

Abstract
Purpose
To quantify the effectiveness of anti-VEGF antibodies (bevacizumab and B20-4.1.1) as mitigators of radiation-induced, CNS (brain) necrosis in a mouse model.
Experimental Design
Cohorts of mice were irradiated with single-fraction 50- or 60-Gy doses of radiation targeted to the left hemisphere (brain) using the Leksell Perfexion Gamma Knife. The onset and progression of radiation necrosis were monitored longitudinally by in vivo, small-animal MRI, beginning four weeks post-irradiation. MRI-derived necrotic volumes for antibody (Ab)-treated and untreated mice were compared. MRI results were supported by correlative histology.
Results
Hematoxylin and eosin stained sections of brains from irradiated, non-Ab-treated mice confirmed profound tissue damage, including regions of fibrinoid vascular necrosis, vascular telangiectasia, hemorrhage, loss of neurons, and edema. Treatment with the murine anti-VEGF antibody B20-4.1.1 mitigated radiation-induced changes in an extraordinary, highly statistically-significant manner. The development of radiation necrosis in mice under treatment with bevacizumab (a humanized anti-VEGF antibody) was intermediate between that for B20-4.1.1-treated and non-Ab-treated animals. MRI findings were validated by histologic assessment, which confirmed that anti-VEGF-antibody treatment dramatically reduced late-onset necrosis in irradiated brain.
Conclusions
The single-hemispheric-irradiation mouse model, with longitudinal MRI monitoring, provides a powerful platform for studying the onset and progression of radiation necrosis and for developing and testing new therapies. The observation that anti-VEGF antibodies are effective mitigants of necrosis in our mouse model will enable a wide variety of studies aimed at dose optimization and timing and mechanism of action with direct relevance to ongoing clinical trials of bevacizumab as a treatment for radiation necrosis.
Introduction
Radiation is a key component in the treatment of both benign and malignant central nervous system tumors, including gliomas, metastases, meningiomas, schwanomas, pituitary adenomas, and other less common neoplasms. Multiple radiation-treatment schemes have been developed to treat various neoplasms in the brain. These treatment protocols utilize a variety of different fractionation and conformational schemes designed to deliver focused radiation to regions in the brain to maximize control of tumor growth and minimize deleterious effects on normal brain tissue. Outcomes of these clinical protocols may be complicated by radiation effects on non-neoplastic tissue, resulting in a spectrum of phenotypes, ranging from minimal change with no observable clinical symptoms, to delayed radiation necrosis with severe neurological sequelae. The delayed effects from radiation may produce cerebral edema and necrosis of normal brain parenchyma, resulting in untoward neurologic effects that are difficult to differentiate from recurrent tumor growth.
Radiation necrosis, a delayed radiation neurotoxicity that can occur after radiation treatment of the CNS, can develop between 3 months and 10 years after radiotherapy, with most cases occurring in the first two years (1). Necrosis following radiation is not uncommon, occurring in 3-24% of patients receiving focal irradiation (1). The incidence may be threefold higher with concurrent chemotherapy (2, 3). Currently, only limited options for therapeutic intervention are available for patients with symptomatic radiation necrosis. Surgical resection of necrotic tissue is often not possible due to the location of the necrosis in eloquent regions of the brain. Prolonged treatment with corticosteroids is often employed (4), but is complicated by cushingoid side-effects, including weight gain, myopathy, immunosuppression, psychiatric disturbances, and occasionally arthritic sequelae, such as avascular necrosis affecting the shoulders and hips (5). Hyperbaric oxygen treatment has also been considered as a therapeutic modality (6, 7). However, it is cumbersome to deliver, expensive, and available in few medical centers. Its benefit has only been shown in a relatively small number of cases (8).
Two models of the pathogenesis of radiation necrosis have been proposed. These models involve radiation-induced injury to vasculature, radiation-induced injury to glial cells (apoptosis), or a combination thereof (9). In particular, radiation necrosis has been associated with breakdown of the blood brain barrier, leading to increased vascular permeability and elevated levels of vascular endothelial growth factor (VEGF) (1, 10). Elevated VEGF levels can, in turn, damage vascular endothelial cells and, together with subsequent narrowing of vessels due to fibrosis, can result in edema and necrosis (11).
Bevacizumab, a humanized monoclonal antibody against VEGF, was first approved by the FDA in 2004 for use in treating metastatic colorectal cancer. Since then, it has also been approved for the treatment of non-small-cell lung cancer, metastatic breast cancer, and recurrent glioblastoma (12). Bevacizumab has been reported to normalize the vasculature, thereby enhancing the efficient delivery of drugs (13, 14). There is emerging clinical evidence that bevacizumab substantially decreases the effects of radiation necrosis (15-23). A recent randomized double-blind study of bevacizumab therapy for the patients with radiation necrosis (19) provided evidence of its efficacy in mitigating radiation necrosis. These studies relied on MR imaging, and, in particular, T1 post-gadolinium enhancement to characterize radiation necrosis, which is complicated by the presence of recurrent tumor. Also, because it is generally not possible to correlate time-course MR observations with histologic findings in patients, these human studies lack information regarding the mechanisms of action of bevacizumab. Thus, further studies are needed to validate the effects and mechanisms of bevacizumab in the treatment of radiation necrosis.
