

Abstract
We report an unusual case of Axenfeld–Rieger Syndrome with secondary glaucoma managed with Ologen® implant. A 35-year-old male presented with complaints of decreased vision in both eyes of 22 years duration. His best corrected visual acuity (BCVA) was no perception of light in right eye and 20/30 in left eye. Gonioscopy revealed anterior insertion of iris into trabecular meshwork, prominent iris processes and broad-based synechiae with prominent Schwalbe's line along the angle circumference with cord-like structures taking its origin at the level of Schwalbe's line in both eyes. Fundus examination revealed total glaucomatous optic atrophy in right eye with 0.9:1 cup disc ratio with bipolar notch in left eye. Humphrey visual field analysis showed superior and inferior arcuate scotoma in left eye. Intraocular pressure measured by Goldman applanation tonometry was 30 mmHg and 26 mmHg in right and left eye, respectively. After an unsuccessful medical management, he underwent trabeculectomy with Ologen® implant under local anesthesia in his left eye. Postoperatively, at the end of one year, intraocular pressure (IOP) in his left eye was controlled without medication. This case highlights the management of secondary angle closure glaucoma in Axenfeld–Rieger syndrome with Ologen® implant.
Keywords: Axenfeld–Rieger syndrome, biodegradable implant, glaucoma, Ologen®, trabeculectomy
Introduction
Anterior segment dysgenesis is a group of rare autosomal dominant conditions including posterior embryotoxon, Axenfeld–Rieger syndrome (ARS), Peter's anomaly and aniridia.[1]
Ocular manifestations of ARS include iris stromal hypoplasia, ectropion uveae, corectopia, full-thickness iris defects, severe iris atrophy and extensive peripheral anterior synechiae. Glaucoma develops in 50% of cases, usually during early childhood or early adulthood, due to an associated angle anomaly or secondary synechial angle closure. Ologen® Collagen matrix (Aeon Astron Europe B.V., Leiden, The Netherlands) is a biodegradable, porcine, porous collagen implant developed to improve long-term results of trabeculectomy by reducing subconjunctival fibrosis but with reduced bleb-related complications.[2] A recent study comparing trabeculectomy with and without use of Ologen® implant found no difference in intraocular pressure (IOP) control between two groups.[3] In another pilot study found that success of trabeculectomy in eyes with MMC was similar to the eyes with Ologen® implant and complication rates were similar in the both the groups.[4] We report an unusual case of ARS with secondary glaucoma managed with Ologen® implant. To our knowledge, this is the first case report describing the use of Ologen® implant in the successful management of secondary glaucoma due to ARS.
Case Report
A 35-year-old male presented with complaints of decreased vision in both eyes of 22 years duration. He also gave history of deafness since 10 years of age for which he has been wearing a hearing aid for the past 6 years [Figure 1]. His best corrected visual acuity (BCVA) was no perception of light in right eye and 20/30 in left eye. Examination of both eyes which included a 4 mirror gonioscopy revealed presence of 360 degree iridocorneal adhesions, anteriorly displaced Schwalbe's line and presence of white cord like structures having adhesions to iris along its course traversing the anterior chamber in both eyes [Figures 2 and 3]. Intraocular pressure measured by Goldman applanation tonometry was 30 mmHg and 26 mmHg in right and left eye, respectively.
Figure 1.

Patient wearing a hearing aid for the past 6 years
Figure 2.
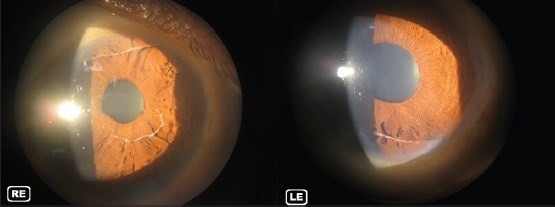
White cord like structure traversing the anterior chamber
Figure 3.
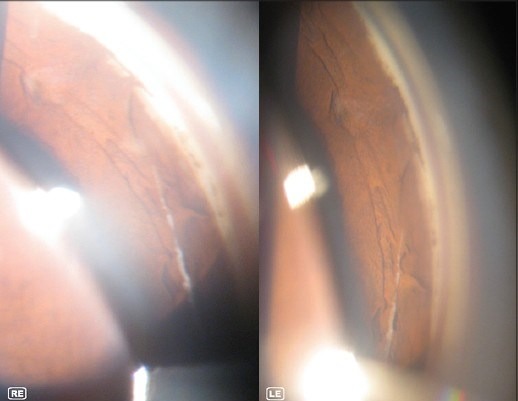
Gonioscopic photograph showing insertion of iris into trabecular meshwork, prominent iris processes, broad-based synechiae with prominent Schwalbe's line and white cord like structure in the angle
Fundus examination showed total glaucomatous optic atrophy in right eye with 0.9:1 cup disc ratio with bipolar notch in left eye [Figure 4]. Humphrey visual field analysis revealed superior and inferior arcuate scotoma in left eye.
