14:509–540. [Google Scholar]
- McGrath N, Nyirenda M, Hosegood V, Newell M-L. Age at first sex in Rural South Africa. Sexually Transmitted Infections. 2009;85(Suppl. I):i49–i55. doi: 10.1136/sti.2008.033324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meadows SO, McLanahan SS, Brooks-Gunn J. Stability and change in family structure and maternal health trajectories. American Sociological Review. 2008;73:314–334. doi: 10.1177/000312240807300207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mensch BS, Clark WH, Lloyd CB, Erulkar AS. Premarital sex, schoolgirl pregnancy, and school quality in rural Kenya. Studies in Family Planning. 2001;32:285–301. doi: 10.1111/j.1728-4465.2001.00285.x. [DOI] [PubMed] [Google Scholar]
- Monasch R, Boerma JT. Orphanhood and childcare patterns in sub-Saharan Africa: An analysis of national surveys from 40 countries. AIDS. 2004;18(Suppl.2):S55–S65. doi: 10.1097/00002030-200406002-00007. [DOI] [PubMed] [Google Scholar]
- Morrison DR, Cherlin AJ. The divorce process and young children’s wellbeing: A prospective analysis. Journal of Marriage and Family. 1995;57:800–812. [Google Scholar]
- National AIDS and STI Control Programme (NASCOP), Ministry of Health. Kenya AIDS indicator survey 2007: Final report. 2009 Retrieved from http://www.aidskenya.org/public_site/webroot/cache/article/file/Official_KAIS_Report_20091.pdf.
- National Research Council and Institute of Medicine. Growing up global: The changing transitions to adulthood in developing countries. Panel on transitions to adulthood in developing countries. In: Lloyd CB, editor. Committee on population and board on children, youth, and families. Division of behavioral and social sciences and education. Washington, DC: The National Academies Press; 2005. [Google Scholar]
- Ngom P, Magadi MA, Omuor T. Parental presence and adolescent reproductive health among the Nairobi Urban Poor. Journal of Adolescent Health. 2003;33:369–377. doi: 10.1016/s1054-139x(03)00213-1. [DOI] [PubMed] [Google Scholar]
- Nnko S, Boerma JTJ, Urassa M, Mwaluko G, Zaba B. Secretive females or swaggering males? An assessment of the quality of sexual partnership reporting in Rural Tanzania. Social Science & Medicine. 2004;59:299–310. doi: 10.1016/j.socscimed.2003.10.031. [DOI] [PubMed] [Google Scholar]
- Nyamukapa C, Gregson S. Extended family’s and women’s roles in safeguarding orphans’ education in AIDS-afflicted Rural Zimbabwe. Social Science & Medicine. 2005;60:2155–2167. doi: 10.1016/j.socscimed.2004.10.005. [DOI] [PubMed] [Google Scholar]
- Nyamukapa CA, Gregson S, Lopman B, Salto S, Watts HJ, Monasch R, Jukes MCH. HIV-associated orphanhood and children’s psychosocial distress: Theoretical framework tested with data from Zimbabwe. American Journal of Public Health. 2008;98:133–141. doi: 10.2105/AJPH.2007.116038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Operario D, Pettifor A, Cluver L, MacPhail C, Rees H. Prevalence of parental death among young people in South Africa and risk for HIV infection. Journal of Acquired Immune Deficiency Syndromes. 2007;44:93–98. doi: 10.1097/01.qai.0000243126.75153.3c. [DOI] [PubMed] [Google Scholar]
- Orubuloye IO, Caldwell JC, Caldwell P. Perceived male sexual needs and male sexual behaviour in southwest Nigeria. Social Science & Medicine. 1997;44:1195–1207. doi: 10.1016/s0277-9536(96)00254-7. [DOI] [PubMed] [Google Scholar]
- Osborne C, McLanahan S. Partnership instability and child well-being. Journal of Marriage and Family. 2007;69:1065–1083. [Google Scholar]
- Palermo T, Peterman A. Are female orphans at risk for early marriage, early sexual debut, and teen pregnancy? Evidence from Sub-Saharan Africa. Studies in Family Planning. 2009;40:101–112. doi: 10.1111/j.1728-4465.2009.00193.x. [DOI] [PubMed] [Google Scholar]
- Pettifor AE, van der Straten A, Dunbar MS, Shiboski SC, Padian NS. Early age at first sex: A risk factor for HIV infection among women in Zimbabwe. AIDS. 2004;18:1435–1442. doi: 10.1097/01.aids.0000131338.61042.b8. [DOI] [PubMed] [Google Scholar]
