

Abstract
Athletes at high risk of groin strains in sports such as hockey and soccer often choose to wear shorts with directional compression to aid in prevention or recovery from hip adductor strains. Large eccentric contractions are known to result in or exacerbate strain injuries, but it is unknown if these shorts have a beneficial effect on hip adductor muscle activity. In this study, surface electromyography of the adductor longus and ground reaction force (GRF) data were obtained simultaneously on 29 healthy individuals without previous history of serious injury while performing unanticipated 45° run-to-cut maneuvers in a laboratory setting wearing shorts with non-directional compression (control, HeatGear, Under Armour, USA) or shorts with directional compression (directional, CoreShort PRO, Under Armour, USA), in random order. Average adductor activity in the stance leg was significantly lower in the directional condition than in the control condition during all parts of stance phase (all p<0.042). From this preliminary analysis, wearing directional compression shorts appears to be associated with reduced stance limb hip adductor activity. Athletes seeking to reduce demand on the hip adductors as they approach full return to activities may benefit from the use of directional compression shorts.
Keywords: biomechanics, adductor, strain, groin
1. INTRODUCTION
Groin strain injury is a significant problem in athletes, especially in change-of-direction sports such as soccer and ice hockey, with estimates from 0.8 to 3.2 injuries per 1000 hours of participation (Ekstrand & Hilding, 1999; Emery & Meeuwisse, 2001; Maffey & Emery, 2007). Aside from previous adductor strain injury, which has been shown to be a significant risk factor (Arnason et al., 2004; Emery & Meeuwisse, 2001; Hölmich, Thorborg, Dehlendorff, Krogsgaard, & Gluud, 2013), the causes and risk factors for groin strain injury remain elusive, with conflicting reports on the importance of adductor flexibility, adductor strength, age, and pre-season training (Emery & Meeuwisse, 2001; Engebretsen, Myklebust, Holme, Engebretsen, & Bahr, 2010; Maffey & Emery, 2007; Thorborg et al., 2011; Tyler, Nicholas, Campbell, & McHugh, 2001; Witvrouw, Danneels, Asselman, D’Have, & Cambier, 2003). Moreover, adductor strain injuries can often be very slow to heal (Hölmich et al., 1999; Thorborg & Hölmich, 2013), leading to a chronic musculoskeletal condition that an athlete must manage. Regardless of etiology or acuteness of symptoms, the adductor strain injury in an athlete can be defined as “pain during adduction against resistance,” (Nicholas & Tyler, 2002) which suggests that limiting the requirement for active contraction of the adductors during activity may result in some relief of symptoms.
Anecdotally, many athletes in sports such as ice hockey and soccer, where groin muscle strains are common, have chosen to wear compression shorts to aid in the prevention or recovery from adductor strains. Compression shorts are becoming increasingly popular with athletes, with annual sales in the U.S. estimated at $8.4 million in 2010, a 56% increase over 2009 (Day, 2011). These shorts are often used by athletes hoping to improve performance and lower the likelihood of injury. Compression shorts are thought to aid the athlete by dynamically supporting the muscle to enhance venous return and reduce edema (Kraemer et al., 2001), or by enhancing proprioception at the hip joint (Bernhardt & Anderson, 2005; Kraemer et al., 1998). However, the benefit of compression shorts to athletes has been variable in laboratory testing (Bernhardt & Anderson, 2005; Bringard, Perrey, & Belluye, 2006; Doan et al., 2003; Kraemer, et al., 1998). In particular, compression shorts have not demonstrated performance benefits in speed, agility, balance or vertical jump height (Bernhardt & Anderson, 2005; Duffield & Portus, 2007), although they have been observed to reduce muscle soreness in the legs 24 hours after exercise (Duffield & Portus, 2007). Part of the discrepancy found in the literature could be due to the testing of compression shorts of varying material, compression or design, and the measuring of endpoints that are multifactorial in nature (athletic performance, fatigue, etc.) instead of testing more specific effects (e.g. muscle activation).
