

Abstract
Objectives
The present study examined the quality of obturation in root canals obturated by GuttaCore, a gutta-percha-based core-carrier system with a cross-linked thermoset gutta-percha carrier, by comparing the incidence of gaps and voids identified from similar canals obturated by cold lateral compaction or warm vertical compaction.
Methods
Thirty single-rooted premolars with oval-shaped canals were shaped and cleaned, and obturated with one of the three obturation techniques (N=10): GuttaCore, warm vertical compaction or cold lateral compaction. Filled canals were scanned with micro-computed tomography (micro-CT); reconstructed images were analysed for the volumetric percentage of gaps and voids at 3 canal levels (0-4 mm, 4-8 mm and 8-12 mm from working length). The roots were subsequently sectioned at the 4-mm, 8-mm and 12-mm levels for analyses of the percentage of interfacial gaps, and area percentage of interfacial and intracanal voids, using scanning electron microscopy (SEM) to examine negative replicas of root sections. Data were analysed with parametric or non-parametric statistical methods at α=0.05.
Results
Both micro-CT and SEM data indicated that canals obturated with GuttaCore core-carriers had the lowest incidence of interfacial gaps and voids, although the results were not significantly different from canals obturated by warm vertical compaction. Both the GuttaCore and the warm vertical compaction groups, in turn, had significantly lower incidences of gaps and voids than the cold lateral compaction group.
Conclusions
Because of the similarity in obturation quality between GuttaCore and warm vertical compaction, practitioners may find the GuttaCore core-carrier technique a valuable alternative for obturation of oval-shaped canals.
Keywords: cold lateral compaction, core-carrier, cross-linked thermoset gutta-percha carrier, micro-computed tomography, negative replica, scanning electron microscopy, warm vertical compaction
Introduction
Success in root canal treatment was founded upon the triad of thorough canal débridement, effective disinfection and obturation of the canal space.1 Although contemporary research indicates that shaping and cleaning are strategically more significant than obturation of the canal space for eliminating root canal infections,2 a significant share of this triad has historically been allocated to obturation of the canal space.3 Three-dimensional obturation of the canal space to the working length4 has been depicted as the most critical component of root canal treatment for sealing and isolating the canal space from irritants that remain after shaping and cleaning, and for eliminating leakage from the periradicular tissues or oral cavity into the filled canal space.5,6 Results from these early studies are supported by recent outcome studies that highlight the contribution of root filling quality to the success of primary and secondary root canal treatment.7-10 It is undeniable that a high quality coronal seal is important for endodontic success;11 apical periodontitis has been shown to heal in teeth with unfilled canals following meticulous shaping and cleaning, and placement of a coronal seal.12 However, insisting that healing reliably occurs in the presence of a defective root filling is to have created a very shortsighted view on the important roles played by root canal obturation in preserving the environment created by shaping and cleaning and preventing microbial reinfection of the canal space,13,14 both of which are essential for maintenance of long-term periradicular health.15
Interfacial gaps and voids present in filled root canals are clinically relevant because as low as 1% shrinkage of root canal sealers can result in gaps that are large enough for penetration of bacteria and their noxious products.16,17 Different methods have been utilised for examination of interfacial gaps and sealer penetration within filled root canals, including destructive and nondestructive methods. Destructive methods involve sectioning of the filled root canals and examination by light microscopy, confocal laser scanning electron microscopy or scanning electron microscopy (SEM). Although light microscopy and laser confocal scanning microscopy are useful for examining the extent of sealer penetration into dentinal tubules and the percentage of gutta-percha-filled areas, sealer-filled areas and large voids,18-20 these morphological evaluation techniques lacked the resolution to quantify thin interfacial gaps between the root filling and intraradicular dentine. Scanning electron microscopy of sectioned slabs of root-filled canals has also been used to evaluate the penetration of root canal sealers into dentinal tubules. These SEM techniques offer a number of advantages. Images produced using SEM permit observation of the interfacial quality at higher resolution. The main disadvantage of SEM is the potential for producing artefacts during specimen preparation; dehydration of the specimens during laboratory processing and examination in a high vacuum environment create artefactual interfacial gaps. This renders evaluation of the interfacial quality of the root canal fillings futile using conventional scanning electron microscopes. However, this limitation may be overcome by examining polyvinylsiloxane impressions (i.e. negative replicas) of the root fillings directly,21 or positive epoxy resin replicas prepared indirectly from those impressions.22 Micro-computed tomography (micro-CT) is a non-destructive three-dimensional (3-D) imaging technique that has been adopted in endodontics for analysing the interfacial quality of root fillings.23-29 Because micro-CT imaging is non-invasive, specimens remain intact during examination and may be subsequently sectioned and examined by SEM for confirmation of the image reconstruction results. An enormous amount of information may be generated from scans; planar slices may be recreated in any plane and data may be represented as two-dimensional (2-D) or 3-D images and evaluated qualitatively or quantitatively.
The most common techniques employed for root canal obturation include cold lateral compaction, warm vertical compaction and core-carrier techniques.30 Coating metal carriers such as gold wire, silver points and endodontic files with heat-softened gutta-percha for three-dimensional obturation of the canal space31-34 has long existed before the commercialisation of different prefabricated alpha-phase gutta-percha-based or polycaprolactone-based core-carrier systems. These core-carrier systems are claimed to enhance adaptation of the gutta-percha to the canal wall, and flow of the filling material into lateral canals. Due to the difficulties encountered in retreatment and in the preparation of post spaces, the original metal carriers were subsequently replaced by plastic obturators.35,36 Recently, a new core-carrier system was introduced (GuttaCore, Dentsply Tulsa Dental Specialties, Tulsa, OK, USA) in which the Vectra (a liquid crystal polymer) or polysulphone plastic carriers in Thermafil Plus (Dentsply Tulsa Dental Specialties) were replaced by cross-linked thermoset gutta-percha, which enables the carrier (obturator) to be removed more easily during retreatment. The cross-linked thermoset gutta-percha does not melt by heat used in an obturator oven, and is insoluble in common organic solvents employed for root canal retreatment.37 Removal of this modified obturator during retreatment may be achieved by mechanical trephining through the carrier.38
Although the core-carrier obturation technique has been regarded by some as the only genuine warm gutta-percha technique for adaptation to the apical third of the canal space,39,40 the quality of root canal obturation achieved by the new core-carrier system that incorporates cross-linked thermoset gutta-percha carriers has not been reported. Thus, the objective of the present in vitro study was to examine the quality of obturation in single-rooted canals obturated by the GuttaCore core-carrier system by comparing the results with similar canals obturated by the cold lateral compaction technique or the warm vertical compaction technique, using non-destructive (micro-CT) and destructive (SEM) methods of investigation. The null hypothesis tested was that there are no differences in the percentage of interfacial gaps and voids in single-rooted canals obturated by the GuttaCore core-carrier technique, gutta-percha cold lateral compaction technique and gutta-percha warm vertical compaction technique using the same root canal sealer.
