

Abstract
Adult patients with developmental dysplasia of the hip develop secondary osteoarthritis and eventually end up with total hip arthroplasty (THA) at younger age. Because of altered anatomy of dysplastic hips, THA in these patients represents technically demanding procedure. Distorted anatomy of the acetabulum and proximal femur together with conjoined leg length discrepancy present major challenges during performing THA in patients with developmental dysplasia of the hip. In addition, most patients are at younger age, therefore, soft tissue balance is of great importance (especially the need to preserve the continuity of abductors) to maximise postoperative functional result. In this paper we present a variety of surgical techniques available for THA in dysplastic hips, their advantages and disadvantages. For acetabular reconstruction following techniques are described: Standard metal augments (prefabricated), Custom made acetabular augments (3D printing), Roof reconstruction with vascularized fibula, Roof reconstruction with pedicled iliac graft, Roof reconstruction with autologous bone graft, Roof reconstruction with homologous bone graft, Roof reconstruction with auto/homologous spongious bone, Reinforcement ring with the hook in combination with autologous graft augmentation, Cranial positioning of the acetabulum, Medial protrusion technique (cotyloplasty) with chisel, Medial protrusion technique (cotyloplasty) with reaming, Cotyloplasty without spongioplasty. For femoral reconstruction following techniques were described: Distraction with external fixator, Femoral shortening through a modified lateral approach, Transtrochanteric osteotomies, Paavilainen osteotomy, Lesser trochanter osteotomy, Double-chevron osteotomy, Subtrochanteric osteotomies, Diaphyseal osteotomies, Distal femoral osteotomies. At the end we present author’s treatment method of choice: for acetabulum we perform cotyloplasty leaving only paper-thin medial wall, which we break during acetabular cup impacting. For femoral side first we peel of all rotators and posterior part of gluteus medius and vastus lateralis from greater trochanter on the very thin flake of bone. This method allows us to adequately shorten proximal femoral stump, with possibility of additional resection of proximal femur. Furthermore, several advantages and disadvantages of this procedure are also discussed.
Keywords: Hip, Arthroplasty, Dysplasia, Reconstruction, Techniques, Acetabulum, Femur, Osteoarthritis, Developmental dysplasia of the hip
Core tip: Total hip arthroplasty (THA) in adult patients with developmental dysplasia of the hip is technically demanding procedure. In this paper we present a variety of surgical techniques available for THA in dysplastic hips, their advantages and drawbacks, ending with the author’s treatment method of choice.
INTRODUCTION
Developmental dysplasia of the hip (DDH) is common cause of secondary hip osteoarthritis[1]. The prevalence of DDH varies among different ethnic groups; from 5.4 to 12.8% in the Danish population, 1.8% in Koreans, 2.4% in Turkish people and 7.3% in Singaporeans[2]. The aetiology of DDH is multifactorial, involving both genetic and intrauterine environmental factors. The group of patients at risk includes those with one or combination of the following risk factors: female gender, first born, positive family history or ethnic background, breech delivery, oligohydramnios, torticollis, and lower-limb deformity[3]. Despite new-born screening programs[4], some cases are missed, or incorrectly treated. These patients develop secondary osteoarthritis and eventually end up with total hip arthroplasty (THA) at younger age. Due to changed anatomy of dysplastic hips, THA in these patients is technically very demanding procedure[5-7]. Functional results after THA in dysplastic hips are often not excellent[8,9]. At the beginnings of modern arthroplasty it was considered that THA in these patients is not possible[10]. Better surgical techniques were developed over time to achieve a painless, stable and long-lasting hip endoprosthesis customized to increased functional needs of these young patients. In this paper we present a variety of surgical techniques available for THA in dysplastic hips, their advantages and drawbacks, ending with the author’s treatment method of choice[7].
ANATOMY AND BIOMECHANICS OF DYSPLASTIC HIP
Anatomy of dysplastic hip is usually significantly altered. Acetabulum and femur are underdeveloped and femur is often displaced. Hip biomechanics is altered and there is no ideal stimulation for development of proper acetabulum and proper femoral head. Different morphological alterations are seen, not only on femur and acetabulum but also on pelvis[11-13]. In simplest degrees of dysplasia acetabulum is just a little bit shallower with lover acetabular angle but in the most complex cases of dysplasia acetabulum is underdeveloped, shallow and lacking bone stock medially. Since femoral head is situated more proximal (dislocated), a new acetabulum (neoacetabulum) is formed (Figure 1). Pelvic bone stock is rearranged and there is more bone thickness available more posteriorly in relation to the level of the true acetabulum[13]. Acetabular retroversion represents additional problem. Incidence of acetabular retroversion in dysplastic hips ranges from 1 in 6 according to Li et al[14] to 1 in 3 according to Mast et al[15]. Dysplastic femur has increased anteversion, shorter neck and narrower and straighter femoral canal[16,17]. Femoral head is elliptic which causes incongruity of the hip joint[17]. All of mentioned alterations in dysplastic hip anatomy are responsible for functionally “weaker” hip joint unable to withstand increased load. In short, dysplastic hips are incongruent, centre of rotation is displaced, hip abductors and flexors are shortened and weakened. If dysplasia is one-sided, pelvic disbalance is often present with limping and leg length discrepancy. All of these factors can increase forces in hip joint, which can cause quicker deterioration of cartilage and bone tissue with earlier onset of osteoarthritis of the hip joint[10,18].
Figure 1.
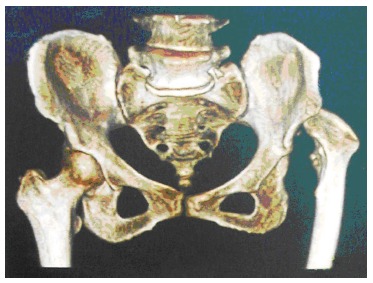
On the right side hip is normally developed and on the left side the acetabulum is underdeveloped, shallow and lacking bone stock medially and at the level of normal (ideal) acetabular roof. The femoral head is more proximal (dislocated) with increased anteversion, shorter neck and narrower and straighter femoral canal.
CLASSIFICATION OF DYSPLASTIC HIP
There are different classifications of dysplastic hips in adults. Those classifications are developed so that different treatments can be compared and so that the surgeon can plan and prepare operation and predict outcome based on the degree of dysplasia. Since in majority of the cases the diagnosis is formed based on the clinical exam and X-rays, most common classifications are based on X-rays of the pelvis and the hips. The most common is classification according to the Crowe[19] with 4 different degrees of dysplasia (Figure 2). There are more recent classification like Eftekhar[20] and Hartofilakidis et al[11,21] which take into account both femoral and acetabular side. Hartofilakidis et al[11] acknowledged importance at the acetabular side for operative treatment so in 1988 he based his classification on relations between femoral head and acetabulum and the difference between true and false (neo) acetabulum[11]. Then, in 2008, he additionally developed his classification by adding subtypes regarding to the shape of the acetabulum[12]. This classification is very useful for surgeon but requires additional education and is more complicated. Special imaging modalities, including computed tomography (CT) of the hip, may be useful in complex hip arthroplasty. CT provides 3-dimensional information about anterior and posterior column deficiencies, socket size, thickness of the anterior and posterior walls and medial bone stock (thickness) at the level of the ideal acetabular roof which help us in preoperative planning[22]. Although Crowe classification is based on two-dimensional analysis of the pelvic X-ray and on, basically, just a vertical displacement of the femoral head, it is still predominant classification due to simplicity and availability.
Figure 2.
