

Abstract
Background:
While laser resurfacing remains the most effective treatment option for atrophic acne scars, the high incidence of post-treatment adverse effects limits its use. Fractional laser photothermolysis attempts to overcome these limitations of laser resurfacing by creating microscopic zones of injury to the dermis with skip areas in between.
Aim:
The aim of the present study is to assess the efficacy and safety of fractional CO2 laser resurfacing in atrophic facial acne scars.
Materials and Methods:
Sixty patients with moderate to severe atrophic facial acne scars were treated with 3-4 sessions of fractional CO2 laser resurfacing at 6-week intervals. The therapeutic response to treatment was assessed at each follow up visit and then finally 6 months after the last laser session using a quartile grading scale. Response to treatment was labelled as ‘excellent’ if there was >50% improvement in scar appearance and texture of skin on the grading scale while 25-50% response and <25% improvement were labelled as ‘good’ and ‘poor’ response, respectively. The overall satisfaction of the patients and any adverse reactions to the treatment were also noted.
Results:
Most of the patients showed a combination of different morphological types of acne scars. At the time of final assessment 6 months after the last laser session, an excellent response was observed in 26 patients (43.3%) while 15 (25%) and 19 patients (31.7%) demonstrated a good and poor response respectively. Rolling and superficial boxcar scars responded the best while pitted scars responded the least to fractional laser monotherapy. The commonest reported adverse effect was transient erythema and crusting lasting for an average of 3-4 and 4-6 days, respectively while three patients developed post-inflammatory pigmentation lasting for 8-12 weeks.
Conclusions:
Fractional laser resurfacing as monotherapy is effective in treating acne scars especially rolling and superficial boxcar scars with minimal adverse effects.
KEYWORDS: Acne scars, fractional CO2 laser resurfacing, fractional laser, scars, treatment
INTRODUCTION
Atrophic scars can result from any inflammatory skin disease causing sufficient damage to the epidermis and to the dermal collagen. The most common causes of atrophic scars especially on the face are severe nodular or nodulocystic acne, infections like varicella and Herpes simplex, trauma including burns and lastly, surgical procedures. Facial scars resulting from any of these etiologies are associated with psychological trauma and loss of self esteem.[1] Successful treatment of these scars can be a satisfying experience to the patient and the treating physician.
Facial scars resulting from acne are either hypertrophic or atrophic depending upon whether they are elevated or depressed in relation to the skin surface. The atrophic facial scars are divided into different morphological types depending on the shape and depth of the scars.[2,3] The four main morphological types of atrophic post acne scars are icepick pitted scars, superficial or deep boxcar scars, rolling scars and linear scars. Treatment of each morphological scar type varies and while one scar type responds the best to some treatment modality, the same treatment option may not be necessarily effective in other type of scars.[4]
Facial resurfacing with fractional lasers is currently claimed to be one of the most effective treatment options for facial scars.[5,6] Fractional lasers treat only a ‘fraction’ or a column of the affected skin leaving intervening areas of skin untreated. These untreated areas help in rapid re-epithelisation of the skin, minimising the chances of prolonged and serious adverse effects.[7] Fractional lasers are divided into either non-ablative or ablative fractional lasers. While the former are claimed to be the safer of the two types, the latter have been shown to be more effective in treating facial imperfections with better patient satisfaction.[8] Fractional CO2 laser resurfacing has been used in the treatment of atrophic scars with varying degrees of success.[9,10,11,12] Adverse effects in the form of persistent post-treatment erythema, crusting, post-inflammatory hyper pigmentation, purpura and even aggravation of scarring have been described as adverse reactions to this treatment option.[13,14]
For fractional laser resurfacing to be effective, the depth of penetration of the laser is a very crucial factor. And it is important to realise that the depth shows a non-linear correlation with the density and energy settings that are used with an individual laser.[15]
For the present study we used a fractional CO2 laser Qray-FRX from Dosis, Korea marketed by Coherent India Ltd. The machine has two separate hand-pieces for fractional CO2 laser and non-ablative radio-frequency with infrared non-ablative laser combination. For treating acne scars, only the Fractional CO2 hand-piece was used.
MATERIALS AND METHODS
Sixty patients of moderate to severe atrophic facial acne scars were treated with fractional CO2 laser resurfacing monotherapy over a period of three years from February 2010 to January 2013. Exclusion criteria included keloidal tendency, pregnancy, active acne, immunosuppression and concomitant isotretinoin use. Patients who were using any topical treatments for acne or for scars were told to stop these medications at least 1-week before the start of fractional laser treatment. No concomitant cosmetic procedures were allowed between the laser sessions and no topical drugs were prescribed except sunscreens and topical antibiotic creams in the post-procedure period.
