

Abstract
Double cecal appendix is a rare anatomical variation. Approximately 100 cases have been reported worldwide. It is usually diagnosed incidentally during emergency appendectomies due to inflammatory processes in the cecal appendix. Case presentation: male, white, 36 years old, obese, presenting with pain in the lower abdomen for 24 h followed by nausea, vomiting and mild fever. He was subjected to additional tests, with the leukogram showing leukocytosis and abdominal ultrasonography depicting cecal appendix with thickened wall, locally associated with small quantities of liquid and intestinal loop obstruction. He underwent laparotomy, revealing acute appendicitis. Another intestinal loop obstruction was identified next to the ileum, leading to recognizing another cecal appendix after local dissection. Double appendectomy and segmental iliectomy were performed although not needed. Results of the anatomopathological examination of the surgical samples showed acute inflammation in the two cecal appendices. So, performing a routine retroperitoneal release and a complete cecum evaluation during such surgical procedures is recommended and suggested due to the possibility of not identifying a second cecal appendix.
Keywords: Appendix, Anatomic variation, Appendicitis, Appendectomy, General surgery
Core tip: Double cecal appendix is a rare (about 100 cases reported worldwide) anatomical variation often incidentally diagnosed in the face of inflammation in the organ. The current paper presents the first case reported in South America. The case is extremely important for the study of this possible anatomical variation since the lack of a diagnosis in a second cecal appendix can cause further complications for the patient and the physician. Moreover, it is associated with the presence of other anatomical variations, such as intestinal, genitourinary and bone. Such variations will be investigated in cases of the aforementioned diagnosis.
INTRODUCTION
Double cecal appendix is a rare anatomical variation, found in 0.004%[1] to 0.009%[2] of performed appendectomies. Approximately 100 cases of double cecal appendix[3-5] have been described worldwide so far, with no case reports in South America[2,3,6-37].
CASE REPORT
A male, white, 36 years old, slightly obese [body mass index (BMI) = 31.1 kg/m2], presented with abdominal pain in the lower abdomen for 24 h, followed by nausea, vomiting and mild fever (axillary temperature = 37.9 °C). He was subjected to blood tests that only showed leukocytosis without left shift. In addition, abdominal ultrasonography depicted cecal appendix with thickened wall, locally associated with small quantities of intra-abdominal fluid and local obstruction of intestinal loops.
He underwent laparotomy with a McBurney’s incision. The presence of an inflamed cecal appendix in its usual position after lysis of adhesions and cecum release was identified. Another intestinal loop obstruction was identified near the ileum. After the release of dense adhesions, it was possible to recognize the presence of a second cecal appendix, also with an inflammatory aspect (Figure 1), with its origin along the taenia coli.
Figure 1.

A photograph taken during a laparotomy procedure depicting an inflamed double cecal appendix. Minor (black arrow) and major (green arrow) inflamed cecal appendix. Surgeon’s hand is on the left side of the picture, holding the proximal segment of the ileum (arrow with white edges).
A double appendectomy and segmental iliectomy in the part of the devascularized intestinal loop, resulting from ileum dissection, was performed in order to provide the release and excision of the second cecal appendix. Both appendices showed no sign of perforation despite the inflammatory aspect, i.e., the occurrence of increased dimensions, thickened and erythematous wall, associated with fibrin and local tissue fragility.
The anatomopathological examination of the surgical samples corroborated the diagnosis of inflammation in both cecal appendices and resected segment of small intestine (ileum), with subserosal congestion and acute fibrinous serositis with eosinophils.
The patient had no postoperative complications and was discharged on the third day after surgery.
DISCUSSION
Since 1892 after the first case of double cecal appendix[27] was reported, less than 100 cases have been reported worldwide[3]. It demonstrates the rarity of such variations and why the current reported case is the first one to be described in South America[2,3,6-37].
Over time, some authors have presented classifications to categorize anatomical variations of cecal appendix. The first classification was developed in 1936 by Cave[28]. His classification was modified in 1962 by Wallbridge[29]. Since then, a number of authors have made some changes to it, leading to the modified classification by Cave-Walbridge, which is now the most widely used[17,30].
The classification modified by Cave-Wallbridge categorizes double cecal appendix into three types: A, B and C. Type A is characterized by the presence of two cecal appendices with a common origin in a single cecum. In type B, two appendices emerge from different cecal origins from a single cecum. This type is also subdivided into B1 and B2. In subtype B1, the two appendices emerge from a single cecum, one from each side of the ileocecal valve, symmetrically. On the other hand, in subtype B2, one of the appendices is in its usual position and the second one is located alongside the taenia coli. Finally, type C is characterized by the existence of two caeca, each with a cecal appendix (Figure 2).