Materials and Methods
Root canal obturation
Thirty intact, caries-free human single-rooted premolars with oval-shaped canals were obtained with patient informed consent under a protocol approved by the Human Assurance Committee of the Georgia Regents University. The teeth were stored in 0.9% NaCl solution containing 0.02% sodium azide at 4 °C until use. Each tooth was radiographed in the mesiodistal direction to ensure that it contained a single oval-shaped canal. After preparation of the access cavity, each tooth was further examined under an operating microscope to confirm the presence of a single oval-shaped canal. For each tooth, canal patency was achieved using a size 10 stainless steel K-file. Working length was established at 1 mm short of the anatomical apex. Canal shaping was performed with 0.02 taper K-files and 0.04 taper Vortex Blue nickel-titanium rotary instruments (Dentsply Tulsa Dental Specialties), using a crown down technique until a size 40 apical seat was established. Final shaping was achieved using a 0.06 taper, size 40 Vortex Blue nickel-titanium rotary instrument. To ensure optimal cutting efficacy, a new set of rotary instruments was used for the shaping of each root canal.
After shaping, the apex of each root was sealed with sticky wax to simulate a closed canal system. Each instrumented canal was irrigated with 5.25% sodium hypochlorite (NaOCl) solution during preparation. One milliliter of NaOCl was used between successive files. After completion of canal instrumentation, the canal was irrigated with 5 mL of 0.5 M of QMix® 2in1 (Dentsply Tulsa Dental Specialties) and 5 mL NaOCl to remove the inorganic and organic components of the smear layer, respectively. The solutions were delivered using 30-gauge side-vented irrigation syringes to 1 mm short of the working length. The canal was dried with paper points. After shaping and cleaning, the 30 teeth were randomly divided into 3 groups (N = 10) for filling of the instrumented canal spaces, using one of the three obturation techniques:
Core-carrier technique
Each canal was obturated with a size 40, 0.06 taper GuttaCore Obturator and ThermaSeal Plus sealer (Dentsply Tulsa Dental Specialties), using the directions specified by the manufacturer. Briefly, the shape of the canal space at working length and passive fit of the obturator were verified using a size verifier that reached the apical constriction passively without significant resistance or twisting. A GuttaCore Obturator was heated in the obturator oven while the canal was coated with the root canal sealer. The heated GuttaCore Obturator was slowly inserted to working length without twisting or forcing. The shaft and handle of the obturator was removed at the cementoenamel junction using a round bur in a high-speed handpiece under copious water spray.
Warm vertical compaction technique
Each canal was fitted with a size 40, 0.06 taper gutta-percha cone that was used to apply the ThermaSeal Plus sealer to the canal walls. The gutta-percha was down-packed to 5 mm from the working length with a heated plugger (Calamus Dual, Dentsply Tulsa Dental Specialties), and backfilled with warmed, cartridge-dispensed gutta-percha (Calamus Dual) to the cementoenamel junction.
Cold lateral compaction technique
Each canal was initially filled with a size 40, 0.06 taper gutta-percha cone as the master obturation cone and ThermaSeal Plus sealer. The master gutta-percha cone was coated with sealer, inserted to working length, and laterally compacted with a finger spreader for insertion of accessory gutta-percha points until no more points could be inserted. The master cone and accessory gutta-percha points were then seared off at the cementoenamel junction with a heated instrument.
The access cavity of each tooth was filled with a temporary dressing after obturation of the canal space. The teeth were stored in sterile distilled water at 37 °C and 100% relative humidity to ensure complete setting of the root canal sealer. Each tooth was then marked with pencil at 4 mm, 8 mm and 12 mm coronal to the working length of the root (i.e. at 5 mm, 9 mm and 13 mm from the anatomical apex), to delineate the 3 canal levels to be examined. Each tooth was placed in a separate scintillation vial containing deionised water.
Micro-CT scanning and image reconstruction
A SkyScan 1174 (Micro Photonics Inc., Allentown, PA, USA) compact X-ray micro-CT scanner was used to scan the teeth. Each tooth was stabilised in foam, covered with a moist tissue to prevent dehydration, and positioned with the longitudinal axis of the root perpendicular to the specimen stage. Every tooth was scanned with the same parameters, using a 0.5 mm thick aluminum filter to remove low energy radiation derived from the polychromatic X-ray source to reduce image noise. Each tooth was scanned from the anatomical apex to 12 mm above the root tip (as indicated by the pencil line), using a spatial resolution of 14.52 mm at 50 kV and 800 μA. Scanning was performed with a rotational angle of 360° around the longitudinal axis of the root, using a 0.9° rotation step and 4000 msec exposure time. A 40% beam hardening correction and a ring artefact reduction value of 10 were employed to reduce ring artefacts during the reconstruction phase with the Skyscan NRecon software.
Following image reconstruction, 2-D virtual sections of the inner structures of the root canal space were acquired in the coronal, axial and sagittal planes using the Skyscan CT-analyser (CTAn) software. Thresholding or segmentation of the grey scale levels was performed to produce binary images for discrimination of the gaps and voids from the sealer, gutta-percha and hard tooth structures. Two-dimensional distribution of interfacial gaps and voids from the working length to the 12-mm level of each root was initially examined by plotting the percentage distribution of the area of gaps and voids within the canal space of each axial slice as a function of distance from the working length (i.e. 0-mm level). The CTAn software was further employed for 3-D analysis and quantification of the volume of interfacial gaps and voids within the volume of interest (VOI). Interfacial gaps and voids were presented as a percentage of the total canal volume from the working length to the coronal 12 mm of the root canal. The Skyscan CT-Volume (CTVol) software was used for 3-D visualisations of the obturated canal within the root and for preparing movies.
The volumetric percentages of interfacial gaps and voids in canals filled by the three obturation techniques were statistically analysed for the entire VOI (i.e. 0-12 mm of the filled canal space), at the 8-12 mm canal level, at the 4-8 mm canal level, and at the 0-4 mm canal level. As the normality and equal variance assumptions of the data set and subsets appeared to be violated, the VOI dataset and the 3 canal levels data subsets were logarithmically transformed to render the data parametric, prior to analysis using separate one-factor analysis of variances. For each of the 4 analyses, post-hoc multiple comparisons were performed with the Tukey-Kramer statistic. Statistical significance were preset at α = 0.05 for all analyses.
SEM evaluation
Because micro-CT scanning could not distinguish interfacial gaps from voids, SEM was used to examine these features at a higher resolution. After completion of the non-destructive part of the evaluation, each tooth was sectioned at 4, 8 and 12 mm from the working length using a 0.3 mm thick diamond blade (Isomet, Buehler Ltd., Lake Bluff, IL, USA) at slow speed with water-cooling. The cuts were made perpendicular to the longitudinal axis of the root. Each surface to be examined was polished with 1200-grit silicon carbide paper under constant water-cooling until a relatively smooth surface was achieved. This surface was treated with a 3 min application of 0.5 M ethylenediamine tetra-acetic acid to remove the smear layer created by cutting and polishing and to bring the surface into relief. The polished surface was rinsed with deionised water. An ultralow viscosity polyvinylsiloxane impression material (Aquasil Ultra XLV Regular Set, Dentsply DeTrey, Konstanz, Germany) was used for taking an impression of the smear layer-depleted surface. After dispensing the mixed impression material onto the specimen surface, a gentle air stream was used to displace the impression material into potential gaps and voids along the sealer-dentine interface and within the sealer-filling material. This was followed by the placement of a thicker layer of impression material to produce a negative impression of the specimen surface.