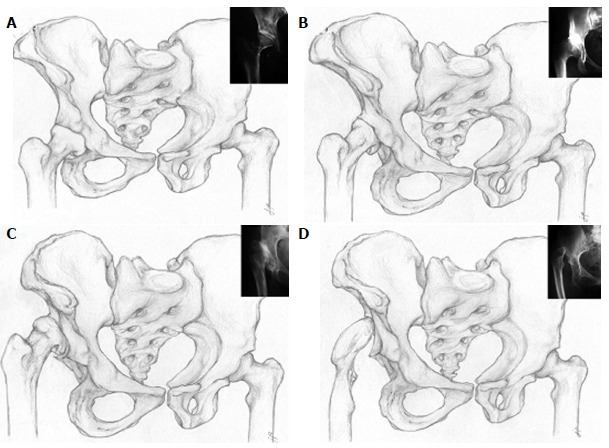
Left hip is normal, right hip is dysplastic. A: Crowe type 1-proximal head subluxation is less than 50% of vertical diameter of the femoral head (less than 10% of the pelvic height); B: Crowe type 2-proximal head subluxation is between 50% and 75% of vertical diameter of the femoral head (between 10% and 15% of the pelvic height); C: Crowe type 3-proximal head subluxation is between 75% and 100% of vertical diameter of the femoral head (between 15% and 20% of the pelvic height); D: Crowe type 4-proximal head dislocation with proximal movement of the femoral head for more than 100% of vertical diameter of the femoral head (head is moved proximally for more than 20% of the pelvic height).
OPERATIVE TECHNIQUES IN DYSPLASTIC HIP ARTHROPLASTY
Secondary osteoarthritis due to DDH occurs at a younger age because of abnormal anatomy (an average of 53 years according to Hartofilakidis et al[23]). The key point of surgical treatment is to ensure long-term stability of the endoprosthesis by restoration of anatomical and biomechanical relationships. This is not an easy task because total hip arthroplasty in DDH is technically demanding due to deficient acetabular bone stock, abnormal femoral anatomy with increased neck-shaft angle and valgus orientation, increased anteversion, muscle contracture and leg-length discrepancy[10,24]. Despite an initial discouraging statement that THR should be avoided in patients who have DDH, various techniques have been developed to approach this problem[10]. The surgeon has to address several issues. Distorted anatomy of the acetabulum and proximal femur is always a challenge. Then there is a leg length discrepancy. And finally, since majority of patients are at younger age, the soft tissue balance is of great importance (especially the need to preserve the continuity of abductors) to maximise postoperative functional result[7,25]. Technical options are numerous (Table 1).
Table 1.
Different operative treatment options for total hip arthroplasty in secondary hip osteoarthritis in developmental dysplasia of the hip
| Techniques for acetabular reconstruction | Techniques for femoral reconstruction |
| Standard metal augments (prefabricated) | Distraction with external fixator |
| Custom made acetabular augments (3D printing) | Femoral shortening through a modified lateral approach |
| Roof reconstruction with vascularized fibula | Transtrochanteric osteotomies |
| Roof reconstruction with pedicled iliac graft | Paavilainen osteotomy |
| Roof reconstruction with autologous bone graft | Lesser trochanter osteotomy |
| Roof reconstruction with homologous bone graft | Double-chevron osteotomy |
| Roof reconstruction with auto/homologous spongious bone | Subtrochanteric osteotomies |
| Reinforcement ring with the hook in combination with autologous graft augmentation | Diaphiseal osteotomies |
| Cranial positioning of the acetabulum | Distal femoral osteotomies |
| Medial protrusion technique (cotyloplasty) with chisel | |
| Medial protrusion technique (cotyloplasty) with reaming | |
| Cotyloplasty without spongioplasty |
Surgical alternatives to THA
There are also alternatives to THA in dysplastic hips such as pelvic osteotomies[14,26]. Pelvic osteotomies may provide excellent results for patients with early or no osteoarthritis and with moderate or no pain. The purpose of the pelvic osteotomy is to obtain an increased acetabular weight-bearing surface for the femoral head either by reshaping the acetabulum or by enlarging its margins. Different types of osteotomies are described in literature[14,26]. In the past, procedures such as the Chiari osteotomy or shelf augmentation of the acetabulum were used to treat adolescent and adult hip dysplasia but today realignment osteotomies would be used since they result with the reposition or acetabulum into a more favorable position over the femoral head and improve load distribution. Their main advantage is that the femoral head is covered with hyaline cartilage instead of fibrocartilage. Their disadvantage is the complexity of the operations. Some of them are used only when the triradiate cartilage is open like Pemberton and Dega osteotomies. Others are single innominate osteotomy of Salter, the triple innominate osteotomies of Steel, Carlioz, and Tönnis and the periacetabular osteotomy of Ganz. The major disadvantage is that when there is advanced osteoarthritis of the dysplastic hip only THA can completely relieve the pain and restore the function of the hip joint.
Acetabular reconstruction
The major concern with total hip arthroplasty in DDH is the containment and incorporation of the acetabular cup. Placement of the cup is technically difficult because normal anatomic landmarks are obscured. There is a need for fine balance in adjusting the cup size, inclination, cup anteversion and coverage. A compromise can be made by setting acetabular component away from the ideal centre of rotation, but in such a way to ensure a good stability of the endoprosthesis. High placement of the acetabular component has been proposed (Figure 3A). Russotti et al[27] reports good long-term results with “high hip centre” acetabulum placement. Kaneuji et al[28] shows no differences in polyethylene wear with rotation centre placed 20 mm proximal from the figure of tears. However, according to Bicanic et al[29] one has to take into account that for every millimetre of proximalisation, load on the hip increases for about 0.1%. At this level bone stock is usually insufficient and the lever arm for body weight remains much longer than that of the abductors, resulting in excessive loading of the hip joint. In addition, at this level, shearing forces acting on the acetabular component may lead to an early loosening, and in unilateral cases a proximally placed acetabular component contributes to limping and limb-length discrepancy[23,30,31]. Placement of the acetabular component in the anatomical position and augmentation of the superior segmental defect with structural autologous graft (autograft) or allograft has also been proposed (Figure 3B). Cementless acetabular cups with 30% to 40% of uncoverage may be acceptable[32-34], more than that should be covered. Some authors recommend spongioplasty of the acetabular roof for smaller uncovered areas (Figure 3C)[35]. For larger defects structural autograft or allograft can be used. Autografts can be free or vascularized. For vascularized autografts it is expected to better integrate with iliac bone (Figure 3D)[36]. Usually vascularised iliac graft is used, although Fujiwara reported good outcome of acetabular roof reconstruction with free vascularized fibular graft[37]. Long-term survival rates of such bone grafts proved to be different in various studies. While some authors report good long-term results of free auto- or allografts[24,38,39] and vascularized autografts[37,40-42], others warn about graft resorption and secondary instability of acetabular component in structural bone grafting[43-45]. Acetabular bone stock deficiency can be managed with specially constructed acetabular components or using special 3-dimensional porous materials which simulates bone structure and allow faster and better endoprosthesis–bone integration (Figure 3F)[46-48]. For that purpose trabecular metal is used in form of acetabular cup or trabecular metal augments. That is manly used in revision surgery, but can be useful in dysplastic hip THA[48,49]. Potential advantage of trabecular metal is to avoid the use of structural bone grafts, avoid the need for custom shaped implants and provide excellent bone ingrowth on small contact area. Major disadvantage is potential difficulty if the cup should be removed because of infection. Oblong-shaped cementless implant (oblong cup) can be used for acetabular reconstruction. Abeyta et al[50] presented satisfactory long-term results in using oblong cup for reconstruction of the acetabulum. The reinforcement ring with the hook in combination with autologous graft augmentation has been designed for cases with severe bone-stock deficiencies (Figure 3E)[51,52]. This technique enables reconstruction of the anatomic hip centre by positioning the hook around the inferior margin of the acetabular floor (incisura acetabuli). The hook does not act as a fixation device but helps prevent high or lateral placement of the ring and helps adequate coverage of the polyethylene liner, regardless of the degree of anatomical deformity. Pitto et al[53] presented how reinforcement ring with hook provides adequate stability in poor bone-stock settings and prevents bone graft resorption showing good mid-term results of this kind of treatment. According to fact that medialisation of acetabular cup decreases hip load and that satisfactory supero-lateral support of the component with host bone is a better option, a method named cotyloplasty was introduced. Later, in 2008 Bicanic et al[29] proved that every millimetre of lateral displacement of the acetabular cup (relative to the ideal centre of rotation) results with an increase of 0.7% in hip load, and for every millimetre of proximal displacement an increase of 0.1% in hip load should be expected (or decreased if displacement is medial or distal). That suggest acetabular placement as far medially as possible for optimal results. Cotyloplasty is a technique that involves making a perforation of the medial wall of a shallow acetabulum and then inserting an acetabular cup with the medial aspect of its dome beyond the Kohler’s line. In 1976, Dunn et al[54] presented a method that involved intentional medial wall fracture using osteotome with cup placement beyond the ilioischial line, avoiding bone grafting but still achieving cemented acetabular cup stability (Figure 3G). At the meeting of the Greek Orthopaedic Association in 1984, technique of cotyloplasty for the preparation of the acetabulum was reported by Hartofilakidis et al[11]. This method involved the use of a T-handle curette to enlarge the socket. When the acetabulum was large enough they fracture the paper-thin medial wall using a deepening reamer. Acetabulum was filled with a large amount of autogenous cancelous bone graft and cup is cemented in position without pressure. Hartofilakidis et al[11,12] modified this method by perforating the medial acetabular wall with a reamer instead of an osteotome and called the technique cotyloplasty (Figure 3H). Satisfactory reports were published later concerning the results of implanting cemented cups using cotyloplasty. Dorr et al[55] reported good results when implanting porous-coated acetabular components using this technique. Cotyloplasty has advantages over other techniques of fixing an acetabular component in a dysplastic acetabulum. This technique has advantages over superior cup placement because it usually restores the normal hip joint biomechanics, it restores the leg length discrepancy and it has less chance of impingement that may lead to dislocation. Major disadvantage of the cotyloplasty is that it is difficult to control the amount of the medial wall fracture and complication such as fracture-dislocation of the cup inside the pelvis can occur.
