

Abstract
Introduction
There is ongoing debate regarding the relative impact of youth behavior problems on placement change in child welfare compared to the impact of placement change on behavior problems. Existing studies provide some support for either perspective. The purpose of this study was to prospectively examine the relationships of behavior problems and placement change in a nationally representative sample of youths in the National Survey of Child and Adolescent Well-Being (NSCAW).
Methods
The sample for the present study consists of 422 youths having only out-of-home placements over the course of the NSCAW study. We used multi-level path analysis of a cross-lag design to examine reciprocal effects of behavior problems and placement change over time.
Results
We found that behavior problems predicted placement change consistently for the sample and in analyses by gender and age. In contrast, we found only isolated effects of placement changes on subsequent behavior problems.
Conclusions
In keeping with recommendations from a number of professional bodies, we suggest that initial and ongoing screening for internalizing and externalizing behavior problems be instituted as part of standard practice for youths entering or transitioning in the child-welfare system.
Introduction
For more than a quarter century, child welfare policy and practice have aimed to achieve permanency and stability for abused and neglected children removed from their primary caretaker and placed into out-of-home care. Despite these efforts, a significant number of children in out-of-home care have continued to experience extended stays in care and repeated placement changes (U.S. Department of Health and Human Services, 2007). The Adoption and Safe Families Act of 1997 (Public Law 105-89) placed renewed emphasis on permanency and adoption and encouraged expansion of “state standards to ensure quality services for children in foster care” U.S. Department of Health and Human Services, n.d.). Since then, states have been required to collect and report data on placement stability. While more than 80 percent of states meet placement stability performance standards for shorter periods of time in care, the percentage decreases significantly when children stay in care longer (Child Welfare Outcomes, 2003). There is further indication from regional studies that between 25% to 50% of children experience more than two placements while in out-of-home care, and that about 10% to 15% experience very high numbers of placement changes (Pardeck, 1984a; Usher, Randolph & Gogan, 1999; Webster, Barth & Needell, 2000). Such instability is almost universally considered to be harmful (Barber, 2003).
Empirical studies have for some time examined predictors as well as outcomes of placement stability (e.g, Barber et al., 2001; Cooper et al, 1987; James et al., 2004; Pardeck, 1984b; Palmer, 1996; Webster et al., 2000). Studies vary widely in methodology and rigor, but four variables have consistently been linked to a higher number of placement changes –higher levels of behavioral or emotional problems, age of the child, extended stays in care and placement type (Barth et al., 2007; Barber et al., 2001; James, 2004; Leathers, 2006; Webster et al., 2000). Findings regarding the association between placement instability and other factors, such as gender and race/ethnicity of the child, characteristics of the biological family or caseworker characteristics have remained equivocal (Cooper et al., 1987; Palmer, 1996; Pardeck, 1983; Stone & Stone, 1983).
Of particular interest to the child welfare community is the relationship between placement instability and behavior problems given growing evidence of the prevalence of emotional and behavioral problems among children in foster care (Child Welfare League of America, 2005; McMillen et al., 2005). The majority of empirical studies that have investigated the relationship between the two variables have been cross-sectional, therefore precluding any definitive inferences about the directionality of effects. Assignment of placement change as either independent or dependent variable has been conceptually driven and has been guided by two basic hypotheses: (1) Children experience placement instability because of their attributes upon entering care; more specifically, the presence of behavior problems leads to a higher risk of experiencing more frequent placement changes. (2) Placement instability causes poor developmental outcomes, including increased levels of behavior problems. This latter hypothesis is generally grounded in notions of attachment theory and argues that frequent placement changes undermine children’s ability to build stable relationships (e.g., Gauthier, Fortin & Jéliu, 2004), ultimately leading to a host of adverse outcomes in the short- and long-term. This research inevitably suggests a need for the child welfare system to improve well-being outcomes by prioritizing services and interventions aimed at stabilizing children’s out-of-home care experience. At this point, there is empirical support for both perspectives. Studies investigating behavior problems as a predictor to placement changes have found higher levels of behavior problems, in particular externalizing problems, to be one of the most consistent predictors of frequent placement changes (Barth et al., 2007; Barber et al., 2001; Fanshel & Shinn, 1978; James, 2004; Leathers, 2006; Olsen, 1982; Palmer, 1996; Webster et al., 2000). Fewer studies have attempted to examine whether placement changes are the cause of behavior problems. Empirical inquiries have produced inconsistent findings. Several studies demonstrate that a higher number of placement changes is associated with adverse developmental outcomes (Eckenrode, Rowe, Lairde & Brathwaite, 1995; Lewis, Dozier, Ackerman & Sepulveda-Kozakowski, 2007; Newton, Litrownik, and Landsverk 2000; Rubin, O’Reilly, Luan & Localio, 2007; Zima et al., 2000); other research on preschoolers in foster care reports no variation in child outcomes by placement length or number of placements (Pears & Fisher, 2005a, 2005b).