Figure 4.

Fundus picture showing advanced glaucomatous optic atrophy in both eyes
ENT evaluation revealed bilateral sensorineural deafness. As the intraocular pressure was uncontrolled with topical 0.5% timolol maleate eye drops and 0.005% Latanoprost eye drops, patient underwent trabeculectomy with Ologen® implant under local anesthesia [Figure 5]. Postoperative regimen consisted of topical moxifloxacin eye drops four times a day for a week and prednisolone eye drops six times a day tapered over 6 weeks. Follow-up visits were arranged on first postoperative day, at 1 and 2 weeks and 1, 2, 3, 6 months and 1 year after surgery. At 3 months post-op, patient maintained a BCVA of 20/30 in left eye. When last seen one year post-op, the BCVA of 20/30 was maintained and intraocular pressure was 9 mmHg without any anti-glaucoma medication. There was a diffuse bleb with no changes observed in visual field in left eye [Figure 6].
Figure 5.
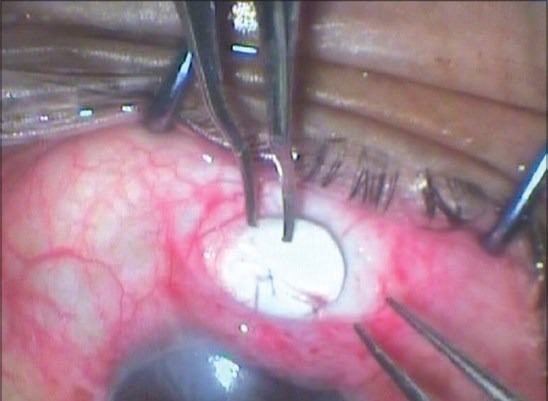
Ologen® implant being placed over the sclera flap
Figure 6.
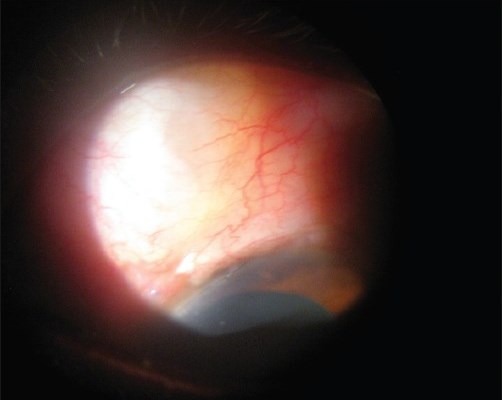
Post-operative picture showing diffuse bleb in left eye
Discussion
Corneal stroma, Schwalbe's line, trabecular meshwork and iris stroma develop from neural crest cells. Presence of detached Schwalbe's line with attached iris tissue could be attributed to the common origin of Schwalbe's line and iris tissue from neural crest cells.[5]
Espana et al. reported a case of a bilateral detached Schwalbe's line in the anterior chamber in a 37-year-old patient diagnosed with A-R syndrome.[6] Parikh R S et al. reported the presence of unique cord-like structure in the anterior chamber in the case of a 14-year-old patient presenting with megalocornea and Haab's striae in right eye and posterior embryotoxon in both eyes who underwent trabeculectomy with mitomycin-C in right eye. They felt that the presence of a thread or worm-like structure in the anterior chamber as was seen in our case could be considered a rare clinical sign in ARS with developmental glaucoma.[5] Medical management is instituted for developmental glaucoma with an onset in late childhood or early adulthood, aqueous suppressants being more effective than miotics. In congenital diseases, trabeculectomy is preferred over goniotomy in view of the technical difficulties that can be encountered due to the presence of iris adhesions.[7] Mandal et al. suggest that trabeculectomy augmented with mitomycin–C may be used in eyes that have failed angle surgery.[8] Laser procedures have not been found to be useful in the management of ARS-associated glaucoma except for relief of iatrogenic pupillary block or for cyclo-destruction in refractory cases.[7] A penetrating anti-glaucomatous surgical procedure allow good reduction of intraocular pressure and is probably better than non-penetrating surgery, especially in the long term.[9] Effective long-term intraocular pressure control following trabeculectomy is limited by filtration failure due to scarring at the level of conjunctiva-Tenon's-episcleral interface, the sclera flap, its overlying episclera or the internal ostium. Antiproliferative agents like 5-fluorouracil or mitomycin C are used in glaucoma filtration surgery to enhance filtration and improve long-term bleb function but produce complications including blebitis and endophthalmitis,[10] cataract, avascular filtering blebs, thinning of conjunctiva, hypotony, anterior chamber reaction and endothelial toxicity if mitomycin-C enters into the eye. They increase success rate of trabeculectomy by reducing scarring at the site of filtration.[11] The current focus is on the development of less toxic agents and implants to prevent cicatrization without producing adverse effects. A porous collagen-glycosaminoglycan matrix (Ologen®) biodegradable implant was found to decrease early postoperative scarring.[2] Studies have shown that the use of Ologen® implant produces comparable IOP reduction with trabeculectomy and a lower risk profile when compared with use of antimetabolites.[9] One pilot study however found that the use of Ologen® implant did not offer a significant advantage compared with trabeculectomy alone.[3] Patient has significant sensory deprivation as he is deaf in both his ears and has a non-functional eye. At 35 years of age and with advanced glaucomatous damage in his only seeing eye, his remaining good eye is his only window to the world and is especially valuable to him. Since use of mitomycin-C is associated with significant complications, it was felt that use of Ologen® is a better option. Option of use of antimetabolites with trabeculectomy remains. We did not detect any Ologen® specific side effects like translocation of implant, erosion of conjunctiva or allergy in our patient. We have started teaching the patient visual rehabilitation and use of low visual aids so as to prepare him for the future. Further studies are warranted to establish the future role of Ologen® implant in management of glaucoma in patients with Axenfeld-Rieger syndrome.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared.