Figure 3.
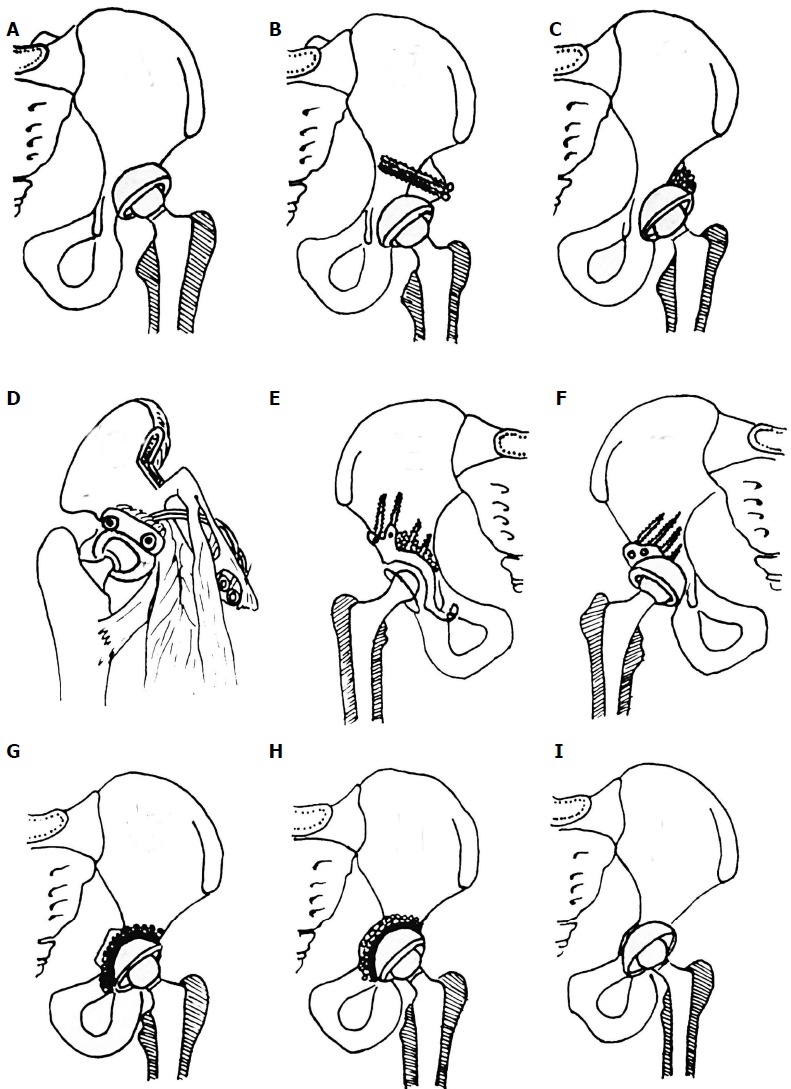
Different options for acetabular reconstruction. A: Higher placement of the acetabular cup; B: Placement of the acetabular component in the anatomical position and augmentation of the superior segmental defect with structural autograft or allograft fixed with screws; C: Placement of the acetabular component in the anatomical position and spongioplasty of the acetabular roof for smaller uncovered areas (30%-40%); D: Anatomical position of acetabular cup and augmentation of the superior segmental defect with vascularised iliac graft; E: Reinforcement ring with the hook in combination with autologous graft augmentation for cases with severe bone-stock deficiencies. Anatomic hip centre is reconstructed by positioning the hook around the inferior margin of the acetabular floor. The hook prevents high or lateral placement of the ring and helps adequate coverage of the polyethylene liner, regardless of the degree of anatomical deformity; F: Acetabular bone stock deficiency can be managed with specially constructed acetabular components or using special 3-dimensional porous materials which simulates bone structure and allow faster and better endoprosthesis-bone integration. For that purpose trabecular metal (tantalum) is used in form of acetabular cup or trabecular metal augments. Oblong-shaped cementless implants can be used for acetabular reconstruction; G: Cotyloplasty with chisel - intentional medial wall fracture using osteotome with cup placement beyond the ilioischial line with bone grafting; H: Cotyloplasty with reamer - first, perforation of the medial acetabular wall with a reamer is performed, then acetabulum is filled with a large amount of autogenous cancelous bone graft and cup is cemented in position without pressure; I: Cotyloplasty without spongioplasty - implantation of porous-coated cementless acetabular components without spongioplasty.
Preoperative skeletal traction
According to fact that long term stability of the prosthesis with better abductor function and leg-length equalization is best achieved by placing the endoprosthesis near the normal anatomic level, some authors suggests iliofemoral distraction to reduce high congenital dislocation of the hip before THA[56,57] (Figure 4A). Grill was the first to describe the application of distraction between the ilium and femur before open reduction for DDH in children[58]. Lai et al[56] used Wagner’s apparatus for distraction, and showed how laxity after distraction and close-to-normal position of the femur to the acetabulum made THA much easier than in those performed without distraction. Operative time, blood loss, and surgical complications were reduced, and the functional results were as good as those of ordinary THA. Holinka et al[57] modified surgical procedure according to Lai et al[56], with immediate femoral head resection and extensive soft tissue release prior to distraction and showed satisfying five-year results in unilateral and bilateral Crowe type IV high hip dislocations. Complications, such as pin tract infection, peroneal nerve palsy, cup protrusions are described for such procedures[57].
Figure 4.