Despite these findings, determining the precise relationship between behavior problems and placement changes has remained difficult given methodological constraints (Berger, Bruch, Johnson, James & Rubin, under review). A few studies have tried to address these constraints and get closer at disentangling the complex relationship between behavior problems and placement changes. Two studies deserve further attention. In an often cited 2000 study, Newton and colleagues tried to specifically disentangle the relationship between behavior problems and placement change, using child welfare administrative and clinical survey data in an 18-month longitudinal foster care cohort study. The researchers divided their sample of 415 subjects into two groups. One group scored below borderline cutpoints on the three Child Behavior Checklist broad-band scales (internalizing, externalizing and total behavior problems); the second group scored above on at least one cutpoint. The study generated several important findings: (a) externalizing behavior problems are a significant predictor of a higher number of placement changes; (b) frequent placement changes contribute negatively to both internalizing and externalizing behavior problems; and (c) a high number of placement changes even affected children who initially did not score above the borderline cut point. Results ultimately suggested that behavior problems should be conceptualized as both a cause as well as an effect of placement disruptions. A recent study by Rubin et al. (2007) used data from the National Survey on Child and Adolescent Well-Being (NSCAW), a prospective national cohort study, to examine the independent impact of placement stability on behavioral outcomes, controlling for baseline attributes. Using a propensity score matching approach, the authors found that children experiencing instability in foster care were more likely to have behavior problems regardless of their initial risk level. However, the study did not use all waves of data, included youths under age two at baseline (with temperament as a proxy for behavior problems), and used categorical, rather than continuous measures of behavior problems (i.e., normal vs. abnormal) and placement stability (i.e., early stability, late stability, unstable) .
The current study uses a prospective multilevel cross-lag modeling approach to further disentangle the complex relationship between placement change and behavior problems. Using data from NSCAW, the first national probability study of children and families involved with the child welfare system, our analysis capitalizes on the availability of placement as well as clinical survey data collected at several data points over a 36-month period. Beyond examining the relationship between placement change and behavior problems, this study also investigates how age, gender and placement status moderate this relationship.
Methods
Overview
NSCAW was authorized under the Personal Responsibility and Work Opportunity Reconciliation Act of 1996 (P.L. 104-193) and is the first national prospective study to examine the experiences of children and families involved with the child welfare system. NSCAW used a stratified two-stage cluster sampling strategy to select 100 primary sampling units (PSUs) from a national sampling frame, with the probability of PSU selection proportional to the size of the PSU’s service population. Of the 100 PSUs identified by the sampling strategy, the NSCAW study ultimately collected child-level data in 92 PSUs representing 96 counties in 36 states. The NSCAW study has involved four waves of data collection to date (baseline, 12 months, 18 months and 36 months). The sampling approach used in the study generated national estimates for the full population of children and families entering the child welfare system (NSCAW Research Group, 2002). Unless otherwise indicated all parameters presented in this article are weighted.
Sample
In participating counties, 5501 children were selected from among the population of children aged birth to 15 (one 16 year-old at the time of the baseline interview), for whom an investigation of abuse or neglect had been opened by the child welfare system during a 15-month period beginning in October 1999. Approval for this study was given by the U.S. Office of Management and the Budget and the Institutional Review Boards (IRB) of the Research Triangle Institute, University of California at Berkeley, Children’s Hospital in San Diego; and numerous state or county institutional review boards (IRB) representing PSUs involved with the study. The sample for the current analysis includes those children who: 1) had been in out-of-home care for the entire 36-month study period, 2) were 2-15 years old at baseline [children younger than age 2 were excluded because scores on our measure of behavioral problems were not available], and 3) had complete data on study variables. This yielded a final sample of 422 youths aged 2-15 years.
Procedures
Field representatives conducted face-to-face interviews with child welfare workers and caregivers and entered all data directly into laptop computers. Baseline interviews with social workers were completed an average of 5.1 months after the onset of the child welfare investigation (SD = 2.1 months) and caregiver interviews were completed on average 5.5 months after the investigation (SD = 2.50months). Wave 2 was conducted 13.7 (SD=2.7) months after baseline and consisted of interviews with case-managers only; data that were relevant to the present study. Wave 3 and Wave 4 follow-up interviews with caregivers were conducted an average of 20.5 (SD=2.8) and 36.8 (SD=2.7) months after the onset of the child welfare investigation.
Measures
Demographics
Demographics were collected as part of the initial case identification procedures and confirmed by caregiver and child-welfare worker interviews.
Number of placements
In the NSCAW study, placement into out-of-home care was defined as any removal from home with at least one overnight stay. To be counted as a placement change, the child’s physical location of residence needed to have changed. Hence, if the child fled placement for several days but was returned to the same residence, no placement change would have been recorded. In contrast, if the child was placed into a shelter or detention, a placement change would have occurred.
Behavioral problems
The Child Behavior Checklist (CBCL), a widely used and psychometrically established measure (Achenbach, 1991), was used to estimate emotional and behavioral problems in the clinical range for youth. Two caregiver report forms of the CBCL were used—one for children ages 2 to 3 years and another for children ages 4 to 18 years. Children falling at or above the clinical cut-point (T ≥ 64) on internalizing or externalizing problems were categorized as having clinically significant levels of need.