Each negative replica was mounted on an aluminum stub, sputter-coated with gold/palladium and examined using a field emission-SEM (XL-30 FEG; Philips, Eindhoven, The Netherlands) operating at 10 kV. With the use of a negative replica, the root filling-radicular dentine interface along an axial section of a filled root canal appears as a closed loop with a well-defined, traceable circumference. Interfacial gaps appear as elevated ridges or flaps of impression material. An intracanal void appears as a raised knob of impression material above the surface of the gutta-percha or sealer, while an interfacial void appears as a raised knob of impression material with one part of the knob touching the canal circumference. The percentage of interfacial gap at each canal level was measured for each specimen and expressed as a percentage of the canal circumference at that level. In the event that an interfacial void was encountered, the part of the interfacial void that was in contact with the canal circumference was treated as part of the interfacial gap and measured accordingly. Areas derived from intracanal and interfacial voids of a single negative replica were summated and expressed as a percentage of root canal area at the respective canal level.
Since only three sectioned surfaces were examined for each tooth, data from the three canal levels were pooled together (N = 30) for statistical analysis of the effect of obturation techniques on the manifestation of interfacial gaps or voids, with each parameter analysed separately. Because the dataset from either parameter was not normally distributed even after data transformation, each dataset was analysed with Kruskal-Wallis analysis of variance and Dunn's multiple comparison test. Statistical significance were preset at α = 0.05 for all analyses.
Results
Figure 1 shows the coronal, axial and sagittal aspects a root canal filling reconstructed from micro-CT scan. The different components of the root filling, voids and root dentine could be discerned because of their different grey scale levels. Because voids and interfacial gaps were highly radiolucent and appeared dark grey to black, generation of binary images was not difficult for 2-D and 3-D measurement of their percentage distribution. A schematic of how reconstructed axial root sections were used to produce a 2-D plot of the percentage distribution of voids and gaps along the entire region of interest (0-12 mm from working length of a filled canal) is shown in Figure 2A. Representative examples of the distribution of interfacial voids in root canals filled by the GuttaCore core-carrier technique, the warm vertical compaction technique and the cold lateral compaction technique are shown in Figures 2B, 2C and 2D, respectively. None of the obturation techniques produced completely gap- and void–free root fillings, although gaps and voids were not universally present in every 2-D axial section, especially for the core-carrier and the warm vertical compaction techniques.
Figure 1.
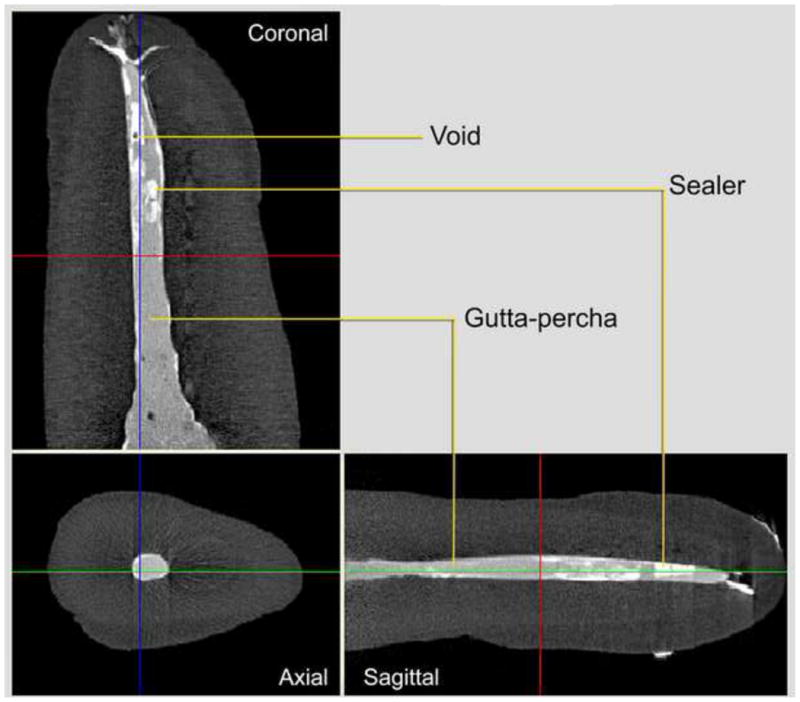
Micro-CT scan of a single-rooted upper premolar after root canal filling with gutta-percha and an epoxy resin-based sealer, using one of the three obturation techniques described in the text. Two-dimensional reconstructed views of the root canal filling are shown from the coronal, axial and sagittal aspects. The root and different components of the root filling can be identified with different grey scale levels (dark grey for root dentine and cementum, light grey for gutta-percha, dark, white for the highly radiopaque sealer). Voids are highly radiolucent and appear black.
Figure 2.
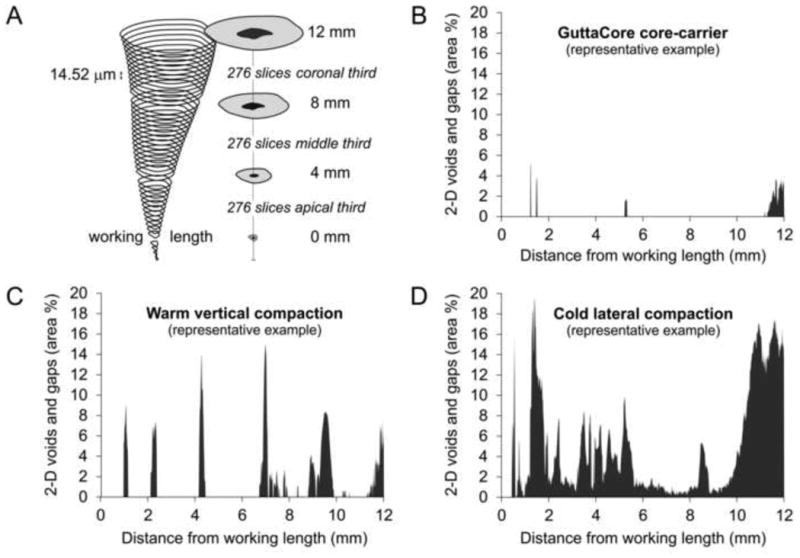
A. Schematic illustrating the use of axial sections for analyzing the variation in percentage area distribution of gaps and voids along the longitudinal axis of an obturated canal space. At a spatial resolution of 14.52 μm, 276 axial slices were obtained for each of the three canal levels, commencing from the working length (0-4 mm level, 4-8 mm level and 8-12 mm level). Representative examples are shown for the percentage distribution of 2-D gaps and voids in roots obturated using the B. GuttaCore core-carrier technique; C. warm vertical compaction technique; and D. cold lateral compaction technique.
Representative examples of 3-D visualisations of root canals that were obturated using the GuttaCore core-carrier technique, the warm vertical compaction technique and the cold lateral compaction technique are shown in Figures 3A, 3B and 3C, respectively. Movies prepared from these representative examples may be found in Supplementary Material. Because it not possible to discern interfacial gaps from voids in volume-rendered reconstructions, these features were collectively reported and analysed quantitatively. Figure 4A shows the volumetric percentages of gaps and voids present in the VOI (0-12 mm level) of canals obturated by the three techniques. The volumetric distribution of gaps and voids along the three canal levels are shown in Figures 4B (8-12 mm level), 4C (4-8 mm level) and 4D (0-4 mm level). For the VOI and for each canal level, one-factor ANOVA indicated significant differences in the volumetric percentages of gaps and voids among the three obturation techniques (p < 0.001 for VOI; p = 0.01 for the 8-12 mm level; p = 0.007 for the 4-8 mm level; p = 0.004 for the 0-4 mm level). Post-hoc multiple comparisons indicated that there were no statistically significant differences in the volumetric distribution of gaps and voids between the cold lateral compaction and the warm vertical compaction techniques, and between the warm vertical compaction and the GuttaCore core-carrier techniques. However, significantly higher percentages of gaps and voids were found in root canals obturated with the cold lateral technique, when compared with the GuttaCore core-carrier technique (p < 0.05 for VOI and all canal levels).