We have recently developed a mouse model of delayed time-to-onset injury (24) that recapitulates the histologic features observed in patients suffering from CNS radiation necrosis. This model provides a platform for studies aimed at developing methods to identify/detect, monitor, protect against, and mitigate radiation necrosis, and distinguish it from tumor regrowth. In the work reported herein, this model is employed to validate the efficacy of both murine and humanized anti-VEGF-A monoclonal antibodies as mitigators of radiation necrosis following high-dose radiation treatment.
Materials and Methods
Animals
All studies were performed in accordance with the guidelines of the IACUC and in accordance with protocols approved by the Washington University Division of Comparative Medicine that met or exceeded American Association for the Accreditation of Laboratory Animal Care standards. Female Balb/c mice were used for the study and observed daily and weighed weekly to ensure that interventions were well tolerated.
Irradiation and Treatment
Mice were irradiated with the Leksell Gamma Knife® Perfexion™ (Elekta; Stockholm, Sweden; http://www.elekta.com/), a state-of-the-art unit used for stereotactic irradiation of patients with malignant brain tumors. Mice were supported on a specially designed platform mounted to the stereotactic frame that attaches to the treatment couch of the Gamma Knife. Mice were anesthetized with a mixture of ketamine (25 mg/kg), acepromazine (5 mg/kg) and xylazine (5 mg/kg), injected intraperitoneally 5 min before the start of irradiation. 35 female Balb/c mice were irradiated with either 60 Gy or 50 Gy, as described below, and the resulting brain parenchymal changes were characterized by both MRI and histology.
VEGF inhibitory monoclonal antibody
Bevacizumab (Genentech/Roche) is a humanized mAb (monoclonal antibody) that inhibits VEGF-A. Anti-VEGF antibody B20-4.1.1 (Genentech), heretofore referred to as B20-4.1.1, is a cross-species reactive, function-blocking mAb targeting both human and murine VEGF-A.
Experimental Outline
As part of the overall study, two different sets of experiments, designated as “A” and “B” were performed. In experiment “A”, two cohorts of mice (n=10 each) received a single 50-Gy dose (50% isodose) of Gamma Knife radiation. At this dose, the onset of radiation necrosis typically occurs approximately 4 weeks post-irradiation. Mouse cohort #1 was an irradiated, non-antibody (Ab)-treated, control group; cohort #2 received B20-4.1.1 (10 mg/kg), twice weekly, from 4-to-13 weeks post-irradiation. In experiment “B”, three cohorts of mice received a single fraction of 60-Gy radiation (50% isodose). At this dose, the onset of radiation necrosis typically occurs ~3 weeks post-irradiation. Mouse cohort #1 (n=5) was an irradiated, non-Ab-treated antibody, control group; cohort #2 (n=5) received B20-4.1.1 (10 mg/kg), twice weekly, from 3-to-10 weeks post-irradiation; cohort #3 (n=5) received bevacizumab (10 mg/kg, twice weekly) from 3-to-10 weeks post-irradiation. Antibodies were administered intraperitoneally.
MR Imaging
Images were collected in an Agilent/Varian (Santa Clara, CA) 4.7-T small-animal MR scanner equipped with a DirectDrive™ console. The scanner is built around an Oxford Instruments (Oxford, United Kingdom) 33-cm, clear-bore magnet equipped with 21-cm inner diameter, actively shielded Agilent/Magnex gradient coils (maximum gradient, 28 G/cm; rise time approximately 200 ms) and Oy International Electric Company (IEC; Helsinki, Finland) model A-240 amplifiers (300 V and 300 A). MRI data were collected using an actively decoupled coil pair: 1.5-cm outer diameter surface coil (receive) and a 9-cm inner diameter Helmholtz coil (transmit). Before the imaging experiments, mice were anesthetized with isoflurane/O2 (3% [vol/vol]) and maintained on isoflurane/O2 (1% [vol/vol]) throughout the experiments. Mice were restrained in a laboratory-constructed Teflon head holder with ear bars and a tooth bar. To maintain the body temperature of the mice at approximately 37°, mice placed on a water pad circulating warm water. Mice were injected intraperitoneally with 0.5 mL Omniscan (gadodiamide; GE Healthcare, Princeton, NJ) contrast agent, diluted 1:10 in sterile saline.
Non-Ab-treated mice treated with 50 Gy of radiation were imaged 4, 8, and 13 weeks post-irradiation. Ab-treated mice that had received 50 Gy of radiation were imaged 4, 5, 7, 9, 11, and 13 weeks post-irradiation. Mice that had received 60 Gy of radiation were imaged weekly from 3-to-10 weeks post-irradiation (non-Ab-treated mice were not imaged at week 9). Multislice, T2-weighted, spin-echo transaxial images were collected beginning ~3 minutes following gadodiamide administration with the following parameters: time to repetition [TR] = 1.5 s, time to echo [TE] = 0.05 s, field of view [FOV] = 1.5 × 1.5 cm2, slice thickness = 0.5 mm, 21 slices to cover the whole brain; total acquisition time = 12 minutes. Multislice, T1-weighted, spin-echo transaxial images were then collected over 5 minutes with the following parameters: TR = 0.65 s, TE = 0.02 s, FOV = 1.5 × 1.5 cm2, slice thickness = 0.5 mm, 21 slices to cover the whole brain.