Analyses
We conducted a series of multilevel cross-lag path analyses. All analyses controlled for the nested design of the NSCAW study and applied sampling weights in order to allow generalization back to the population of youths in child welfare who had at least one out of home placement. The level of aggregation was the PSU (k=92). The path analytic approach has advantage of testing the sequential relationships of the key variables in the model (i.e. behavior problems and placement changes) reflecting the longitudinal design of the study and the potential bi-directionality of effects (i.e., the effects of behavior problems on subsequent placement changes and the effects of placement changes on subsequent behavior problems). Figure 1 shows the general path analytic model to be tested. We conducted a series of analyses to examine global effects of behavior problems on placement change and placement change on behavior problems, and two sets of analyses to examine potential moderator effects (i.e., age and gender) of behavior problems and placement changes. We also conducted analyses comparing youths with 2 or fewer placement changes to those with 3 or more placement changes and results were substantively the same as those presented below.
Figure 1.
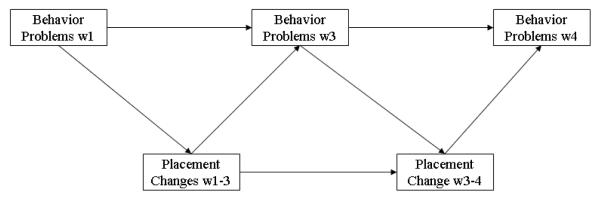
Path Analytic Model of Reciprocal Effects of Behavior Problems and Placement Changes.
Note: w=wave, Behavior problems were assessed only at waves 1, 3, and 4; w1-3 indicates number of placement changes between waves 1 and 3; w3-4 indicates number of placement changes between waves 3 and 4.
Results
Table 1 presents descriptive data for the study sample. As shown, the sample was predominantly non-Hispanic African-American although there was some variability in race/ethnic diversity. Table two shows the proportion of youths at each wave meeting clinical criteria for internalization, externalizing, and both internalizing and externalizing problems. For the overall analysis and analyses examining effects of age, gender and in-home vs. out-of-home placement at baseline, we report overall model fit as well as path coefficients and significance level. We describe path coefficients and refer to effect sizes to describe the magnitude of effects (Cohen, 1988) .
Table 1.
Sample Demographics
| % | Mean (se) | |
|---|---|---|
|
|
||
| Age | ||
| 2-5 | 25.6 (5.4) | |
| 6-10 | 50.9 (5.9) | |
| 11+ | 23.5 (3.6) | |
| Gender | ||
| Male | 48.7 (6.8) | |
| Female | 51.3 (6.8) | |
| Race | ||
| Black | 49.2(6.4) | |
| White | 32.2(5.7) | |
| Hispanic | 13.3(4.6) | |
| Other | 5.3(2.6) | |
| CBCL T-Scores | ||
| CBCL Externalizing (w1) | 58.59(1.35) | |
| CBCL Externalizing (w3) | 56.68(1.67) | |
| CBCL Externalizing (w4) | 56.72(1.17) | |
| CBCL Internalizing (w1) | 56.00(1.35) | |
| CBCL Internalizing (w3) | 53.47(1.30) | |
| CBCL Internalizing (w4) | 52.92(1.01) | |
| Number of OOH placements | ||
| Number of OOH w1-w3 | 1.92(0.15) | |
| Number of OOH w3-w4 | 0.28(0.06) | |
Notes: N=422: w = wave; OOH = out of home placement; N of Number of OOH w1-w3 = number of out-of-home placements from Wave 1 to Wave 3; Number of OOH w3-w4 = number of out-of-home placements from Wave 3 to Wave 4.
Overall model
Two separate path analytic models were estimated to examine overall effects for externalizing and internalizing behavior problems. In Figure 2 and subsequent figures, the path coefficients are arranged with the externalizing behavior problems coefficient labeled with the superscript “a” and placed above the coefficient for internalizing behavior problems (labeled with the superscript “b”). As shown in Figure 2, both externalizing (p <.01) and internalizing behavior problems (p < .001) significantly predicted placement changes between Waves 1-3 with small to medium effect sizes. Externalizing (p < .001) and internalizing (p < .01) behavior problems assessed at Wave 3 also significantly predicted placement changes between Waves 3-4, showing an effect size similar to the Wave 1 effect for externalizing problems but a smaller effect size for internalizing behavior problems relative to Wave 1. Placement changes between Waves 1-3 predicted more externalizing behavior problems at Wave 3 (p <.01) but not internalizing problems. Placement changes between Waves 3-4 did not significantly predict behavior problems at Wave 4.
Figure 2.
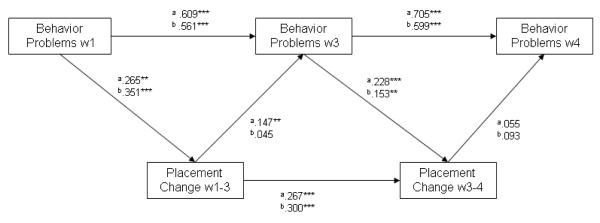
Overall Model of CBCL Externalizing/Internalizing Disorder and Placement Changes Over Four Waves.
a Externalizing X2=.556, p=.9064, CFI=1.000, TLI=1.034, RMSEA=.000, SRMR=.007.
b Internalizing X2=5.598, p=.1329; CFI=.986, TLI=.952, RMSEA=.045, SRMR=.030.
Note: N=422 (Our of home only)
Significance tests two tailed, *p<.05, **p<.01, ***p<.001
Moderated models
We next conducted three separate multi-group multi-level path analyses in order to determine if age or gender had an impact on the relationship between behavior problems and placement changes. This approach allows for simultaneous estimation of path coefficients for each of the levels the moderator variables of interest: age (2-5 years, 6-10 years, and 11 years and older, at baseline) and gender (male, female).