After an informed consent was taken, a baseline photograph showing all the scars to be treated was taken using standard camera angle and light settings. Then, a topical anaesthetic cream containing a eutectic mixture of topical tetracaine and lignocaine in a cream base (TetralidR cream) was applied for 1 hour on the treatment area to achieve a satisfactory anaesthetic effect. After satisfactory anaesthesia was achieved, the treatment area was cleaned with a mild cleanser followed by 70% ethanol solution. Fractional CO2 laser treatment was then delivered to each atrophic scar present. Fluence ranging from 15-25 J/cm2 was used at densities of 100-150 MTZ/cm2, thus providing about 40-45mJ of energy and an ablation depth of 1.0-1.2 mm at each spot. A single or double pass was used over each scar along with its margins. Each morphological type of scar was treated in a similar manner and the patient was advised skin cooling with ice-packs for 5-10 minutes after the procedure to take care of post-treatment erythema, oedema and burning sensation.
The patients were instructed to prevent sun exposure for the next 4-5 days after each procedure and a topical non-occlusive antibiotic cream formulation was prescribed over this period. The patients were also encouraged to use a broad-spectrum sunscreen liberally in between the laser sessions. Oral acyclovir was prescribed only to those patients who had a history of recurrent Herpes simplex infections.
Laser procedure was repeated every 6 weeks and a total of 3-4 sessions were performed in each patient. The laser parameters were kept identical at each visit and if the patient was satisfied with the results obtained after the 3rd session, the 4th session was not performed. Digital photographs were taken using identical lighting, angle and face position settings at every follow up visit. The final assessment was made subjectively by a single observer at the last follow-up visit, 6 months after the last laser session and a quartile grading scale was used to assess the response objectively. A score of 0, 1, 2 and 3 was thus given if the response was <25%, 25-50%, 51-75% and >75%, respectively. The response was termed as excellent if the score was 2 or more and good if the score obtained was 1. Patients getting a score of <1 were termed as ‘poor’ responders. In addition to the photographic and clinical assessment, the patient's satisfaction to the treatment was also recorded at the final visit. Adverse effects, if any, were also monitored at each follow-up visit.
RESULTS
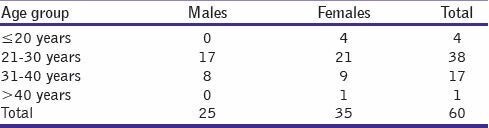
The demographic profile of the patients is given in Table 1. There were 25 males and 35 females in the study group and majority of them (38 patients) were in the 3rd decade of life. There were 3 patients with Fitzpatrick skin type 2, 39 patients with skin type 3 and 18 patients with skin type 4.
Table 1.
Demographic data of patients
All the cases had moderate to severe atrophic post-acne scars (Grade 3 and 4 scars by Goodman and Baron Classification system).[15] In majority of cases (35 out of 60), all the different morphological types of atrophic scars were present. The commonest sites involved were the cheeks followed by temples and forehead.
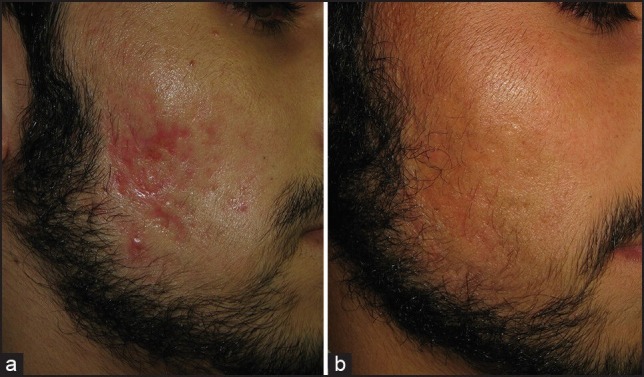
At the 6-month follow-up visit after the last laser session, a positive response with either good or excellent results was documented in 41 patients corresponding to 68.3% of the study group. Of these 41 responders, there were 11 patients (18.3%) in whom >75% improvement was seen in scars and skin texture [Figure 1] while in 15 others, the improvement was in the range of 51-75%. Thus, excellent response (score 2 or more on quartile grading scale) was observed in a total of 26 patients (43.3%). Fifteen patients (25%) showed a good response while 19 patients (31.7%) failed to demonstrate any significant response to treatment with <25% improvement on the quartile scale [Table 2].