Histology
Immediately after the last MR imaging session (13 weeks post-irradiation for mice receiving 50-Gy irradiation, 10 weeks post-irradiation for mice receiving 60-Gy irradiation), all the mice were perfused intracardially with 0.1 M Phosphate-buffered saline and formalin. The heads were then dissected and immersed in formalin for 24 hrs. All the brains were removed from skulls and embedded in paraffin. A single, 8-micron-thick coronal tissue section was taken from each brain near the radiation center and stained with hematoxylin and eosin (H&E) according to standard protocols. Histologic comparison of tissue sections was facilitated by the accurate targeting of radiation, ensuring that all histologic slices reflected the same anatomic features.
Statistical Analysis
For experiment “A”, Laird and Ware's growth curve method (25) was used to compare the differences in the rates of progression of radiation necrosis, since the Ab-treated and non-Ab-treated irradiated cohorts were imaged at different time points. For experiment “B”, in addition to the overall rates of progression, two-way ANOVA for repeated measurement data was also used to compare the MRI-derived necrotic volumes between Ab-treated and non-Ab-treated irradiated cohorts, followed by ad hoc multiple comparisons for differences at specific time points. All the tests were two-sided and a p-value of 0.05 or less was taken to indicate statistical significance. The statistical analysis was performed using SAS 9.3 (SAS Institutes, Cary, NC).
Results
MRI detects radiation necrosis as image hyperintensity in T2-weighted images
We have established a robust murine model of radiation necrosis using a Gamma Knife Perfexion to hemispherically target mouse brain. Representative T2-weighted spin-echo images of control, bevacizumab-treated, and B20-4.1.1-treated mice, covering the same anatomic region of the brain and collected at 3, 6, and 10 weeks following a single 60 Gy dose of radiation, are shown in Figure 1. Hyperintense areas in these images correspond with region of radiation necrosis in the brain. Significant hyperintense regions are clearly seen in non-Ab-treated, control mice at 6 weeks post irradiation and these regions expand significantly in extent by 10 weeks. The images of mice treated with B20-4.1.1 show minimal hyperintensity, even at 10 weeks post irradiation, while the images of bevacizumab-treated mice describe an intermediate situation, showing no hyperintense regions at 6 weeks but small such regions at 10 weeks post irradiation.
Figure 1.

MRI can detect radiation necrosis in irradiated brain. Representative, transaxial, T2-weighted spin-echo images acquired longitudinally from non-Ab-treated, bevacizumab-treated, and B20-4.1.1-treated mice at 3 (top), 6 (middle) and 10 weeks (bottom) following a single 60 Gy at (50% isodose) of radiation. Slices are chosen to display the same anatomic region of the brain at all three time points.
Necrosis volumes can be measured quantitatively from MR images
An important aspect of the non-invasive MR imaging is the ability to measure quantitatively the progression of radiation necrosis. For each set of T2-weighted spin-echo images, regions of interest were drawn around the entire brain in several contiguous image slices, chosen to include the entire hyperintense region. Each brain was divided along the midline into left (irradiated) and right (nonirradiated) hemispheres. The image intensity for each individual pixel in the left hemisphere was normalized by the average of the 25 pixels (5 × 5 square) including and immediately surrounding its mirror-image pixel in the right hemisphere, and histograms of normalized intensity for the irradiated hemisphere were constructed, as shown in Figure 2. The same analysis was performed on a cohort (n=10) of non-irradiated mice. The histogram of average intensity distribution for non-irradiated subjects, shown in Figure 2A, is symmetric; 99% of the pixels are distributed in the intensity range 0.6 – 1.4 about a normalized mean of 1.0. Therefore, an intensity threshold of 1.4 was chosen as the cutoff for normal brain tissue. For images of irradiated mice with/without treatment at different weeks post-irradiation, the number of pixels exceeding this threshold serves to measure the necrotic volume at each time point. Figure 2B shows image-pixel intensity histograms for B20-4.1.1- and bevacizumab-treated mice at 6 and 10 weeks following a single 60-Gy dose of radiation. The rates of progression of radiation necrosis over the designated time period can be derived from the slopes of least-squares fits of number of pixels versus time over the designated period.
Figure 2.