Age
We conducted two multi-group multi-level path analytic models (one for externalizing problems and the other for internalizing problems), simultaneously estimating path coefficients for each of the three age groups (2-5 years, 6-10 years, and 11 years and older, at baseline). Figure 3 shows results for these models. As in the previous model, the path coefficients are arranged so that the top row indicates externalizing problem coefficients and the bottom row internalizing problem coefficients. The coefficients read from left to right: 2-5 years/6-10 years/11 years and older at baseline. Thus at Wave 3 age groups were 4-8 years, 8-12 years and 13+ years, and at Wave 4 were 5-9, 9-13 and 14+ years. However, we refer to the groups based on their ages at baseline. As shown in Figure 3, externalizing and internalizing behavior problems at Wave 1 predicted placement changes between Waves 1-3 for the 6-10 year olds (p’s < .001), and the 11+ age group (p < .01 for externalizing; p < .001 for internalizing) but not for the youngest age group. Placement changes between Waves 1-3 did predict behavior problems at Wave 3 only for externalizing problems for the 6-10 year age group (p < .05). Externalizing and internalizing behavior problems at Wave 3 significantly predicted placement changes between Waves 3-4 for externalizing behavior problems for the 2-5 age group (p < .05) (although this was a small effect size) and for both externalizing (p < .001) and internalizing (p < .01) problems for the 11+ age group (medium effect sizes). As in the previous model, placement changes between Waves 3-4 did not significantly predict behavior problems at Wave 4.
Figure 3.
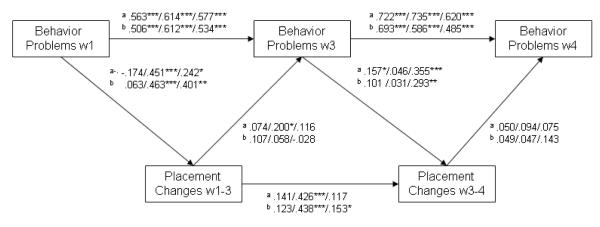
Behavior Problems and Placement Changes by Age over Four Waves.
a Externalizing behavior problems: X2=11.264; p=.2581; cfi=.993, TLI=.977, RMSEA=.042, SRMR=.031.
b Internalizing behavior problems: X2=15.527; p=.0775; CFI=.973, TLI=.911, RMSEA=.072, SRMR=.042.
Note: N=422; Order of coefficients: age 2-5 (n=109)/age 6-10 (n=169)/age 11+(n=144); Significance tests two tailed: *p<.05, **p<.01, ***p<.001
Gender
The final set of analyses examined whether the relationship of behavior problems and placement change varied by gender. As shown in Figure 4, externalizing (p < .01) and internalizing (p < .001) behavior problems at Wave 1 significantly predicted placement changes between Waves 1-3 for boys but not for girls. The path coefficients represent a medium effect size for externalizing problems and a large effect size for internalizing problems. Placement changes between Waves 1-3 predicted increased externalizing problems at Wave 3 only for girls (p < .01). All of these latter effect sizes were in the small to medium size range. Externalizing behavior problems at Wave 3 significantly predicted placement changes between Waves 3-4 for both boys and girls (p’s < .01) and internalizing problems predicted placement changes only for boys (p < .01). Finally, placement changes between Waves 3-4 did not significantly predicted externalizing behavior problems at Wave 4 for boys or girls.
Figure 4.
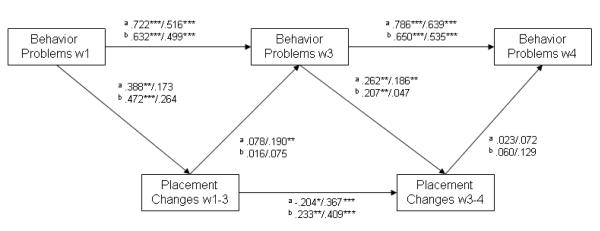
Behavior Problems and Placement Changes by Gender over Four Waves.
a Externalizing behavior problems: X2(3)=1.196; p=0.9771; CFI=1.000, TLI=1.054, RMSEA=0.0000, SRMR=.009.
b Internalizing behavior problems: X2(3)=7.771; p=.2553; CFI=.991, TLI=.968, RMSEA=.037, SRMR=.033.
Note: N=422; Order of coefficients: age = male (n=202)/female (n=220); Significance tests two tailed: *p<.05, **p<.01, ***p<.001
Discussion
The present study found that behavior problems predict placement changes more consistently relative to placement changes predicting behavior problems. In contrast to previous studies that used only one time point, this study prospectively examined these relationships. Specifically, in the overall model, externalizing and internalizing problems at Wave 1 and at Wave 3 both consistently predicted placement changes during the Wave 1-3 and Wave 3-4 periods, respectively. In contrast, placement changes between Wave1-3 predicted internalizing behavior problems at Wave 3 but no other effects of placement change on behavior problems was found in the overall model.