In spite of the popularity of compression shorts, especially with those interested in avoiding or recovering from adductor strains, little testing has been performed on the effects of specialized compression shorts on muscle recruitment or activation during athletic movements. Several manufacturers have employed directional compression fabrics in an effort to change the properties of the garment. One model of directional compression shorts, the CoreShort PRO (Under Armour, USA), differs from traditional compression shorts through their use of both traditional isotropic compression (i.e. fabric stretches the same amount in all directions) and circumferential compression applied in a diagonal band around the core and hips (Bernhardt & Anderson, 2005). The diagonal compression is intended to mimic the diagonal pull of the hip adductor muscles (Neumann, 2010), potentially aiding in resisting abduction of the hips during athletic movements. This diagonal band of fabric only stretches along a single axis, effectively compressing more tightly along the axis perpendicular to the band. Though previous research on these particular shorts focused on athletic performance (Bernhardt & Anderson, 2005), this study focused in particular on activation of the hip adductors during a run-to-cut maneuver, a movement which includes an eccentric contraction of the hip adductors and can be especially painful and difficult in a patient recovering from an adductor injury (Nicholas & Tyler, 2002). The goal of this study was to test whether the directional compression afforded by the directional shorts reduces hip adductor activation. We tested the hypothesis that average activation of the adductor longus muscle would be different during the stance phase of a run-to-cut maneuver with directional compression shorts than with traditional compression shorts.
2. METHODS
2.1 Participants
The university’s IRB approved this study. 46 participants were recruited to participate. Participants had no prior history of lower extremity or abdominal surgery. Participants had no history of serious lower extremity injury (ACL, ligament, tendon, muscle, or meniscus tear) or abdominal hernia. No participants had any history of a groin-related injury, and none experienced any discomfort while participating in the study. Participants with a BMI greater than 30 were excluded due to the inaccuracy of measuring muscle activation in the presence of excessive subcutaneous fatty tissue (Hemingway, Biedermann, & Inglis, 1995; Kuiken, Lowery, & Stoykov, 2003; Nordander et al., 2003). Participants had to have been active in athletic participation at least 3 times a week for the previous 3 months before testing. All participants self-reported a Tegner activity score of at least 5 (Tegner & Lysholm, 1985). This Tegner score of 5 or more ensured that, at minimum, participants cycled, cross-country skied, or ran on uneven ground at least twice a week. Other inclusion criteria included a complete dataset with both force plate and adductor EMG data. Surface electromyography of the adductor longus and ground reaction force (GRF) data were successfully obtained from 29 participants in the study (16M, 13F; age 23.4±4.8y; height 1.76±0.11m; mass 71.1±12.7kg). 87% (25/29) of these participants reported regular participation in sports including rapid changes of direction, including soccer, basketball, tennis, ice hockey, crossfit, American football, racquetball, rugby, gymnastics, badminton, softball and volleyball (Tegner score of at least 6). The dominant leg was identified as the one with which the participant would prefer to kick a ball.
2.2 Compression shorts
Participants were fitted with both a standard compression short with isotropic stretch (HeatGear, Under Armour, USA) and directional compression shorts (CoreShort PRO, Under Armour, USA) (Figure 1). For both shorts, hip and waist circumference measurements were made with a measuring tape, and sizes were determined based on the manufacturer’s recommendation using waist circumference for males, and hip circumference for females. The diagonal bands of material in the directional compression shorts (black in Figure 1) restrict stretch across their width, creating additional compression along the net line of action of the primary and secondary hip adductor muscles (Neumann, 2010). Due to the obvious difference in appearance between the control and directional compression shorts (Figure 1), it was not possible to blind either the participants or testers to the shorts condition at the time of testing.
Figure 1.

Participant wearing traditional compression shorts which stretch isotropically in all 4 directions (left), and directional compression shorts (right) with diagonal bands of fabric that only stretch along their length (black fabric). The same sizing guidelines were used to fit both types of shorts to each participant.
2.3 Electromyography
As an approximation of general hip adductor muscle activity, activation of the adductor longus were quantified using telemetric surface electromyography (EMG) (Telemyo DTS; Noraxon, USA). Moreover, adductor-related groin injuries have been reported to be most often associated with the adductor longus in soccer players (Hölmich, 2007). The surface of the skin was prepped by shaving the spot of electrode placement if necessary, and scrubbing with an alcohol pad until the skin was slightly pink to reduce impedance. Disposable self-adhesive dual Ag/AgCl surface electrodes (40mm inter-electrode distance, Vermed, USA) were placed bilaterally over the adductor longus. Electrodes were placed according to Criswell (Criswell, 2011). A single experienced male examiner placed all electrodes on the male participants, while a single experienced female examiner placed all electrodes on the female participants. Both examiners were formally trained by a sports physical therapist with over 10 years in practice (author LCS) to ensure consistent electrode placement. Raw EMG data were recorded at 1500Hz with a built-in 10–500Hz band pass filter, then high-pass filtered at 10Hz with a zero-lag 4th order Butterworth filter to remove motion artifact. Filtered EMG data were then full wave rectified and smoothed using an RMS filter with a 20ms window. The RMS data was then normalized by a maximum voluntary isometric contraction (MVIC) for each side to obtain continuous EMG curves of %MVIC. All EMG data post-processing was performed using custom scripts in MATLAB (Mathworks, USA).