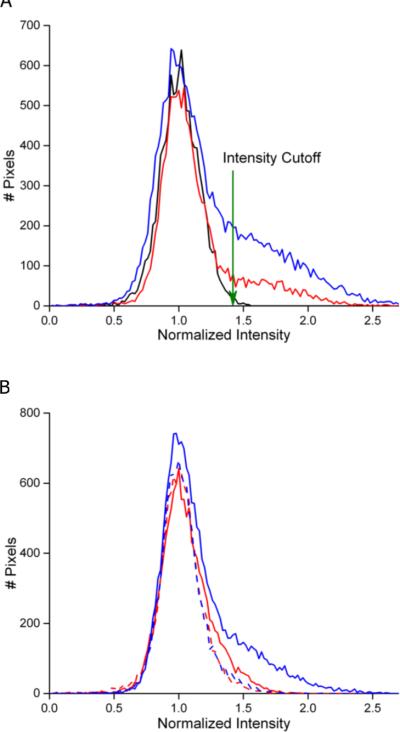
Histogram analysis enables quantitative MRI measurement of necrotic volume. (A) Image-pixel intensity histograms for the same non-Ab-treated mouse at 6 and 10 weeks following a single 60 Gy of radiation (red, blue) and average intensity histogram for 10 non-irradiated non-Ab-treated mice (black). The intensity cutoff used to define hyperintense pixels, corresponding to necrotic tissue, is indicated by the labeled arrow at a normalized intensity of 1.4. (B) Image-pixel intensity histograms for the same B20-4.1.1-treated (red) and bevacizumab-treated (blue) mice at 6 (dash line) and 10 (solid line) weeks following a single 60-Gy dose of radiation.
Anti-VEGF antibodies slow the progression of radiation necrosis in irradiated brain tissue
Treatment with anti-VEGF antibodies is an important potential strategy for mitigating the development of radiation necrosis. Figure 3 shows the progression of the mean volumes of MRI-derived necrotic regions for non-Ab-treated and B20-4.1.1-treated mice in Experiment A, in which all the mice received a single, 50-Gy dose of radiation. There was almost no progression of radiation necrosis in the B20-4.1.1-treated cohort (p < 0.0001, week 13) compared to non-Ab-treated control, indicating a significant mitigative effect due to the treatment.
Figure 3.

MRI-derived necrotic volumes in mice irradiated hemispherically with a single 50-Gy dose of GK radiation. MRI-defined volumes, mean ± SD (n = 10), of radiation necrosis vs. time post-irradiation for non-Ab-treated and B20-4.1.1-treated mice; all the mice received a single 50-Gy of radiation (50% isodose). At 13 weeks post-irradiation, the difference in MRI-derived necrotic volumes for the B20-4.1.1-treated cohort and the non-Ab-treated controls was statistically significant (p < 0.0001).
Figure 4A shows the progression of the mean volumes of necrotic region for non-Ab-treated, bevacizumab-treated, and B20-4.1.1-treated cohorts in Experiment B, in which all the mice received a single 60 Gy dose of radiation. The overall slope of the progression curve for B20-4.1.1-treated mice is slightly negative, demonstrating the mitigative effect of B20-4.1.1 where the treated cohort had a greatly diminished volume of necrosis at weeks 6 - 10 post-irradiation compared to non-Ab-treated controls (p < 0.0001, weeks 6, 7, 8 and 10). Bevacizumab also slows the overall rate of progression (p<0.0001, weeks 6, 7, 8 and 10). Considering the initial 3-7 week period post-irradiation, bevacizumab has the same mitigative effect as B20-4.1.1 (p = 0.8, week 7). However, for the latter 7-10 week period, radiation-induced necrosis developed at a higher rate than in the B20-4.1.1-treated cohort (p<0.0001, week 10), indicating that the mitigative effect of bevacizumab was weaker than B20-4.1.1 in the late period following the initiation of treatment.
Figure 4.

MRI-derived necrotic volumes in mice irradiated hemispherically with a single 60-Gy dose of GK radiation. (A) MRI-defined volumes, mean ± SD (n = 5), of radiation necrosis vs. time post-irradiation for non-Ab-treated, bevacizumab -treated, and B20-4.1.1-treated mice; all the mice received a single 60-Gy of radiation (50% isodose). Necrotic volumes for both B20-4.1.1-treated and bevacizumab-treated cohorts were significantly smaller than for the non-Ab-treated cohort (p<0.0001 at weeks 6, 7, 8, and 10 post-irradiation). MR-derived necrotic volumes for B20-4.1.1-treated and bevacizumab-treated cohorts were significantly different from one another at weeks 8, 9, and 10 post-irradiation (p<0.0001), but not at week 7 post-irradiation (p = 0.8).
(B) MRI-defined volumetric rate of radiation necrosis progression, mean ± SD (n = 5), derived from the slope of the curves in the left panel, for the 3-7 and 7-10 week periods. The rate of progression of necrosis for the B20-4.1.1-treated cohort was smaller than that for the non-Ab-treated cohort over both the 3-7 week (p<0.0001) and 7-10 week (p=0.0002) post-irradiation periods. For the bevacizumab-treated cohort, the rate of progression of necrosis was smaller than that for the non-Ab-treated cohort over the initial 3-7 week post-irradiation period (p<0.0001), but not over the 7-10 week post-irradiation period (p=0.2).
These effects are evident in Figure 4B, in which the rates of progression of radiation necrosis for the three cohorts are plotted. The progression rate for the B20-4.1.1-treated cohort was substantially reduced relative to the non-Ab-treated cohort over both the 3-7 week (p<0.0001) and 7-10 week periods (p=0.0002) post-irradiation. While bevacizumab treatment slowed the rate of progression relative to the non-Ab-treated cohort during the initial 3-7 week period (p<0.0001), its effect was lost over the latter 7-10 week period (p=0.2). It is apparent that in mice, B20-4.1.1 was a more potent mitigator of radiation necrosis compared to bevacizumab.