The general patterns found in the overall model held when separate multigroup analyses considered effects of youth age and gender, although some exceptions were identified. For example, Wave 1 behavior problems in preschoolers did not influence placement changes and this finding is comparable to a previous study (Pears and Fisher, 2005a, 2005b). In contrast, Wave 3 externalizing behavior problems did predict placement changes for this group. This may partially reflect children’s older age by Wave 3 and subsequent caregiver difficulty in managing behaviors of older youths. Conversely, age-group analyses demonstrated that behavior problems at Wave 1 - but not at Wave 3 - predicted placement changes for 6-10 year-olds. In a more consistent finding, behavior problems at both Waves 1 and 3 predicted subsequent placement changes for youth who were 11 years of age and older at baseline. However, there were isolated instances where placement change predicted subsequent behavior problems and these instances are discussed later in this section.
In regard to gender differences, both externalizing and internalizing behavior problems predicted placement changes for boys at both Wave 1 and Wave 3, while only externalizing behavior problems at Wave 3 predicted placement changes for girls. This may reflect lower levels of behavior problems in girls or greater caregiver tolerance for such behavior in girls.
While stronger and more consistent effects were seen examining youth behavior problems on subsequent placement changes, we found some reciprocal effects of placement changes on behavior problems. For example, in the overall model, we found small effects for placement changes between Waves 1-3 in predicting externalizing behavior problems at Wave 3. With regard to age and gender, we found a small effect for impact of placement changes on externalizing behaviors for 6-10 year olds and on internalizing behaviors in girls. We found no significant effects of placement change on subsequent externalizing or internalizing behavior problems between Waves 3-4 in any of the models. While there was some impact of placement change on subsequent behavior problems, the far more consistent and larger effects of behavior change on subsequent placement change should be attended to.
Age differences in effects of placement changes on subsequent externalizing problems
The fact that placement changes were only associated with subsequent behavioral problems for middle childhood and adolescence may reflect less caregiver indulgence toward these children than toward the youngest children. Recalling that the age category refers to ages at baseline, this cohort was 6-10 years old at baseline and 8-12 years old by wave 3. These are no longer the youngest children, toward whom caregivers may feel particularly tender and thus buffer from the negative effects of placement moves. One consequence may be more acting out by children. In addition, 8-12 year olds are increasingly exposed to pre-teen and teenage role modeling, which may lead to attitudes that are less tolerable to caregivers than even the expressed unhappiness of younger children. These interpretations, however, do not explain why placement changes were associated with externalizing problems for middle childhood and not for adolescence, a period generally considered to be even more challenging. One possibility is that adolescents’ stronger peer affiliations may buffer them from the effects of placement instability; however placement changes often imply neighborhood and school changes, which would undermine those peer networks. Thus, further work is needed to better understand the lack of effect of placement change on subsequent behavioral problems for adolescents.
Gender difference in effects of placement changes
The finding that placement changes did not predict externalizing problems for boys appears to contradict Ryan and Testa’s (2005) finding that placement instability increased risk of delinquency for boys. For girls there was only one instance where placement changes predicted subsequent externalizing behavior problems. While the effect size was small, this finding warrants further exploration. For example, females may respond to placement disruption differently than males, however the mechanisms by which this occurs remain to be identified.
Why did placement change not consistently predict subsequent behavioral problems?
The most puzzling finding reported here is that placement changes did not reliably predict subsequent behavioral problems. There may be a number of reasons for this. First, in contrast to studies by Rubin et al. (2007) and Newton et al. (2000) we used a prospective rather than cohort design assessing behavior problems and placement changes at multiple time points. This allowed us to examine the sequencing of behavior problems and placement changes. Second, other studies examining the impact of placement change focused on other outcomes such as educational functioning (Eckenrode et al., 1995) or help-seeking patterns (Zima et al., 2000), or used samples with characteristics different from ours (e.g., young adopted children) (Lewis et al., 2007).
We can speculate that new caregivers are less likely to detect behavioral problems than caregivers who have had children in their homes for longer periods of time. Thus, decreased measurement sensitivity may affect detected changes in child behaviors. Future research could test this speculation at least for youth 11 and over by comparing youth self-reported behaviors with caregiver reports across multiple points in time.
Another possible explanation is that placement changes are not as damaging as generally believed. Children may generally possess sufficient resilience to sustain functioning despite placement changes. A recent qualitative study of former foster youth with multiple placement moves highlights a range of coping strategies utilized by youth to adapt after a placement disruption (Unrau, Seita & Putney, 2008). The ability to cope despite experiences of loss could account for the absence of significant associations between wave 1-3 placement changes and subsequent internalizing problems as well as between wave 3-4 placement changes and either internalizing or externalizing problems at wave 4.
In addition, for children engaged in the child welfare system, the alternative to out of home placements may not be stability. Maltreating families tend to move more than other families (Eckenrode, Rowe, Lairde & Brathwaite, 1995) and to experience changes in household composition (e.g., attendant to partner violence or a parent being incarcerated) that may in some respects be as challenging for children as out of home placements. Indeed, there is some evidence that outcomes for youth who returned to their families after placement in foster care have more behavioral and emotional problems than youth who do not return (Taussig, Clyman & Landsverk, 2001). Our findings combined with Eckenrode et al.’s (1995) finding that foster care did not moderate the effects of general placement mobility on academic achievement, may imply that out-of-home placements do not generally disadvantage children relative to other children in the child welfare system.