Figure 3.
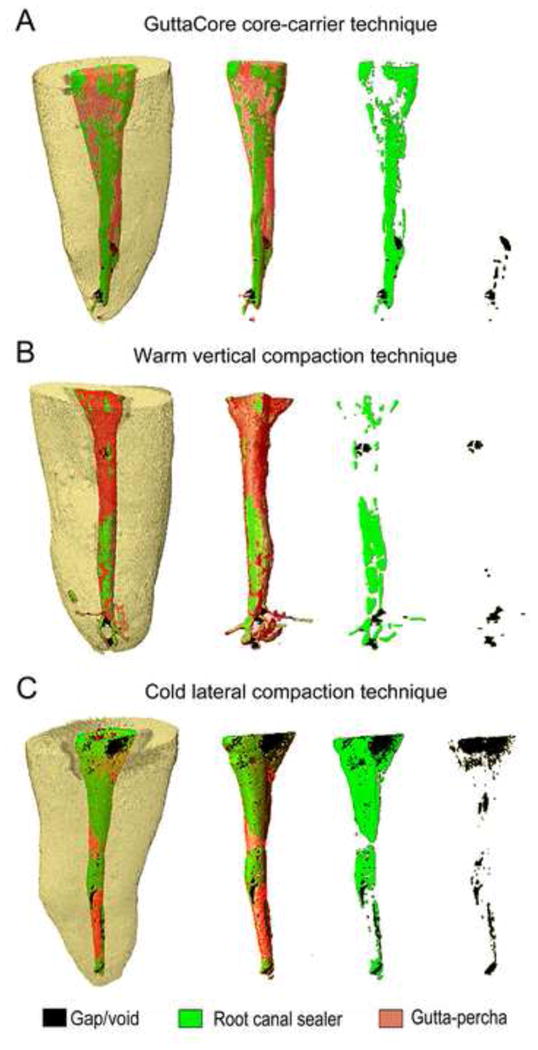
Examples of three-dimensional visualisations of root canals that were obturated using the A. GuttaCore core-carrier technique; B. warm vertical compaction technique; and C. cold lateral compaction technique. Based on grey scale thresholds, virtual-coloured images were generated showing the different components of the root filling and interfacial gaps and voids within the root (far left), without the root dentine (left), without the root dentine and gutta-percha (right), and depiction of the interfacial gaps and voids alone (far right).
Figure 4.
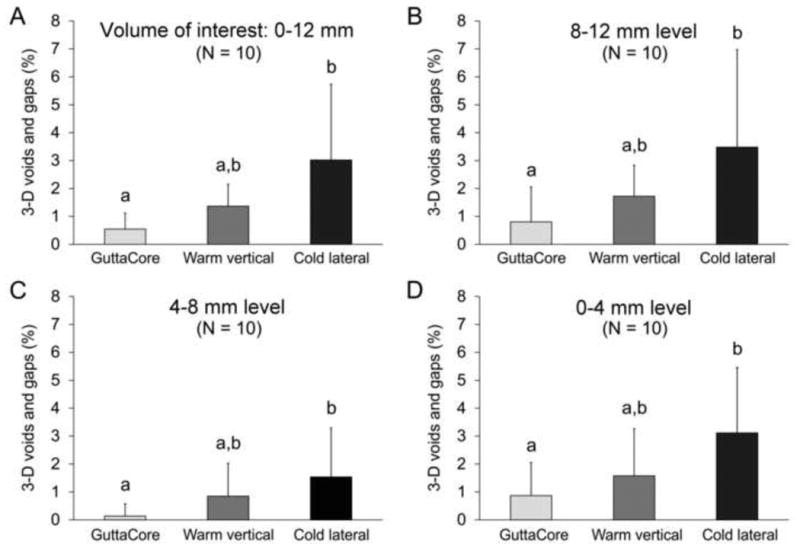
Volumetric percentages of 3-D gaps and voids present in root canals that were filled using the three obturation techniques within A. the entire VOI (i.e. from working length (0 mm) to 12 mm coronal to the working length); B. at the 8-12 mm level; C. at the 4-8 mm level; D. at the 0-4 mm level. Each column represents the means and standard deviation of data collected from the respective group. For each chart, columns identified with the same lower case letter are not significantly different (p>0.05).
Scanning electron microscopy enabled interfacial gaps to be discerned from interfacial voids and intracanal voids. Figure 5A is a SEM image of a gap- and void-free obturated canal surface. Figure 5B is an example of an interfacial gap that was identified as a protruded flap of impression material along the sealer-dentine interface. Figure 5C is an example of a specimen containing an interfacial gap that was continuous with an interfacial void. Figure 5D is an example of a specimen containing both intracanal voids and an interfacial void.
Figure 5.
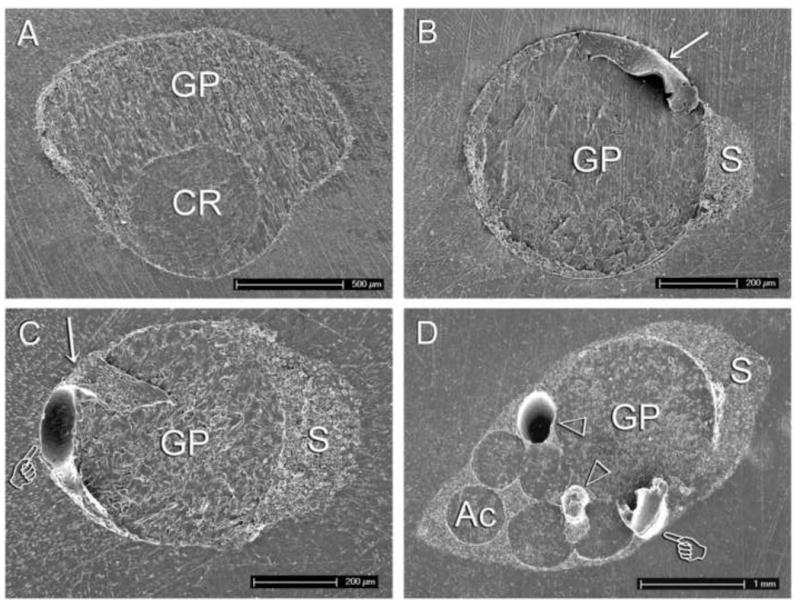
Examples of scanning electron microscopy images of polyvinylsiloxane (PVS) negative replicas of sectioned root surfaces. A. A gap- and void-free surface taken from the 8-mm level of a root canal obturated with the GuttaCore core-carrier technique. CR: cross-linked gutta-percha carrier; GP: thermoplasticised gutta-percha core. B. An axial surface taken from the 4-mm level of a root canal obturated with the warm vertical compaction technique. Interfacial gap may be identified as a flap of PVA material extruding from the specimen surface (arrow). GP: gutta-percha cone; S: root canal sealer. C. An axial surface taken from the 8-mm level of a canal obturated by warm vertical compaction, showing an interfacial gap (arrow) that is continuous with an interfacial void (pointer). The latter is presented as a knob of PVS material extruding from the specimen surface. D. An axial surface taken from the 12-mm level of a canal obturated by cold lateral compaction, showing an interfacial void (pointer) and two intracanal voids (open arrowheads). Ac: accessory gutta-percha cone.