Figure 1.
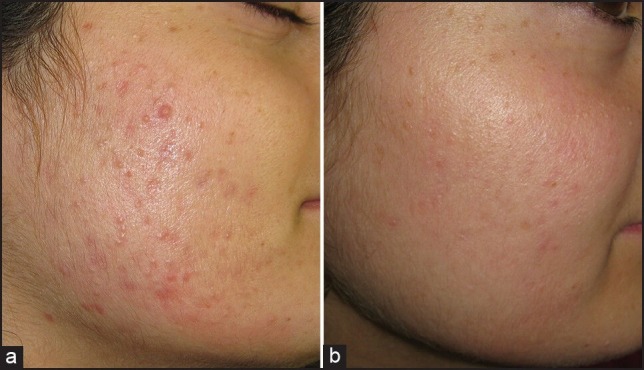
(a) Acne scars in early stage, (b) Excellent response, seen 6 months after the 4th laser session
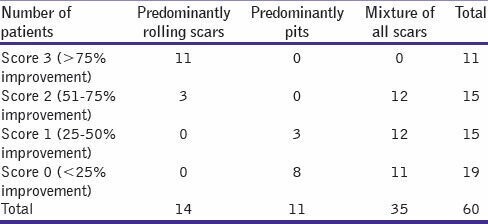
Table 2.
Response to treatment shown by different morphological types of scars
Patient satisfaction survey revealed that about 73% (44 cases out of the total of 60) were satisfied with the treatment results. For the remaining 16 cases, the improvement achieved was not up to their expectations.
In general, rolling scars were seen to respond the best to fractional laser resurfacing monotherapy [Figure 2] while icepick pitted scars responded the least. In fact, almost all of the rolling scars showed excellent response to treatment and all the 11 patients who showed >75% improvement in scars had predominantly rolling type of scars [Table 2]. On the other hand, patients who achieved the minimum improvement score had predominantly ice-pick scars or deep boxcar scars on their face [Figure 3].
Figure 2.
(a) Predominantly rolling scars (b) Excellent response after 3 sessions of fractional CO2 laser resurfacing
Figure 3.

(a) Predominantly boxcar scarring (b) Partial response to fractional laser resurfacing
Adverse effects to the treatment regimen were usually transient and included erythema that usually lasted for an average of 3-4 days, superficial crusting lasting for 4-6 days and mild transient edema. Transient acneiform lesions were seen in 6 patients and in 2 of these, oral treatment was necessitated. The only significant adverse effect observed was post-inflammatory hyperpigmentation that developed in 3 cases in our study. This pigmentation resolved with topical therapy over a period of 2-3 months.
DISCUSSION
It is always a challenge to treat a patient with moderate to severe acne scars. There are morphologically different types of scars and the individual depth of these scars also varies in between patients and even in a single patient. All these factors make the assessment of efficacy of any therapeutic option difficult to judge across all the patients.
Laser resurfacing with CO2 laser or Er:YAG laser gives excellent results when used in the treatment of aging skin and acne scars.[16,17] However, the risks associated with the procedure including the chances of prolonged erythema lasting for weeks to months, oozing and crusting and post-inflammatory pigmentation especially in darker skin limit the usefulness of this therapeutic option.[18] Fractional laser technology obviates many of these drawbacks as only a ‘fraction’ of the whole skin is treated and the integrity of epidermis is not compromised. As each microscopic wound created by the laser device is surrounded by normal, healthy tissue, the healing is rapid and the adverse effects are reduced to a considerable degree.
A number of clinical studies have documented a positive therapeutic effect of ablative fractional laser resurfacing with either Er:YAG or CO2 laser. Alster et al., in a study on 53 patients documented a clinical improvement in the range of 51-75% in about 90% of their patients with fractional erbium-doped fibre laser. No significant adverse effects or prolonged down-time after the procedure were seen.[9]
Fractional CO2 laser, with a wavelength of 10,600 nm, has also been employed in the treatment of acne scars in both Caucasian as well as Asian patients. Chapas et al., in their study on facial acne scars, documented improvement of 26-50% in texture and atrophy of the skin in all patients.[20] The investigators also used an imaging system (Primos) to analyse the change in the topography of scars. This imaging system also documented an objective improvement in the depth of individual scars ranging from 43% to 79.9% with a mean improvement of 66.8%. The adverse effects seen in the patients were again self-resolving and none of the enrolled patients developed any long-term or permanent adverse effects.[18]
In a single-blinded randomised study on acne scars, Hedelund et al. demonstrated statistically significant improvement in skin texture and atrophy in comparison with placebo after 3 monthly laser sessions with fractional CO2 device.[21] The study was conducted on 13 patients and the patients were also quoted as being ‘satisfied’ with the treatment option. Relatively higher energies in the range of 48-56mJ with a treatment density of 13% were used in this study.