These findings may also reflect the generally low mean number of placement changes, which averaged under 2 between wave 1 and 3 and just over a quarter of one change between wave 3 and 4 (Table 1). Alternatively, previous research has linked worse outcomes with multiple placement changes (Dozier et al., 2007; Ryan and Testa 2005; Rubin et al., 2007; Zima et al., 2000), with the highest risks being associated with having had a high number of such moves (Newton et al., 2000; Thornberry et al. 1999). For example, Thornberry and colleagues (1999) found greatly increased risk of delinquency for youth with more than four placement changes. Thus, there may be a step function such that fewer than one or two changes result in lower risk whereas some number greater than two does increase risk. However, when we ran a model comparing youths with up to two placement changes (about 55% of our sample) with youths with three or more placement changes, we found no evidence of placement change predicting subsequent behavior problems. However, there may be other thresholds not identified in the present study and this should be explored further.
Finally, it is possible that the effects of placement changes are not entirely negative. In general, youths may change placement due to a number events (e.g., youth behavior problems, foster-parent availability, availability of kinship care, court rulings) (James, 2004). Children who have been removed from their homes of origin typically need to learn a range of new behaviors and ways of interpreting others’ behaviors. For at least some of these children, new homes may present new opportunities to relate effectively with caregivers, foster siblings, and peers at school (see Unrau et al., 2008). Such second (or greater) chances could counteract the trauma attendant to placement moves. For example, a child who has been confrontational with an initial set of foster parents might try more cooperative behaviors in a new home, unencumbered by resentment of discipline incurred from previous infractions. In turn, the new parents may be more able to see appropriate behaviors because they don’t have a negative history with her.
Clinical, Policy, and Research Implications
This data strongly suggests that behavior problems evidenced in the time period following an investigation and initial placement in out-of-home care impact the number of placement changes youth experience in subsequent months. Both externalizing and internalizing problems were found to affect placement changes but there was also overlap in symptoms suggesting even more complexity than that represented in analyses presented in this paper. The cost associated with each placement change can be substantial and work done in the United Kingdom should be replicated in the United States to provide a deeper understanding of these issues (Ward & Holmes 2008). The additional complexity of behavior problems and the costs associated with placement change supports the importance of early identification and treatment of behavior problems within a constrained period following placement in foster care.
The present study identified a small impact of placement changes between Waves 1 and 3 on externalizing symptom development in 6-10 year olds and of internalizing problems among girls. It may be that certain subpopulations of youth entering out-of-home care will require targeted interventions to mollify the effect of placement changes on the development of certain behaviors. A more in-depth analysis of these issues could help us to better understand the impact of placement changes on the development of behavioral problems.
Limitations
Some limitations of the present study should be noted. First, we did not examine the impact of different types of placement changes and there may be differential effects of placement to foster care vs. congregate care. For example, we know that older age correlates with more placements in congregate care settings which may have a positive or negative effect. Second, we did not stratify by the numbers of placement changes experienced by youths. Although there was a wide range of placement changes, the mean number was low suggesting that most youths in foster care experience few placement changes. Exploration of this issue was beyond the purview of the present study but is an area for future research. Third, the variables used in the present study did not mirror other studies examining similar issues. However, the present study made use of all available waves of data to inform the prospective approach, modeling, and analyses. Finally, we did not examine onset of new behavior problems nor did we stratify by number of placement changes experienced. We chose our analytic approach to include continuous measures of both behavior problems and placement change in order to capture the full range of the variables, rather than using data reduction approaches that could limit the variability to be included in the analyses.
Conclusions
Because behavioral problems tend to persist, and because behavior problems affect stability of placement, these findings suggest that initial screening and assessment for emotional or behavioral problems have the potential to reduce not only emotional distress but to decrease future placement disruptions among children in the child welfare system. The need for such surveillance has been asserted in national standards proposed by the Child Welfare League of America (Child Welfare League of America, 1988), the American Academy of Pediatrics (American Academy of Pediatrics Committee on Early Childhood Adoption and Dependent Care, 1994, 2002), and the American Academy of Child and Adolescent Psychiatry (American Academy of Child and Adolescent Psychiatry, 2001, 2003). These recommendations are all highly convergent, and suggest that all children should receive: (1) a mental health screening when placed into foster care; followed by (2) a comprehensive mental health assessment by a mental health professional within a month of being placed into foster care. They also outline the need for a systematic, coordinated approach to the delivery of mental health services to meet children’s ongoing mental health needs, incorporating (3) repeat screenings at the time of transitions in living arrangements, and (4) referral to mental health services if need is confirmed. Unfortunately, only a third of key informants in state and county mental health agencies report being aware of these standards, and only about half of mental health agencies play significant roles in the design of services to child welfare populations (Raghavan, Inkelas, Franke, & Halfon, 2007). Absent shared case-finding and coordinated service delivery mechanisms with their respective mental health departments, child welfare agencies may be unable to achieve better performance on placement standards on their own.
Table 2.