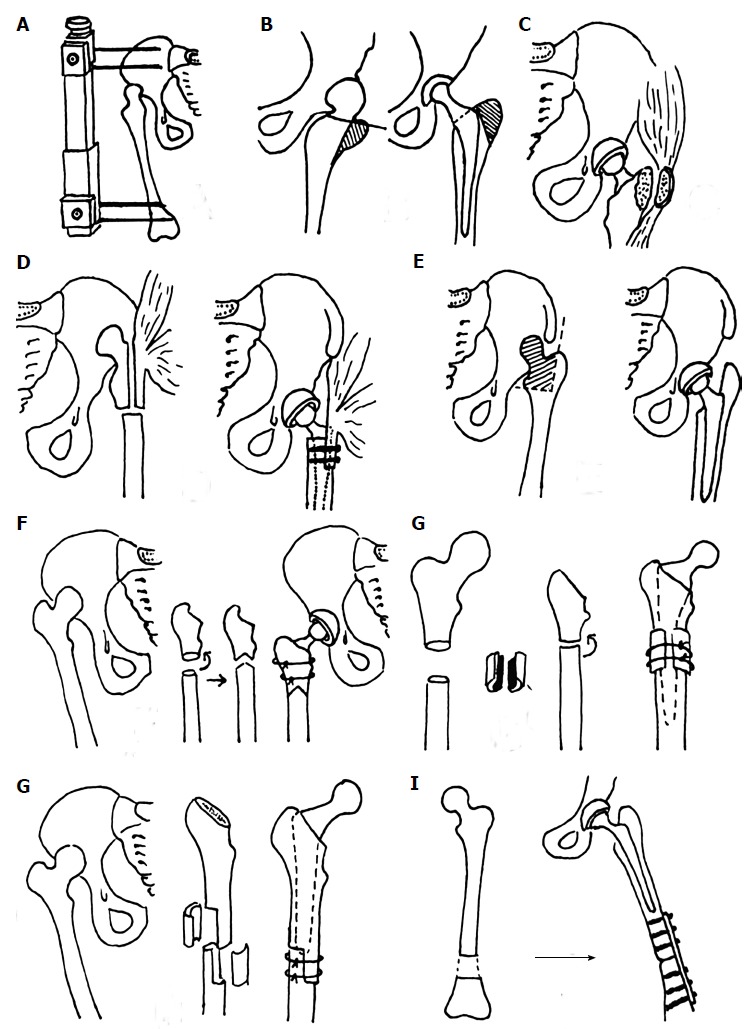
Different types of femoral reconstruction options. A: Wagner’s apparatus for preoperative skeletal traction to reduce high congenital dislocation of the hip before total hip arthroplasty; B: Trochanteric osteotomy in total hip arthroplasty; C: Delimar et al[7] modification of the direct lateral approach to the hip. Anterior half of the continuous tendon is detached either by cautery or with a chisel. If the chisel is used, a thin layer of bone from the greater trochanter remains attached to the continuous tendon of the gluteus medius and the vastus lateralis. The posterior half of the continuous tendon of the gluteus medius and the vastus lateralis is always detached with the chisel leaving a bone flake of at least 2 to 3 mm thickness attached to tendons. In that way, the abductor muscles are stripped from the greater trochanter and there is no trochanteric osteotomy during the approach, which allows preservation of the continuity of the abductor muscles; D: Paavilainen's procedure of metaphyseal shortening osteotomy combined with distal sliding of the greater trochanter with intact attachment of the abductor muscles; E: Progressive femoral shortening at the level of lesser trochanter; greater trochanter remains intact, thus providing better functional results; F: Combined procedure of femoral subtrochanteric shortening with derotational double-chevron osteotomy. Transverse osteotomy was first performed, followed by rotational alignment in order to correct anteversion. Later, double chevron osteotomy was performed. Such method allows intraoperative derotation and shortening adjustment; G: Subtrochanteric osteotomy - modified technique; osteotomy sites were covered with onlay grafts of the excised fragments and fixed with two cerclage wires; H: Diaphyseal step-cut shortening osteotomy performed after reaming and stabilized with two to three cerclage bands with or without bone grafting. After stabile fixation, intramedullary reaming is done until optimal cortical contact is achieved, especially distal to the osteotomy site; I: Distal femur shortening procedure. First, total hip arthroplasty with acetabulum in anatomic position is performed followed by the femoral shortening that is done distal to stem so that the first screw of the plate would be more than 2 cm from the stem. Later, plate fixation of the femoral osteotomy site was performed.
Femoral reconstruction
According to the Crowe classification, arthroplasty procedures performed on dysplastic hips that belong to Crowe I or II class allow positioning of femoral head in optimal hip rotation centre without performing any of the femoral shortening procedures. In contrast, arthroplasty procedures performed on Crowe III or IV dysplastic hips commonly require one of the femoral shortening procedures. However, here we have to emphasize that this is not a real “clear cut” division whether to perform femoral shortening or not since in Crowe I and II dysplastic hips the complex deformities and variations of the dysplastic femur may be present and thus require femoral shortening procedure.
After placement of the acetabular component in anatomic position femur often becomes too long and needs to be shortened. Thus, shortening femoral osteotomies are developed, which further allow both: (1) hip arthroplasty without sciatic nerve stretching; and (2) correction of the proximal femoral anteversion. After these procedures are performed, abductor mechanism of the hip is restored with equal final leg length[59]. Femoral procedures can be roughly divided according to the level of procedure: proximal femur, femoral shaft and distal femoral procedure.
One of the most commonly performed procedures on proximal femur during THR includes trochanteric osteotomies. Trochanteric osteotomies in total hip arthroplasty were first introduced by Charnley[60] in 1972. Over long period of time several modifications of the initial procedure were developed such as changes in shape of skin incision, different approach to the hip, instrumentation etc. These procedures are nowadays reserved mainly for complex primary hip arthroplasty procedures (including arthroplasty in DDH) or complex revision procedures of THR. Trochanteric osteotomies have several major advantages. First, they provide excellent visualization of both, femur and acetabulum, i.e., whole operating region. Second, by performing trochanteric osteotomy abductor mechanism of the hip is preserved and easily repositioned back to original position, altogether resulting in stable hip without risk for dislocation. An example of modified trans-trochanteric approach technique was presented by Kerboull et al[61] in 2007. These authors describe transtrochanteric approach as a method which allows easier hip dislocation with good visualization of the operating region and preserved hip abductory mechanism. This approach was also offered as one of the solutions in treatment of severe femoral deformities present in DDH. Namely, transtrochanteric approach allows performance of corrective osteotomies in the area of femoral metaphysis. Such procedure together with reposition of abductory muscles provide near-optimal anatomic relations in operated hip[61] (Figure 4B). Despite these evidences this approach is still controversial and under debate because of unclear conclusion about relatively high rate of around 6% of nonunion of greater trochanter after such procedures[61-64]. Paavilainen et al[32] reported procedure of femoral shortening on proximal femur during THR in DDH in 1990 - method included a cementless THR procedure where the acetabular cup is placed in anatomic position together with proximal femur shortening osteotomy with distal sliding of the greater trochanter (Figure 4D). Thorup et al[65] reported in 2010 a follow-up of 1.5 to 10 years after Paavilainen procedure on 19 hips with relatively low rate of complications reported after this procedure. Lesser trochanteric osteotomies represent method of progressive femoral shortening at the level of lesser trochanter in order to provide optimal positioning of acetabular cup in anatomic centre in patients with DDH (Figure 4E). Major advantage of this procedure is the fact that greater trochanter remains intact, thus providing better results and potentially lower rate of complications[66]. Bao et al[66], 2013 evaluated the efficacy of lesser trochanteric osteotomy for femoral shortening in total hip arthroplasty in treatment of 28 cases of Crowe IV DDH. After follow-up period of 55.3 mo method was proven to be safe and effective since complications were rare - sciatic nerve palsy was reported in two hips and positive Trendelenburg sign in two hips at the final follow-up. According to report of Bao et al[66] lesser trochanteric osteotomy could serve as valuable solution for femoral shortening in DDH; however, larger groups with longer follow-up are needed in order to bring up propper conclusion. In 2008 we described a modification of the direct lateral approach to the hip, which enables excellent exposure of both, femur and acetabulum and presents an optimal approach through which it is easy to shorten the proximal femur and neutralize leg length discrepancy[7] (Figure 4C). First, anterior half of the continuous tendon is mobilized either by cautery or with a chisel. If the chisel is used, a thin layer of bone from the greater trochanter remains attached to the continuous tendon of the gluteus medius and the vastus lateralis. The posterior half of the continuous tendon of the gluteus medius and the vastus lateralis is always detached with the chisel leaving a bone flake of at least 2 to 3 mm thickness attached to tendons. In that way, the abductor muscles are stripped from the greater trochanter and there is no trochanteric osteotomy during the approach, which allows preservation of the continuity of the abductor muscles. This approach eliminates the necessity for osteotomies of the trochanter and transverse cuts or detachment of the abductor muscles, thus reducing incidence of relatively often complications related to those method[7].