Figure 2.
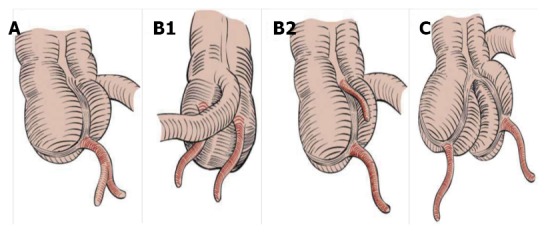
Classification modified by Cave-Wallbridge[30], including type A, subtype B1, subtype B2 and type C.
The present reported case describes the occurrence of a patient with double cecal appendix type B. There are reports of other rarer forms presenting with anatomic variations of the cecal appendix, such as the horseshoe appendix[31] and the triple appendix[32].
The existence of an cecal appendix duplication is asymptomatic and its diagnosis only comes during investigations on inflammation processes[3,17,33,34]. This is what happened in our patient’s case. According to clinical data, he had no complaints related to his cecal appendix duplication until the occurrence of acute appendicitis.
Despite the rarity of anatomical variations in the cecal appendix, the awareness of them is of great importance to surgeons. An inadequate surgical evaluation of the cecum due to unawareness of such variations can leave a second or third cecal appendix[17,30] unidentified. This may lead to further reoperations, diagnostic difficulties and medicolegal problems regarding malpractice because of the possibility of new inflammation in the remaining appendices[17,30].
For instance, this happened in a child whose cecal appendix duplication was not identified in the first appendectomy. Five months later, another laparotomy was needed in order to remove a second appendix which had also become inflamed[35]. Such a situation is most commonly found in patients with double cecal appendix type B[30]. It is worth mentioning that there is an increase in the postoperative morbidity and mortality[17,30] in patients in whom anatomical variations of the cecal appendix are not identified.
Finally, the importance of being aware of the association between double or triple cecal appendix and other anatomical variations, intestinal, genitourinary and osseous, should be highlighted[36,37]. These are most often associated with duplications of the cecal appendix types B1 and C[3]. Thus, when two or three cecal appendices are identified, investigating these other anatomical variations is recommended[3].
As a final conclusion, although double or triple cecal appendices are rare, surgeons must be aware of them and identify cecal appendix anatomical variations. Such a procedure is recommended when doctors surgically approach a patient with acute appendicitis. They should perform a complete cecum evaluation after the retroperitoneal release in order to avoid further complications. Surgeons should remember that in the face of such changes, they will need to investigate the presence of intestinal, genitourinary or bone anatomic variations.
ACKNOWLEDGEMENTS
We thank the patient for allowing the disclosure of his medical report and intraoperative photographic records.
COMMENTS
Case characteristics
Male, white, 36 years old, slightly obese, presenting with acute appendicitis.
Clinical diagnosis
Abdominal pain in the lower abdomen for 24 h, followed by nausea, vomiting and mild fever (axillary temperature = 37.9 °C).
Differential diagnosis
Causes of acute inflammatory abdomen.
Laboratory diagnosis
Leukocytosis without left shift.
Imaging diagnosis
Abdominal ultrasonography depicting cecal appendix with thickened wall, locally associated with small quantities of intra-abdominal fluid and intestinal loop local obstruction.
Pathological diagnosis
Inflammation in both cecal appendices.
Treatment
Laparotomy with a McBurney’s incision, followed by the performance of a double appendectomy and segmental iliectomy.
Related reports
Double cecal appendix is a rare (about 100 cases reported worldwide) anatomic variation most often incidentally diagnosed in face of inflammation of that organ.
Term explanation
The classification modified by Cave-Wallbridge categorizes double cecal appendix.
Experiences and lessons
The surgeon must be aware and identify cecal appendix anatomical variations. The procedure is recommended when surgeons surgically approach a patient with acute appendicitis. It is worth performing a complete cecum evaluation after the retroperitoneal release.
Peer review
This case report is well designed and presents a wide range of information about the subject, spreading the right messages and broadly contributing to the literature.