Histology reveals that anti-VEGF antibodies mitigate radiation necrosis in irradiated brain tissue
To validate these imaging findings, histologic studies were performed on perfused mouse-brain tissue. Figure 5(A) shows representative 2x (top), 10x (middle) H&E histologic images and corresponding T2W MR images (bottom) for non-Ab-treated, bevacizumab -treated, and B20-4.1.1-treated mice at 10 weeks following a single, 60-Gy dose of radiation. Corresponding histologic images and T2-weighted images of control and B20-4.1.1 –treated mice following a single, 50-Gy fraction of radiation are shown in Figure 5(B). The irradiated hemispheres of the control mice demonstrated many of the classic histologic features of radiation necrosis, including fibrinoid vascular necrosis (black arrow), vascular telangiectasia (yellow arrows), hemorrhage (red arrow), and loss of neurons and edema (blue arrows) (26). In contrast, the irradiated hemisphere of the bevacizumab-treated mouse showed only modest tissue damage and the irradiated hemisphere of the B20-4.1.1-treated mouse displayed no visible tissue damage. These histologic findings support the MR data shown in Figs. 3 and 4, demonstrating a significant mitigative effect of anti-VEGF-A therapy.
Figure 5.
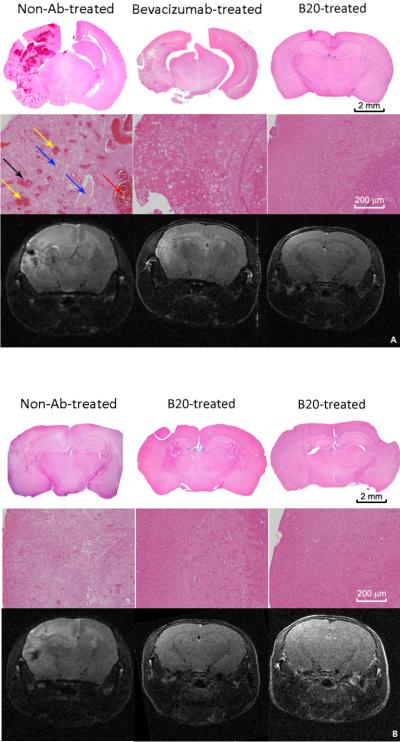
H&E-stained sections display characteristic histologic features of radiation necrosis and demonstrate mitigation by anti-VEGF Ab. (A) Representative 2× (top) and 10× (middle) H&E histology slices chosen near the radiation isocenter, and corresponding T2W images (bottom) for non-Ab-treated, bevacizumab-treated, and B20-4.1.1-treated mice at 10 weeks following a single 60-Gy fraction of radiation. (B) Representative 2× (top) and 10x (middle) H&E histology slices, and corresponding T2W images (bottom) for one control and two B20-4.1.1-treated mice at 13 weeks following a single 50-Gy fraction of radiation. The irradiated hemispheres of the control mice show many of the histologic features that are characteristic of radiation necrosis, including fibrinoid vascular necrosis (black arrow), vascular telangiectasia (yellow arrows), hemorrhage (red arrow), loss of neurons and edema (blue arrows). In addition, the tissue injury observed on the histology slices are highly correlated with the hyperintense regions on T2W images.
Discussion
Surgery, chemotherapy, and/or radiation are modalities utilized in treatment protocols for patients with brain neoplasms. The risk of late-onset radiation necrosis significantly limits the dose of radiation that can be employed in these protocols. The identification of agents that mitigate the delayed effects of radiation-induced changes on normal tissue, while not reducing the therapeutic efficacy of radiation on tumor tissue, could significantly increase the therapeutic ratio. Currently, the clinical therapeutic options for treating radiation necrosis are limited.
It has been suggested that radiation necrosis results from local tissue injury characterized by disruption of the blood-brain barrier and consequent tissue edema. Endothelial cell death, which results in breakdown of the blood-brain barrier, edema, and hypoxia and enhanced expression of VEGF has been described as an important step in the development of radiation necrosis (10). The mitigative potential of anti-VEGF therapy using bevacizumab in the treatment of radiation necrosis has been shown in several retrospective human studies and a recent prospective human study in a small number of patients (17-19, 22), though these studies lacked statistical power. MRI monitoring of the onset and progression of radiation necrosis, in concert with Gamma Knife irradiation, offers an attractive strategy for validating and optimizing anti-VEGF-Ab therapy. We have established an animal model that faithfully reproduces the histology of radiation necrosis observed in patients. Herein, we demonstrate that anti-VEGF antibodies can delay the onset of radiation necrosis and believe that the results of mitigation studies in the mouse will provide essential dosing and mechanism-of-action information, with direct relevance to ongoing clinical trials of bevacizumab.