- Plummer ML, Ross DA, Wight D, Changalucha J, Mshana G, Wamoyi J, Hayes RJ. “A bit more truthful”: The validity of adolescent sexual behaviour data collected in rural Northern Tanzania using five methods. Sexually Transmitted Infections. 2004;80(Suppl. II):ii49–ii56. doi: 10.1136/sti.2004.011924. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Poulin M. Reporting on first sexual experience: The importance of interviewer-respondent interaction. Demographic Research. 2010;22(article 11):237–288. doi: 10.4054/DemRes.2010.22.11s. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Reniers G. Marital strategies for regulating exposure to HIV. Demography. 2008;45:417–438. doi: 10.1353/dem.0.0002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rwenge M. Sexual risk behaviors among young people in Bamenda, Cameroon. International Family Planning Perspectives. 2000;26:118–123. 130. [Google Scholar]
- Ryan S, Franzetta K, Schelar E, Manlove J. Family structure history: Links to relationship formation behaviors in young adulthood. Journal of Marriage and Family. 2009;71:935–953. doi: 10.1111/j.1741-3737.2009.00645.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sambisa WC, Stokes S. Rural/urban residence, migration, HIV/AIDS, and safe sex practices among men in Zimbabwe. Rural Sociology. 2006;71:183–211. [Google Scholar]
- Shanahan MJ. Pathways to adulthood in changing societies: Variability and mechanisms in life course perspective. Annual Review of Sociology. 2000;26:667–692. [Google Scholar]
- South SJ, Haynie DL, Bose S. Residential mobility and the onset of adolescent sexual activity. Journal of Marriage and Family. 2005;67:499–514. [Google Scholar]
- Stack S. The effect of geographic mobility on premarital sex. Journal of Marriage and the Family. 1994;56:204–208. [Google Scholar]
- Sun Y, Li Y. Children’s well-being during parents’ marital disruption process: A pooled time-series analysis. Journal of Marriage and Family. 2002;64:472–488. [Google Scholar]
- Teachman JD. The living arrangements of children and their educational well-being. Journal of Family Issues. 2008;29:734–761. [Google Scholar]
- Townsend N, Madhavan S, Tollman S, Garenne M, Kahn K. Children’s residence patterns and educational attainment in rural South Africa, 1997. Population Studies. 2002;56:215–225. [Google Scholar]
- Uhlenberg P, Mueller M. Family context and individual well-being: Patterns and mechanisms in life course perspective. In: Mortimer JT, Shanahan MJ, editors. Handbook of the life course. New York: Kluwer Academic/Plenum Publishers; 2003. pp. 123–148. [Google Scholar]
- UNAIDS. Report on the global AIDS epidemic. New York: UNAIDS; 2008. [Google Scholar]
- UNAIDS, UNICEF, and USAID. Children on the brink 2004: A joint report of new orphan estimates and a framework for action. New York: UNAIDS; 2004. [Google Scholar]
- United Nations. World youth report 2007, young people’s transition to adulthood: Progress and challenges. New York: Department of Economic and Social Affairs, United Nations; 2007. [Google Scholar]
- Varga CA. How gender roles influence sexual and reproductive health among South African adolescents. Studies in Family Planning. 2003;34:160–172. doi: 10.1111/j.1728-4465.2003.00160.x. [DOI] [PubMed] [Google Scholar]
- White MJ, Muhidin S, Andrzejewski C, Tagoe E, Knight R, Reed H. Urbanization and fertility: An event-history analysis of coastal Ghana. Demography. 2008;45:803–816. doi: 10.1353/dem.0.0035. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wu LL. Effects of family instability, income, and income instability on the risk of a premarital birth. American Sociological Review. 1996;61:386–406. [Google Scholar]
- Wu LL, Thomson E. Race differences in family experience and early sexual initiation: Dynamic models of family structure and family change. Journal of Marriage and Family. 2001;63:682–696. [Google Scholar]