The number of interfacial gap-free specimens found at the three sectioned levels (4-mm, 8-mm and 12-mm) of root canals filled by the three obturation techniques is graphically presented in Figure 6A. From the modified box and whisker plot of specimens pooled from the 3 canal levels (Figure 6C, left), significant difference in the percentage canal circumference occupied by interfacial gaps could be seen among the three groups ( p < 0.001); the percentage of interfacial gaps in the cold lateral compaction technique was significantly higher than the GuttaCore core-carrier technique (p < 0.05).
Figure 6.
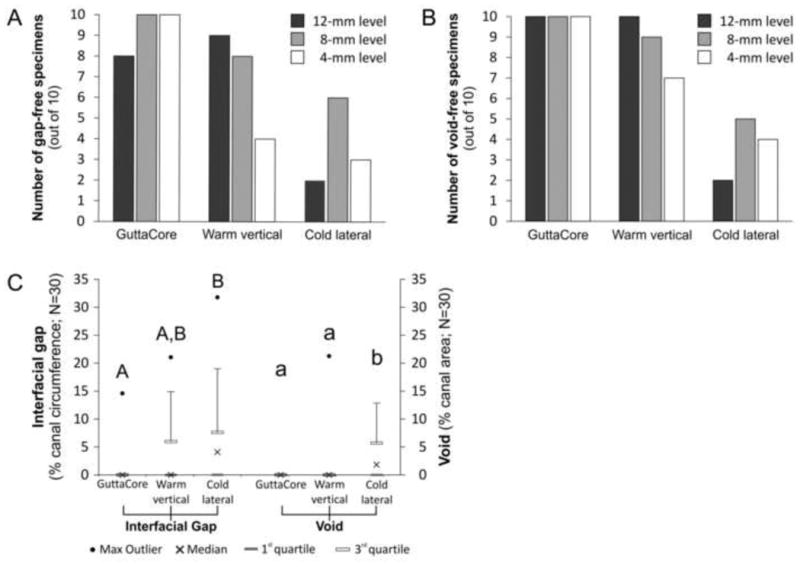
A. Number of gap-free specimens at the 12-mm, 8-mm and 4-mm root levels (measured from the working length), in canals that were filled by the three obturation techniques. B. Number of void-free specimens at the 12-mm, 8-mm and 4-mm root levels in canals that were filled by the three obturation techniques. C. Modified box and whisker plots of the distribution of interfacial gaps (as a percentage of canal circumference) and voids (as a percentage of canal area) in root canals that were filled by the three obturation techniques. For each technique, data from the 3 canal levels were pooled together for statistical analysis. For interfacial gap (left), columns identified by the same upper case letter are not significantly different (p>0.05). For void (right), columns identified by the same lower case letter are not significantly different (p>0.05).
The number of void-free specimens found at the three sectioned levels of root canals filled by the three obturation techniques is graphically presented in Figure 6B. From the modified box and whisker plot of specimens pooled from the 3 canal levels (Figure 6C, right), significant difference in the percentage canal area occupied by voids could be seen among the three groups (p < 0.001); the percentage of voids identified from root canals obturated with the cold lateral compaction technique was significantly higher than root canals obturated by the warm vertical compaction technique (p < 0.05) or the GuttaCore core-carrier technique (p < 0.05).
Discussion
Under the conditions of the present study, the volumetric percentages of specimens exhibiting combined gaps and voids in a filled canal volume of interest (VOI) along 0-12 mm of the canal length, as determined by micro-CT analysis, were significantly different among the three obturation techniques. Likewise, both the circumferential percentages of interfacial gaps, and the area percentages of interfacial and intracanal voids, as determined by SEM at specific canal levels of 4 mm, 8 mm and 12 mm, were also significantly different in root canals filled by the three obturation techniques. These results warrant rejection of the null hypothesis that there are no differences in the percentage of interfacial gaps and voids in single-rooted canals obturated by the GuttaCore core-carrier technique, gutta-percha cold lateral compaction technique and gutta-percha warm vertical compaction technique using the same root canal sealer.
The reproducibility and accuracy in using micro-CT for analysing root canal fillings have been well demonstrated in previous studies.23-29,41 This non-destructive technique provides rapid imaging of the gaps and voids present in the filled canal space and produces impressive 3-D visualisation of the orientation and continuity of these deficiencies within the filled canal VOI. Nevertheless, micro-CT axial sections lack the resolution, when compared with SEM, in discerning interfacial gaps from interfacial and intracanal voids. Thus, both non-destructive and destructive methods of investigations were used to provide complementary information in the present study. A polyvinylsiloxane negative replica technique was adopted in lieu of epoxy resin positive replicas as the former technique eliminated bubble artefacts generated on the epoxy resin surface by the release of hydrogen gas from polymerised polyvinylsiloxane impressions, even when platinum or palladium was incorporated in the impression material to absorb the released gas.42 Formation of gas bubbles on the epoxy resin surface interfered with identification of gaps and voids on the specimen surface. Scanning electron microscopy of polished sections has limitations in that only a small number of sections could be examined using this labour-intensive technique. Thus, data derived from SEM examination of interfacial gaps and voids are only representative of sectioned canal levels examined. In spite of this limitation, analyses of data derived from SEM examination of interfacial gaps (circumference) and voids (area) at specific canal levels generated results that are confirmative of those derived from analysis of volume-rendered micro-CT scans.
In general, the high variance of the data acquired is an indirect indicator of the unpredictability of commonly used obturation techniques in perfectly adapting to the canal walls and root filling materials. For the cold lateral compaction technique, the incidence of combined volume of gaps and voids identified at all canal levels was not significantly different from that seen in the warm vertical compaction technique. A similar conclusion was reached when stereomicroscopy was used to examine voids present in central incisors that were obturated with cold lateral compaction or continuous wave warm vertical compaction.43 When interfacial gaps and voids were analysed separately with SEM in the present work, no significant difference in the circumferential percentage of interfacial gaps was observed between the cold lateral and warm vertical compaction techniques, while there was a significant higher area percentage of voids in oval-shaped canals obturated by the cold lateral compaction technique. Recent studies on the quality of obturation achieved by these two techniques in oval-shaped canals of premolars reported that warm vertical compaction produced a significantly greater volume of gutta-percha in the canal space than cold lateral compaction.41,44 One of these studies also identified a significantly higher volumetric percentage of voids in oval-shaped canals obturated with the cold lateral compaction technique.41 These voids may represent spaces left behind by the spreader during lateral compaction of the accessory gutta-percha cones, shrinkage of the root canal sealer, or the result of the inability of the spreader to dispense the sealer into canal fins when conventional, non-canal wall adaptive nickel titanium rotary instruments were used to prepare oval-shaped canals. Although there was a higher incidence of voids associated with cold lateral compaction in the aforementioned micro-CT study,41 difference between the two compaction techniques was not statistically significant at the apical root level. Clinical outcome studies remain the gold standard for evaluating the performance of root filling materials and techniques. A quantitative systematic review analysed the long-term clinical outcomes from 10 clinical studies involving the use of the cold lateral and warm vertical compaction techniques.45 The similar obturation quality achieved by cold lateral and warm vertical compaction techniques supports the conclusion derived from the meta-analysis of those 10 clinical studies, in that there wa no difference in treatment outcomes between the two obturation techniques.45 Although a subsequent retrospective clinical study revealed a tendency of better healing in teeth that were obturated using warm vertical compaction,8 the authors of that study opined that additional randomised control trials were required to validate the finding in primary root canal treatment of teeth with preoperative apical periodontitis.