In this study, the onset and progression of radiation necrosis in mouse brain were characterized by the volume of hyperintense regions on T2-weighted images. Characterization employing contrast-enhanced T1-weighted images yielded essentially equivalent findings (data not shown). The greatly reduced progression of radiation necrosis in treated mice, as measured longitudinally by in vivo MR imaging, and the much lighter tissue damage observed in H&E-stained tissue sections for bevacizumab- and B20-4.1.1-treated mice, demonstrated the efficacy of anti-VEGF-A therapy. B20-4.1.1 has a better mitigative effect than bevacizumab in the mouse model of radiation necrosis. The mitigative effects of bevacizumab disappeared approximately 4 weeks after the start of treatment (Fig. 4). This may be due to an anti-idiotypic immunogenic response (27-29), whereby murine antibodies directed against the antigen specific part of bevacizumab are produced, thereby inhibiting its binding to mouse VEGF. The greater therapeutic efficacy of B20-4.1.1 is likely due to its higher affinity for mouse VEGF-A (30).
Although the results of the present study demonstrate that bevacizumab and B20-4.1.1 can significantly reduce the progression of radiation necrosis, the mechanism of the mitigative effect of these VEGF inhibitors remains undetermined and requires further investigation. Outstanding questions also remain regarding the ideal dosing schemes and the treatment periods for anti-VEGF-Ab therapy. Multiple dosing schemes, ranging from 5 mg/kg to 10 mg/kg have been reported in the treatments of tumor and radiation necrosis in both human (17, 19) and animal studies (31). Typically, bevacizumab, with a half-life of approximately 20 days in humans, is administered once every 2 or 3 weeks in patients (17, 19, 32), and once or twice weekly in mice (31, 33). For our mitigation study, a high-end dosing scheme (10 mg/kg, twice weekly) was chosen and demonstrated promising mitigative effects on radiation necrosis in mice. Nonetheless, minimizing the dose required to effective control the progression of necrosis will reduce patient costs and potential side effects, thereby improving the likelihood of effective clinical translation.
Conclusion
Herein, we describe a novel mouse model that can provide a platform for the development of methods to detect and monitor the progression of radiation necrosis, and for the identification of agents to protect against and mitigate radiation-induced necrosis. This mouse model will also enable studies to assess mechanism of action and optimize dosing of potential therapeutic agents. The data in this study demonstrate a significant mitigative effect of both bevacizumab and B20-4.1.1 on radiation necrosis. By reducing the development of necrosis following irradiation, anti-VEGF-Ab therapy may overcome the deleterious effects of focal irradiation to effectively treat lesions with fewer side effects.
Efforts to measure the effects of using lower doses of B20-4.1.1 in our mouse model are ongoing. Also, in the current studies, irradiated mice were treated with bevacizumab or B20-4.1.1 for 7 or 8 weeks, beginning with the first radiographic sign of radiation necrosis. However, the mitigative effectiveness found upon initiating the treatment earlier (e.g., immediately following irradiation) or stopping the treatment after a fixed period of time (e.g., 4 weeks) remain to be investigated. Future studies that address mechanism of action will include Dynamic Contrast-Enhanced MRI, an imaging method for quantitatively measuring vascular permeability (34, 35) and specific histological stains targeting permeability, such as Evans Blue (36).
Translational Relevance.
Radiation necrosis is a severe, but late occurring type of injury to normal tissue, within and surrounding a radiation treatment field, which can lead to significant complications for neurooncology patients. Radiation necrosis is difficult to distinguish from recurrent tumor by either neurologic examination or clinical imaging protocols. Concerns for the development of radiation necrosis often limit therapeutic radiation doses. Current treatment options for radiation necrosis are limited. In the present study, we demonstrate that treatment with anti-VEGF antibodies significantly reduces late-onset necrosis in irradiated brain in a mouse model of radiation necrosis. The animal model highlighted in these experiments can serve as a platform for studies aimed at optimizing the dosing and timing of anti-VEGFAb therapy. Findings from this work can provide direct, powerful support for ongoing and future clinical studies with bevacizumab, a FDA-approved humanized anti-VEGF antibody, for the treatment of radiation necrosis.
Acknowledgments
We thank Drs. Dinesh Thotala and Carlos Perez-Torres for valuable discussions and feedback. This project has been supported by NIH grants R01 CA155365 (JRG), R01 CA174966 (DEH), and R01 CA140220-01 (DEH), and funding from the Alvin J. Siteman Cancer Center, an NCI-comprehensive cancer center, P30 CA091842, the Barnes-Jewish Hospital Foundation Cancer Frontier Fund, and Elekta Instruments AB (Stockholm, Sweden). We gratefully acknowledge Genentech (South San Francisco, CA) for donation of anti-VEGF antibody B20-4.1.1.