Prevalence of Externalizing, Internalizing, and both Externalizing and Internalizing Problems Meeting the Clinical Cutoff
| Externalizing | Internalizing | Externalizing & Internalizing |
|
|---|---|---|---|
|
|
|||
| n (%) | n (%) | n (%) | |
|
|
|||
| Wave 1 | 164 (36.9) | 132 (23.8) | 90 (16.4) |
| Wave 3 | 169 (30.4) | 113 (17.4) | 86 (12.0) |
| Wave 4 | 150 (27.6) | 109 (20.2) | 82 (16.6) |
Note: N=422; Clinical cutoff score is >= 64; n’s are unweighted; Percents are weighted
Acknowledgements
This work was primarily supported by NIMH grants R01MH059672 (PI: Landsverk) and in part by R01MH072961 (PI: Aarons)
Reference List
- American Academy of Child and Adolescent Psychiatry. 2001 [Google Scholar]
- American Academy of Child and Adolescent Psychiatry. 2003 [Google Scholar]
- Achenbach TM. The derivation of taxonomic constructs: A necessary stage in the development of developmental psychopathology. Cicchetti, Dante. 1991;3:43–74. [Google Scholar]
- The Adoption and Safe Families Act. 1997 [Google Scholar]
- American Academy of Pediatrics Committee on Early Childhood Adoption and Dependent Care Health Care of Children in Foster Care. Pediatrics. 1994;93:335–338. [PubMed] [Google Scholar]
- American Academy of Pediatrics Committee on Early Childhood Adoption and Dependent Care Health care of children in foster care. Pediatrics. 2002;100:536–541. [PubMed] [Google Scholar]
- Barber JG. Social work through the lifecycle. Tertiary Press; Melbourne,Australia: 2003. [Google Scholar]
- Barber JG, Delfabbro PH, Cooper LL. The predictors of unsuccessful transition to foster care. The Journal of Child Psychology and Psychiatry. 2001;42:785–790. [PubMed] [Google Scholar]
- Barth RP, Lloyd EC, Green RL, James S, Leslie LK, Landsverk J. Predictors of placement moves among children with and without emotional and behavioral disorders. Journal of Emotional and Behavioral Disorders. 2007;15(1):46–55. [Google Scholar]
- Berger LM, Bruch SK, Johnson EI, James S, Rubin D. Estimating the “impact” of out-of-home placement on child well-being: Approaching the problem of selection bias. Child Development. doi: 10.1111/j.1467-8624.2009.01372.x. (In review) [DOI] [PMC free article] [PubMed] [Google Scholar]
- Child Welfare League of America . Standards for Health Care Services for Children in Out-of-Home Care. Child Welfare League of America; Washington, DC: 1988. [Google Scholar]
- Child Welfare League of America . Residential Group Care Quarterly. Child Welfare League of America; Washington, DC: 2005. [Google Scholar]
- Children’s Bureau in the U.S. Department of Health and Human Services Child Welfare and Outcomes Report 2003: Annual Report. 2006 [Google Scholar]
- Cohen J. Set correlation and contingency tables. Applied Psychological Measurement. 1988;12(4):425–434. [Google Scholar]
- Cooper CS, Peterson NL, Meier JH. Variables associated with disrupted placement in a select sample of abused and neglected children. Child Abuse & Neglect. 1987;11(1):75–86. doi: 10.1016/0145-2134(87)90035-4. [DOI] [PubMed] [Google Scholar]
- Dozier CL, Vollmer TR, Borrero JC, Borrero CS, Rapp JT, Bourret J, et al. Assessment of preference for behavioral treatment versus baseline conditions. Behavioral Interventions. 2007;22(3):245–261. [Google Scholar]
- Dozier M, Grasso D, Lindhiem O, Lewis E. The role of caregiver commitment in foster care: Insights from the This Is My Baby Interview. Oppenheim, David. 2007 [Google Scholar]
- Eckenrode J, Rowe E, Laird M, Brathwaite J. Mobility as a mediator of the effects of child maltreatment on academic performance. Child Development. 1995;, 66(4):1130–1142. [PubMed] [Google Scholar]
- Fanshel D, Shinn EB. Children in foster care. Columbia University Press; New York: 1978. [Google Scholar]
- Gauthier Y, Fortin G, Jeliu G. Clinical application of attachment theory in permanency planning for children in foster care: The importance of continuity of care. Infant Mental Health Journal. Special Issue: The Added Value of Attachment Theory and Research for Clinical Work. 2004;25(4):379–396. [Google Scholar]
- James S. Why do foster care placements disrupt? An investigation of reasons for placement change in foster care. Social Service Review. 2004;78(4):601–627. [Google Scholar]
- James S, Landsverk J, Slymen DJ, Leslie LK. Predictors of outpatient mental health service use-The role of foster care placement change. Mental Health Services Research. 2004;6(3):127–141. doi: 10.1023/b:mhsr.0000036487.39001.51. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leathers SJ. Placement disruption and negative placement outcomes among adolescents in long-term foster care: The role of behavior problems. Child Abuse & Neglect. 2006;, 30(3):307–324. doi: 10.1016/j.chiabu.2005.09.003. [DOI] [PubMed] [Google Scholar]
- Lewis EE, Dozier M, Ackerman J, Sepulveda-Kozakowski S. The effect of placement instability on adopted children’s inhibitory control abilities and oppositional behavior. Developmental Psychology. 2007;Vol., 43(6):1415–1427. doi: 10.1037/0012-1649.43.6.1415. [DOI] [PubMed] [Google Scholar]