One MVIC trial was performed for hip adduction while standing on each side using non-elastic nylon straps attached to a wall and wrapped around the shank just above the malleoli. Strap lengths and participant positions were adjusted to ensure that all participants performed MVIC trials at 0° of hip adduction. Intra-session reliability of adductor strength measurements in this configuration is high, with an ICC ≥ 0.85 (Kollock, Onate, & Van Lunen, 2010). Participants wore running shorts over the electrodes for these trials. Raw EMG data was viewed in real time to confirm that the participant was achieving strong adductor longus contraction each time. MVIC trials were filtered at 10Hz, rectified and smoothed using an RMS filter with a 20ms window. A 500ms running average of the RMS smoothed data was calculated for each muscle during each of the MVIC trials. The highest 500ms running average was used for normalization.
2.4 Unanticipated run-to-cut maneuver
Participants performed 45° unanticipated side-step run-to-cut maneuvers to both sides in one pair of shorts, then the other in random order. Unanticipated cutting at this angle was used because it closely matches the movements experienced during soccer, when players have to react to changing game situations. Furthermore, differences in knee loading have been reported between anticipated and unanticipated cutting (Besier et al., 2001a). For the cut, participants started on a pressure sensitive mat, took three steps at a self-selected pace, then planted the desired foot within an area (80cm wide × 60cm long) defined by two force plates collecting data at 1500Hz (Bertec 4060-10; Bertec, USA) placed side-by-side (Figure 2). The distance between the starting mat and the force plate was customized so that each participant could maintain a natural stride and strike the force plate with the desired foot after the three run-up steps. At a set delay after leaving the start mat of between 0.5s–1.4s, one of two arrows, chosen at random, would illuminate instructing the participant to either continue to run straight ahead or to perform the side-step cut. This delay was initially set at 0.5s for each participant, then increased until the participant could successfully complete the maneuver. A successful cut was one in which the participant planted his/her desired foot within the area of the force plates and his/her new direction lay over a line drawn on the ground at a 45° angle to the approach path, originating at the center of the force plates. The task was performed for one randomly selected foot first until 4 successful trials were collected, followed by 4 successful trials for the other foot. Participants were permitted to rest as much as they desired between trials to avoid fatigue effects.
Figure 2.
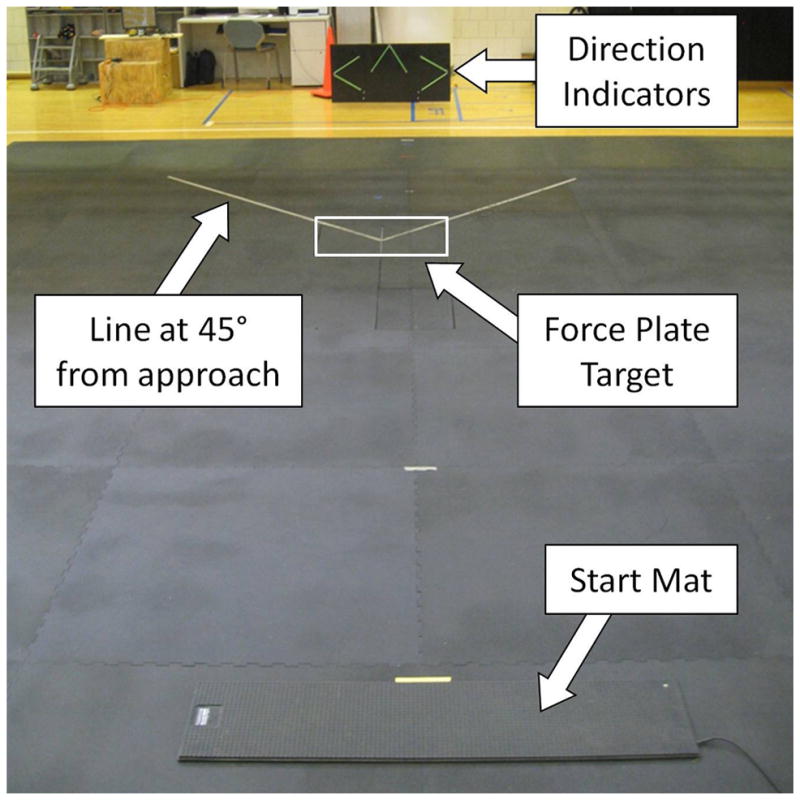
Unanticipated run-to-cut maneuver set-up. Participants started on the pressure sensitive start mat, took three steps at a self-selected jog pace, then planted their foot within the target area. A direction indicator would light up during the approach indicating whether to continue to run straight or to perform the side-step cut. Direction was chosen at random. Both right and left foot plants are possible with this set-up.