When cold lateral compaction and the GuttaCore core-carrier technique were compared, both non-destructive and destructive methods of investigations identified significant lower percentages of interfacial gaps and voids in canals that were obturated with GuttaCore core-carriers. GuttaCore represents the latest generation of carrier-based root canal filling material that uses thermoplasticised gutta-percha as the core material. Studies on the previous generation of this class of carrier-based obturators, ThermaFil Plus, yielded favourable results in terms of their adaptation to canal walls, although void-free fillings in oval-shaped canals were not consistently achieved.46 Earlier studies by Wolcott et al.47 and Clinton and Van Himel48 reported that the ThermaFil core-carrier technique allowed thermoplastic gutta-percha to flow better into lateral canals, had fewer voids, and replicated the root surface better. More recent studies reported that canals obturated with core-carrier techniques had the highest gutta-percha content within the filled canal space.49,50 Reduction of sealer content may help reduce the amount of leachable sealer-derived cytotoxic products from filled root canals into the periapex.51 Although the ability of core-carrier techniques to enhance the flow of thermoplasticised gutta-percha into lateral canals has been impressively demonstrated with the use of micro-CT, the belief that lateral canals and apical ramifications must be injected with filling material to enhance treatment outcome was challenged in a recent study by Ricucci and Siqueira.52 In that study, the authors demonstrated histologically that lateral canals in necrotic teeth that were shown to be optimally filled radiographically were actually not well-obturated; gutta-percha and sealer were simply compacted against incompletely-removed inflamed necrotic tissues and biofilms.
Although in vitro studies on core-carrier techniques with plastic carriers generally reported significantly less voids in the filled canal space when compared with those obturated with cold lateral compaction, such a difference was not reflected by improvements in treatment outcome in clinical studies. Results from two retrospective studies came to the same consensus that there was no significant difference in the success rate achieved when the core-carrier technique or the cold lateral compaction technique was employed for primary root canal treatment.53,54 An important issue to consider, however, is that the teeth involved in those two clinical studies were not stratified into those with or without preoperative apical periodontitis. As the rate of treatment success associated with teeth without preoperative periodontitis is high (circa 90%),7,8 this could have masked the beneficial effect of the core-carrier technique on healing of teeth with preoperative apical periodontitis. Moreover, the contribution of thorough chemomechanical débridement cannot be overstated in clinical outcome studies. As the fluid dynamics of chemomechanical debridement within the root canal system is becoming better understood,55 it is of clinical relevance to compare the treatment outcomes for root canal treatment of teeth with preoperative apical periodontitis only, using contemporary state-of-the-art irrigants and irrigant delivery technology for chemomechanical débridement, prior to obturating these canals with the cold lateral compaction technique or the GuttaCore core-carrier technique.
Both non-destructive and destructive methods of investigations identified no significant difference in the percentage of interfacial gaps and voids in canals that were obturated by warm vertical compaction or GuttaCore core-carriers. These results obtained from the new GuttaCore system are consistent with those reported for the earlier TheramFil version.36,56 It is noteworthy from the SEM findings at the 4-mm sectioned canal level, that specimens obturated with GuttaCore core-carriers were completely gap-free and void-free, while specimens obturated with the warm vertical compaction technique were only 40% gap-free (Figure 6A) and 70% void-free (Figure 6B). Understandably, when the warm vertical compaction technique was used for down packing a gutta-percha cone to approximately 5 mm from the working length, the apical third of the canal was essentially filled by a single-cone technique.
Conclusion
Similar to many of the in vitro studies that examined the incidence of gaps and voids in filled root canals, gap- and void-free root canal fillings could not be predictably and consistently identified from any of the three groups examined in the present study. Nevertheless, root canals obturated with GuttaCore core-carriers exhibited the lowest incidence of interfacial gaps and voids among the three groups, although the results were not statistically significant from those canals obturated by warm vertical compaction. Both the GuttaCore group and the warm vertical compaction group, in turn, had significantly lower incidences of gaps and voids than the cold lateral compaction group. Because of the similarity in obturation quality between the GuttaCore core-carrier group and the warm vertical compaction group, practitioners may find the GuttaCore core-carrier technique a valuable alternative to the use of warm vertical compaction for filling oval-shaped canals; the warm vertical technique may be perceived by some clinicians as more technique sensitive and more difficult to master compared with the cold lateral compaction technique. Because the carrier in GuttaCore is composed of cross-linked thermoset gutta-percha, retreatment is comparatively easier than the previous ThermaFil Plus core-carrier system. This may be achieved by trephining through the GuttaCore carrier to enable files to re-negotiate to working length. It is pertinent to point out that the conclusion reached in the present study is based solely on the incidence of interfacial gaps and voids identified in root canals obturated with the three techniques. Further studies on issues such as the propensity of sealer extrusion with the use of GuttaCore core-carriers, and the potential of stripping of the thermoplasticised gutta-percha core from the cross-linked thermoset gutta-percha carrier should provide valuable information for clinicians to make an evidence-based decision in the selection of a root canal obturation technique.