In Asian patients, Sung Bin Cho and co-workers demonstrated the efficacy as well as safety of fractional CO2 laser resurfacing in acne scars.[22] Half of the 20 patients enrolled in this study achieved clinical improvement of >50% while another 7 patients achieved 26-50% improvement. The mean post-treatment erythema and crusting lasted for 2.8 ± 4.6 days and 6.3 ± 3.0 days, respectively.
In our study, we used energy in the range of 12-20J/cm2 and treatment density of 150-200 MTZ/cm2 in all patients. These treatment parameters were decided on the basis of the skin type of our patients as most of them had Fitzpatrick skin type 3 or 4. We treated all individual scars with the same laser fluence and treatment density irrespective of their depth or morphological type. Good to excellent response was achieved in about 67% patients on the quartile grading scale. This figure is in conformity with the figures quoted in most of the studies on CO2 fractional laser resurfacing in acne scars.[19,20,21,22,23] While about 40% patients achieved >50% improvement, additional 27% patients were seen to have 25-50% improvement in scar morphology and texture in the study group. Subjectively also, majority of the patients were satisfied with the results obtained after the end of treatment schedule.
Adverse effects seen were not significant and none of the enrolled patients had any long-term or permanent side effects from the procedure. However, there is certainly some down-time associated with fractional CO2 laser resurfacing as patients do experience crusting for a few days after the procedure. This crusting makes it impossible for patients to resume their normal work for a few days after each laser session. A nice way to circumvent this problem is to perform the procedure just before a weekend so that the patients get a rest of 2 days and no professional commitments are missed after the laser sessions. Additionally, post-inflammatory hyper pigmentation was observed in 3 patients in our series which resolved with topical treatments over a span of 6-12 weeks. This warrants the use of broad spectrum sunscreens and limitation of sun exposure after the laser sessions are performed.
Of all the scar types, rolling scars were seen to respond the best while icepick pitted scars responded the least to treatment in the study population. This observation carries a lot of therapeutic importance as simple fractional laser resurfacing monotherapy is unlikely to take care of pitted scars. Thus, if pits or ice-pick scars are the predominant scar type in any individual patient, the patient is unlikely to be satisfied with fractional laser resurfacing monotherapy alone. Such a patient would need either supplementary treatment with TCA CROSS (Chemical Reconstruction of scars by 80-100% Trichloracetic acid) technique or surgical techniques like punch excision or punch floatation if practically feasible.[24,25]
While commenting on the therapeutic results achieved with fractional laser resurfacing, it is important to realise that there is a lack of uniform objective assessment of the therapeutic benefit achieved. Majority of the clinical studies on fractional laser technology have used quartile grading systems or patient satisfaction as the criteria to assess the therapeutic results. Both of these criteria are fraught with subjective bias and there is an urgent need for a proper objective tool that can be used across the whole spectrum of post acne scars to assess any therapeutic benefit.[26]
Another important fact is that there are just a few studies that have commented upon the therapeutic results in different morphological types of acne scars.[27,28,29,30,31] All other studies have made a generalised or a sweeping statement on the results obtained without taking into account the differences in the response between the morphological scar types.
Lastly, it is important to realise that a typical patient has scars of different morphological types and grades and it is difficult to treat all these scar types satisfactorily with a single treatment option and multiple techniques are required. However, of all the treatment options available to treat post-acne scars, fractional photothermolysis is probably the only monotherapy that offers the highest degree of scar amelioration and patient satisfaction.
Footnotes
Source of Support: Nil.
Conflict of Interest: None declared.