To identify whether differences in muscle activations occurred throughout the activity or only during specific phases, the average activation of the ipsilateral adductor longus (of the leg that was planted on the floor) was calculated over 5 specific phases based on the vertical ground reaction force (Figure 3). The pre-contact (PC) phase was defined as the 50ms before foot strike. The early contact (EC) phase was defined as the first 50ms after foot strike. Peak Push Off (PPO) phase was defined as 20% of the total stance phase (foot strike to toe off) centered about the local peak of the vertical ground reaction force near midstance (Besier, Lloyd, Cochrane, & Ackland, 2001). Weight acceptance (WA) phase was defined from the end of EC to the beginning of PPO, while Final Push Off (FPO) was defined from the end of PPO until toe off, which we modified from Besier’s method (Besier, et al., 2001) to eliminate any gaps between phases.
Figure 3.
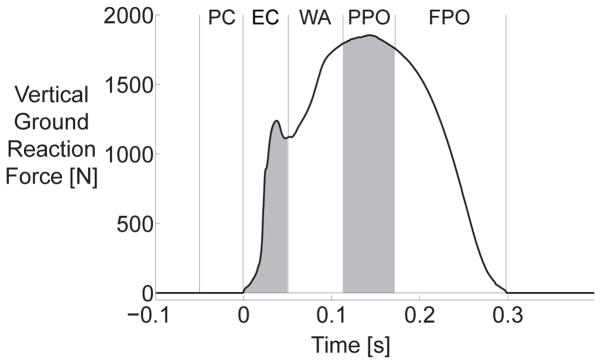
A typical vertical ground reaction force curve showing the five identified phases for analysis. The pre-contact (PC) phase was defined as the 50ms before foot strike. The early contact (EC) phase was defined as the first 50ms after foot strike. Peak Push Off (PPO) phase was defined as 20% of the total stance phase (foot strike to toe off) centered about the local peak of the vertical ground reaction force near midstance. (Besier, et al., 2001) Weight acceptance (WA) phase was defined from the end of EC to the beginning of PPO, while Final Push Off (FPO) was defined from the end of PPO until toe off.
Each raw and processed EMG signal for each trial was manually inspected to maintain quality control. EMG of questionable quality (inappropriate magnitude or frequency suggesting movement of electrodes or missing data due to loss of connection between wireless transmitters and receiver during testing) was marked as invalid and withheld from subsequent analysis. 26 participants had a complete dataset for both legs, while 3 additional participants had a complete dataset for one leg only, providing 29 total participants for statistical analysis. During the data reduction and inspection phases, all data processing personnel were blinded to the shorts condition.
2.5 Statistical Analysis
The muscle activations of the adductor longus at different phase of activities were summarized for the two shorts conditions for each planting leg (dominant vs. non-dominant). To test the difference of the muscle activation between the two shorts conditions, mixed models for repeated measures with random planting foot effects were used for each of the five phases of the activity (SAS 9.2, SAS Institute, USA). All conclusions were confirmed by sensitivity analyses with different statistical models, including (1) mixed models using the five phases & planting foot as a random effect, and (2) mixed models using log transformed data. In an exploratory analysis to determine whether the results could be influenced by a difference in performance of the cutting maneuver, a similar mixed model was used to examine any differences in the total ground reaction force impulse over the entire stance phase between the shorts conditions.