Shortening procedures performed on femoral metaphysis (subtrochanteric osteotomies) are the most frequently used procedures for femoral shortening in DDH. Double Chevron osteotomy was first described by Becker et al[67] in 1995, where total hip arthroplasty was combined with a femoral subtrochanteric shortening derotational double-chevron osteotomy in DDH. First results were promissing, but method of Becker and Gustilo did not allow any intraoperative changes and required complex and detailed preoperative planning that was sometimes hard to perform during surgery. Several modification of the first technique were reported so far, such as the one from Li et al[59] where transverse osteotomy was first performed, followed by rotational alignment in order to correct anteversion. Later, after vertical alignment (length) double chevron osteotomy was performed at the site of the previous transverse osteotomy (Figure 4F). Such method allowed more precise (intraoperative) derotation and shortening adjustment. Several authors with several differences in techniques described transverse subtrochanteric osteotomies. First, Reikeraas et al[68] presented transverse osteotomy in 25 cases, with the use of 4 cemented stems and 21 noncemented stems. The torsional stability was not performed with any fixation. Surprisingly, at 3-7 years later 96% satisfactory results were reported, with no revision procedures or mechanical complications and only 1 delayed union and 1 varus malunion. Similar to this procedure, Yasgur et al[69] reported in 1997 modified techique with enhanced torsional stability with noncemented fully porous-coated stems, press-fit into the diaphysis and augmented with allograft struts and cables on 9 patients. After 2-7 years period 1 patient suffered nonunion of the osteotomy site and one had failure of a distally ingrown porous device, which required revision. Later on, Masonis et al[70] supported the use of a transverse subtrochanteric femoral osteotomy in high DHH with secondary arthritis. 5 years after the procedure was performed a follow-up report was published where authors concluded that the transverse osteotomy union rate was identical to the report using a step-cut method[71]; with one important advantage - it allows intraoperative adjustment of femoral anteversion correction. On the other side, cemented total hip arthroplasty with subtrochanteric transverse osteotomy for Crowe group IV HDD was described by Kawai et al[72] in 2011. Authors descibed procedure where shortening osteotomy sites were covered with grafts of the excised fragments fixed with cerclage wires (Figure 4G). Authors presented good short-term results without significant complications. Bruce et al[73] reported in 2000 a femoral shortening technique with use of straight cylindrical prosthesis that acts as an intramedullary nail. Such prosthesis provides stability control of the distal fragment. First, femoral osteotomy was performed with prosthesis in situ, then, prosthesis was advanced distally and morcellized autologous bone-graft was applied to the osteotomy site. In that way, one of the most important complications after femoral shortening procedure: nonunion of the osteotomy site - was reduced to a minimun[69,72]. This method has all the characteristics of a simple, reliable and flexible surgical technique. Togrul et al[74] in 2010 presented a similar technique of femoral fixation that uses a transverse osteotomy for subtrochanteric shortening with the use of bone pegs prepared from the resected femoral segments which are then placed in the medullar canal around the stem thus providing femoral fixation. Authors reported 21 case with adequate union present in all cases, and early dislocation in only 2 cases.
Shortening procedures performed on femoral diaphysis were reported by Sener et al[71] in 2002, where proximal diaphyseal step-cut shortening osteotomy was performed after femoral reaming. Afterwards, step-cut was stabilised with two to three cerclage wires with the use of bone grafting. After fixation, intramedullary femoral reaming was continued until satisfactory cortical contact was achieved. Special attention was focused on the tight contact in distal fragment of the osteotomized femur (Figure 4H). Authors presented very good 5-year follow-up results. Results of very similar method with promising short-term to mid-term results for a Crowe’s group IV DDH in adult patients were reported by Makita et al[75] in 2007. Later on, Neumann reported the results of very similar technique, but did not use any of the bone grafting techniques at the osteotomy sites[76].
Koulouvaris et al[77] reported in 2008 an interesting combined procedure where distal femoral shortening procedure was performed as an addition to THR of dysplastic and difficult-to-reduce hips. Authors used newer technologies such as the use of customized femoral implants and the use of 3D CT scan as an important tool in preoperative planning[77]. First, total hip arthroplasty with placement of acetabulum in anatomic position was performed. Then, femoral shortening procedure was performed on distal femur in the way that the first screw of the plate would be more than 2 cm separated from the femoral stem. The fixation of the femoral osteotomy was achieved with LC-DCP titanium femoral plate (Figure 4I). One of the major advantages of this technique is the possibility of conjoined correction of the ipsilateral knee valgus deformity, which can be performed simply by changing the shape of osteotomized fragment. In that case, regular fixation for valgus osteotomy of the knee was performed. Twenty-four patients were reported in the study, with follow-up period of 4.5 years. Authors reported excellent results: only 1 delayed union was observed, which resulted in malunion after 9 mo.
As shown above, large number of the femoral shortening procedures is described in literature. However, we have to emphasize that anatomical deformities on the femoral sides of dysplastic hip often require combined correction procedures that are frequently very challenging. According to our and other author’s opinion, such procedures often require detailed preoperative planning combined with experienced surgeon’s skills[78].
CONCLUSION
For severe dysplastic hips, Crowe type III and IV, we perform THA through modified direct lateral approach[7] and then we clean and prepare the acetabulum at the level of the ideal centre of rotation. Even though advantages of the modified approach are numerous one has to take into account that this approach cannot be extended proximally more than 3-4 cm above the tip of greater trochanter and there are some patients that develop pain over greater trochanter. Since there is always lack of bone mass at the level of the ideal acetabular roof, we perform cotyloplasty leaving only paper-thin medial wall, which we break during acetabular cup impacting (Figure 3I and Figure 5). In this way our acetabular dome is always protruding beyond Kohler’s line in the pelvis but with solid primary stability, which we additionally improve by placing 2-3 screws in the superior direction. One has to be aware, as mentioned before, that it is difficult to control the amount of the medial wall fracture and complication such as fracture-dislocation of the cup inside the pelvis can occur. Superolateral area of the acetabulum is left uncovered as much as needed, even more than 30%. Then we proceed with femoral shortening according to Delimar et al[7]. First we peel of all rotators and posterior part of gluteus medius and vastus lateralis from greater trochanter on the very thin flake of bone. Then we shorten proximal femoral stump as much as it is necessary. After femoral broaching and trial reposition we can additionally resect proximal femur. When final components are placed, abductors are sutured (anterior and posterior part one to another but not to the greater trochanter) and leg is lengthened. Postoperative X-rays are taken (Figure 6). Rehabilitation starts on the second day with the same rehabilitation protocol as for any standard THA (when elongation of more than 5 cm is performed than for the first few days extension is not forced). After 4 to 6 wk full weight bearing is allowed but muscle strengthening is continued for additional 6 mo.
Figure 5.
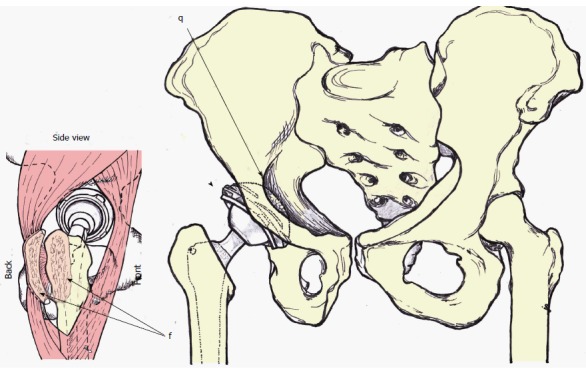
Anterior-posterior and latero-lateral (side) view of the author preferred method of treatment. Anterior-posterior view - acetabular cup is medialized (cotyloplasty) so that the dome of the cup is protruding beyond Kohler’s line inside the pelvis (q marked with single arrow). Superolateral part of the cup is uncovered by the bone (marked with arrowhead). The cup is usually additionally secured with the screws (not show on the picture). latero-lateral (side) view-posterior part of the gluteus medius and vastus lateralis together with the external rotators are detached with the chisel on a thin flake of bone (f marked with double arrows). This is a modified direct lateral approach.
