

Abstract
Gallstone ileus is a rare complication of cholelithiasis that has high morbidity and mortality. An intestinal obstruction can be caused by migration of a large gallstone through a biliary enteric fistula or by impaction within the intestinal tract. In this study, we present the case of an 81-year-old woman with a mechanical bowel obstruction by a gallstone that was treated by laparoscopy.
Keywords: gallstone, ileus, laparoscopy
Introduction
Gallstone ileus is a rare complication of cholelithiasis with high morbidity and mortality that accounts for 1–4% of all bowel obstructions. Cholecystoenteric fistulas develop in less than 1% of patients with gallstones.1 An intestinal obstruction can develop from a large gallstone migrating through a biliary enteric fistula or becoming impacted in the intestinal tract; the small bowel, duodenum, and colon could also be obstructed by a gallstone.2 The treatment is based on an enterolithotomy, and fistula repair is controversial.3 Here, we report a gallstone ileus case that was treated with a laparoscopic enterolithotomy without a fistula repair and cholecystectomy.
Case Presentation
An 81-year-old Turkish woman with a mechanical bowel obstruction was referred to our emergency department. The patient had complained of acute abdominal pain, vomiting, and mechanical obstruction for five days before her admission to our emergency service. Her records confirmed that she had cholecystolithiasis for 15 years; a cholecystectomy was offered to her many times by different surgeons, but she refused to undergo the surgery. At physical examination, her abdomen was moderately distended, and tympanic bowel sounds were auscultated. The rectal examination revealed empty ampulla recti. The laboratory test an elevated total leukocyte count (15.6 × 109 cells/L) and slightly increased renal function test values, which could be considered as an indication of pre-renal azotemia. The liver function test results and serum bilirubin levels were normal. Plain radiographs of the abdomen revealed multiple air–fluid levels in the small intestine. The patient was treated with intravenous fluids and antibiotics in the tertiary hospital. On the fifth day of hospitalization, she was referred to our hospital because of the deterioration of her clinical condition. After the initial examination, computed tomography (CT) was performed, which demonstrated small-bowel obstruction by a 40 mm high-density image in a jejunal loop (Fig. 1). Additionally, the scan showed pneumobilia in the left hepatic biliary branch and thickening between the gallbladder and the duodenal walls (Fig. 2). The contrast liquid was observed in the gallbladder, and the air–fluid levels were detected on the CT scan. A cholecystoduodenal fistula resulting from chronic cholelithiasis was suspected.
Figure 1.
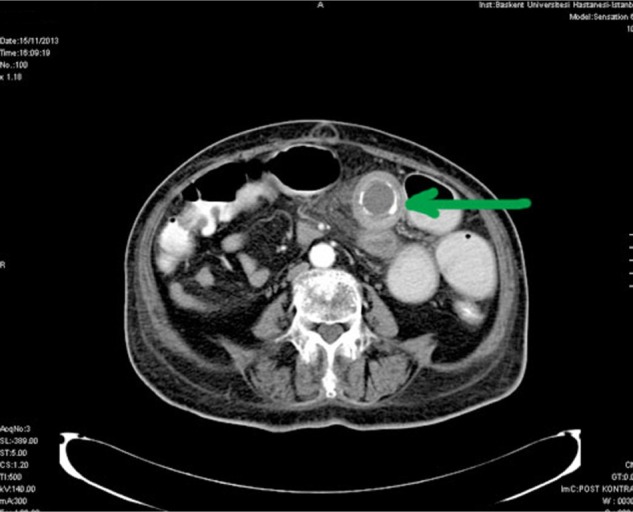
CT image demonstrating small-bowel obstruction due to a 40 mm high-density image within a jejunal loop.
Figure 2.
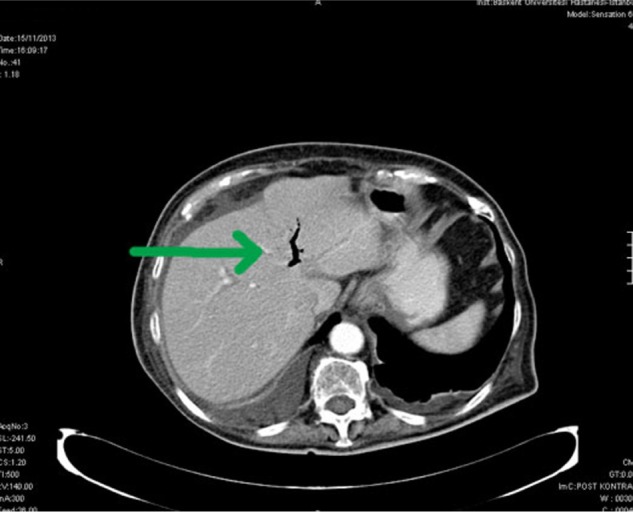
CT images demonstrating free air in the left hepatic biliary branch.