3. RESULTS
The ipsilateral adductor longus activation during the five phases for different shorts and different leg (dominant or non-dominant) are summarized in Figure 4. We found a significantly lower activation of the adductor when participants were wearing the directional compression shorts in every phase of the run-to-cut task: during the pre-contact (PC), early contact (EC), weight acceptance phases (WA), peak push off (PPO), and final push off (FPO). No significant difference was observed between the dominant and non-dominant foot overall (p=0.16), although a significant difference was observed between dominant and non-dominant feet during the FPO phase (p=0.048). No significant shorts x foot interaction was observed for any phases (overall p=0.44), implying both legs reduced adductor activation in the directional shorts to a similar degree. Total ground reaction force impulse over the entire stance phase was not significantly different between the shorts conditions (p=0.26).
Figure 4.

Ipsilateral adductor longus activation during the five phases of stance divided by foot and shorts condition. Total ground reaction force impulse across the entire stance phase is also shown (bottom rows).
Secondary analyses showed the activation of these five phases are highly associated with each other (Pearson correlation for the log transformed data range from 0.62 to 0.89, all p<0.001), but the mean %MVIC values are different at different phases (p<0.001). However, no statistically significant shorts x phase interaction was observed (p=0.20), indicating that the overall pattern of activation across stance remains consistent between the directional and the control shorts conditions.
4. DISCUSSION
The results of this study supported the hypothesis that the directional compression shorts altered adductor activation during run-to-cut maneuvers and demonstrated reduced adductor activation in the directional condition. Given that muscle strain injuries to the adductors typically occur in conditions where athletes are eccentrically contracting the muscle (Friden & Lieber, 1992; Lieber & Friden, 1993), reduced demand on the adductor longus may reduce the risk of a strain injury during cutting or other lateral change-of-direction maneuvers. These results also give a preliminary indication that these shorts may provide some symptomatic relief to individuals experiencing pain due to adductor strain injury since these injuries are defined by “pain during adduction against resistance.” (Nicholas & Tyler, 2002) An examination of previous data for run-to-cut maneuvers (Jamison, Pan, & Chaudhari, 2012) qualitatively demonstrates several kinematic patterns that may implicate use of the hip adductor complex. The hip adducts just before contact, perhaps to position the plant foot. During early and middle stance, the hip remains isometric in the presence of an external hip abduction moment. During late stance and early swing, the hip adducts. All of these motions would utilize the hip adductors, so a reduction in demand for the adductor longus could reduce the risk of a strain injury. The present analysis did not include measurement of joint kinematics or kinetics or activations of other muscles, but future work may shed additional light on the movements associated with the observed muscle activations as well as any alterations of other muscles to either reciprocally inhibit adductor activation or compensate for reduced adductor activation.
While this study was performed with uninjured individuals, the results indicate the potential benefit of directional compression shorts in athletes recovering from an adductor muscle strain. Active training programs, including strength training of the core and hip (including the adductor complex) muscles along with coordination and balance activities, are advocated in preventing adductor injuries (Holmich, Larsen, Krogsgaard, & Gluud, 2010; Tyler, Nicholas, Campbell, Donellan, & McHugh, 2002), as well as treating athletes with adductor-related injuries (Holmich, Nyvold, & Larsen, 2011; Hölmich, et al., 1999). A reduction in the demand on the adductor muscles as observed in this study in the directional condition may be beneficial in the advanced phases of rehabilitation as the patient is progressed toward cutting, pivoting or sport-specific activities and during continued sports participation. However, it should be noted that reduced activation does not necessarily equate to a reduced demand on the muscle. Reduced activation combined with similar demand could lead to increased passive stretch of the muscle fibers or the musculotendinous junction. Future work is warranted to evaluate the influence of directional compression in athletes with adductor-related groin injuries, as well as the influence of reduced adductor muscle activation on injury recovery and outcome.
While it was beyond the scope of this study to examine changes in joint kinematics or load sharing between the shorts and the muscles, these both could trigger the differences observed. If the directional compression shorts were stiff enough to limit frontal plane or transverse plane motion at the hip, the thigh could remain relatively adducted such that there was a reduced requirement for the adductors to pull the thigh into adduction. Moreover, stretch of the material could potentially aid in energy storage and recovery such that the adductors received assistance in adducting the thigh. A more complete characterization of the mechanical properties of the directional compression shorts combined with in vivo measurement of the strain in the fabric would be necessary to determine how much of a hip adduction moment can be generated by the shorts themselves to reduce the requirements on the adductors.