Figure 6.
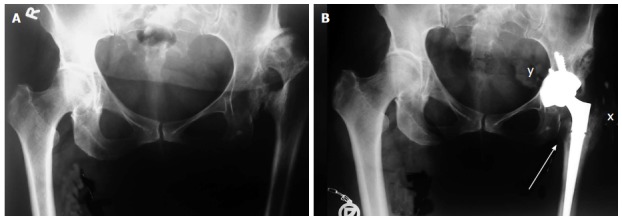
X-rays of patient with Crowe type 4 dysplasia on the left side and normal hip on right side. A: Preoperative X-ray with secondary osteoarthritis due to dysplasia, neoacetabulum formed superolaterally from original, true acetabulum and significant leg length discrepancy; B: Postoperative X-ray with implanted uncemented acetabular cup and femoral stem. Acetabular cup is protruding beyond the Kohler’s line inside the pelvis (marked with y) and secured with 3 additional screws. Lesser trochanter is brought distally to the normal level so there is no leg length discrepancy postoperatively (marked with a single arrow). Modified direct lateral approach was used and posterior part of the gluteus medius and vastus lateralis together with the external rotators were detached with the chisel on a thin flake of bone, now they are completely attached and healed to greater trochanter (marked with x).
Footnotes
P- Reviewer: Aprato A, FisherDA, Klotz MCM S- Editor: Wen LL L- Editor: A E- Editor: Wu HL
References
- 1.Papachristou G, Hatzigrigoris P, Panousis K, Plessas S, Sourlas J, Levidiotis C, Chronopoulos E. Total hip arthroplasty for developmental hip dysplasia. Int Orthop. 2006;30:21–25. doi: 10.1007/s00264-005-0027-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Kumar JN, Kumar JS, Wang VT, Das De S. Medium-term outcome of total hip replacement for dysplastic hips in Singapore. J Orthop Surg (Hong Kong) 2010;18:296–302. doi: 10.1177/230949901001800308. [DOI] [PubMed] [Google Scholar]
- 3.Weinstein S. Developmental hip dysplasia and dislocation. In: Morrissy R, Weinstein S editors Lovell and Winter’s pediatric orthopaedics, editors. Philadelphia: Lippincott Williams and Wilkins; 2001. [Google Scholar]
- 4.Shorter D, Hong T, Osborn DA. Screening programmes for developmental dysplasia of the hip in newborn infants. Cochrane Database Syst Rev. 2011;(9):CD004595. doi: 10.1002/14651858.CD004595.pub2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Erdemli B, Yilmaz C, Atalar H, Güzel B, Cetin I. Total hip arthroplasty in developmental high dislocation of the hip. J Arthroplasty. 2005;20:1021–1028. doi: 10.1016/j.arth.2005.02.003. [DOI] [PubMed] [Google Scholar]
- 6.Yang S, Cui Q. Total hip arthroplasty in developmental dysplasia of the hip: Review of anatomy, techniques and outcomes. World J Orthop. 2012;3:42–48. doi: 10.5312/wjo.v3.i5.42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Delimar D, Bicanic G, Korzinek K. Femoral shortening during hip arthroplasty through a modified lateral approach. Clin Orthop Relat Res. 2008;466:1954–1958. doi: 10.1007/s11999-008-0292-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Kılıçarslan K, Yalçın N, Karataş F, Catma F, Yıldırım H. Cementless total hip arthroplasty for dysplastic and dislocated hips. Eklem Hastalik Cerrahisi. 2011;22:8–15. [PubMed] [Google Scholar]
- 9.Yalcin N, Kilicarslan K, Karatas F, Mutlu T, Yildirim H. Cementless total hip arthroplasty with subtrochanteric transverse shortening osteotomy for severely dysplastic or dislocated hips. Hip Int. 2010;20:87–93. doi: 10.1177/112070001002000113. [DOI] [PubMed] [Google Scholar]
- 10.Charnley J, Feagin JA. Low-friction arthroplasty in congenital subluxation of the hip. Clin Orthop Relat Res. 1973:98–113. doi: 10.1097/00003086-197303000-00015. [DOI] [PubMed] [Google Scholar]
- 11.Hartofilakidis G, Stamos K, Ioannidis TT. Low friction arthroplasty for old untreated congenital dislocation of the hip. J Bone Joint Surg Br. 1988;70:182–186. doi: 10.1302/0301-620X.70B2.3346284. [DOI] [PubMed] [Google Scholar]
- 12.Hartofilakidis G, Yiannakopoulos CK, Babis GC. The morphologic variations of low and high hip dislocation. Clin Orthop Relat Res. 2008;466:820–824. doi: 10.1007/s11999-008-0131-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Steppacher SD, Tannast M, Werlen S, Siebenrock KA. Femoral morphology differs between deficient and excessive acetabular coverage. Clin Orthop Relat Res. 2008;466:782–790. doi: 10.1007/s11999-008-0141-7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Li PL, Ganz R. Morphologic features of congenital acetabular dysplasia: one in six is retroverted. Clin Orthop Relat Res. 2003;(416):245–253. doi: 10.1097/01.blo.0000081934.75404.36. [DOI] [PubMed] [Google Scholar]
- 15.Mast JW, Brunner RL, Zebrack J. Recognizing acetabular version in the radiographic presentation of hip dysplasia. Clin Orthop Relat Res. 2004;(418):48–53. doi: 10.1097/00003086-200401000-00009. [DOI] [PubMed] [Google Scholar]
- 16.Noble PC, Kamaric E, Sugano N, Matsubara M, Harada Y, Ohzono K, Paravic V. Three-dimensional shape of the dysplastic femur: implications for THR. Clin Orthop Relat Res. 2003;(417):27–40. [PubMed] [Google Scholar]
- 17.Robertson DD, Essinger JR, Imura S, Kuroki Y, Sakamaki T, Shimizu T, Tanaka S. Femoral deformity in adults with developmental hip dysplasia. Clin Orthop Relat Res. 1996;(327):196–206. doi: 10.1097/00003086-199606000-00025. [DOI] [PubMed] [Google Scholar]
- 18.Korzinek K, Muftić O. Biomechanical analysis of hip function after Chiari pelvic osteotomy. Arch Orthop Trauma Surg. 1989;108:112–115. doi: 10.1007/BF00932167. [DOI] [PubMed] [Google Scholar]
- 19.Crowe JF, Mani VJ, Ranawat CS. Total hip replacement in congenital dislocation and dysplasia of the hip. J Bone Joint Surg Am. 1979;61:15–23. [PubMed] [Google Scholar]
- 20.Eftekhar N. Congenital dysplasia and dislocation. In: Eftekhar N, editor. Total Hip Arthroplasty: St.Louis, V.Mosby; 1993. p. 92. [Google Scholar]
- 21.Hartofilakidis G, Stamos K, Karachalios T, Ioannidis TT, Zacharakis N. Congenital hip disease in adults. Classification of acetabular deficiencies and operative treatment with acetabuloplasty combined with total hip arthroplasty. J Bone Joint Surg Am. 1996;78:683–692. doi: 10.2106/00004623-199605000-00007. [DOI] [PubMed] [Google Scholar]
- 22.Blackley HR, Howell GE, Rorabeck CH. Planning and management of the difficult primary hip replacement: preoperative planning and technical considerations. Instr Course Lect. 2000;49:3–11. [PubMed] [Google Scholar]
- 23.Hartofilakidis G, Karachalios T. Total hip arthroplasty for congenital hip disease. J Bone Joint Surg Am. 2004;86-A:242–250. doi: 10.2106/00004623-200402000-00005. [DOI] [PubMed] [Google Scholar]
- 24.Kobayashi S, Saito N, Nawata M, Horiuchi H, Iorio R, Takaoka K. Total hip arthroplasty with bulk femoral head autograft for acetabular reconstruction in developmental dysplasia of the hip. J Bone Joint Surg Am. 2003;85-A:615–621. doi: 10.2106/00004623-200304000-00005. [DOI] [PubMed] [Google Scholar]