Supplementary Material
Acknowledgments
The authors reported no conflicts of interest in this work. The GuttaCore system employed in the present study was graciously sponsored by Dentsply Tulsa Dental Specialties. This work was supported by grants R01 DE015306-06 from the National Institute of Dental & Craniofacial Research (PI: David H Pashley) and grant 81130078 from National Nature Science Foundation of China (PI: Ji-hua Chen). The authors thank Mrs. Michelle Barnes and Mrs. Marie Churchville for their secretarial support.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.Schilder H. Vertical compaction of warm gutta-percha. In: Gerstein H, editor. Techniques in Clinical Endodontics. Philadelphia, PA: WB Saunders; 1983. pp. 76–98. [Google Scholar]
- 2.Haapasalo M, Endal U, Zandi H, Coil JM. Eradication of endodontic infection by instrumentation and irrigation solutions. Endodontic Topics. 2005;10:77–102. [Google Scholar]
- 3.Gutmann JL. Clinical, radiographic, and histologic perspectives on success and failure in endodontics. Dental Clinics of North America. 1992;36:379–92. [PubMed] [Google Scholar]
- 4.Schilder H. Filling root canals in three dimensions. Dental Clinics of North America. 1967;11:723–44. [PubMed] [Google Scholar]
- 5.Ingle JI, Beveridge EE, Glick DH, Weichman JA. Endodontic success & failure: the Washington Study Chapter 1: Modern Endodontic Therapy. In: Ingle JL, Bakland LK, editors. Endodontics. 4th. Baltimore, MD: Williams & Wilkins; 1994. pp. 21–45. [Google Scholar]
- 6.Sjögren U, Hägglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. Journal of Endodontics. 1990;16:498–504. doi: 10.1016/S0099-2399(07)80180-4. [DOI] [PubMed] [Google Scholar]
- 7.Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature - Part 2. Influence of clinical factors International Endodontic Journal. 2008;41:6–31. doi: 10.1111/j.1365-2591.2007.01323.x. [DOI] [PubMed] [Google Scholar]
- 8.de Chevigny C, Dao TT, Basrani BR, Marquis V, Farzaneh M, Abitbol S, et al. Treatment outcome in endodontics: the Toronto study - phase 4: initial treatment. Journal of Endodontics. 2008;34:258–63. doi: 10.1016/j.joen.2007.10.017. [DOI] [PubMed] [Google Scholar]
- 9.de Chevigny C, Dao TT, Basrani BR, Marquis V, Farzaneh M, Abitbol S, et al. Treatment outcome in endodontics: the Toronto study - phases 3 and 4: orthograde retreatment. Journal of Endodontics. 2008;34:131–7. doi: 10.1016/j.joen.2007.11.003. [DOI] [PubMed] [Google Scholar]
- 10.Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: part 1: periapical health. International Endodontic Journal. 2011;44:583–609. doi: 10.1111/j.1365-2591.2011.01872.x. [DOI] [PubMed] [Google Scholar]
- 11.Gillen BM, Looney SW, Gu LS, Loushine BA, Weller RN, Loushine RJ, et al. Impact of the quality of coronal restoration versus the quality of root canal fillings on success of root canal treatment: a systematic review and meta-analysis. Journal of Endodontics. 2011;37:895–902. doi: 10.1016/j.joen.2011.04.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Sabeti MA, Nekofar M, Motahhary P, Ghandi M, Simon JH. Healing of apical periodontitis after endodontic treatment with and without obturation in dogs. Journal of Endodontics. 2006;32:628–33. doi: 10.1016/j.joen.2005.12.014. [DOI] [PubMed] [Google Scholar]
- 13.Bergenholtz G, Spångberg L. Controversies in endodontics. Critical Reviews in Oral Biology and Medicine. 2004;15:99–114. doi: 10.1177/154411130401500204. [DOI] [PubMed] [Google Scholar]
- 14.Ricucci D, Lin LM, Spångberg LS. Wound healing of apical tissues after root canal therapy: a long-term clinical, radiographic, and histopathologic observation study. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology & Endodontics. 2009;108:609–21. doi: 10.1016/j.tripleo.2009.05.028. [DOI] [PubMed] [Google Scholar]
- 15.Li GH, Niu LN, Zhang W, Olsen M, De-Deus G, Eid AA, et al. Ability of new obturation materials to improve the seal of the root canal system: A review. Acta Biomaterialia. 2014;10:1050–63. doi: 10.1016/j.actbio.2013.11.015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Ørstavik D, Nordahl I, Tibballs JE. Dimensional change following setting of root canal sealer materials. Dent Materials. 2001;17:512–9. doi: 10.1016/s0109-5641(01)00011-2. [DOI] [PubMed] [Google Scholar]
- 17.Weis MV, Parashos P, Messer HH. Effect of obturation technique on sealer cement thickness and dentinal tubule penetration. International Endodontic Journal. 2004;37:653–63. doi: 10.1111/j.1365-2591.2004.00839.x. [DOI] [PubMed] [Google Scholar]
- 18.Gharib SR, Tordik PA, Imamura GM, Baginski TA, Goodell GG. A confocal laser scanning microscope investigation of the epiphany obturation system. Journal of Endodontics. 2007;33:957–61. doi: 10.1016/j.joen.2007.03.011. [DOI] [PubMed] [Google Scholar]
- 19.Schäfer E, Köster M, Bürklein S. Percentage of gutta-percha-filled areas in canals instrumented with nickel-titanium systems and obturated with matching single cones. Journal of Endodontics. 2013;39:924–8. doi: 10.1016/j.joen.2013.04.001. [DOI] [PubMed] [Google Scholar]
- 20.Kokkas A, Boutsioukis A, Vassiliadis L, Stavrianos CK. The influence of the smear layer on dentinal tubule penetration depth by three different root canal sealers: an in vitro study. Journal of Endodontics. 2004;30:100–2. doi: 10.1097/00004770-200402000-00009. [DOI] [PubMed] [Google Scholar]
- 21.Gwinnett AJ, Kanca J., 3rd Micromorphological relationship between resin and dentin in vivo and in vitro. American Journal of Dentistry. 1992;5:19–23. [PubMed] [Google Scholar]
- 22.Gondim E, Zaia AA, Gomes BP, Ferraz CC, Teixeira FB, Souza-Filho FJ. Investigation of the marginal adaptation of root-end filling materials in root-end cavities prepared with ultrasonic tips. International Endodontic Journal. 2003;36:491–9. doi: 10.1046/j.1365-2591.2003.00679.x. [DOI] [PubMed] [Google Scholar]
- 23.Rhodes JS, Ford TR, Lynch JA, Liepins PJ, Curtis RV. Micro-computed tomography: a new tool for experimental endodontology. International Endodontic Journal. 1999;32:165–70. doi: 10.1046/j.1365-2591.1999.00204.x. [DOI] [PubMed] [Google Scholar]
- 24.Jung M, Lommel D, Klimek J. The imaging of root canal obturation using micro-CT. International Endodontic Journal. 2005;38:617–26. doi: 10.1111/j.1365-2591.2005.00990.x. [DOI] [PubMed] [Google Scholar]
- 25.Metzger Z, Zary R, Cohen R, Teperovich E, Paqué F. The quality of root canal preparation and root canal obturation in canals treated with rotary versus self-adjusting files: a three-dimensional micro-computed tomographic study. Journal of Endodontics. 2010;36:1569–73. doi: 10.1016/j.joen.2010.06.003. [DOI] [PubMed] [Google Scholar]
- 26.Zaslansky P, Fratzl P, Rack A, Wu MK, Wesselink PR, Shemesh H. Identification of root filling interfaces by microscopy and tomography methods. International Endodontic Journal. 2011;44:395–401. doi: 10.1111/j.1365-2591.2010.01830.x. [DOI] [PubMed] [Google Scholar]
- 27.El-Ma'aita AM, Qualtrough AJ, Watts DC. A micro-computed tomography evaluation of mineral trioxide aggregate root canal fillings. Journal of Endodontics. 2012;38:670–2. doi: 10.1016/j.joen.2012.01.009. [DOI] [PubMed] [Google Scholar]