The results of this study should be considered in light of its limitations. As mentioned above, kinematic data for the hip and other joints was not collected. Therefore, it is unknown whether the participants were as effective in performing the run-to-cut maneuver while wearing the directional compression shorts as while wearing the control shorts. However, as a check for overall performance the total ground reaction impulse was examined, and it did not differ significantly between conditions (Figure 4, bottom). This lack of a difference suggests that participants were pushing off the floor to change direction with a similar level of intensity in both shorts conditions. The lack of kinematic data or electromyography data of more distal muscles also makes it impossible to tell whether participants employed any compensations, positive or negative, in response to reduced usage of the adductor longus.
Surface electromyography during this dynamic maneuver also had its limitations in this study. Both motion artifacts and data loss due to wireless signal loss reduced the number of available participants from those initially recruited. In addition, due to the close proximity of the hip adductors and difficulty in pinpointing activation of individual adductor muscles with surface electrodes, we used an electrode placement that targeted adductor longus as a surrogate for all hip adductor activity. However, the individual muscles may not all activate in unison, so the reduction in adductor activity observed here may not apply equally to all hip adductor muscles.
Another limitation lies in the lack of blinding in this study. Participants reported that the directional compression shorts had a tighter fit, and the visible difference in appearance of the two shorts made it clear to both tester and participant which was which. However, this fact was unlikely to influence the results, because the participants were not familiar with the hypothesis of the study. Moreover, during data processing all study personnel were blinded to the condition until after all the results were calculated.
Lastly, while this population represented a wide variety of sport experience, body size, strength, and other factors, it does not ideally represent the soccer or ice hockey athletes who are at high risk of adductor strains. The study sample was chosen to test the differences that might occur across all the populations who may choose to wear these shorts. High level soccer or ice hockey athletes may demonstrate different patterns of muscle activity from the tested population at the speeds tested, as well as much higher speeds of activity during game situations. Moreover, athletes who are recovering from a groin muscle strain may have altered muscle activation patterns either due to or pre-dating the index injury, and may therefore respond differently to these compression shorts than the general population.
5. CONCLUSION
Wearing the directional compression shorts was associated with reduced ipsilateral adductor longus activity during run-to-cut maneuvers, which could potentially aid in the relief of symptoms in individuals recovering from adductor strain injuries or even alter the risk of suffering an adductor strain injury. While our findings from this study are encouraging, further evaluation of the influence of the directional compression shorts is necessary. Randomized controlled trials of the directional shorts v. traditional compression shorts would determine the effectiveness of the directional shorts to reduce symptoms, accelerate return to sport, or reduce incidence of adductor strain injuries.
Acknowledgments
Support for this study came via a research grant from Under Armour, Inc. X. Pan is also partially supported by the United States National Center for Advancing Translational Sciences (8UL1TR000090-05). The authors also gratefully acknowledge the assistance of Julie Thompson in data collection.
References
- Arnason A, Sigurdsson SB, Gudmundsson A, Holme I, Engebretsen L, Bahr R. Risk Factors for Injuries in Football. The American Journal of Sports Medicine. 2004;32(1 suppl):5S–16S. doi: 10.1177/0363546503258912. [DOI] [PubMed] [Google Scholar]