- McMillen JC, Zima BT, Scott LD, Jr., Auslander WF, Munson MR, Ollie MT, et al. Prevalence of psychiatric disorders among older youths in the foster care system. Journal of the American Academy of Child & Adolescent Psychiatry. 2005;44(1):88–95. doi: 10.1097/01.chi.0000145806.24274.d2. [DOI] [PubMed] [Google Scholar]
- Newton RR, Litrownik AJ, Landsverk JA. Children and youth in foster care: Disentangling the relationship between problem behaviors and number of placements. Child Abuse and Neglect. 2000;, 24(10):1363–1374. doi: 10.1016/s0145-2134(00)00189-7. [DOI] [PubMed] [Google Scholar]
- NSCAW Research Group Methodological lessons from the National Survey of Child and Adolescent Well-Being: The first three years of the USA’s first national probability sample of children and families investigated for abuse and neglect. Children and Youth Services Review. 2002;24:513–543. [Google Scholar]
- Olsen L. Services for minority children in out-of-home care. Social Service Review. 1982;, 56(4):572–585. [Google Scholar]
- Palmer SE. Placement stability and inclusive practice in foster care: An empirical study. Children and Youth Services Review. 1996;18(7):589–601. [Google Scholar]
- Pardeck JT. An empirical analysis of behavioral and emotional problems of foster children as related to re-placement in care. Child Abuse & Neglect. 1983;7(1):75–78. doi: 10.1016/0145-2134(83)90033-9. [DOI] [PubMed] [Google Scholar]
- Pardeck JT. Multiple placement of children in foster family care: An empirical analysis. Social Work. 1984a;29(6):506–509. [Google Scholar]
- Pardeck JT. An exploration of factors associated with the stability and continuity of the foster care system in the United States. International Social Work. 1984b;27(1):5–9. [Google Scholar]
- Pears K, Fisher PA. Developmental, cognitive, and neuropsychological functioning in preschool-aged foster children: Associations with prior maltreatment and placement history. Journal of Developmental & Behavioral Pediatrics. 2005a;26(2):112–122. doi: 10.1097/00004703-200504000-00006. [DOI] [PubMed] [Google Scholar]
- Pears KC, Fisher PA. Emotion understanding and theory of mind among maltreated children in foster care: Evidence of deficits. Development and Psychopathology. 2005b;17(1):47–65. doi: 10.1017/s0954579405050030. [DOI] [PubMed] [Google Scholar]
- Personal Responsibility and Work Opportunity Reconciliation Act 1996 http://www.access.gpo.gov/congress/wm015.txt.
- Raghavan R, Inkelas M, Franke T, Halfon N. Administrative barriers to the adoption of high-quality mental health services for children in foster care: A national study. Administration and Policy in Mental Health and Mental Health Services Research. 2007;34(3):191–201. doi: 10.1007/s10488-006-0095-6. [DOI] [PubMed] [Google Scholar]
- Rubin DM, O’Reilly ALR, Luan X, Localio AR. The Impact of placement stability on behavioral well-being for children in foster care. Journal of the American Academy of Child & Adolescent Psychiatry. 2007;46(5):610. doi: 10.1542/peds.2006-1995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ryan JP, Testa MF. Child maltreatment and juvenile delinquency: Investigating the role of placement and placement instability. Children and Youth Services Review. 2005;27(3):227–249. [Google Scholar]
- Stone NM, Stone SF. The prediction of successful foster placement. Social Casework. 1983;64(1):11–17. [Google Scholar]
- Taussig H, Clyman R, Landsverk J. Children who return home from foster care: A 6-year perspective study of behavioral health outcomes in adolescence. Pediatrics. 2001;108(1):1–7. doi: 10.1542/peds.108.1.e10. [DOI] [PubMed] [Google Scholar]
- Thornberry TP, Smith CA, Rivera C, Huizinga D, Stouthamer-Loeber M. Family Disruption and Delinquency. Juvenile Justice Bulletin. Report: NCJ, 178285. 1999 [Google Scholar]
- U.S. Department of Health and Human Services . U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services, National Institutes of Health, National Institute of Mental Health; Rockville, MD: 2007. [Google Scholar]
- U.S. Department of Health and Human Services . U.S. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Center for Mental Health Services, National Institutes of Health, National Institute of Mental Health; Rockville, MD: (n.d.) [Google Scholar]
- Unrau YA, Seita JR, Putney KS. Former foster youth remember multiple placement moves: A journey of loss and hope. Children and Youth Services Review. 2008;30(11):1256–1266. [Google Scholar]
- Usher CL, Randolph KA, Gogan HC. Placement patterns in foster care. Social Service Review. 1999;74:22–36. [Google Scholar]
- Ward H, Holmes L. Calculating the costs of local authority care for children with contrasting needs. Child & Family Social Work. 2008;13(1):80–90. [Google Scholar]
- Webster D, Barth RP, Needell B. Placement stability for children in out-of-home care: A longitudinal analysis. Child Welfare. 2000;79(5):614–632. [PubMed] [Google Scholar]
- Zima BT, Bussing R, Freeman S, Yang X, Belin TR, Forness SR. Behavior problems, academic skill delays and school failure among school-aged children in foster care: Their relationship to placement characteristics. Journal of Child and Family Studies. 2000;, 9(1):87–103. [Google Scholar]