Footnotes
P- Reviewer: Haveman JW, Ince V, Karateke F, Tsuda M S- Editor: Ding Y L- Editor: Roemmele A E- Editor: Lu YJ
References
- 1.Collins DC. A study of 50,000 specimens of the human vermiform appendix. Surg Gynecol Obstet. 1955;101:437–445. [PubMed] [Google Scholar]
- 2.Kjossev KT, Losanoff JE. Duplicated vermiform appendix. Br J Surg. 1996;83:1259. [PubMed] [Google Scholar]
- 3.Griffiths EA, Jagadeesan J, Fasih T, Mercer-Jones M. Bifid vermiform appendix: a case report. Curr Surg. 2006;63:176–178. doi: 10.1016/j.cursur.2006.02.001. [DOI] [PubMed] [Google Scholar]
- 4.Sobhian B, Mostegel M, Kunc C, Karner J. [Appendix vermiformis duplex--a rare surprise] Wien Klin Wochenschr. 2005;117:492–494. doi: 10.1007/s00508-005-0390-3. [DOI] [PubMed] [Google Scholar]
- 5.Oğuzkurt P, Oğuzkurt L, Kayaselcuk F, Oz S. An unusual cause of acute abdomen: torsion of colonic duplication over a duplicated appendix. Pediatr Surg Int. 2004;20:722–723. doi: 10.1007/s00383-004-1283-7. [DOI] [PubMed] [Google Scholar]
- 6.McNeill SA, Rance CH, Stewart RJ. Fecolith impaction in a duplex vermiform appendix: an unusual presentation of colonic duplication. J Pediatr Surg. 1996;31:1435–1437. doi: 10.1016/s0022-3468(96)90849-0. [DOI] [PubMed] [Google Scholar]
- 7.Eroglu E, Erdogan E, Gundogdu G, Dervisoglu S, Yeker D. Duplication of appendix vermiformis: a case in a child. Tech Coloproctol. 2002;6:55–57. doi: 10.1007/s101510200010. [DOI] [PubMed] [Google Scholar]
- 8.Mahmood A, Mahmood NF, Williams JL. Acute abdominal pain presenting as a rare appendiceal duplication: a case report. J Med Case Rep. 2012;6:79. doi: 10.1186/1752-1947-6-79. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Barreto FT, Alonso JRC, Blanco DP, Reyes DS, Casanova AD. Appendicular duplication. Rev Cubana Cir. 2011;50:348–352. [Google Scholar]
- 10.De Lagausie P, Billing A, Eymeri JC, Tavakoli D. [Hypotrophic and duplicated appendix. A case in a child] Chir Pediatr. 1989;30:216–217. [PubMed] [Google Scholar]
- 11.Kim EP, McClenathan JH. Unusual duplication of appendix and cecum: extension of the Cave-Wallbridge classification. J Pediatr Surg. 2001;36:E18. doi: 10.1053/jpsu.2001.26400. [DOI] [PubMed] [Google Scholar]
- 12.López-Deogracias M, Naranjo-Gozalo S, Sánchez-Moreno L, Gómez-Fleitas M. [Duplicated appendix in the presence of an adenocarcinoma] Cir Esp. 2008;83:333. doi: 10.1016/s0009-739x(08)70591-8. [DOI] [PubMed] [Google Scholar]
- 13.Theodoropoulos GE, Tsamis D, Linardoutsos D, Stamopoulos P, Zoumpouli C, Zagouri F, Michalopoulos NV. Ruptured cystadenoma of a duplicated appendix. Am Surg. 2010;76:341–343. [PubMed] [Google Scholar]
- 14.Freeman HJ. Duplicated appendix complicated by appendiceal cancer. World J Gastroenterol. 2011;17:135–136. doi: 10.3748/wjg.v17.i1.135. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Christodoulidis G, Symeonidis D, Spyridakis M, Koukoulis G, Manolakis A, Triantafylidis G, Tepetes K. Acute appendicitis in a duplicated appendix. Int J Surg Case Rep. 2012;3:559–562. doi: 10.1016/j.ijscr.2012.08.004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Oruç C, Işık O, Ureyen O, Kahyaoğlu OS, Köseoğlu A. An extremely rare appendiceal anomaly: horseshoe appendicitis. Ulus Travma Acil Cerrahi Derg. 2013;19:385–386. doi: 10.5505/tjtes.2013.67424. [DOI] [PubMed] [Google Scholar]
- 17.Tutcu Şahin S, Erhan Y, Aydede H. Double acute appendicitis in appendical duplication. Ulus Travma Acil Cerrahi Derg. 2013;19:83–85. doi: 10.5505/tjtes.2013.80557. [DOI] [PubMed] [Google Scholar]
