

A 30-year-old male was admitted to our hospital for a 3-month history of cough. The computed tomography (CT) scan of chest revealed multiple lesions with sporadic calcification (popcorn calcification) in the upper and middle lobes of the right lung (Fig. 1). A presumptive diagnosis of chondroid hamartoma was made according to the CT-guided percutaneous biopsy. Systemic positron emission tomography-CT (PET-CT) scan was also negative for other lesions. A posterolateral thoracotomy was performed and innumerous firm round yellowish-white nodules were found and spread over the right upper and middle lobes (Fig. 2, arrow). The two lobes involved were successfully excised. The final specimen was 25 cm × 15 cm × 10 cm in size, firm, and full of nodules (Fig. 3). Postoperative pathological examination confirmed the diagnosis of pulmonary chondroid hamartomas (Fig. 4). The patient was discharged 7 days after the surgery without any main complication, and there is no sign of recurrence 3 months later.
FIGURE 1.

Computed tomography scan of chest showed multiple lesions of the right upper lobe, whereas the lower lobe seemed to be tumor free. Popcorn calcification, a typical imaging manifestation of pulmonary chondroid harmatoma, could be observed.
FIGURE 2.

The two lobes involved (arrow) seemed to out of physical function because they had fused and presented abnormal color.
FIGURE 3.

More yellow-white granules were found after the dissecting of the specimen.
FIGURE 4.
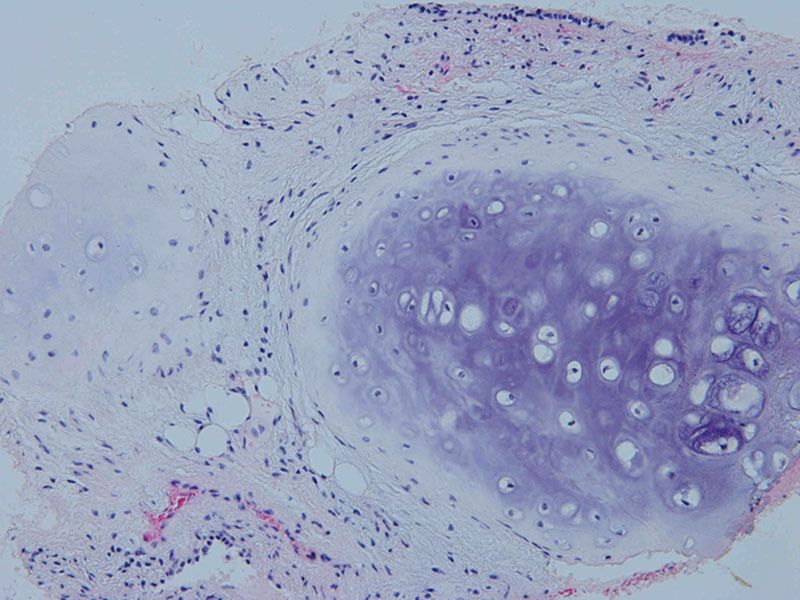
The tumor was mainly composed of chondroid tissue which was surrounded by epithelium, adipose tissue, and smooth muscle tissue could also be observed (hematoxylin and eosin stain, 200X).
Pulmonary chondroid hamartoma, as a subtype of pulmonary harmatoma, is defined when chondroid tissue predominates in the composition of the tumor. Harmatoma is the most common benign tumor of the lung, which accounts for 8% of pulmonary neoplasms. It is well known that harmatomas are composed of tissue elements normally found at that site, but which are growing in a disorganized mass, usually seem as single, round nodules with distinct boundaries.1 A cytogenetic analysis of the pulmonary hamartomas showed an abnormal karyotype and revealed recombinations between chromosomal bands 6p21 and 14q24,2 which supported that a hamartoma of the lung was a true neoplasm. Solitary pulmonary hamartoma is a common benign tumor that is usually seen in males, whereas multiple pulmonary hamartomas are rare and predominate in females.3,4 Only a few reports of multiple pulmonary chondroid hamartomas were described so far. Here we presented an extremely rare case of multiple pulmonary chondroid hamartomas with innumerous nodules in the right upper and middle lobes. Most patients with pulmonary hamartoma are asymptomic, whereas some patients may have respiratory symptoms such as hemoptysis, cough, phlegm, or chest pain.5 Generally speaking, a non-anatomical resection is curative for a benign lesion although the location of the lesion plays an important role in the decision of surgical type.1 Video-assisted thoracic surgery now seems to be a trend in dealing with benign tumors because of less morbidity of surgical complications and hospital stay compared with traditional thoracotomy. On the other hand, endobronchial hamartomas can be well managed by endoscopy and laser ablation.6
Footnotes
Disclosure: The authors declare no conflict of interest.
REFERENCES
- 1.Bini A, Grazia M, Petrella F, Chittolini M. Multiple chondromatous hamartomas of the lung. Interact Cardiovasc Thorac Surg. 2002;1:78–80. doi: 10.1016/s1569-9293(02)00058-0. [DOI] [PubMed] [Google Scholar]
- 2.Johansson M, Dietrich C, Mandahl N, et al. Recombinations of chromosomal bands 6p21 and 14q24 characterise pulmonary hamartomas. Br J Cancer. 1993;67:1236–1241. doi: 10.1038/bjc.1993.231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Nili M, Vidne BA, Avidor I, Paz R, Levy MJ. Multiple pulmonary hamartomas; a case report and review of the literature. Scand J Thorac Cardiovasc Surg. 1979;13:157–160. doi: 10.3109/14017437909100984. [DOI] [PubMed] [Google Scholar]
- 4.van den Bosch JM, Wagenaar SS, Corrin B, Elbers JR, Knaepen PJ, Westermann CJ. Mesenchymoma of the lung (so called hamartoma): a review of 154 parenchymal and endobronchial cases. Thorax. 1987;42:790–793. doi: 10.1136/thx.42.10.790. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Lien YC, Hsu HS, Li WY, et al. Pulmonary hamartoma. J Chin Med Assoc. 2004;67:21–26. [PubMed] [Google Scholar]
- 6.Cosío BG, Villena V, Echave-Sustaeta J, et al. Endobronchial hamartoma. Chest. 2002;122:202–205. doi: 10.1378/chest.122.1.202. [DOI] [PubMed] [Google Scholar]