REFERENCES
- 1.Layton AM. Psychosocial aspects of acne vulgaris. J Cutan Med Surg. 1998;2(Suppl 3):19–23. [PubMed] [Google Scholar]
- 2.Jacob CI, Dover JS, Kaminer MS. Acne scarring: A classification system and review of treatment options. J Am Acad Dermatol. 2001;45:109–17. doi: 10.1067/mjd.2001.113451. [DOI] [PubMed] [Google Scholar]
- 3.Goodman GJ. Postacne scarring: A review of its pathophysiology and treatment. Dermatol Surg. 2000;26:857–71. doi: 10.1046/j.1524-4725.2000.99232.x. [DOI] [PubMed] [Google Scholar]
- 4.Kadunc BV, Trindade de Almeida AR. Surgical treatment of facial acne scars based on morphologic classification: A Brazilian experience. Dermatol Surg. 2003;29:1200–9. doi: 10.1111/j.1524-4725.2003.29388.x. [DOI] [PubMed] [Google Scholar]
- 5.Geronemus RG. Fractional photothermolysis: Current and future applications. Lasers Surg Med. 2006;38:169–76. doi: 10.1002/lsm.20310. [DOI] [PubMed] [Google Scholar]
- 6.Rivera AE. Acne scarring: A review and current treatment modalities. J Am Acad Dermatol. 2008;59:659–76. doi: 10.1016/j.jaad.2008.05.029. [DOI] [PubMed] [Google Scholar]
- 7.Susan W, Brian ST, James C, Gregory A, Andrei E, Ilya Y, et al. Fractional photothermolysis: A novel aesthetic laser surgery modality. Dermatol Surg. 2007;33:525–34. doi: 10.1111/j.1524-4725.2007.33110.x. [DOI] [PubMed] [Google Scholar]
- 8.Cho SB, Lee SJ, Cho S, Oh SH, Chung WS, Kang JM, et al. Non-ablative 1550-nm erbium-glass and ablative 10 600-nm carbon dioxide fractional lasers for acne scars: A randomized split-face study with blinded response evaluation. J Eur Acad Dermatol Venereol. 2010;24:921–5. doi: 10.1111/j.1468-3083.2009.03551.x. [DOI] [PubMed] [Google Scholar]
- 9.Alster TS, Tanzi EL, Lazarus M. The use of fractional laser photothermolysis for the treatment of atrophic scars. Dermatol Surg. 2007;33:295–9. doi: 10.1111/j.1524-4725.2007.33059.x. [DOI] [PubMed] [Google Scholar]
- 10.Gold MH, Heath AD, Biron JA. Clinical evaluation of the SmartSkin fractional laser for the treatment of photodamage and acne scars. J Drugs Dermatol. 2009;8:s4–8. [PubMed] [Google Scholar]
- 11.Hu S, Chen MC, Lee MC, Yang LC, Keoprasom N. Fractional resurfacing for the treatment of atrophic facial acne scars in asian skin. Dermatol Surg. 2009;35:826–32. doi: 10.1111/j.1524-4725.2009.01139.x. [DOI] [PubMed] [Google Scholar]
- 12.Rahman Z, Tanner H, Jiang K. Treatment of atrophic scars with the 1550nm erbium-fiber fractional laser. Lasers Surg Med. 2006;38:24. [Google Scholar]
- 13.Campbell TM, Goldman MP. Adverse Events of Fractionated Carbon Dioxide Laser: Review of 373 Treatments. Dermatol Surg. 2010;36:1645–50. doi: 10.1111/j.1524-4725.2010.01712.x. [DOI] [PubMed] [Google Scholar]
- 14.Metelitsa AI, Alster TS. Fractionated laser skin resurfacing treatment complications: A review. Dermatol Surg. 2010;36:299–306. doi: 10.1111/j.1524-4725.2009.01434.x. [DOI] [PubMed] [Google Scholar]
- 15.Sardana K, Garg VK, Arora P, Khurana N. Histological validity and clinical evidence of use of fractional lasers for acne scars. J Cutan Aesthet Surg. 2012;5:75–90. doi: 10.4103/0974-2077.99431. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Alexiades-Armenakas MR, Dover JS, Arndt KA. The spectrum of laser skin resurfacing: Nonablative, fractional, and ablative laser resurfacing. J Am Acad Dermatol. 2008;58:719–37. doi: 10.1016/j.jaad.2008.01.003. [DOI] [PubMed] [Google Scholar]
- 17.Fitzpatrick RE, Goldman MP, Satur NM, Tope WD. Pulsed carbon dioxide laser resurfacing of photoaged facial skin. Arch Dermatol. 1996;132:395–402. [PubMed] [Google Scholar]