- Bernhardt T, Anderson GS. Influence of moderate prophylactic compression on sport performance. Journal of Strength and Conditioning Research. 2005;19(2):292–297. doi: 10.1519/1533-4287(2005)19[292:IOMPCO]2.0.CO;2. [DOI] [PubMed] [Google Scholar]
- Besier TF, Lloyd DG, Cochrane JL, Ackland TR. External loading of the knee joint during running and cutting maneuvers. Medicine and Science in Sports and Exercise. 2001;33(7):1168–1175. doi: 10.1097/00005768-200107000-00014. [DOI] [PubMed] [Google Scholar]
- Bringard A, Perrey S, Belluye N. Aerobic energy cost and sensation responses during submaximal running exercise positive effects of wearing compression tights. International Journal of Sports Medicine. 2006;27(5):373–378. doi: 10.1055/s-2005-865718. [DOI] [PubMed] [Google Scholar]
- Criswell E. Cram’s Introduction to Surface Electromyography. 2. Sudbury, MA: Jones and Bartlett; 2011. [Google Scholar]
- Day J. Compression apparel tightening grip on market. Sports Insight. 2011 Mar-Apr;:65–66. [Google Scholar]
- Doan BK, Kwon YH, Newton RU, Shim J, Popper EM, Rogers RA, Kraemer WJ. Evaluation of a lower-body compression garment. Journal of Sports Sciences. 2003;21(8):601–610. doi: 10.1080/0264041031000101971. [DOI] [PubMed] [Google Scholar]
- Duffield R, Portus M. Comparison of three types of full-body compression garments on throwing and repeat-sprint performance in cricket players. British Journal of Sports Medicine. 2007;41(7):409–414. doi: 10.1136/bjsm.2006.033753. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ekstrand J, Hilding J. The incidence and differential diagnosis of acute groin injuries in male soccer players. Scandinavian Journal of Medicine and Science in Sports. 1999;9(2):98–103. doi: 10.1111/j.1600-0838.1999.tb00216.x. [DOI] [PubMed] [Google Scholar]
- Emery CA, Meeuwisse WH. Risk factors for groin injuries in hockey. Medicine and Science in Sports and Exercise. 2001;33(9):1423–1433. doi: 10.1097/00005768-200109000-00002. [DOI] [PubMed] [Google Scholar]
- Engebretsen AH, Myklebust G, Holme I, Engebretsen L, Bahr R. Intrinsic Risk Factors for Groin Injuries Among Male Soccer Players: A Prospective Cohort Study. The American Journal of Sports Medicine. 2010;38(10):2051–2057. doi: 10.1177/0363546510375544. [DOI] [PubMed] [Google Scholar]
- Friden J, Lieber RL. Structural and mechanical basis of exercise-induced muscle injury. Medicine and Science in Sports and Exercise. 1992;24(5):521–530. [PubMed] [Google Scholar]
- Hemingway MA, Biedermann HJ, Inglis J. Electromyographic recordings of paraspinal muscles: Variations related to subcutaneous tissue thickness. Biofeedback and Self-Regulation. 1995;20(1):39–49. doi: 10.1007/bf01712765. [DOI] [PubMed] [Google Scholar]
- Hölmich P. Long-standing groin pain in sportspeople falls into three primary patterns, a “clinical entity” approach: a prospective study of 207 patients. British Journal of Sports Medicine. 2007;41(4):247–252. doi: 10.1136/bjsm.2006.033373. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Holmich P, Larsen K, Krogsgaard K, Gluud C. Exercise program for prevention of groin pain in football players: a cluster-randomized trial. [Randomized Controlled Trial] Scandinavian Journal of Medicine and Science in Sports. 2010;20(6):814–821. doi: 10.1111/j.1600-0838.2009.00998.x. [DOI] [PubMed] [Google Scholar]
- Holmich P, Nyvold P, Larsen K. Continued significant effect of physical training as treatment for overuse injury: 8- to 12-year outcome of a randomized clinical trial. [Randomized Controlled Trial] The American Journal of Sports Medicine. 2011;39(11):2447–2451. doi: 10.1177/0363546511416075. [DOI] [PubMed] [Google Scholar]
- Hölmich P, Thorborg K, Dehlendorff C, Krogsgaard K, Gluud C. Incidence and clinical presentation of groin injuries in sub-elite male soccer. British Journal of Sports Medicine. 2013 doi: 10.1136/bjsports-2013-092627. [DOI] [PubMed] [Google Scholar]
- Hölmich P, Uhrskou P, Ulnits L, Kanstrup IL, Nielsen MB, Bjerg AM, Krogsgaard K. Effectiveness of active physical training as treatment for long-standing adductor-related groin pain in athletes: randomised trial. The Lancet. 1999;353(9151):439–443. doi: 10.1016/S0140-6736(98)03340-6. http://dx.doi.org/10.1016/S0140-6736(98)03340-6. [DOI] [PubMed] [Google Scholar]