- 28.Gandolfi MG, Parrilli AP, Fini M, Prati C, Dummer PM. 3D micro-CT analysis of the interface voids associated with Thermafil root fillings used with AH Plus or a flowable MTA sealer. International Endodontic Journal. 2013;46:253–63. doi: 10.1111/j.1365-2591.2012.02124.x. [DOI] [PubMed] [Google Scholar]
- 29.Moeller L, Wenzel A, Wegge-Larsen AM, Ding M, Kirkevang LL. Quality of root fillings performed with two root filling techniques. An in vitro study using micro-CT. Acta Odontologica Scandinavica. 2013;71:689–96. doi: 10.3109/00016357.2012.715192. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Whitworth J. Methods of filling root canals: principles and practices. Endodontic Topics. 2005;12:2–24. [Google Scholar]
- 31.Perry SG. Preparing and filling the roots of teeth. Dent Cosmos. 1883;25:185–94. [Google Scholar]
- 32.Welch SE. Gutta percha coated silver cones as root canal filling material. Illinois Dental Journal. 1978;47:604–10. [PubMed] [Google Scholar]
- 33.Negm MM. Filling root canals with silver percha cones: a clinical study. Oral Surgery Oral Medicine Oral Pathology. 1983;55:81–5. doi: 10.1016/0030-4220(83)90311-0. [DOI] [PubMed] [Google Scholar]
- 34.Johnson WB. A new gutta-percha technique. Journal of Endodontics. 1978;4:184–8. doi: 10.1016/S0099-2399(78)80173-3. [DOI] [PubMed] [Google Scholar]
- 35.Gutmann JL, Saunders WP, Saunders EM, Nguyen L. An assessment of the plastic Thermafil obturation technique. Part 2. Material adaptation and sealability. International Endodontic Journal. 1993;26:179–83. doi: 10.1111/j.1365-2591.1993.tb00790.x. [DOI] [PubMed] [Google Scholar]
- 36.Kytridou V, Gutmann JL, Nunn MH. Adaptation and sealability of two contemporary obturation techniques in the absence of the dentinal smear layer. International Endodontic Journal. 1999;32:464–74. doi: 10.1046/j.1365-2591.1999.00248.x. [DOI] [PubMed] [Google Scholar]
- 37.Gutmann JL. The future of root canal obturation. Dentistry Today. 2011;30:128, 130–1. [PubMed] [Google Scholar]
- 38.Beasley RT, Williamson AE, Justman BC, Qian F. Time required to remove GuttaCore, Thermafil Plus, and thermoplasticized gutta-percha from moderately curved root canals with ProTaper files. Journal of Endodontics. 2013;39:125–8. doi: 10.1016/j.joen.2012.10.014. [DOI] [PubMed] [Google Scholar]
- 39.Zogheib C, Naaman A, Sigurdsson A, Medioni E, Bourbouze G, Arbab-Chirani R. Comparative micro-computed tomographic evaluation of two carrier-based obturation systems. Clinical Oral Investigations. 2013;17:1879–83. doi: 10.1007/s00784-012-0875-1. [DOI] [PubMed] [Google Scholar]
- 40.Alkahtani A, Al-Subait S, Anil S. An in vitro comparative study of the adaptation and sealing ability of two carrier-based root canal obturators. The Scientific World Journal. 2013;2013:532023. doi: 10.1155/2013/532023. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Keleş A, Alcin H, Kamalak A, Versiani MA. 3D Micro-CT evaluation of root filling quality in oval-shaped canals. Clinical Oral Investigations. 2013 doi: 10.1111/iej.12269. [DOI] [PubMed] [Google Scholar]
- 42.McCrosson J, Sharkey SW, Smith GM, Anderson RA. Quantification of hydrogen gas released from polyvinylsiloxane impression materials in contact with die stone materials. Journal of Dentistry. 1987;15:129–32. doi: 10.1016/0300-5712(87)90069-8. [DOI] [PubMed] [Google Scholar]
- 43.Keçeci AD, Unal GC, Sen BH. Comparison of cold lateral compaction and continuous wave of obturation techniques following manual or rotary instrumentation. International Endodontic Journal. 2005;38:381–8. doi: 10.1111/j.1365-2591.2005.00954.x. [DOI] [PubMed] [Google Scholar]
- 44.Wu MK, Kast'áková A, Wesselink PR. Quality of cold and warm gutta-percha fillings in oval canals in mandibular premolars. International Endodontic Journal. 2001;34:485–91. doi: 10.1046/j.1365-2591.2001.00463.x. [DOI] [PubMed] [Google Scholar]
- 45.Peng L, Ye L, Tan H, Zhou X. Outcome of root canal obturation by warm gutta-percha versus cold lateral condensation: a meta-analysis. Journal of Endodontics. 2007;33:106–9. doi: 10.1016/j.joen.2006.09.010. [DOI] [PubMed] [Google Scholar]
- 46.De-Deus G, Reis C, Beznos D, de Abranches AM, Coutinho-Filho T, Paciornik S. Limited ability of three commonly used thermoplasticized gutta-percha techniques in filling oval-shaped canals. Journal of Endodontics. 2008;34:1401–5. doi: 10.1016/j.joen.2008.08.015. [DOI] [PubMed] [Google Scholar]
- 47.Wolcott J, Himel VT, Powell W, Penney J. Effect of two obturation techniques on the filling of lateral canals and the main canal. Journal of Endodontics. 1997;23:632–5. doi: 10.1016/S0099-2399(97)80176-8. [DOI] [PubMed] [Google Scholar]
- 48.Clinton K, Van Himel T. Comparison of a warm gutta-percha obturation technique and lateral condensation. Journal of Endodontics. 2001;27:692–5. doi: 10.1097/00004770-200111000-00010. [DOI] [PubMed] [Google Scholar]
- 49.Gençoğlu N. Comparison of 6 different gutta-percha techniques (part II): Thermafil, JS Quick-Fill, Soft Core, Microseal, System B, and lateral condensation. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontics. 2003;96:91–5. doi: 10.1016/s1079-2104(02)91704-x. [DOI] [PubMed] [Google Scholar]
- 50.De-Deus G, Gurgel-Filho ED, Magalhães KM, Coutinho-Filho T. A laboratory analysis of gutta-percha-filled area obtained using Thermafil, System B and lateral condensation. International Endodontic Journal. 2006;39:378–83. doi: 10.1111/j.1365-2591.2006.01082.x. [DOI] [PubMed] [Google Scholar]
- 51.Gulsahi K, Cehreli ZC, Kuraner T, Dagli FT. Sealer area associated with cold lateral condensation of gutta-percha and warm coated carrier filling systems in canals prepared with various rotary NiTi systems. International Endodontic Journal. 2007;40:275–81. doi: 10.1111/j.1365-2591.2006.01213.x. [DOI] [PubMed] [Google Scholar]
- 52.Ricucci D, Siqueira JF., Jr Fate of the tissue in lateral canals and apical ramifications in response to pathologic conditions and treatment procedures. Journal of Endodontics. 2010;36:1–15. doi: 10.1016/j.joen.2009.09.038. [DOI] [PubMed] [Google Scholar]
- 53.Chu CH, Lo EC, Cheung GS. Outcome of root canal treatment using Thermafil and cold lateral condensation filling techniques. International Endodontic Journal. 2005;38:179–85. doi: 10.1111/j.1365-2591.2004.00929.x. [DOI] [PubMed] [Google Scholar]
- 54.Hale R, Gatti R, Glickman GN, Opperman LA. Comparative analysis of carrier-based obturation and lateral compaction: a retrospective clinical outcomes study. International Journal of Dentistry. 2012;2012:954675. doi: 10.1155/2012/954675. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Gulabivala K, Ng YL, Gilbertson M, Eames I. The fluid mechanics of root canal irrigation. Physiological Measurement. 2010;31:R49–R84. doi: 10.1088/0967-3334/31/12/R01. [DOI] [PubMed] [Google Scholar]
- 56.Marciano MA, Ordinola-Zapata R, Cunha TV, Duarte MA, Cavenago BC, Garcia RB, et al. Analysis of four gutta-percha techniques used to fill mesial root canals of mandibular molars. International Endodontic Journal. 2011;44:321–9. doi: 10.1111/j.1365-2591.2010.01832.x. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.