Footnotes
Conflict of Interest: none
References
- 1.Giglio P, Gilbert MR. Cerebral radiation necrosis. Neurologist. 2003;9:180–8. doi: 10.1097/01.nrl.0000080951.78533.c4. [DOI] [PubMed] [Google Scholar]
- 2.Stupp R, Mason WP, van den Beuf MJ. Radiotherapy plus concomitant and adjuvant temozolomide for newly diagnosed glioblastoma (vol 352, pg 19, 2005). Annals of Oncology. 2005;16:949. [Google Scholar]
- 3.Stupp R, Hegi ME, Mason WP, van den Bent MJ, Taphoorn MJB, Janzer RC, et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncology. 2009;10:459–66. doi: 10.1016/S1470-2045(09)70025-7. [DOI] [PubMed] [Google Scholar]
- 4.Shaw PJ, Bates D. Conservative Treatment of Delayed Cerebral Radiation Necrosis. Journal of Neurology Neurosurgery and Psychiatry. 1984;47:1338–41. doi: 10.1136/jnnp.47.12.1338. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Siu A, Wind JJ, Iorgulescu JB, Chan TA, Yamada Y, Sherman JH. Radiation necrosis following treatment of high grade glioma-a review of the literature and current understanding. Acta Neurochirurgica. 2012;154:191–201. doi: 10.1007/s00701-011-1228-6. [DOI] [PubMed] [Google Scholar]
- 6.Tibbles PM, Edelsberg JS. Medical progress - Hyperbaric-oxygen therapy. New England Journal of Medicine. 1996;334:1642–8. doi: 10.1056/NEJM199606203342506. [DOI] [PubMed] [Google Scholar]
- 7.But QC, Lieber M, Withers HR, Corson K, van Rijnsoever M, Elsaleh H. The efficacy of hyperbaric oxygen therapy in the treatment of radiation-induced late side effects. International Journal of Radiation Oncology Biology Physics. 2004;60:871–8. doi: 10.1016/j.ijrobp.2004.04.019. [DOI] [PubMed] [Google Scholar]
- 8.Kohshi K, Imada H, Nomoto S, Yamaguchi R, Abe H, Yamamoto H. Successful treatment of radiation-induced brain necrosis by hyperbaric oxygen therapy. Journal of the Neurological Sciences. 2003;209:115–7. doi: 10.1016/s0022-510x(03)00007-8. [DOI] [PubMed] [Google Scholar]
- 9.Rahmathulla G, Marko NF, Weil RJ. Cerebral radiation necrosis: A review of the pathobiology, diagnosis and management considerations. J Clin Neurosci. 2013;20:485–502. doi: 10.1016/j.jocn.2012.09.011. [DOI] [PubMed] [Google Scholar]
- 10.Wong CS, Van der Kogel AJ. Mechanisms of radiation injury to the central nervous system: implications for neuroprotection. Molecular Interventions. 2004;4:273–84. doi: 10.1124/mi.4.5.7. [DOI] [PubMed] [Google Scholar]
- 11.Remler MP, Marcussen WH, Tiller-Borsich J. The late effects of radiation on the blood brain barrier. Int J Radiat Oncol Biol Phys. 1986;12:1965–9. doi: 10.1016/0360-3016(86)90133-1. [DOI] [PubMed] [Google Scholar]
- 12.Norden AD, Drappatz J, Wen PY. Antiangiogenic therapies for high-grade glioma. Nat Rev Neurol. 2009;5:610–20. doi: 10.1038/nrneurol.2009.159. [DOI] [PubMed] [Google Scholar]
- 13.Jain RK. Normalization of tumor vasculature: An emerging concept in antiangiogenic therapy. Science. 2005;307:58–62. doi: 10.1126/science.1104819. [DOI] [PubMed] [Google Scholar]
- 14.Dings RPM, Loren M, Heun H, McNiel E, Griffioen AW, Mayo KH, et al. Scheduling of radiation with angiogenesis inhibitors anginex and avastin improves therapeutic outcome via vessel normalization. Clinical Cancer Research. 2007;13:3395–402. doi: 10.1158/1078-0432.CCR-06-2441. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Ananthnarayan S, Bahng J, Roring J, Nghiemphu P, Lai A, Cloughesy T, et al. Time course of imaging changes of GBM during extended bevacizumab treatment. Journal of Neuro-Oncology. 2008;88:339–47. doi: 10.1007/s11060-008-9573-x. [DOI] [PubMed] [Google Scholar]
- 16.Boothe D, Young R, Yamada Y, Prager A, Chan T, Beal K. Bevacizumab as a treatment for radiation necrosis of brain metastases post stereotactic radiosurgery. Neuro Oncol. 2013;15:1257–63. doi: 10.1093/neuonc/not085. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Gonzalez J, Kumar AJ, Conrad CA, Levin VA. Effect of bevacizumab on radiation necrosis of the brain. International Journal of Radiation Oncology Biology Physics. 2007;67:323–6. doi: 10.1016/j.ijrobp.2006.10.010. [DOI] [PubMed] [Google Scholar]
- 18.Jeyaretna DS, Curry WT, Batchelor TT, Stemmer-Rachamimov A, Plotkin SR. Exacerbation of Cerebral Radiation Necrosis by Bevacizumab. Journal of Clinical Oncology. 2011;29:E159–E62. doi: 10.1200/JCO.2010.31.4815. [DOI] [PubMed] [Google Scholar]