- 18.Marshall AP, Issar NM, Blakely ML. Appendiceal duplication in children presenting as an appendiceal tumor and as recurrent intussusception. J Pediatr Surg. 2013;48:e9–e12. doi: 10.1016/j.jpedsurg.2013.01.036. [DOI] [PubMed] [Google Scholar]
- 19.Canbay E, Akman E. Appendix perforation in appendix duplication in a man: a case report. J Med Case Rep. 2011;5:162. doi: 10.1186/1752-1947-5-162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sani R, Harouna Y, Hama Y, Nouhou H, Faucheron JL. First case of double appendicitis complicating duplication of a vermiform appendix in an adult patient. Colorectal Dis. 2010;12:1162–1163. doi: 10.1111/j.1463-1318.2010.02200.x. [DOI] [PubMed] [Google Scholar]
- 21.Geurts BA, van Rijn AB, Koelma IA. [Acute appendicitis in a boy with an earlier appendectomy and a second appendix] Ned Tijdschr Geneeskd. 2006;150:2876–2879. [PubMed] [Google Scholar]
- 22.Yanar H, Ertekin C, Unal ES, Taviloglu K, Guloglu R, Mete O. The case of acute appendicitis and appendiceal duplication. Acta Chir Belg. 2004;104:736–738. doi: 10.1080/00015458.2004.11679655. [DOI] [PubMed] [Google Scholar]
- 23.Hennekinne S, Pessaux P, Regenet N, Fauvet R, Tuech JJ, Arnaud JP. [Double appendicitis: a rare clinical form in appendix duplication] Presse Med. 2001;30:23–24. [PubMed] [Google Scholar]
- 24.Mazziotti MV, Marley EF, Winthrop AL, Fitzgerald PG, Walton M, Langer JC. Histopathologic analysis of interval appendectomy specimens: support for the role of interval appendectomy. J Pediatr Surg. 1997;32:806–809. doi: 10.1016/s0022-3468(97)90624-2. [DOI] [PubMed] [Google Scholar]
- 25.Konstantinov PI, Titarenko IaA. [Duplication of the appendix in a child] Vestn Khir Im I I Grek. 1997;156:109. [PubMed] [Google Scholar]
- 26.Lin BC, Chen RJ, Fang JF, Lo TH, Kuo TT. Duplication of the vermiform appendix. Eur J Surg. 1996;162:589–591. [PubMed] [Google Scholar]
- 27.Khanna AK. Appendix vermiformis duplex. Postgrad Med J. 1983;59:69–70. doi: 10.1136/pgmj.59.687.69. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Cave AJ. Appendix Vermiformis Duplex. J Anat. 1936;70:283–292. [PMC free article] [PubMed] [Google Scholar]
- 29.Wallbridge PH. Double appendix. Br J Surg. 1962;50:346–347. doi: 10.1002/bjs.18005022124. [DOI] [PubMed] [Google Scholar]
- 30.Travis JR, Weppner JL, Paugh JC. Duplex vermiform appendix: case report of a ruptured second appendix. J Pediatr Surg. 2008;43:1726–1728. doi: 10.1016/j.jpedsurg.2008.04.023. [DOI] [PubMed] [Google Scholar]
- 31.Mesko TW, Lugo R, Breitholtz T. Horseshoe anomaly of the appendix: a previously undescribed entity. Surgery. 1989;106:563–566. [PubMed] [Google Scholar]
- 32.Tinckler LF. Triple appendix vermiformis--a unique case. Br J Surg. 1968;55:79–81. doi: 10.1002/bjs.1800550122. [DOI] [PubMed] [Google Scholar]
- 33.Kabay S, Yucel M, Yaylak F, Hacioglu A, Algin MC, Olgun EG, Sahin L, Aydin T. Combined duplication of the colon and vermiform appendix in an adult patient. World J Gastroenterol. 2008;14:641–643. doi: 10.3748/wjg.14.641. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Akhtar J, Ejaz T, Guiney EJ. Appendix vermiformis duplex - a lesson for the unwary. Pediatr Surg Int. 1994;9:429–30. [Google Scholar]
- 35.Maizels G. Duplication of the vermiform appendix. S Afr Med J. 1966;40:1123–1125. [PubMed] [Google Scholar]
- 36.Gilchrist BF, Scriven R, Nguyen M, Nguyen V, Klotz D, Ramenofsky ML. Duplication of the vermiform appendix in gastroschisis. J Am Coll Surg. 1999;189:426. doi: 10.1016/s1072-7515(99)00174-x. [DOI] [PubMed] [Google Scholar]
- 37.Scarff JE, Harrold MW, Wylie JH. Duplication of the vermiform appendix: new variant of a rare anomaly. South Med J. 1982;75:860–862. doi: 10.1097/00007611-198207000-00024. [DOI] [PubMed] [Google Scholar]