- 25.Wu X, Li SH, Lou LM, Cai ZD. The techniques of soft tissue release and true socket reconstruction in total hip arthroplasty for patients with severe developmental dysplasia of the hip. Int Orthop. 2012;36:1795–1801. doi: 10.1007/s00264-012-1622-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Turchetto L, Massè A, Aprato A, Barbuio A, Ganz R. Developmental dysplasia of hip: joint preserving surgery in the adolescent and young adult. Minerva Ortopedica e Traumatologica. 2013;64:41–52. [Google Scholar]
- 27.Russotti GM, Harris WH. Proximal placement of the acetabular component in total hip arthroplasty. A long-term follow-up study. J Bone Joint Surg Am. 1991;73:587–592. [PubMed] [Google Scholar]
- 28.Kaneuji A, Sugimori T, Ichiseki T, Yamada K, Fukui K, Matsumoto T. Minimum ten-year results of a porous acetabular component for Crowe I to III hip dysplasia using an elevated hip center. J Arthroplasty. 2009;24:187–194. doi: 10.1016/j.arth.2007.08.004. [DOI] [PubMed] [Google Scholar]
- 29.Bicanic G, Delimar D, Delimar M, Pecina M. Influence of the acetabular cup position on hip load during arthroplasty in hip dysplasia. Int Orthop. 2009;33:397–402. doi: 10.1007/s00264-008-0683-z. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Yoder SA, Brand RA, Pedersen DR, O’Gorman TW. Total hip acetabular component position affects component loosening rates. Clin Orthop Relat Res. 1988;(228):79–87. [PubMed] [Google Scholar]
- 31.Hartofilakidis G, Stamos K, Karachalios T. Treatment of high dislocation of the hip in adults with total hip arthroplasty. Operative technique and long-term clinical results. J Bone Joint Surg Am. 1998;80:510–517. doi: 10.2106/00004623-199804000-00007. [DOI] [PubMed] [Google Scholar]
- 32.Paavilainen T, Hoikka V, Solonen KA. Cementless total replacement for severely dysplastic or dislocated hips. J Bone Joint Surg Br. 1990;72:205–211. doi: 10.1302/0301-620X.72B2.2312556. [DOI] [PubMed] [Google Scholar]
- 33.Shen B, Yang J, Wang L, Zhou ZK, Kang PD, Pei FX. Midterm results of hybrid total hip arthroplasty for treatment of osteoarthritis secondary to developmental dysplasia of the hip-Chinese experience. J Arthroplasty. 2009;24:1157–1163. doi: 10.1016/j.arth.2009.07.002. [DOI] [PubMed] [Google Scholar]
- 34.Haddad FS, Masri BA, Garbuz DS, Duncan CP. Primary total replacement of the dysplastic hip. Instr Course Lect. 2000;49:23–39. [PubMed] [Google Scholar]
- 35.Li H, Wang L, Dai K, Zhu Z. Autogenous impaction grafting in total hip arthroplasty with developmental dysplasia of the hip. J Arthroplasty. 2013;28:637–643. doi: 10.1016/j.arth.2012.07.007. [DOI] [PubMed] [Google Scholar]
- 36.Delimar D, Cicak N, Klobucar H, Pećina M, Korzinek K. Acetabular roof reconstruction with pedicled iliac graft. Int Orthop. 2002;26:344–348. doi: 10.1007/s00264-002-0381-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Fujiwara M, Nishimatsu H, Sano A, Misaki T. Acetabular roof reconstruction using a free vascularized fibular graft. J Reconstr Microsurg. 2006;22:349–352. doi: 10.1055/s-2006-946712. [DOI] [PubMed] [Google Scholar]
- 38.Inao S, Matsuno T. Cemented total hip arthroplasty with autogenous acetabular bone grafting for hips with developmental dysplasia in adults: the results at a minimum of ten years. J Bone Joint Surg Br. 2000;82:375–377. doi: 10.1302/0301-620x.82b3.10465. [DOI] [PubMed] [Google Scholar]
- 39.Kim M, Kadowaki T. High long-term survival of bulk femoral head autograft for acetabular reconstruction in cementless THA for developmental hip dysplasia. Clin Orthop Relat Res. 2010;468:1611–1620. doi: 10.1007/s11999-010-1288-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Delimar D, Bohacek I, Pecina M, Bicanic G. Acetabular roof reconstruction with pedicled iliac graft: ten years later. Int Orthop. 2014;38:199–201. doi: 10.1007/s00264-013-2170-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Delimar D. Comments about “Vascularised pedicled iliac crest graft for selected total hip acetabular reconstructions: a cadaver study”. Surg Radiol Anat. 2004;26:426–427. doi: 10.1007/s00276-004-0266-7. [DOI] [PubMed] [Google Scholar]
- 42.Delimar D, Bićanić G, Pećina M, Korzinek K. Acetabular roof reconstruction with pedicled iliac graft: early clinical experience. Int Orthop. 2004;28:319–320. doi: 10.1007/s00264-004-0555-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43.Shinar AA, Harris WH. Bulk structural autogenous grafts and allografts for reconstruction of the acetabulum in total hip arthroplasty. Sixteen-year-average follow-up. J Bone Joint Surg Am. 1997;79:159–168. doi: 10.2106/00004623-199702000-00001. [DOI] [PubMed] [Google Scholar]
- 44.Kwong LM, Jasty M, Harris WH. High failure rate of bulk femoral head allografts in total hip acetabular reconstructions at 10 years. J Arthroplasty. 1993;8:341–346. doi: 10.1016/s0883-5403(06)80032-x. [DOI] [PubMed] [Google Scholar]
- 45.Mulroy RD, Harris WH. Failure of acetabular autogenous grafts in total hip arthroplasty. Increasing incidence: a follow-up note. J Bone Joint Surg Am. 1990;72:1536–1540. [PubMed] [Google Scholar]
- 46.Bobyn JD, Stackpool GJ, Hacking SA, Tanzer M, Krygier JJ. Characteristics of bone ingrowth and interface mechanics of a new porous tantalum biomaterial. J Bone Joint Surg Br. 1999;81:907–914. doi: 10.1302/0301-620x.81b5.9283. [DOI] [PubMed] [Google Scholar]
- 47.Shirazi-Adl A, Dammak M, Paiement G. Experimental determination of friction characteristics at the trabecular bone/porous-coated metal interface in cementless implants. J Biomed Mater Res. 1993;27:167–175. doi: 10.1002/jbm.820270205. [DOI] [PubMed] [Google Scholar]
- 48.Siegmeth A, Duncan CP, Masri BA, Kim WY, Garbuz DS. Modular tantalum augments for acetabular defects in revision hip arthroplasty. Clin Orthop Relat Res. 2009;467:199–205. doi: 10.1007/s11999-008-0549-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 49.Malizos KN, Bargiotas K, Papatheodorou L, Hantes M, Karachalios T. Survivorship of monoblock trabecular metal cups in primary THA : midterm results. Clin Orthop Relat Res. 2008;466:159–166. doi: 10.1007/s11999-007-0008-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 50.Abeyta PN, Namba RS, Janku GV, Murray WR, Kim HT. Reconstruction of major segmental acetabular defects with an oblong-shaped cementless prosthesis: a long-term outcomes study. J Arthroplasty. 2008;23:247–253. doi: 10.1016/j.arth.2007.01.024. [DOI] [PubMed] [Google Scholar]
- 51.Siebenrock KA, Tannast M, Kim S, Morgenstern W, Ganz R. Acetabular reconstruction using a roof reinforcement ring with hook for total hip arthroplasty in developmental dysplasia of the hip-osteoarthritis minimum 10-year follow-up results. J Arthroplasty. 2005;20:492–498. doi: 10.1016/j.arth.2004.09.045. [DOI] [PubMed] [Google Scholar]