- 18.Nanni CA, Alster TS. Complications of carbon dioxide laser resurfacing. An evaluation of 500 patients. Dermatol Surg. 1998;24:315–20. doi: 10.1111/j.1524-4725.1998.tb04161.x. [DOI] [PubMed] [Google Scholar]
- 19.Chapas AM, Brightman L, Sukal S, Hale E, Daniel D, Bernstein LJ, et al. Successful treatment of acneiform scarring with CO 2 ablative fractional resurfacing. Lasers Surg Med. 2008;40:381–6. doi: 10.1002/lsm.20659. [DOI] [PubMed] [Google Scholar]
- 20.Hedelund L, Haak CS, Togsverd-Bo K, Bogh MK, Bjerring P, Haedersdal M. Fractional CO 2 laser resurfacing for atrophic acne scars: A randomized controlled trial with blinded response evaluation. Lasers Surg Med. 2012;44:447–52. doi: 10.1002/lsm.22048. [DOI] [PubMed] [Google Scholar]
- 21.Cho SB, Lee SJ, Kang JM, Kim YK, Chung WS, Oh SH. The efficacy and safety of 10,600-nm carbon dioxide fractional laser for acne scars in Asian patients. Dermatol Surg. 2009;35:1955–61. doi: 10.1111/j.1524-4725.2009.01316.x. [DOI] [PubMed] [Google Scholar]
- 22.Katz B. Efficacy of a new fractional CO 2 laser in the treatment of photodamage and acne scarring. Dermatol Ther. 2010;23:403–6. doi: 10.1111/j.1529-8019.2010.01340.x. [DOI] [PubMed] [Google Scholar]
- 23.Chan NP, Ho SG, Yeung CK, Shek SY, Chan HH. Fractional ablative carbon dioxide laser resurfacing for skin rejuvenation and acne scars in Asians. Lasers Surg Med. 2010;42:615–23. doi: 10.1002/lsm.20974. [DOI] [PubMed] [Google Scholar]
- 24.Bhardwaj D, Khunger N. An assessment of the efficacy and safety of CROSS Technique with 100% TCA in the management of ice pick acne scars. J Cutan Aesthet Surg. 2010;3:93–6. doi: 10.4103/0974-2077.69020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Goodman GJ. Treating scars: Addressing surface, volume and movement to expedite optimal results. Part 2: More severe grades of scarring. Dermatol Surg. 2012;38:1310–21. doi: 10.1111/j.1524-4725.2012.02439.x. [DOI] [PubMed] [Google Scholar]
- 26.Kang WH, Kim YJ, Pyo WS, Park SJ, Kim JH. Atrophic acne scar treatment using triple combination therapy: Dot peeling, subcision and fractional laser. J Cosmet Laser Ther. 2009;11:212–5. doi: 10.3109/14764170903134326. [DOI] [PubMed] [Google Scholar]
- 27.Weiss R, Weiss M, Beasley K. Long-term experience with fixed array 1540 Fractional erbium laser for acne scars. Abstract presented at American Society for Laser Medicine and Surgery Conference; April 2008; Kissimmee, FL. [Google Scholar]
- 28.Sardana K, Manjhi M, Garg VK, Sagar V. Which type of atrophic acne scar (ice-pick, boxcar or rolling) responds to nonablative fractional laser therapy? Dermatol Surg. 2014;40:288–300. doi: 10.1111/dsu.12428. [DOI] [PubMed] [Google Scholar]
- 29.Lee HS, Lee JH, Ahn GY, Lee DH, Shin JW, Kim DH, et al. Fractional photothermolysis for the treatment of acne scars: A report of 27 Korean patients. J Dermatolog Treat. 2008;19:45–9. doi: 10.1080/09546630701691244. [DOI] [PubMed] [Google Scholar]
- 30.Hedelund L, Moreau KE, Beyer DM, Nymann P, Haedersdal M. Fractional nonablative 1,540-nm laser resurfacing of atrophic acne scars. A randomized controlled trial with blinded response evaluation. Lasers Med Sci. 2010;25:749–54. doi: 10.1007/s10103-010-0801-1. [DOI] [PubMed] [Google Scholar]
- 31.Mahmoud BH, Srivastava D, Janiga JJ, Yang JJ, Lim HW, Ozog DM. Safety and efficacy of erbium-doped yttrium aluminum garnet fractionated laser for treatment of acne scars in type IV to VI skin. Dermatol Surg. 2010;36:602–9. doi: 10.1111/j.1524-4725.2010.01513.x. [DOI] [PubMed] [Google Scholar]