References
- 1.Sowden JC. Molecular and developmental mechanisms of anterior segment dysgenesis. Eye (Lond) 2007;21:1310–8. doi: 10.1038/sj.eye.6702852. [DOI] [PubMed] [Google Scholar]
- 2.Chen HS, Ritch R, Krupin T, Hsu WC. Control of filtering bleb structure through tissue bioengineering: An animal model. Invest Ophthalmol Vis Sci. 2006;47:5310–4. doi: 10.1167/iovs.06-0378. [DOI] [PubMed] [Google Scholar]
- 3.Papaconstantinou D, Georgalas I, Karmiris E, Diagourtas A, Koutsandrea C, Ladas I, et al. Trabeculectomy with Ologen® versus trabeculectomy for the treatment of glaucoma: A pilot study. Acta Ophthalmol. 2010;88:80–5. doi: 10.1111/j.1755-3768.2009.01753.x. [DOI] [PubMed] [Google Scholar]
- 4.Senthil S, Rao HL, Babu JG, Mandal AK, Garudadri CS. Comparison of outcomes of trabeculectomy with mitomycin C vs. Ologen® implant in primary glaucoma. Indian J Ophthalmol. 2013;61:338–34. doi: 10.4103/0301-4738.109520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Parikh RS, Parikh SR, Debashish B, Harsha BL, Thomas R. Unusual presentation in Axenfeld- Reiger syndrome. Indian J Ophthalmol. 2011;59:312–14. doi: 10.4103/0301-4738.82003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Espana EM, Mora R, Liebmann J, Ritch R. Bilateral prominent Schwalbe ring in the anterior chamber in a patient with Axenfeld- Reiger Syndrome and megalocornea. Cornea. 2007;26:379–81. doi: 10.1097/ICO.0b013e31802f5033. [DOI] [PubMed] [Google Scholar]
- 7.Chang TC, Summers CG, Schimmenti LA, Grajewski AL. Axenfeld Rieger syndrome: New perspectives. Br J Ophthalmol. 2012;96:318–22. doi: 10.1136/bjophthalmol-2011-300801. [DOI] [PubMed] [Google Scholar]
- 8.Mandal AK, Prasad K, Naduvilath TJ. Surgical results and complications of mitomycin-C augmented trabeculectomy in refractory developmental glaucoma. Ophthalmic Surg Lasers. 1999;30:473–80. [PubMed] [Google Scholar]
- 9.Rosentreter, Schild AM, Jordan JF, Krieglstein GK, Dietlein TS. A prospective randomised trial of trabeculectomy using mitomycin C vs Ologen® implant in open angle glaucoma. Eye. 2010;24:1449–57. doi: 10.1038/eye.2010.106. [DOI] [PubMed] [Google Scholar]
- 10.Rai P, Kotecha A, Kaltos K, Ruddle JB, Murdoch IE, Bunce C, et al. Changing trends in incidence of bleb- related infection in trabeculectomy. Br J Ophthalmol. 2012;96:971–5. doi: 10.1136/bjophthalmol-2011-300926. [DOI] [PubMed] [Google Scholar]
- 11.Chaiam PJ, Arastvad K, Shaikh A, James B. Management of blebitis in the United Kingdom: A survey. Br J Ophthalmol. 2012;96:38–41. doi: 10.1136/bjo.2010.200402. [DOI] [PubMed] [Google Scholar]