- 19.Levin VA, Bidaut L, Hou P, Kumar AJ, Wefel JS, Bekele BN, et al. Randomized Double-Blind Placebo-Controlled Trial of Bevacizumab Therapy for Radiation Necrosis of the Central Nervous System. International Journal of Radiation Oncology Biology Physics. 2011;79:1487–95. doi: 10.1016/j.ijrobp.2009.12.061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lubelski D, Abdullah KG, Weil RJ, Marko NF. Bevacizumab for radiation necrosis following treatment of high grade glioma: a systematic review of the literature. J Neurooncol. 2013;115:317–22. doi: 10.1007/s11060-013-1233-0. [DOI] [PubMed] [Google Scholar]
- 21.Sadraei NH, Dahiya S, Chao ST, Murphy ES, Osei-Boateng K, Xie H, et al. Treatment of Cerebral Radiation Necrosis With Bevacizumab: The Cleveland Clinic Experience. American journal of clinical oncology. 2013 Jun 24; doi: 10.1097/COC.0b013e31829c3139. E pub. [DOI] [PubMed] [Google Scholar]
- 22.Torcuator R, Mohan YS, Lee I, Rock J, Doyle T, Anderson J, et al. Initial experience with bevacizumab treatment for biopsy-confirmed cerebral radiation necrosis. Neuro-Oncology. 2007;9:580–1. doi: 10.1007/s11060-009-9801-z. [DOI] [PubMed] [Google Scholar]
- 23.Wang Y, Pan L, Sheng X, Mao Y, Yao Y, Wang E, et al. Reversal of cerebral radiation necrosis with bevacizumab treatment in 17 Chinese patients. European journal of medical research. 2012;17:25. doi: 10.1186/2047-783X-17-25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Jost SC, Hope A, Kiehl E, Perry A, Travers S, Garbow JR. A Novel Murine Model for Localized Radiation Necrosis and Its Characterization Using Advanced Magnetic Resonance Imaging. International Journal of Radiation Oncology Biology Physics. 2009;75:527–33. doi: 10.1016/j.ijrobp.2009.06.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Laird NM, Ware JH. Random-effects models for longitudinal data. Biometrics. 1982;38:963–74. [PubMed] [Google Scholar]
- 26.Perry A, Schmidt RE. Cancer therapy-associated CNS neuropathology: an update and review of the literature. Acta Neuropathologica. 2006;111:197–212. doi: 10.1007/s00401-005-0023-y. [DOI] [PubMed] [Google Scholar]
- 27.Shawler DL, Bartholomew RM, Smith LM, Dillman RO. Human Immune-Response to Multiple Injections of Murine Monoclonal Igg. Journal of Immunology. 1985;135:1530–5. [PubMed] [Google Scholar]
- 28.Herlyn D, Lubeck M, Sears H, Koprowski H. Specific Detection of Anti-Idiotypic Immune-Responses in Cancer-Patients Treated with Murine Monoclonal-Antibody. Journal of Immunological Methods. 1985;85:27–38. doi: 10.1016/0022-1759(85)90271-6. [DOI] [PubMed] [Google Scholar]
- 29.Fagerberg J, Ragnhammar P, Liljefors M, Hjelm AL, Mellstedt H, Frodin JE. Humoral anti-idiotypic and anti-anti-idiotypic immune response in cancer patients treated with monoclonal antibody 17-1A. Cancer Immunology Immunotherapy. 1996;42:81–7. doi: 10.1007/s002620050255. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Yu LL, Wu XM, Cheng ZY, Lee CV, LeCouter J, Campa C, et al. Interaction between bevacizumab and murine VEGF-A: A reassessment. Investigative Ophthalmology & Visual Science. 2008;49:522–7. doi: 10.1167/iovs.07-1175. [DOI] [PubMed] [Google Scholar]
- 31.de Groot JF, Fuller G, Kumar AJ, Piao Y, Eterovic K, Ji YJ, et al. Tumor invasion after treatment of glioblastoma with bevacizumab: radiographic and pathologic correlation in humans and mice. Neuro-Oncology. 2010;12:233–42. doi: 10.1093/neuonc/nop027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Ferrara N, Hillan KJ, Gerber HP, Novotny W. Discovery and development of bevacizumab, an anti-VEGF antibody for treating cancer. Nature Reviews Drug Discovery. 2004;3:391–400. doi: 10.1038/nrd1381. [DOI] [PubMed] [Google Scholar]
- 33.Ferrara N, Hillan KJ, Novotny W. Bevacizumab (Avastin), a humanized anti-VEGF monoclonal antibody for cancer therapy. Biochemical and Biophysical Research Communications. 2005;333:328–35. doi: 10.1016/j.bbrc.2005.05.132. [DOI] [PubMed] [Google Scholar]
- 34.O'Connor JPB, Jackson A, Parker GJM, Jayson GC. DCE-MRI biomarkers in the clinical evaluation of antiangiogenic and vascular disrupting agents. British Journal of Cancer. 2007;96:189–95. doi: 10.1038/sj.bjc.6603515. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Padhani AR, Husband JE. Dynamic contrast-enhanced MRI studies in oncology with an emphasis on quantification, validation and human studies. Clinical Radiology. 2001;56:607–20. doi: 10.1053/crad.2001.0762. [DOI] [PubMed] [Google Scholar]
- 36.Xu QW, Qaum T, Adamis AP. Sensitive blood-retinal barrier breakdown quantitation using Evans blue. Investigative Ophthalmology & Visual Science. 2001;42:789–94. [PubMed] [Google Scholar]