- 52.Gill TJ, Siebenrock K, Oberholzer R, Ganz R. Acetabular reconstruction in developmental dysplasia of the hip: results of the acetabular reinforcement ring with hook. J Arthroplasty. 1999;14:131–137. doi: 10.1016/s0883-5403(99)90115-8. [DOI] [PubMed] [Google Scholar]
- 53.Pitto RP, Schikora N. Acetabular reconstruction in developmental hip dysplasia using reinforcement ring with a hook. Int Orthop. 2004;28:202–205. doi: 10.1007/s00264-004-0559-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 54.Dunn HK, Hess WE. Total hip reconstruction in chronically dislocated hips. J Bone Joint Surg Am. 1976;58:838–845. [PubMed] [Google Scholar]
- 55.Dorr LD, Tawakkol S, Moorthy M, Long W, Wan Z. Medial protrusio technique for placement of a porous-coated, hemispherical acetabular component without cement in a total hip arthroplasty in patients who have acetabular dysplasia. J Bone Joint Surg Am. 1999;81:83–92. doi: 10.2106/00004623-199901000-00012. [DOI] [PubMed] [Google Scholar]
- 56.Lai KA, Liu J, Liu TK. Use of iliofemoral distraction in reducing high congenital dislocation of the hip before total hip arthroplasty. J Arthroplasty. 1996;11:588–593. doi: 10.1016/s0883-5403(96)80114-8. [DOI] [PubMed] [Google Scholar]
- 57.Holinka J, Pfeiffer M, Hofstaetter JG, Lass R, Kotz RI, Giurea A. Total hip replacement in congenital high hip dislocation following iliofemoral monotube distraction. Int Orthop. 2011;35:639–645. doi: 10.1007/s00264-010-1001-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Grill F. Correction of complicated extremity deformities by external fixation. Clin Orthop Relat Res. 1989;(241):166–176. [PubMed] [Google Scholar]
- 59.Li X, Sun J, Lin X, Xu S, Tang T. Cementless total hip arthroplasty with a double chevron subtrochanteric shortening osteotomy in patients with Crowe type-IV hip dysplasia. Acta Orthop Belg. 2013;79:287–292. [PubMed] [Google Scholar]
- 60.Charnley J. The long-term results of low-friction arthroplasty of the hip performed as a primary intervention. J Bone Joint Surg Br. 1972;54:61–76. [PubMed] [Google Scholar]
- 61.Kerboull L, Hamadouche M, Kerboull M. Transtrochanteric approach to the hip. Interact Surg. 2007;2:149–154. [Google Scholar]
- 62.Nercessian OA, Newton PM, Joshi RP, Sheikh B, Eftekhar NS. Trochanteric osteotomy and wire fixation: a comparison of 2 techniques. Clin Orthop Relat Res. 1996;(333):208–216. [PubMed] [Google Scholar]
- 63.Menon PC, Griffiths WE, Hook WE, Higgins B. Trochanteric osteotomy in total hip arthroplasty: comparison of 2 techniques. J Arthroplasty. 1998;13:92–96. doi: 10.1016/s0883-5403(98)90081-x. [DOI] [PubMed] [Google Scholar]
- 64.Kerboull M, Hamadouche M, Kerboull L. Total hip arthroplasty for Crowe type IV developmental hip dysplasia: a long-term follow-up study. J Arthroplasty. 2001;16:170–176. doi: 10.1054/arth.2001.28368. [DOI] [PubMed] [Google Scholar]
- 65.Thorup B, Mechlenburg I, Søballe K. Total hip replacement in the congenitally dislocated hip using the Paavilainen technique: 19 hips followed for 1.5-10 years. Acta Orthop. 2009;80:259–262. doi: 10.3109/17453670902876789. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Bao N, Meng J, Zhou L, Guo T, Zeng X, Zhao J. Lesser trochanteric osteotomy in total hip arthroplasty for treating CROWE type IV developmental dysplasia of hip. Int Orthop. 2013;37:385–390. doi: 10.1007/s00264-012-1758-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Becker DA, Gustilo RB. Double-chevron subtrochanteric shortening derotational femoral osteotomy combined with total hip arthroplasty for the treatment of complete congenital dislocation of the hip in the adult. Preliminary report and description of a new surgical technique. J Arthroplasty. 1995;10:313–318. doi: 10.1016/s0883-5403(05)80180-9. [DOI] [PubMed] [Google Scholar]
- 68.Reikeraas O, Lereim P, Gabor I, Gunderson R, Bjerkreim I. Femoral shortening in total arthroplasty for completely dislocated hips: 3-7 year results in 25 cases. Acta Orthop Scand. 1996;67:33–36. doi: 10.3109/17453679608995605. [DOI] [PubMed] [Google Scholar]
- 69.Yasgur DJ, Stuchin SA, Adler EM, DiCesare PE. Subtrochanteric femoral shortening osteotomy in total hip arthroplasty for high-riding developmental dislocation of the hip. J Arthroplasty. 1997;12:880–888. doi: 10.1016/s0883-5403(97)90157-1. [DOI] [PubMed] [Google Scholar]
- 70.Masonis JL, Patel JV, Miu A, Bourne RB, McCalden R, Macdonald SJ, Rorabeck CH. Subtrochanteric shortening and derotational osteotomy in primary total hip arthroplasty for patients with severe hip dysplasia: 5-year follow-up. J Arthroplasty. 2003;18:68–73. doi: 10.1054/arth.2003.50104. [DOI] [PubMed] [Google Scholar]
- 71.Sener N, Tözün IR, Aşik M. Femoral shortening and cementless arthroplasty in high congenital dislocation of the hip. J Arthroplasty. 2002;17:41–48. doi: 10.1054/arth.2002.27672. [DOI] [PubMed] [Google Scholar]
- 72.Kawai T, Tanaka C, Ikenaga M, Kanoe H. Cemented total hip arthroplasty with transverse subtrochanteric shortening osteotomy for Crowe group IV dislocated hip. J Arthroplasty. 2011;26:229–235. doi: 10.1016/j.arth.2010.03.029. [DOI] [PubMed] [Google Scholar]
- 73.Bruce WJ, Rizkallah SM, Kwon YM, Goldberg JA, Walsh WR. A new technique of subtrochanteric shortening in total hip arthroplasty: surgical technique and results of 9 cases. J Arthroplasty. 2000;15:617–626. doi: 10.1054/arth.2000.4335. [DOI] [PubMed] [Google Scholar]
- 74.Togrul E, Ozkan C, Kalaci A, Gülşen M. A new technique of subtrochanteric shortening in total hip replacement for Crowe type 3 to 4 dysplasia of the hip. J Arthroplasty. 2010;25:465–470. doi: 10.1016/j.arth.2009.02.023. [DOI] [PubMed] [Google Scholar]
- 75.Makita H, Inaba Y, Hirakawa K, Saito T. Results on total hip arthroplasties with femoral shortening for Crowe’s group IV dislocated hips. J Arthroplasty. 2007;22:32–38. doi: 10.1016/j.arth.2006.02.157. [DOI] [PubMed] [Google Scholar]
- 76.Neumann D, Thaler C, Dorn U. Femoral shortening and cementless arthroplasty in Crowe type 4 congenital dislocation of the hip. Int Orthop. 2012;36:499–503. doi: 10.1007/s00264-011-1293-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 77.Koulouvaris P, Stafylas K, Sculco T, Xenakis T. Distal femoral shortening in total hip arthroplasty for complex primary hip reconstruction. A new surgical technique. J Arthroplasty. 2008;23:992–998. doi: 10.1016/j.arth.2007.09.013. [DOI] [PubMed] [Google Scholar]
- 78.Gustke K. The dysplastic hip: not for the shallow surgeon. Bone Joint J. 2013;95-B:31–36. doi: 10.1302/0301-620X.95B11.32899. [DOI] [PubMed] [Google Scholar]