An exploratory laparoscopy was performed. Moderately dilated jejunal loops proximal to the distal jejunum were observed during the laparoscopy. An obstruction was observed approximately 50–60 cm from the ligament of Treitz, where an enterotomy was performed to extirpate a 5 × 4 × 3 cm gallstone (Fig. 3). After the removal of the gallstone, the defect in the intestinal wall was closed, primarily with vicryl sutures. The patient had an uneventful postoperative course and was discharged on postoperative day 5.
Figure 3.

A 5 × 4 × 3 cm gallstone extracted from jejenum.
Discussion
Gallstone ileus is an uncommon manifestation of gallstones, which is caused by migration of a gallstone through a cholecystoduodenal fistula, with impaction at different levels of the gastrointestinal tract. It is considered to be an illness of elderly patients, predominantly individuals with comorbidities, which could increase the complication rate and cause delays in the diagnosis.4,5
The clinical presentation of gallstone ileus is frequently nonspecific, which includes intermittent symptoms of nausea, vomiting, abdominal distension, and pain. Patients with a medical history of cholecystolithiasis and symptoms such as nausea, vomiting, abdominal distension, and pain should be evaluated with greater attention, and a differential diagnosis of gallstone ileus must be considered. The diagnosis should be based on clinical symptoms and radiological findings; CT and magnetic resonance imaging could facilitate the diagnosis of gallstone ileus.6,7 The classic radiological sign of gallstone ileus is the Rigler triad (called the Rigler sign): pneumobilia, intestinal obstruction, and an ectopic gallstone. Plain abdominal radiography could be valuable in the initial workup of a suspected small-bowel obstruction. However, gallstone ileus is easily missed on plain radiographs, because most gallstones are radiolucent and the three elements of the Rigler triad appeared in only 15% of the cases.8–11
Gallstones resulting in an obstruction are larger than 2.5–3 cm.12 The classical findings on plain abdominal radiography include pneumobilia, intestinal obstruction, and abnormal localization of a gallstone.7–11 CT was used for examining bowel obstruction and has sensitivity, specificity, and diagnostic accuracy of 93%, 100%, and 99%, respectively.12 Aerobilia is not easily detected with trans-abdominal ultrasound, and it might cause a delayed diagnosis. Moreover, 50% of the cases could be diagnosed only during surgery.5 However, gallstones smaller than 2–2.5 cm in diameter could spontaneously pass through the gastrointestinal tract. Gallstone ileus is an abdominal emergency, and the following surgical treatments are used: enterotomy with stone extraction alone; enterotomy, stone extraction, cholecystectomy, and fistula closure; bowel resection alone; and bowel resection with fistula closure.13 Enterotomy with stone extraction, without fistula repair and cholecystectomy, is the most common surgical treatment because of its low complication rate.14 In a review of 1,001 reported cases of gallstone ileus, the mortality rate was 16.9% for the one-stage procedure and 11.7% for enterolithotomy alone.5 Gastrointestinal complications were higher in patients with one-stage surgery, depending on whether fistula closure caused leaks.5,13,14
Preserving the gallbladder as the first step might cause the development of biliary symptoms, patent fistula reflux, or biliary malignancy.5,13,14 However, in elderly patients with multiple comorbidities, edematous surrounding areas, and emergency conditions, the initial procedure should ameliorate the urgent situation. To the best of our knowledge, an enterolithotomy should be performed in elderly patients only as an initial intervention. Bowel resection is sometimes necessary, particularly in the presence of a perforation. Laparoscopy-assisted methods have been reported by Sarli et al, who successfully treated three women with gallstone ileus. The laparoscopic approach has been reported in the literature to have a number of advantages associated with minimal invasive surgery.15 Additionally, impacted gallstones accessible by endoscopy are amenable to less-invasive alternative therapeutic options for fragmentation including electrohydraulic lithotripsy (EHL), extracorporeal shock wave lithotripsy, intracorporal laser lithotripsy, and endoscopic mechanical lithotripsy. A limited number of case reports have demonstrated the successful use of EHL in patients with gallstones impacted within the stomach and small intestine.16 The advances in laparoscopic surgery have shown that emergency procedures could be performed safely in elderly patients. However, it is somewhat more challenging in cases of a dilated and edematous bowel. In our case, we preferred the laparoscopic approach, because we expected an early recovery and a low mortality from the procedure.
Conclusion
Gallstone ileus is a rare condition that occurs predominantly in the elderly population. The affected population has significant comorbidities, which could delay the diagnosis. Laparoscopic enterotomy with stone extraction alone might be the first surgical option because of its low mortality and morbidity.
Acknowledgments
We thank Irmak Bircan, our fluent English speaking colleague, for checking the manuscript.
Footnotes
Author Contributions
BK drafted the manuscript while HYB and UO helped in the case summary. BK and HYB are surgeons who operated the patient. AD and OK amended the English and OK proof read the manuscript. All authors reviewed and approved the final manuscript.