- Jamison ST, Pan X, Chaudhari AMW. Knee Moments During Run-to-Cut Maneuvers Are Associated With Lateral Trunk Positioning. Journal of Biomechanics. 2012;45(11):1881–1885. doi: 10.1016/j.jbiomech.2012.05.031. [DOI] [PubMed] [Google Scholar]
- Kollock RO, Jr, Onate JA, Van Lunen B. The Reliability of Portable Fixed Dynamometry During Hip and Knee Strength Assessments. Journal of Athletic Training. 2010;45(4):349–356. doi: 10.4085/1062-6050-45.4.349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kraemer WJ, Bush JA, Triplett-McBride NT, Koziris LP, Mangino LC, Fry AC, Newton RU. Compression garments: Influence on muscle fatigue. Journal of Strength and Conditioning Research. 1998;12(4):211–215. [Google Scholar]
- Kraemer WJ, Bush JA, Wickham RB, Denegar CR, Gomez AL, Gotshalk LA, Sebastianelli WJ. Continuous compression as an effective therapeutic intervention in treating eccentric-exercise-induced muscle soreness. Journal of Sport Rehabilitation. 2001;10(1):11–23. [Google Scholar]
- Kuiken TA, Lowery MM, Stoykov NS. The effect of subcutaneous fat on myoelectric signal amplitude and cross-talk. Prosthetics and Orthotics International. 2003;27(1):48–54. doi: 10.3109/03093640309167976. [DOI] [PubMed] [Google Scholar]
- Lieber RL, Friden J. Muscle damage is not a function of muscle force but active muscle strain. Journal of Applied Physiology. 1993;74(2):520–526. doi: 10.1152/jappl.1993.74.2.520. [DOI] [PubMed] [Google Scholar]
- Maffey L, Emery C. What are the Risk Factors for Groin Strain Injury in Sport?: A Systematic Review of the Literature. Sports Medicine. 2007;37(10):881–894. doi: 10.2165/00007256-200737100-00004. [DOI] [PubMed] [Google Scholar]
- Neumann DA. Kinesiology of the Hip: A Focus on Muscular Actions. Journal of Orthopaedic and Sports Physical Therapy. 2010;40(2):82–94. doi: 10.2519/jospt.2010.3025. [DOI] [PubMed] [Google Scholar]
- Nicholas SJ, Tyler TF. Adductor Muscle Strains in Sport. Sports Medicine. 2002;32(5):339–344. doi: 10.2165/00007256-200232050-00005. [DOI] [PubMed] [Google Scholar]
- Nordander C, Willner J, Hansson GA, Larsson B, Unge J, Granquist L, Skerfving S. Influence of the subcutaneous fat layer, as measured by ultrasound, skinfold calipers and BMI, on the EMG amplitude. European journal of applied physiology. 2003;89(6):514–519. doi: 10.1007/s00421-003-0819-1. [DOI] [PubMed] [Google Scholar]
- Tegner Y, Lysholm J. Rating Systems in the Evaluation of Knee Ligament Injuries. Clinical orthopaedics and related research. 1985;(198):43–49. [PubMed] [Google Scholar]
- Thorborg K, Hölmich P. Advancing hip and groin injury management: from eminence to evidence. British Journal of Sports Medicine. 2013 doi: 10.1136/bjsports-2012-092090. [DOI] [PubMed] [Google Scholar]
- Thorborg K, Serner A, Petersen J, Madsen TM, Magnusson P, Hölmich P. Hip Adduction and Abduction Strength Profiles in Elite Soccer Players: Implications for Clinical Evaluation of Hip Adductor Muscle Recovery After Injury. The American Journal of Sports Medicine. 2011;39(1):121–126. doi: 10.1177/0363546510378081. [DOI] [PubMed] [Google Scholar]
- Tyler TF, Nicholas SJ, Campbell RJ, Donellan S, McHugh MP. The effectiveness of a preseason exercise program to prevent adductor muscle strains in professional ice hockey players. American Journal of Sports Medicine. 2002;30(5):680–683. doi: 10.1177/03635465020300050801. [DOI] [PubMed] [Google Scholar]
- Tyler TF, Nicholas SJ, Campbell RJ, McHugh MP. The Association of Hip Strength and Flexibility With the Incidence of Adductor Muscle Strains in Professional Ice Hockey Players. The American Journal of Sports Medicine. 2001;29(2):124–128. doi: 10.1177/03635465010290020301. [DOI] [PubMed] [Google Scholar]
- Witvrouw E, Danneels L, Asselman P, D’Have T, Cambier D. Muscle Flexibility as a Risk Factor for Developing Muscle Injuries in Male Professional Soccer Players: A Prospective Study. The American Journal of Sports Medicine. 2003;31(1):41–46. doi: 10.1177/03635465030310011801. [DOI] [PubMed] [Google Scholar]