ACADEMIC EDITOR: Athavale Nandkishor, Associate Editor
FUNDING: Authors disclose no funding sources.
COMPETING INTERESTS: Authors disclose no potential conflicts of interest.
This paper was subject to independent, expert peer review by a minimum of two blind peer reviewers. All editorial decisions were made by the independent academic editor. All authors have provided signed confirmation of their compliance with ethical and legal obligations including (but not limited to) use of any copyrighted material, compliance with ICMJE authorship and competing interests disclosure guidelines and, where applicable, compliance with legal and ethical guidelines on human and animal research participants.
REFERENCES
- 1.Gasparrini M, Liverani A, Catracchia V, et al. Gallstone ileus: a case report and review of the literature. Chir Ital. 2008;60(5):755–9. [PubMed] [Google Scholar]
- 2.Nuño-Guzmán CM, Arróniz-Jáuregui J, Moreno-Pérez PA, Chávez-Solís EA, Esparza-Arias N, Hernández-González CI. Gallstone ileus: one-stage surgery in a patient with intermittent obstruction. World J Gastrointest Surg. 2010;2(5):172–6. doi: 10.4240/wjgs.v2.i5.172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Narjis Y, Chelala E, Dessily M, Allé JL. Biliary ileus: diagnostic and therapeutic aspects. Report of a case. Rev Med Brux. 2010;31(5):463–5. [PubMed] [Google Scholar]
- 4.Brezean I, Aldoescu S, Catrina E, Fetche N, Marin I, Pãcescu E. Gallstone ileus: analysis of eight cases and review of the literature. Chirurgia (Bucur) 2010;105(3):355–9. [PubMed] [Google Scholar]
- 5.Reisner RM, Cohen JR. Gallstone ileus: a review of 1001 reported cases. Am Surg. 1994;60:441–6. [PubMed] [Google Scholar]
- 6.Gupta M, Goyal S, Singal R, Goyal R, Goyal SL, Mittal A. Gallstone ileus and jejunal perforation along with gangrenous bowel in a young patient: a case report. N Am J Med Sci. 2010;2:442–3. doi: 10.4297/najms.2010.2442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ripollés T, Miguel-Dasit A, Errando J, Morote V, Gómez-Abril SA, Richart J. Gallstone ileus: increased diagnostic sensitivity by combining plain film and ultrasound. Abdom Imaging. 2001;26:401–5. doi: 10.1007/s002610000190. [DOI] [PubMed] [Google Scholar]
- 8.Vasilescu A, Cotea E, Palaghia M, Vintilã D, Târcoveanu FE. Gallstone ileus: a rare cause of intestinal obstruction case report and literature review. Chirurgia. 2013;108:741–4. [PubMed] [Google Scholar]
- 9.Al-Obaid O. Gallstone ileus: a forgotten rare cause of intestinal obstruction. Saudi J Gastroenterol. 2007;13:39–42. doi: 10.4103/1319-3767.30465. [DOI] [PubMed] [Google Scholar]
- 10.Yu CY, Lin CC, Shyu RY, et al. Value of CT in the diagnosis and management of gallstone ileus. World J Gastroenterol. 2005;11:2142–7. doi: 10.3748/wjg.v11.i14.2142. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Dai X-Z, Li G-Q, Zhang F, Wang X-H, Zhang CY. Gallstone ileus: case report and literature review. World J Gastroenterol. 2013;19(33):5586–9. doi: 10.3748/wjg.v19.i33.5586. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Halabi WJ, Kang CY, Ketana N, et al. Surgery for gallstone ileus: a nationwide comparison of trends and outcomes. Ann Surg. 2014;259(2):329–35. doi: 10.1097/SLA.0b013e31827eefed. [DOI] [PubMed] [Google Scholar]
- 13.Sarli L, Pietra N, Costi R, Gobbi S. Gallstone ileus: laparoscopic-assisted enterolithotomy. J Am Coll Surg. 1998;186:370–1. doi: 10.1016/s1072-7515(97)00151-8. [DOI] [PubMed] [Google Scholar]
- 14.Soto DJ, Evan SJ, Kavic MS. Laparoscopic management of gallstone ileus. JSLS. 2001;5(3):279–85. [PMC free article] [PubMed] [Google Scholar]
- 15.Zygomalas A, Karamanakos S, Kehagias I. Totally laparoscopic management of gallstone ileus – technical report and review of the literature. J Laparoendosc Adv Surg Tech A. 2012;22(3):265–8. doi: 10.1089/lap.2011.0375. [DOI] [PubMed] [Google Scholar]
- 16.Apel D, Jakobs R, Benz C, Martin WR, Riemann JF. Electrohydraulic lithotripsy treatment of gallstone after disimpaction of the stone from the duodenal bulb (Bouveret’s syndrome) Ital J Gastroenterol Hepatol. 1999;31:876–9. [PubMed] [Google Scholar]